Additive Manufacturing in Orthopaedic Surgery
Anatomical Models: Pre-operative planning, education
Patient-Specific Instruments: Cutting guides, drill guides
Custom Implants: Tumour reconstruction, revision arthroplasty
Key: 3D printing transforms 2D imaging into tangible surgical tools
- CT provides best data for 3D printing (bone segmentation)
- Thin-slice (less than 1mm) CT required for accuracy
- Patient-specific instruments improve implant positioning
- Custom implants for complex reconstruction
- Regulatory requirements for implantable devices
- “DICOM to STL conversion is the key processing step
- “Segmentation quality determines print accuracy
- “Anatomical models reduce operative time in complex cases
- “PSI can improve component alignment in arthroplasty
3D printing is an emerging topic with increasing exam relevance. Understand the workflow from imaging to print, key applications (models, PSI, custom implants), and imaging requirements (thin-slice CT). Know the advantages and limitations of this technology.
PRINTPRINT Framework
Hook:Good orthopaedic printing starts with the imaging dataset, not the printer.
Overview

Three-dimensional printing is a downstream use of imaging, not a separate imaging modality. The quality of the printed model depends first on acquisition, then segmentation, then the clinical relevance of the model that is produced.
For orthopaedics, the strongest indications are complex articular trauma, deformity planning, implant templating, and patient-specific education where spatial understanding genuinely changes decision-making.
PRINTPRINT Workflow
Hook:Remember the 5 stages from image to operating theatre
STERILESTERILE Requirements
Hook:STERILE workflow ensures safe clinical application
Workflow Overview


- Process
- CT/MRI scan
- Key Considerations
- Thin slices (less than 1mm), minimal artefact
- Process
- Send to processing software
- Key Considerations
- Anonymisation, secure transfer
- Process
- Separate structures of interest
- Key Considerations
- Quality determines accuracy
- Process
- Generate surface mesh
- Key Considerations
- STL file format
- Process
- Add guides, cutting slots
- Key Considerations
- Engineering input for instruments
- Process
- Additive manufacturing
- Key Considerations
- Material selection for purpose
- Process
- Cleaning, sterilisation
- Key Considerations
- Regulatory compliance for implants
Systematic Approach to 3D Printing
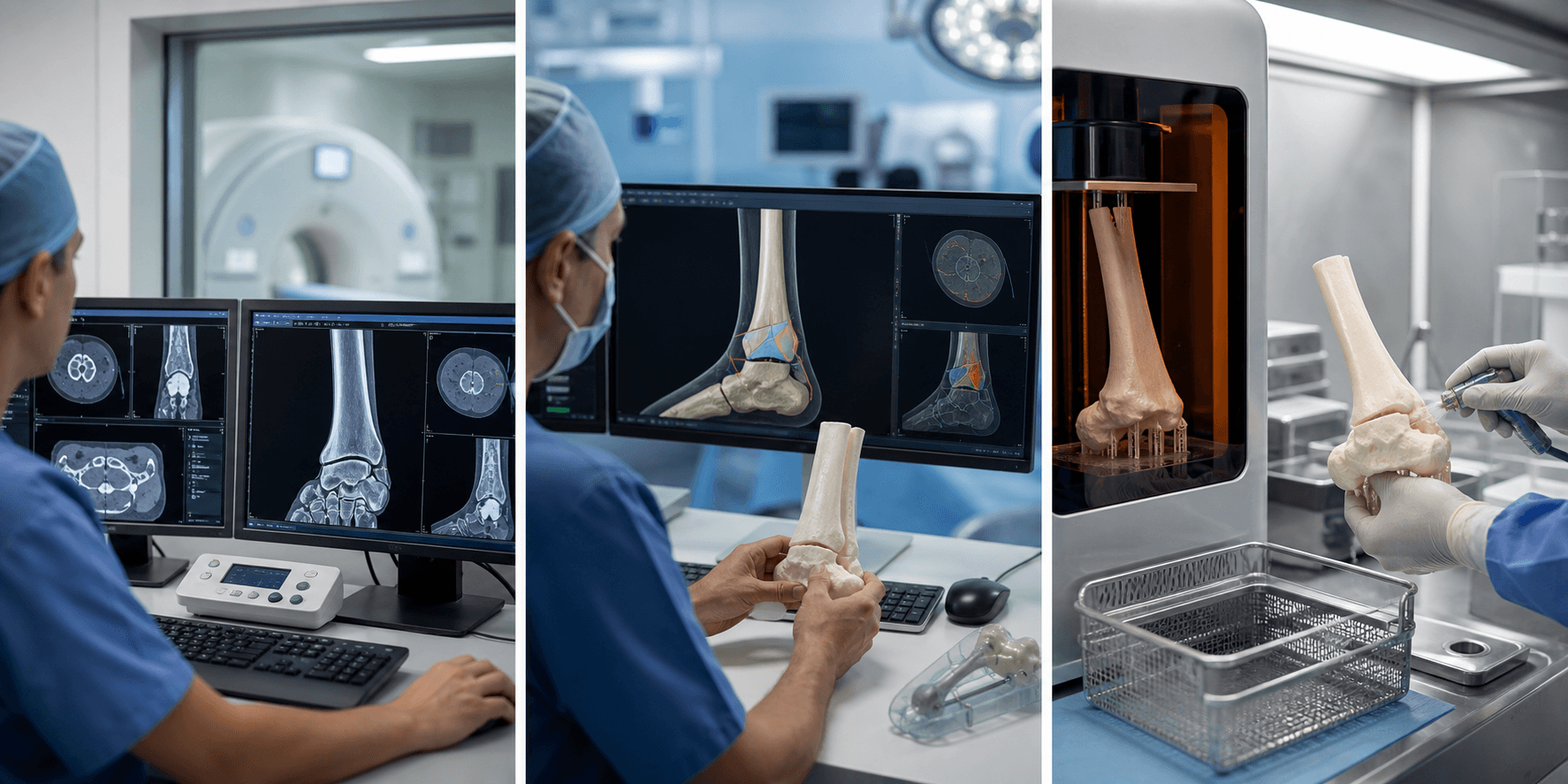
The Five-Stage Workflow
Stage 1: Imaging Acquisition
- Thin-slice CT (less than 1mm) provides optimal data
- MRI for soft tissue assessment in complex cases
- DICOM format required for processing
Stage 2: Segmentation and Modelling
- DICOM to STL conversion
- Threshold-based bone segmentation
- Manual refinement for accuracy
- Quality control checks
Stage 3: Design and Planning
- Virtual surgical planning
- Guide design (cutting planes, drill trajectories)
- Implant templating
- Sterilisation considerations
Stage 4: Manufacturing
- Material selection (PLA, nylon, titanium)
- Printer calibration and quality control
- Surface finishing for theatre use
- Sterilisation validation
Stage 5: Clinical Application
- Pre-operative team briefing with model
- Intra-operative guide placement
- Post-operative validation
- Sterilisation: Gamma irradiation or autoclave compatible materials
- Accuracy: Less than 1mm deviation for implantable devices
- Documentation: Full traceability from imaging to implant

Imaging Requirements

- Recommendation
- CT preferred for bone
- Rationale
- Superior bone-soft tissue contrast
- Recommendation
- Less than 1mm (ideally 0.5-0.625mm)
- Rationale
- Reduces stair-stepping artefact
- Recommendation
- Include relevant anatomy
- Rationale
- Sufficient margins for planning
- Recommendation
- MARS protocol if hardware present
- Rationale
- Improves segmentation accuracy
- Recommendation
- Usually unnecessary for bone
- Rationale
- May help tumour delineation

Clinical Applications

- Benefit
- 3D visualisation of pathology
- Examples
- Complex fractures, tumour resection
- Benefit
- Pre-bend plates, trial implants
- Examples
- Pelvic fractures, spine deformity
- Benefit
- Tangible explanation of surgery
- Examples
- Joint replacement, deformity correction
- Benefit
- Practice complex procedures
- Examples
- Resident education, rare procedures
- Benefit
- Anatomical guide in OR
- Examples
- Tumour margins, fracture reduction


Printing Technologies

- Mechanism
- Extruded thermoplastic
- Applications
- Anatomical models, low-cost
- Mechanism
- UV-cured resin
- Applications
- High detail models, surgical guides
- Mechanism
- Laser-fused powder
- Applications
- Durable guides, nylon models
- Mechanism
- Metal powder laser fusion
- Applications
- Titanium implants
- Mechanism
- Metal powder electron beam
- Applications
- Porous metal implants
Quality Assurance

- Requirement
- Less than 1mm deviation
- Verification
- Calliper measurement, CT comparison
- Requirement
- Matches patient anatomy
- Verification
- Overlay on source CT
- Requirement
- Appropriate for OR use
- Verification
- Validated sterilisation process
- Requirement
- Non-toxic, implant grade
- Verification
- Material certification
- Requirement
- Withstands intended use
- Verification
- Mechanical testing
Limitations

- Explanation
- Days to weeks for complex prints
- Mitigation
- Early planning, in-house printing
- Explanation
- Equipment, materials, expertise
- Mitigation
- Case selection, shared services
- Explanation
- Metal hardware degrades segmentation
- Mitigation
- MARS protocols, manual editing
- Explanation
- Especially for custom implants
- Mitigation
- Partner with approved manufacturers
- Explanation
- Segmentation and design skills
- Mitigation
- Training, dedicated staff
Choosing the Right Technology
Examiners often probe whether a candidate can select the appropriate technology rather than reflexively reaching for a 3D print. The table below contrasts 3D printing with the alternatives it competes with for the same clinical problems.
- 3D-printed model/guide
- Yes
- On-screen virtual planning
- No
- Intra-op CT navigation
- No
- Robotic assistance
- No
- 3D-printed model/guide
- Yes
- On-screen virtual planning
- No
- Intra-op CT navigation
- No
- Robotic assistance
- No
- 3D-printed model/guide
- Low (fixed at print)
- On-screen virtual planning
- n/a (planning only)
- Intra-op CT navigation
- High
- Robotic assistance
- High
- 3D-printed model/guide
- No
- On-screen virtual planning
- No
- Intra-op CT navigation
- Yes
- Robotic assistance
- Yes
- 3D-printed model/guide
- Days to weeks
- On-screen virtual planning
- Hours
- Intra-op CT navigation
- None
- Robotic assistance
- None
- 3D-printed model/guide
- Low to moderate
- On-screen virtual planning
- Low
- Intra-op CT navigation
- High
- Robotic assistance
- Very high
- 3D-printed model/guide
- Complex articular/pelvic trauma, deformity, tumour
- On-screen virtual planning
- Rapid templating, teaching
- Intra-op CT navigation
- Pedicle screws, tumour margins
- Robotic assistance
- Arthroplasty alignment
Guidelines, Registries & Global Practice
- Framework
- Guidance on technical considerations for additively manufactured devices; point-of-care framework
- Practical implication
- Anatomical models and guides have clear pathways; patient-matched implants need validated processes
- Framework
- Custom-made device provisions under MDR 2017/745; notified-body oversight for higher-risk implants
- Practical implication
- Documentation and conformity assessment scale with device risk class
- Framework
- Quality management system for medical devices
- Practical implication
- Required for any site manufacturing implantable or patient-contacting printed devices
- Framework
- Education and consensus on computer-assisted and patient-specific planning
- Practical implication
- Endorse case selection over routine use; emphasise verification against source imaging
- Framework
- Appropriateness and quality criteria for clinical 3D printing in radiology
- Practical implication
- Standardise indications, segmentation QA, and reporting for point-of-care labs
The Fourth Application: Scaffolds and Bioprinting
The anchor review (Wong et al, cited below) names four core orthopaedic uses of additive manufacturing, but the body develops only three - models, patient-specific instruments and custom implants. The fourth is bone/cartilage tissue engineering, where 3D printing is the fabrication route:
- Printed scaffolds. A biodegradable scaffold with a controlled porous architecture is printed from polymers (such as PCL or PLGA), ceramics (such as tricalcium phosphate or hydroxyapatite) or bioactive glass, then seeded with cells (e.g. mesenchymal stem cells) and/or growth factors to regenerate bone or cartilage.
- Bioprinting goes further, depositing living cells suspended in a bio-ink (a hydrogel such as alginate, gelatin or collagen) layer-by-layer to build a living construct.
- This remains largely experimental / pre-clinical: the barriers are vascularising large constructs, maintaining cell viability, achieving load-bearing strength and gaining regulatory approval. The biology of tissue engineering is covered in its own topic; here the point is that 3D printing is the manufacturing method that makes patient-specific scaffolds possible.
Q: Beyond models, PSI and custom implants, what is the fourth core application of 3D printing in orthopaedics?
A: Bone/cartilage tissue engineering - printing biodegradable scaffolds (PCL/PLGA polymers, tricalcium-phosphate/hydroxyapatite ceramics, bioactive glass) with a porous architecture seeded with cells (MSCs) and/or growth factors, and bioprinting (depositing living cells in a hydrogel bio-ink layer-by-layer). It is still largely experimental - barriers are vascularisation, cell viability, load-bearing strength and regulation.
Why a Printed Porous Lattice Beats a Solid Implant
The topic notes that 'porous titanium structures can be designed to match bone modulus and promote osseointegration' but never explains how or why - and the Wong review (below) states printed implants can carry scaffold lattices that reduce stiffness and favour osteointegration.
- Design freedom. Metal additive manufacturing (laser sintering or electron-beam melting) can build a porous or trabecular lattice inside a titanium implant that a solid cast or machined implant cannot - and the porosity can be varied regionally within one part.
- Reducing stress shielding. A lattice lowers the implant's effective elastic modulus toward that of bone (solid titanium is around 110 GPa versus roughly 15 to 20 GPa for cortical bone), so more load is transferred to the surrounding bone and less is shielded - reducing peri-implant bone resorption.
- Promoting osseointegration. The interconnected pores allow bone to grow into the implant (optimal pore size roughly 300-700 micrometres), giving durable biological fixation - the same principle as a trabecular-metal ingrowth surface.
Q: Why is a 3D-printed porous titanium lattice better than a solid implant?
A: Additive manufacturing can build a porous/trabecular lattice a solid cast implant cannot, giving two advantages: (1) it lowers the implant's effective elastic modulus toward bone (solid titanium around 110 GPa versus cortical bone roughly 15-20 GPa) - less stress shielding and bone resorption; and (2) the interconnected pores (optimal roughly 300-700 micrometres) allow bone ingrowth - durable osseointegration, like a trabecular-metal surface. Porosity can be varied regionally within one part.
Imaging Atlas

Controversies and Areas of Uncertainty
- Current position
- No clinically relevant benefit in routine primary TKA (Level I meta-analysis)
- Uncertainty
- May still help in extra-articular deformity or retained hardware where canals cannot be referenced
- Current position
- Reduce operative time, blood loss, fluoroscopy in acetabular fractures
- Uncertainty
- Mostly small single-centre series; few multicentre RCTs; outcome (not process) benefit less proven
- Current position
- Models/guides increasingly printed in-house
- Uncertainty
- Implants almost always require certified manufacturers; in-hospital QMS burden is high
- Current position
- Allow reconstruction otherwise impossible
- Uncertainty
- Long-term survivorship data immature; failure modes and registry capture incomplete
- Current position
- Sub-millimetre dimensional fidelity achievable
- Uncertainty
- No universal validation/verification standard; accuracy degrades with metal artefact and poor segmentation
The single highest-yield controversy: PSI does NOT improve outcomes in routine total knee arthroplasty. Quote the Level I meta-analysis and reserve PSI/3D guides for cases where conventional referencing fails (severe extra-articular deformity, retained hardware, tumour margins).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You are planning surgery for a complex acetabular fracture. How might 3D printing assist your pre-operative planning?”
“A patient requires resection of a pelvic chondrosarcoma with reconstruction. How can 3D printing technology assist?”
“You are considering patient-specific instruments (PSI) for a complex total knee replacement in a patient with severe extra-articular deformity from a malunited tibial fracture.”
Workflow
- CT acquisition (less than 1mm slices)
- DICOM to segmentation software
- Generate STL file
- Print and post-process
- Sterilise if for OR use
Applications
- Anatomical models (planning, education)
- PSI (cutting guides, drill guides)
- Custom implants (tumour, revision)
- Pre-contoured plates
Imaging Requirements
- CT preferred for bone
- Slice thickness less than 1mm
- MARS protocol if metal present
- Include relevant anatomy margins
Limitations
- Time (days to weeks)
- Cost (equipment, materials)
- Regulatory for implants
- Requires expertise
Evidence Base

Landmark and Supporting Studies
Key Points
- Trauma planning: Comparative evidence supports reduced operative time, blood loss, and fluoroscopy with pre-operative 3D models in complex acetabular fractures.
- Deformity guides: Meta-analytic Level I evidence shows 3D-printed drill guides improve pedicle screw accuracy and lower radiation exposure.
- PSI in routine TKA: High-quality Level I evidence shows no clinically relevant outcome benefit — value is confined to selected, atypical anatomy.
- Custom implants: Geometry and stiffness matching are real advantages, offset by cost, multi-week lead time, and loss of intraoperative flexibility.