Cubital Tunnel Syndrome
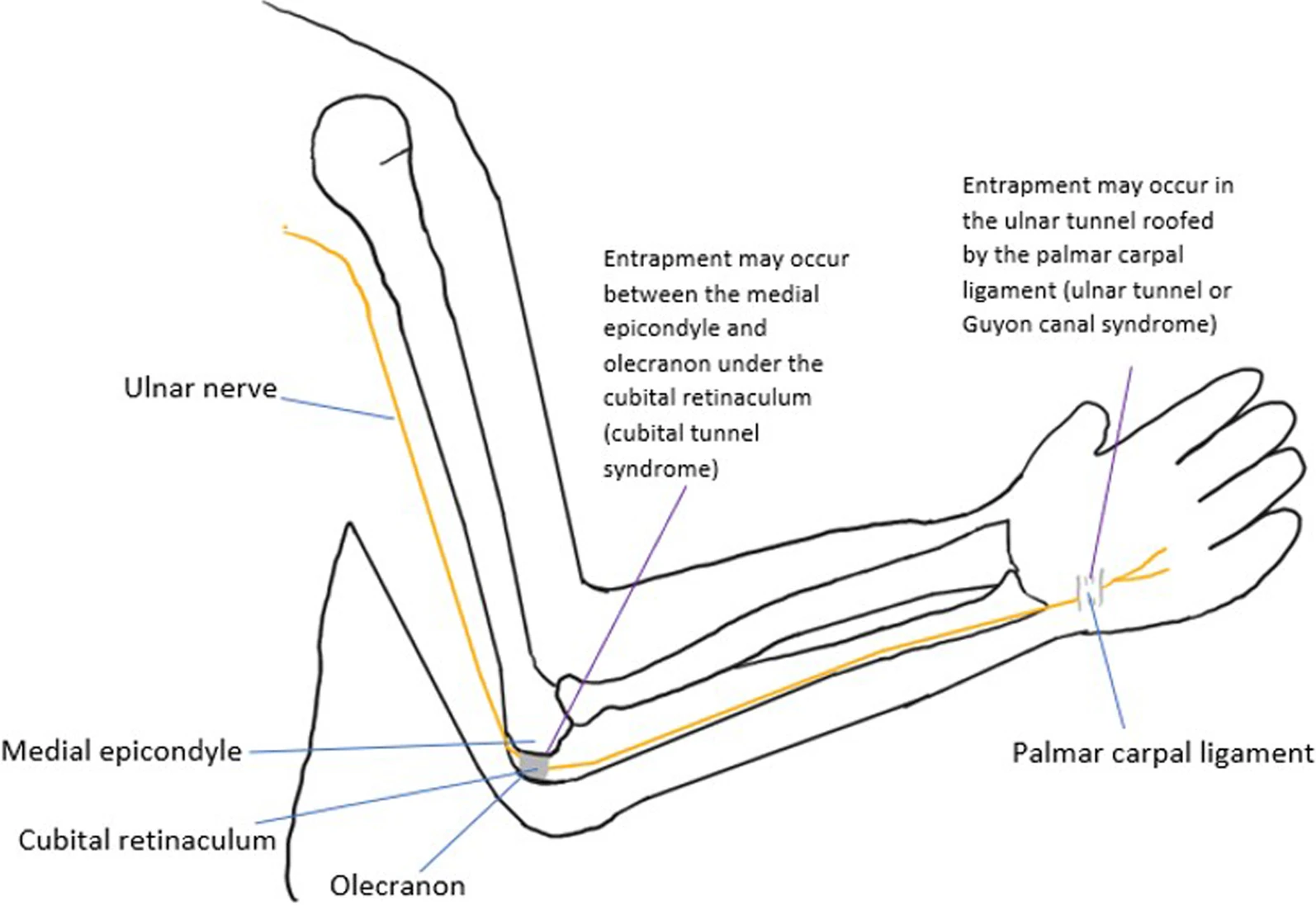
Clinical photograph demonstrating ulnar nerve palsy with intrinsic wasting (first dorsal interosseous, hypothenar) and claw deformity of ring and small fingers (MCP hyperextension, IP flexion). The anatomical diagram shows the course of the ulnar nerve through the cubital tunnel, bounded by the medial epicondyle, olecranon, and Osborne's ligament. FCU muscle belly forms the distal tunnel boundary.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the anatomy of the ulnar nerve at the elbow and potential sites of compression.
What are the clinical features and examination findings?
Describe the surgical options for cubital tunnel syndrome.
How do you investigate and stage the severity?
What are the outcomes and complications of surgery?
How do you differentiate cubital tunnel from other causes of ulnar neuropathy?
Must Mention
- •Second most common entrapment
- •Osborne's ligament = tunnel roof
- •DBUN sensory loss = elbow level
- •Froment's = FPL compensating
- •Wartenberg's = small finger abduction
- •Ulnar paradox = high lesion less claw
Common Pitfalls
- •Missing DBUN
- •Confusing with Guyon's
- •Wrong exam tests
- •Missing ulnar paradox
- •Wrong surgery choice
- •Missing arcade