Dupuytren's Disease
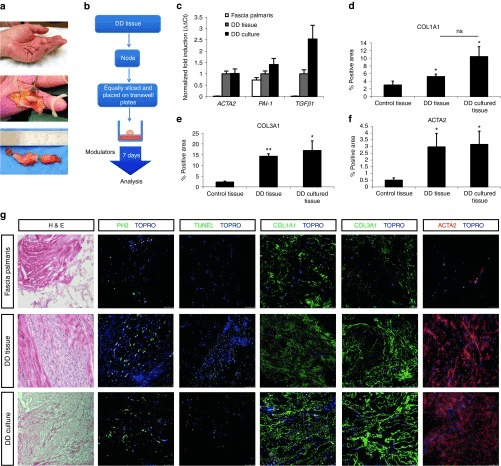
Clinical photograph of the right hand showing Dupuytren's disease. A palpable cord extends from the palm to the ring finger causing MCP flexion contracture of 40° and PIP contracture of 30°. Skin pitting is visible over the cord. The small finger shows early nodule formation. The table-top test is positive (palm cannot be placed flat on table). This patient meets criteria for fasciectomy (MCP >30° or PIP >20°).
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the anatomy of the palmar fascia and the pathological cords in Dupuytren's disease.
What are the risk factors, associations, and clinical features?
Describe the surgical technique for fasciectomy.
What are the treatment options and their indications?
What are the complications and how do you manage them?
Discuss the prognostic factors and recurrence.
Must Mention
- •Spiral cord displaces NV bundle centrally/superficially
- •Table-top test (Hueston)
- •Surgery: MCP >30°, PIP >20°
- •Fasciectomy = gold standard, lowest recurrence
- •Diathesis = bilateral, ectopic, family, young, male
- •PIP = worse prognosis
Common Pitfalls
- •Forgetting spiral cord
- •Wrong surgical threshold
- •Missing diathesis
- •Wrong recurrence rates
- •Missing PIP prognosis
- •Confusing extension vs recurrence