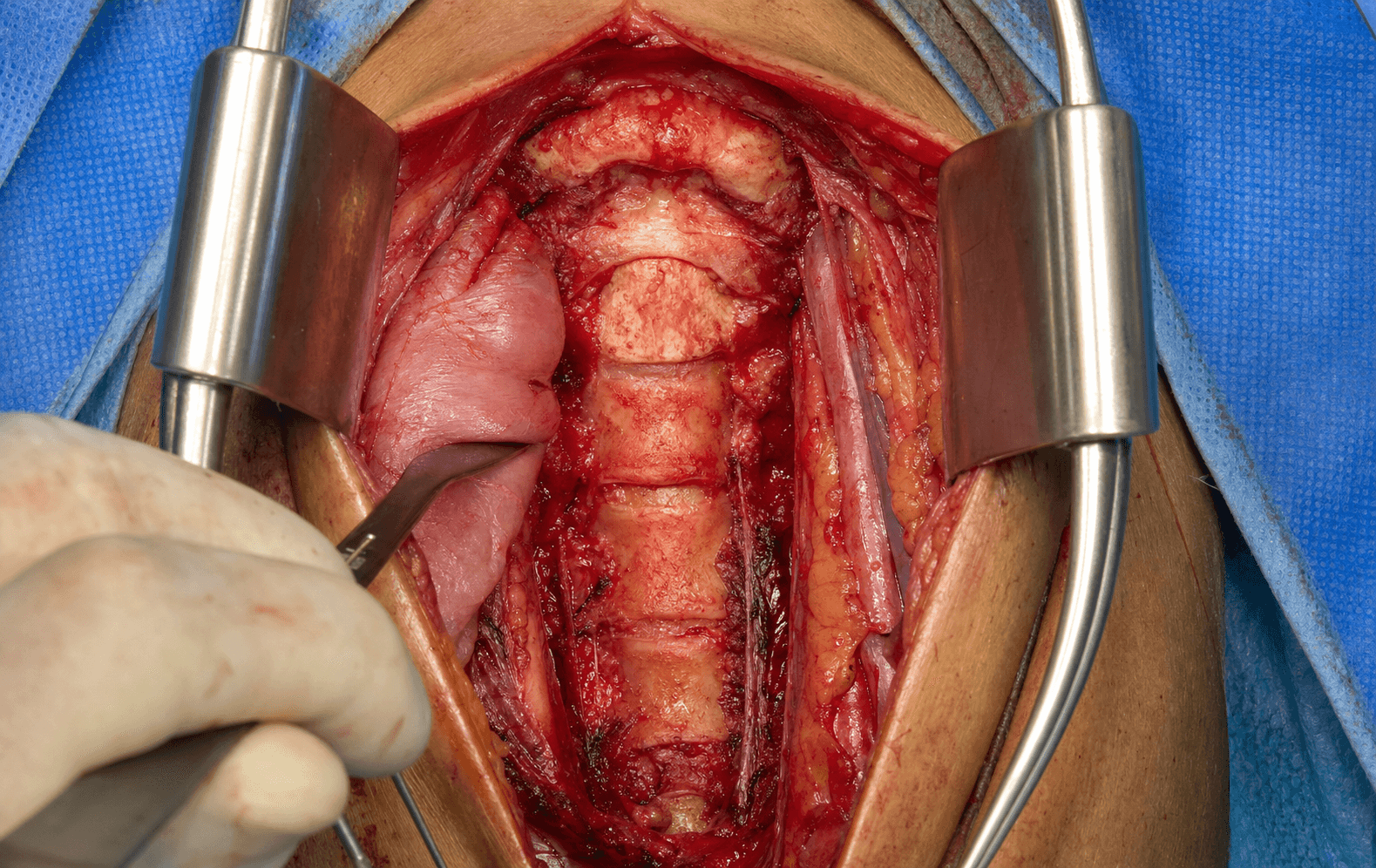
Supine, extraoral exposure of the craniovertebral junction — the plane medial to the carotid sheath and lateral to the visceral column, reaching the anterior arch of C1, the odontoid and the bodies of C2–C3.
- Supine with the head rotated 30–40 degrees away from the operative side and extended 10–15 degrees.
- Protect the marginal mandibular branch of the facial nerve first — ligate the retromandibular vein and facial vessels and retract the nerve cephalad with the submandibular gland.
- The deep plane is medial to the carotid sheath and lateral to the visceral column (pharynx, larynx, trachea, oesophagus) — a true internervous interval (vagus versus pharyngeal plexus), with no muscle divided.
- Identify the hypoglossal nerve at the hyoid (C3) and the superior laryngeal nerve during pharyngeal retraction.
- The longus colli is the midline landmark; the exposure extends caudally into a standard Smith–Robinson approach to reach C3–C7 without repositioning.
When & Why
What it exposes. The anterior retropharyngeal approach (Robinson–Southwick, with the McAfee modification) gives extraoral access to the craniovertebral junction — the anterior arch of C1, the odontoid process, and the bodies of C2 and C3. It reaches the same anterior column as a transoral route but through a sterile, clean field. Why extraoral. By staying clear of the oral cavity it avoids salivary bacterial contamination — infection after retropharyngeal surgery runs 1–4 percent versus 10–20 percent after a transoral route — which matters most for implant work such as odontoid screws, anterior C1–C2 plating and strut grafting. When pathology drops below C3, the same plane continues seamlessly into a standard Smith–Robinson anterior cervical exposure. Indications - Odontoid fracture nonunion or malunion needing direct anterior access
- Basilar invagination or cranial settling with anterior compression
- Upper cervical (C1–C3) tumours — chordoma, metastasis, plasmacytoma
- Pyogenic or tuberculous osteomyelitis or discitis of C1–C3 needing debridement and grafting
- Anterior C1–C2 or C2–C3 corpectomy and reconstruction when the transoral route is contraindicated
- Revision anterior surgery after failed transoral or posterior procedures Contraindications - Active infection of the submandibular or anterior neck skin
- Severe trismus or limited mouth opening (relative — may still be feasible)
- An unstable cervical spine without prior posterior stabilisation (relative)
- Previous radical neck dissection on the ipsilateral side (altered vascular anatomy)
- Patient factors precluding supine positioning with head extension Alternative approaches
- Access
- Extraoral, C1–C3, extends to C7
- Infection risk
- Low (1–4%)
- Best for
- Clean-field implant work, odontoid screws, tumour
- Access
- Direct midline C1–C2
- Infection risk
- High (10–20%)
- Best for
- Midline upper-clival pathology; limited lateral access
- Access
- Posterior stabilisation
- Infection risk
- Low
- Best for
- Posterior compression, instability without anterior decompression
- Access
- More lateral exposure
- Infection risk
- Moderate
- Best for
- Selected lateral pathology; greater morbidity
- Access
- Midline upper clivus
- Infection risk
- Low
- Best for
- Selected centres, purely midline upper clival disease
Position & landmarks. Supine on a radiolucent table, with a shoulder roll and the head extended 10–15 degrees and rotated 30–40 degrees away from the operative side. Gardner–Wells tongs or a Mayfield head holder give controlled positioning for odontoid screw trajectory; arms are tucked with slight traction for fluoroscopic access. The C-arm is set for true lateral and open-mouth AP views of C1–C2, the endotracheal tube is secured on the contralateral side, and MEP/SSEP neuromonitoring is recommended. Palpable landmarks: the inferior border of the mandible (incision placed 2–3 cm below it), the hyoid at C3 (marks the hypoglossal nerve), the thyroid cartilage (C4–C5), the cricoid (C6), the submandibular gland and the carotid pulse. Incision choice
- Incision
- 6–8 cm horizontal, 2 cm below the mandible
- Indication
- Isolated C1–C2 pathology (standard)
- Incision
- From the angle of the mandible along the anterior SCM toward the sternal notch
- Indication
- Multilevel C1–C5; caudal extension
- Incision
- Continuous caudal extension along SCM
- Indication
- C1–C7 pathology, single field
The Exposure
The exposure is built in layers from the skin to the prevertebral fascia: protect the marginal mandibular nerve superficially, open the plane between the carotid sheath and the visceral column, then detach the longus colli to reach the anterior column of C1–C3.
Exposure sequence
- Make a transverse submandibular incision 2 cm below the inferior mandibular border, from the midline to the anterior border of the sternocleidomastoid (about 6–8 cm).
- Divide the platysma in line with the skin incision.
- Identify the marginal mandibular branch of the facial nerve (CN VII) in the subcutaneous plane and protect it by ligating the retromandibular vein and the facial artery and vein, then retracting the nerve cephalad with the submandibular gland.
- Incise the investing deep cervical fascia along the anterior border of the sternocleidomastoid.
- Identify the carotid sheath and retract it laterally with a vessel loop or hand-held retractor; mobilise the visceral column (pharynx, larynx, trachea, oesophagus) medially.
- Identify the hypoglossal nerve (CN XII) crossing the field at the level of the hyoid bone, medial to the carotid sheath, and gently mobilise it laterally.
- Protect the superior laryngeal nerve with gentle medial retraction of the pharynx.
- Divide the prevertebral fascia in the midline to enter the retropharyngeal space.
- The plane is medial to the carotid sheath and lateral to the visceral column — a true internervous interval, with no muscle divided.
- Use the longus colli as the midline landmark; confirm the midline by palpating the anterior tubercle of C1 and the odontoid.
- Detach the longus colli subperiosteally from the anterior tubercles of C1–C3 and reflect it laterally to the uncovertebral joints.
- The anterior arch of C1, the odontoid process and the bodies of C2 and C3 are now exposed; divide the anterior longitudinal ligament in the midline and extend subperiosteally to the lateral masses of C1 and the transverse processes of C2–C3 as needed.
- For odontoid work, divide the apical and alar ligaments only if necessary; decorticate or resect the odontoid as the procedure demands.
- The C1–C2 joint can be reached laterally for intra-articular grafting or screw placement.
- Stay midline and avoid the vertebral artery in the transverse foramen of C2.
- Remove the C2 or C3 body with a high-speed burr and pituitary rongeurs; resect the posterior longitudinal ligament to decompress the thecal sac.
- Prepare the endplates for strut graft or cage reconstruction and anterior plating from C1 to C3.
The deep interval is genuinely internervous: the vagus nerve supplies the laryngeal muscles laterally and the pharyngeal plexus (CN IX and X) supplies the pharyngeal constrictors medially, so no muscle is divided. The technical discipline is to stay lateral to the visceral column and medial to the carotid sheath at every level. Superficially there is no internervous plane — the platysma is split in line and the marginal mandibular nerve is protected by early vessel ligation, not by an interval.
Head extension and pharyngeal retraction produce airway oedema and can make re-intubation difficult. Upper cervical anterior surgery carries a 5–15 percent risk of prolonged or repeat intubation. Plan a delayed-extubation or temporary-tracheostomy strategy before induction for extensive procedures or patients with pre-existing airway compromise.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Marginal mandibular branch (CN VII)
- Consequence of injury
- Ipsilateral lower-lip weakness, cosmetic asymmetry
- Protection
- Ligate the retromandibular vein and facial vessels; retract the nerve cephalad with the gland
- Structure at risk
- Facial artery and vein
- Consequence of injury
- Bleeding; limits gland mobilisation
- Protection
- Ligate and divide to mobilise the gland
- Structure at risk
- Hypoglossal nerve (CN XII)
- Consequence of injury
- Ipsilateral tongue deviation, dysphagia
- Protection
- Identify early, mobilise laterally with a vessel loop; avoid excessive retraction
- Structure at risk
- Superior laryngeal nerve (internal and external branches)
- Consequence of injury
- Loss of supraglottic sensation, aspiration, voice fatigue, hoarseness
- Protection
- Gentle medial retraction of the pharynx; avoid electrocautery near the nerve
- Structure at risk
- Common carotid, internal jugular, vagus
- Consequence of injury
- Stroke, venous congestion, vocal-cord paralysis
- Protection
- Identify early; gentle lateral retraction with hand-held retractors or vessel loops
- Structure at risk
- Sympathetic chain on longus colli
- Consequence of injury
- Horner syndrome (ptosis, miosis, anhidrosis)
- Protection
- Stay strictly midline; do not extend lateral to the uncovertebral joints
- Structure at risk
- Vertebral artery (transverse foramen of C2, over C1)
- Consequence of injury
- Devastating posterior-circulation stroke
- Protection
- Pre-operative CT angiography; stay midline until the lateral extent is confirmed
Nerve-injury management. Marginal mandibular or hypoglossal neuropraxia is observed — most recover within 3–6 months. Superior laryngeal nerve injury is managed with voice therapy and aspiration precautions. A permanent deficit after 12 months may need medialisation thyroplasty or tongue-suspension procedures. Complications
- Incidence
- 20–40% transient
- Prevention
- Gentle retraction, early swallow therapy
- Treatment
- Swallowing exercises; temporary NG feeding
- Incidence
- 5–15%
- Prevention
- Delayed-extubation plan
- Treatment
- Re-intubation or tracheostomy
- Incidence
- 10–20%
- Prevention
- Superior laryngeal nerve protection
- Treatment
- Voice therapy; medialisation if permanent
- Incidence
- 2–5%
- Prevention
- Peri-operative antibiotics
- Treatment
- Irrigation, debridement, antibiotics
- Incidence
- 1–3%
- Prevention
- Midline prevertebral dissection
- Treatment
- Observation; most resolve
- Incidence
- 1–2%
- Prevention
- Watertight dural closure
- Treatment
- Bed rest, lumbar drain, re-exploration
- Incidence
- 5–10%
- Prevention
- Rigid fixation, sound graft
- Treatment
- Revision or posterior augmentation
Extensile options - Caudal (Smith–Robinson): lengthen the incision along the anterior border of the sternocleidomastoid and continue in the same plane to C7 — the commonest extension, allowing ACDF, corpectomy or disc arthroplasty without repositioning.
- Proximal: limited extension toward the mastoid tip by mobilising the facial nerve further cephalad and dividing the posterior belly of digastric; true clival access needs a separate transoral or endoscopic endonasal route.
- Bilateral: two simultaneous retropharyngeal approaches for midline tumours or extensive infection — wider lateral exposure but higher bilateral nerve risk.
- Combined anterior–posterior (360-degree): anterior decompression first, then posterior occiput–C2 or C1–C3 instrumentation in the same or a staged procedure. Closure. Copious antibiotic-saline irrigation and meticulous haemostasis of the retropharyngeal space and carotid sheath. Place a drain in the retropharyngeal space through a separate stab. Approximate the longus colli and prevertebral fascia where possible, close the investing fascia over the carotid sheath, then platysma with absorbable suture and skin with a subcuticular suture. Assess for airway oedema before extubation — keep the patient intubated overnight or perform a tracheostomy if retraction was extensive.
Procedures Through This Approach
- Odontoid screw fixation — anterior single or double screw for a type II odontoid nonunion, preserving C1–C2 rotation.
- Anterior cervical corpectomy — C2 or C3 corpectomy with strut-graft or cage reconstruction.
- Smith–Robinson anterior cervical approach — the caudal extension for C3–C7 work.
- Anterior C1–C2 transarticular screw placement and anterior C1–C2 plating and fusion.
- Anterior debridement and grafting for upper cervical pyogenic or tuberculous osteomyelitis.
- Resection of anterior craniovertebral junction tumours (chordoma, metastasis).
- Basilar invagination decompression (odontoidectomy) and revision anterior surgery after failed transoral or posterior procedures.
Viva & Exam Focus
RETROPHARRETROPHAR — the exposure, step by step
DANGERDANGER — nerves at risk, layer by layer
Exam viva scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old presents with 8 months of neck pain after a motor-vehicle accident. CT shows a displaced type II odontoid fracture with a 4 mm anterior atlantodens interval and no posterior fusion mass. How would you approach this?”
“A 58-year-old with known renal cell carcinoma has progressive neck pain and dysphagia. MRI shows a large C2 body metastasis with anterior epidural compression and greater than 50 percent body destruction. How do you plan the surgery?”
“A 35-year-old with rheumatoid arthritis has progressive myelopathy; MRI shows basilar invagination with odontoid compression of the cervicomedullary junction, the odontoid lying 8 mm above the Chamberlain line. How do you proceed?”
Patient position
- Supine on a radiolucent table, head extended 10–15 degrees and rotated 30–40 degrees away
- Mayfield or Gardner–Wells for controlled positioning; shoulder roll
- C-arm for true lateral and open-mouth AP of C1–C2; endotracheal tube on the contralateral side
Marginal mandibular nerve
- Crosses the mandible 1–2 cm below the inferior border
- Ligate the retromandibular vein and facial vessels early; retract the nerve cephalad with the gland
- Injury causes ipsilateral lower-lip weakness; the commonest nerve injury (transient 10–15%)
Internervous plane
- Medial to the carotid sheath (vagus) and lateral to the visceral column (pharyngeal plexus)
- Truly internervous — no muscle divided
- Longus colli detached subperiosteally as the midline landmark; stay midline to protect the sympathetic chain
Deep nerves at risk
- Hypoglossal nerve (CN XII) at the hyoid (C3) — identify and mobilise laterally
- Superior laryngeal nerve — internal branch for sensation, external for cricothyroid; gentle pharyngeal retraction
- Injury patterns: tongue deviation, aspiration, Horner syndrome
Caudal extension
- Extend along the anterior border of the sternocleidomastoid
- Same plane reaches C3–C7 as a Smith–Robinson exposure
- No repositioning for combined upper and mid-cervical pathology
Airway and swallow
- Pharyngeal and laryngeal retraction causes oedema
- 5–15% risk of prolonged or repeat intubation
- Formal swallow assessment before oral intake; plan delayed extubation or tracheostomy in high-risk cases
References
Global practice. Upper cervical pathology is managed at tertiary spine centres worldwide, and the anterior retropharyngeal approach is recognised across contemporary practice as the standard extraoral route to the craniovertebral junction when a clean field is required. Where guidance converges
- Position
- Extraoral retropharyngeal route for anterior C1–C3 pathology when transoral is contraindicated; CT-based planning and lower-cranial-nerve monitoring emphasised
- Position
- Anterior odontoid screw fixation and C1–C2 plating via the retropharyngeal exposure are accepted; airway and swallow protocols mandatory
- Position
- Multidisciplinary upper cervical MDT; posterior stabilisation often precedes anterior decompression in unstable patients
Population evidence - Odontoid fractures are about 15 percent of all cervical spine fractures; nonunion after non-operative treatment ranges from 10 to 50 percent depending on fracture type and patient factors.
- Anterior odontoid screw fixation fuses in 85 to 95 percent of appropriately selected cases through this exposure.
- Infection after retropharyngeal surgery is consistently lower (1–4 percent) than after transoral surgery (10–20 percent). Consent (globally applicable). Discuss marginal mandibular nerve injury (transient 10–15 percent, permanent less than 3 percent), hypoglossal nerve injury (transient 5–10 percent), superior laryngeal nerve injury with voice change and aspiration (5–15 percent), dysphagia (20–40 percent transient), airway compromise needing re-intubation or tracheostomy (5–15 percent), infection (2–5 percent), nonunion (5–15 percent), and possible future revision or combined posterior stabilisation.
For the Operative Surgery station, describe the approach systematically: supine positioning with head extension and rotation, marginal mandibular nerve protection by vessel ligation and cephalad retraction, the internervous plane medial to the carotid sheath, identification of the hypoglossal and superior laryngeal nerves, and caudal extension into the Smith–Robinson approach. Know the indications for extraoral versus transoral routes and the airway considerations unique to this exposure.
The Anterior Retropharyngeal Approach to the Upper Cervical Spine
- Described the extraoral retropharyngeal route to C1–C3 as a safe alternative to transoral surgery
- Emphasised marginal mandibular nerve protection by facial vessel ligation and cephalad retraction
- Reported successful anterior decompression and fusion in 12 patients with low morbidity
- Established the technique as the preferred clean-field approach for upper cervical pathology
Anatomical aspects and technical note of a modified retropharyngeal approach and reconstruction of the anterior occipitocervical junction
- Detailed anatomical landmarks and technical modifications for retropharyngeal access to the anterior occipitocervical junction with reconstruction
Atlantodentoplasty using the anterior retropharyngeal approach for treating irreducible atlantoaxial dislocation with atlantodental bony obstruction: a retrospective study
- Retrospective series demonstrating anterior retropharyngeal atlantodentoplasty for irreducible atlantoaxial dislocation with bony obstruction
Transcervical, retropharyngeal odontoidectomy — anatomical considerations
- Anatomical study outlining critical considerations for safe transcervical retropharyngeal odontoidectomy