Volar exposure of the scaphoid waist for fractures, nonunion and humpback deformity correction
- The scaphoid's dominant blood supply enters dorsally and distally (retrograde to the proximal pole); the volar approach spares these vessels, making it the vascularity-sparing route for waist and distal pathology. The dorsal approach is reserved for proximal-pole fractures.
- The interval is FCR-based: open the FCR sheath and incise its floor. Staying radial to FCR protects the median nerve and its palmar cutaneous branch; the radial artery lies radial to the field and must be protected.
- The radioscaphocapitate (RSC) ligament crosses the scaphoid waist volarly; it is incised for exposure and MUST be repaired at closure — an unrepaired RSC ligament causes carpal (ulnar translation) instability.
- The volar route corrects humpback (flexion) deformity with a volar opening-wedge corticocancellous graft that restores scaphoid length and the radiolunate/intrascaphoid angles.
- Indicated for scaphoid waist and distal-pole fractures and nonunions, especially with volar resorption and flexion deformity; avoid in established SNAC-wrist arthritis (consider salvage) and a frankly avascular proximal pole (may need a vascularised graft, often dorsal).
When & Why
What it exposes. The volar (Russe) approach exposes the volar surface of the scaphoid through an FCR-based interval. It is the workhorse for scaphoid waist and distal-pole fractures and nonunions — especially those with volar resorption and humpback (flexion) deformity requiring a volar opening-wedge corticocancellous graft to restore length and correct dorsal intercalated segmental instability (DISI). Why volar (and not dorsal). The scaphoid's dominant blood supply enters dorsally (dorsal ridge vessels from the radial artery) and supplies the proximal pole retrogradely — which is why proximal-pole fractures are prone to avascular necrosis and slow union. A volar approach spares these dorsal vessels, so it is the vascularity-sparing choice for waist and distal pathology, and it gives direct access to the volar surface where resorption and flexion deformity occur, allowing length restoration and deformity correction. The dorsal approach is preferred for proximal-pole fractures and nonunions and for many percutaneous or arthroscopic central-screw placements, where it gives a straighter central axis to the proximal pole.
- Volar (Russe)
- Waist and distal-pole; nonunion with humpback deformity
- Dorsal
- Proximal-pole fractures/nonunion; central percutaneous screw
- Volar (Russe)
- Spares the dorsal (retrograde) vessels
- Dorsal
- Risks the dorsal ridge vessels but accesses the proximal pole directly
- Volar (Russe)
- Excellent — volar opening-wedge graft corrects flexion/DISI
- Dorsal
- Limited for humpback correction
- Volar (Russe)
- Radial artery, palmar cutaneous branch, RSC ligament
- Dorsal
- Dorsal ridge vessels, EPL, extensor tendons
- Volar (Russe)
- Volar entry at the tubercle — good for the waist
- Dorsal
- Dorsal entry — straight central axis to the proximal pole
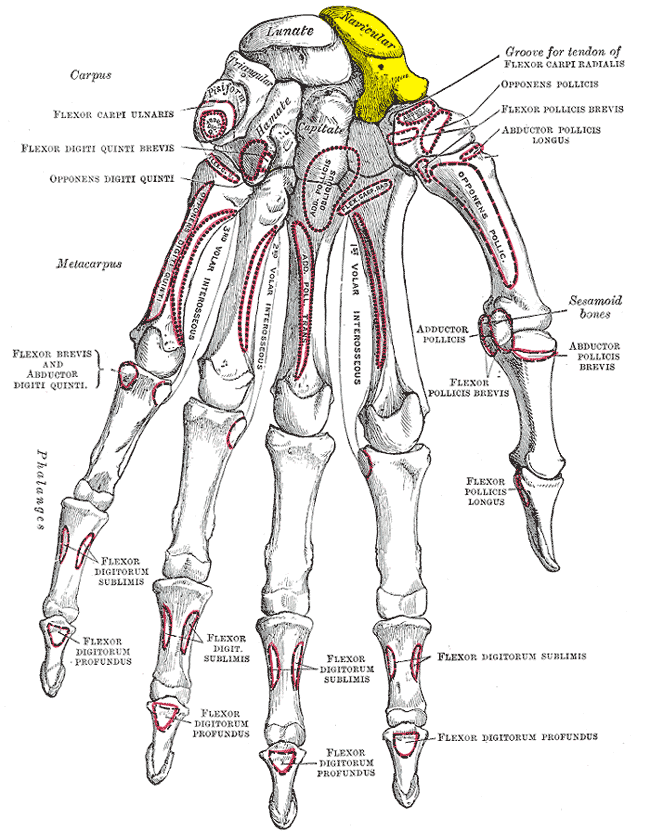
Position & landmarks. Supine, arm on a hand table, wrist extended over a bolster; upper-arm tourniquet and image intensifier available, with the wrist radially or ulnarly deviated to open the scaphotrapezial region. Landmarks are the flexor carpi radialis (FCR) tendon, the scaphoid tubercle (palpable at the radial wrist crease, accentuated by radial deviation) and the radial styloid.
Established SNAC-wrist arthritis warrants salvage (e.g. salvage procedure) rather than reconstruction through this exposure; a frankly avascular proximal pole may require a vascularised graft, which is often placed dorsally. The need to securely repair the radioscaphocapitate ligament is non-negotiable and is covered in the exposure below.
The Exposure
Work down through the layers along the FCR sheath — protecting the radial artery and the palmar cutaneous branch of the median nerve — then incise the sheath floor and the radioscaphocapitate ligament to reach the volar scaphoid waist.

Exposure sequence
- A curved or zig-zag incision over the volar-radial wrist, centred on FCR and extending distally toward the scaphoid tubercle and the scaphotrapezial (STT) region. The classic Russe uses this line; the modern extended FCR/Henry-based variant simply follows FCR.
- Open the FCR sheath. Identify, protect and retract the radial artery, which lies just radial to FCR at the wrist; a small superficial palmar branch may need deliberate ligation.
- Keep the dissection radial to FCR to protect the median nerve and especially its palmar cutaneous branch, which arises about 5 cm proximal to the wrist crease and runs on the radial side of the median nerve (ulnar side of FCR). Injury here causes a painful neuroma over the thenar base.
- Incise the floor of the FCR sheath to reach the volar wrist capsule.
- Avoid stripping volar attachments more than necessary and preserve the STT joint distally.
- Perform a capsulotomy and identify the radioscaphocapitate (RSC) ligament crossing the scaphoid waist volarly.
- Incise it to expose the volar waist, preserving a cuff or performing a step-cut so it can be securely repaired at closure.
- For nonunion: debride the nonunion to bleeding bone, restore length and correct the humpback (flexion) deformity by opening the volar gap, then insert a volar corticocancellous/cancellous graft (e.g. from the distal radius or iliac crest).
- Stabilise with a headless compression screw (volar entry at or near the scaphoid tubercle) or K-wires; confirm length, alignment (radiolunate/intrascaphoid angles) and screw position on fluoroscopy.
- Securely repair the RSC ligament and the volar capsule — essential to prevent carpal/ulnar translation instability.
- Repair the FCR sheath if needed, close subcutaneous tissue and skin, and immobilise in a thumb-spica cast or splint.
- Document radial artery integrity and median/palmar cutaneous nerve function.
The radioscaphocapitate ligament is divided to reach the scaphoid waist and MUST be repaired at closure. An unrepaired RSC ligament is a recognised cause of post-operative carpal (ulnar translation) instability — a classic viva point. Likewise, keep the dissection radial to FCR to protect the radial artery and the palmar cutaneous branch of the median nerve.
The volar surface is exactly where fracture resorption and the flexion (humpback) collapse occur, so opening the volar gap and inserting a trapezoidal/wedge corticocancellous graft restores scaphoid length and corrects the DISI pattern — something the dorsal route cannot do well. This is the single best reason to choose volar for a deformed waist nonunion.
Dangers & Extensions
Structures at risk, by location
- Where it is at risk
- Just radial to FCR at the wrist
- Protection strategy
- Identify, protect and retract; ligate a small superficial palmar branch deliberately
- Where it is at risk
- Ulnar side of FCR (about 5 cm above the crease)
- Protection strategy
- Keep dissection radial to FCR; avoid ulnar wandering
- Where it is at risk
- Crosses the scaphoid waist (incised for access)
- Protection strategy
- Incise with a cuff or step-cut and REPAIR securely at closure
- Where it is at risk
- Dorsal ridge vessels (spared by the volar route)
- Protection strategy
- Avoid dorsal dissection; use minimal volar stripping
- Where it is at risk
- Distal extent of exposure
- Protection strategy
- Preserve the scaphotrapezial joint; avoid unnecessary styloid disruption
Extensile options. The incision follows FCR, so it extends proximally along the radial border of FCR to reach the volar radial carpus and control the radial artery, and distally toward the scaphotrapezial region for concurrent STT work — taking care to preserve the STT joint and avoid unnecessary radial styloid disruption. Closure. The defining step is secure repair of the radioscaphocapitate ligament and the volar capsule (using the preserved cuff or step-cut), followed by repair of the FCR sheath if needed, layered skin closure, and immobilisation in a thumb-spica cast or splint. Confirm and document radial artery integrity and median/palmar cutaneous nerve function before discharge.
Procedures Through This Approach
- Scaphoid fracture fixation — open reduction and headless compression screw fixation of waist and distal-pole fractures via the volar exposure.
- Scaphoid nonunion bone grafting — volar opening-wedge corticocancellous or cancellous grafting (distal radius or iliac crest) with correction of humpback/DISI deformity.
- Volar percutaneous screw fixation — for selected waist delayed and nonunions without significant deformity or proximal-pole avascular necrosis.
- Concurrent volar carpal procedures that share the FCR-based interval.
Viva & Exam Focus
RARERARE — volar scaphoid safety
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You plan to graft a scaphoid waist nonunion with a humpback deformity. Which approach and why, and what is your interval?”
“During the volar approach, which structures must you protect, and what happens if the radioscaphocapitate ligament is not repaired?”
Plane & anatomy
- FCR-based interval; floor of the FCR sheath is incised
- Radial to FCR protects the median nerve and palmar cutaneous branch
- Radial artery lies just radial to FCR
- Radioscaphocapitate ligament crosses the waist and must be repaired
Indications
- Waist and distal-pole fractures
- Waist nonunion with humpback/DISI deformity
- Volar opening-wedge corticocancellous grafting
Dangers
- Radial artery and palmar cutaneous branch of the median nerve
- Unrepaired RSC ligament causes ulnar translation instability
- Dorsal ridge vessels are spared by staying volar
Evidence
- Volar cancellous grafting: 28 of 28 united (Yasuda 2007)
- Volar percutaneous screw: about 92 percent union in nonunion (Gurger 2018)
- Volar screw for delayed union: all united, ROM about 94 percent (Kim 2009)
References
Volar (Russe-type) cancellous grafting for scaphoid nonunion — high union
- Volar approach with curettage and biconcave cancellous bone grafting from the distal radius plus pin fixation for scaphoid nonunion (Russe classification: 6 distal, 19 middle, 3 proximal third).
- Bony union achieved in ALL 28 cases; post-activity pain resolved in every patient.
- Allows concurrent correction of carpal instability without an STT arthrotomy; mean extension 79 degrees and flexion 77 degrees postoperatively.
Volar percutaneous screw fixation for scaphoid nonunion
- Volar percutaneous headless cannulated screw fixation for scaphoid nonunion (waist and proximal pole) under fluoroscopic guidance.
- Union achieved in 11 of 12 patients (91.6 percent); mean time to union 15.5 weeks.
- Modified Mayo Wrist Score excellent in 8 and good in 3 — a minimally invasive volar option in selected nonunions without significant deformity.
Volar percutaneous screw fixation for scaphoid waist delayed union
- Volar percutaneous cannulated screw fixation for scaphoid waist delayed union (without instability, deformity or proximal-pole AVN).
- All fractures united; at 12 months flexion/extension arcs were 94 percent/93 percent and grip strength 92 percent of the uninjured side.
- Confirms the volar route as a reliable, low-morbidity option when there is no significant deformity to correct.
Surgical exposures and the scaphoid blood supply — standard references
The FCR-based interval, the dorsal/retrograde scaphoid blood supply, the radioscaphocapitate ligament and the volar humpback-correction principle reflect standard, well-established surgical-anatomy teaching. PubMed attribution for the three cited series: Yasuda et al. (DOI), Gurger et al. (DOI) and Kim et al. (DOI).