Distal Radius Fracture
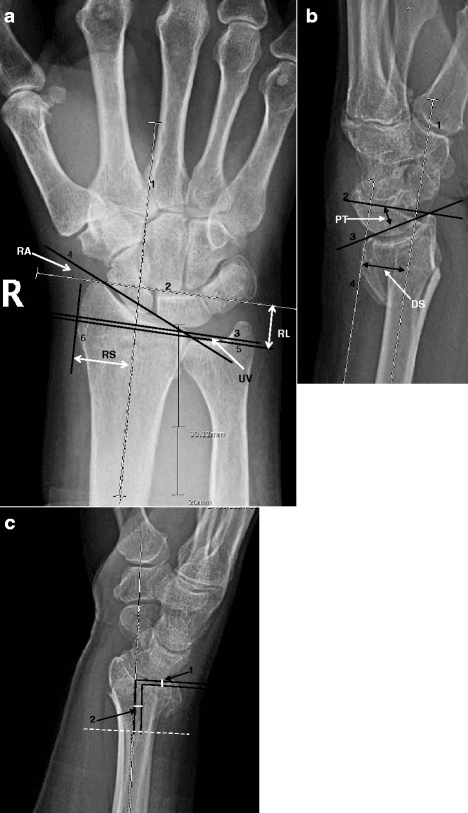
PA and lateral wrist radiographs of a 58-year-old female showing a dorsally displaced distal radius fracture. Key measurements: dorsal tilt 25° (normal 11° volar), radial inclination 12° (normal 22°), radial height 8mm (normal 12mm), positive ulnar variance. Intra-articular step-off of 2mm is visible. This represents an unstable fracture pattern requiring surgical fixation.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the normal radiographic parameters of the distal radius and criteria for instability.
Classify distal radius fractures using the Frykman and AO systems.
Describe the surgical technique for volar locking plate fixation.
What are the associated injuries and how do you assess for them?
What are the complications of distal radius fractures and their management?
Discuss the treatment of distal radius fractures in the elderly.
Must Mention
- •Normal: inclination 22°, height 12mm, volar tilt 11°
- •Instability: dorsal tilt >10°, shortening >5mm, step >2mm
- •Volar plate: proximal to watershed line
- •Check DRUJ stability intra-op
- •EPL rupture = attritional, EIP transfer
- •DRAFFT: no difference plate vs K-wire
Common Pitfalls
- •Wrong normal values
- •Missing DRUJ check
- •Forgetting EPL
- •Not knowing trials
- •Missing watershed line
- •Wrong classification