FGFR3 Mutation and Short Stature
- FGFR3: Gain-of-function mutation.
- Foramen Magnum: Stenosis can cause sudden death in infancy.
- Spinal Stenosis: Symptomatic in 20-30% of adults.
- Genu Varum: Common, may need correction.
- Thoracolumbar Kyphosis: Resolves in most.
- “FGFR3 gain-of-function
- “Foramen magnum stenosis in infancy
- “Spinal stenosis in adults
- “Rhizomelic shortening
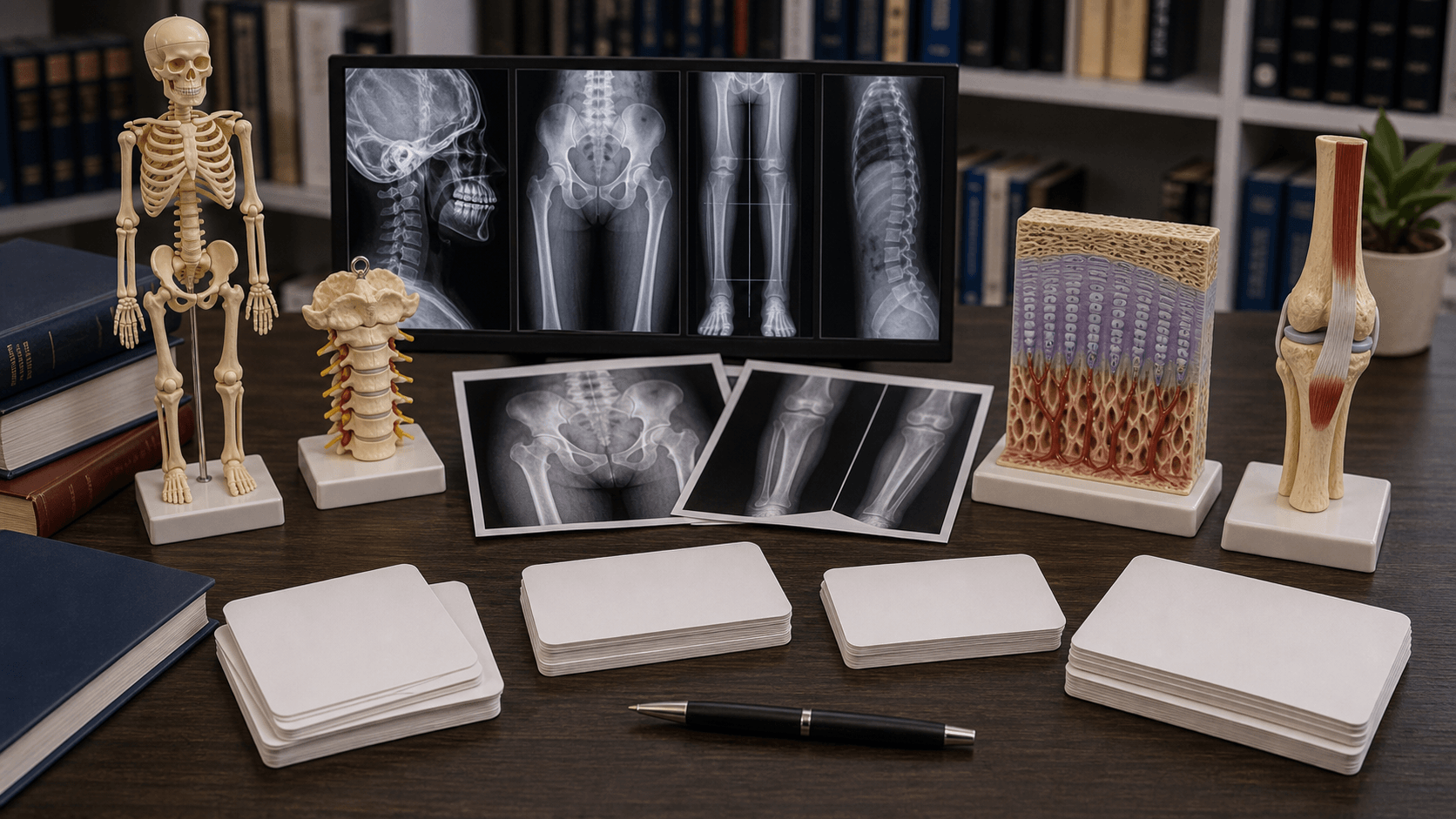
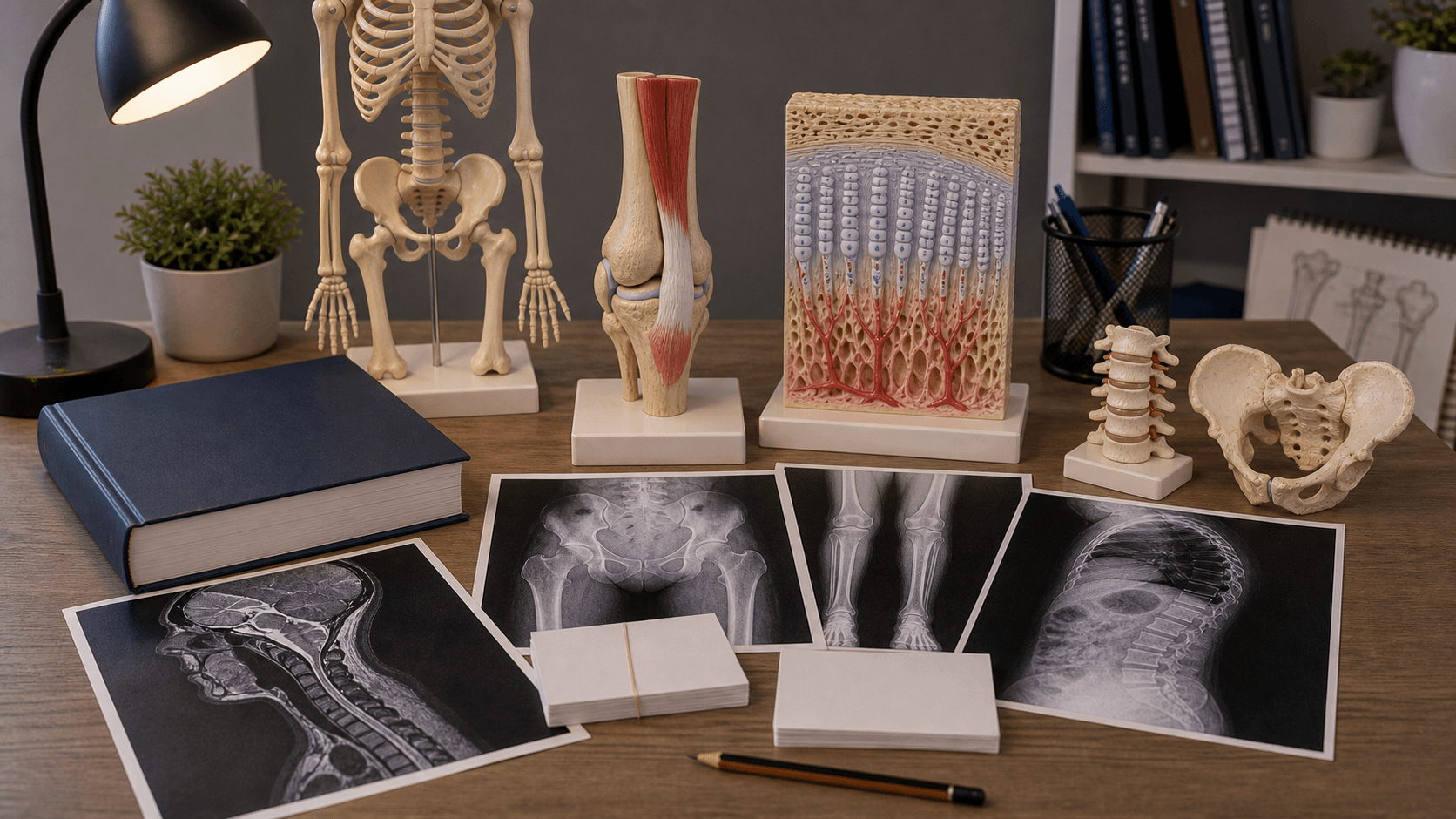
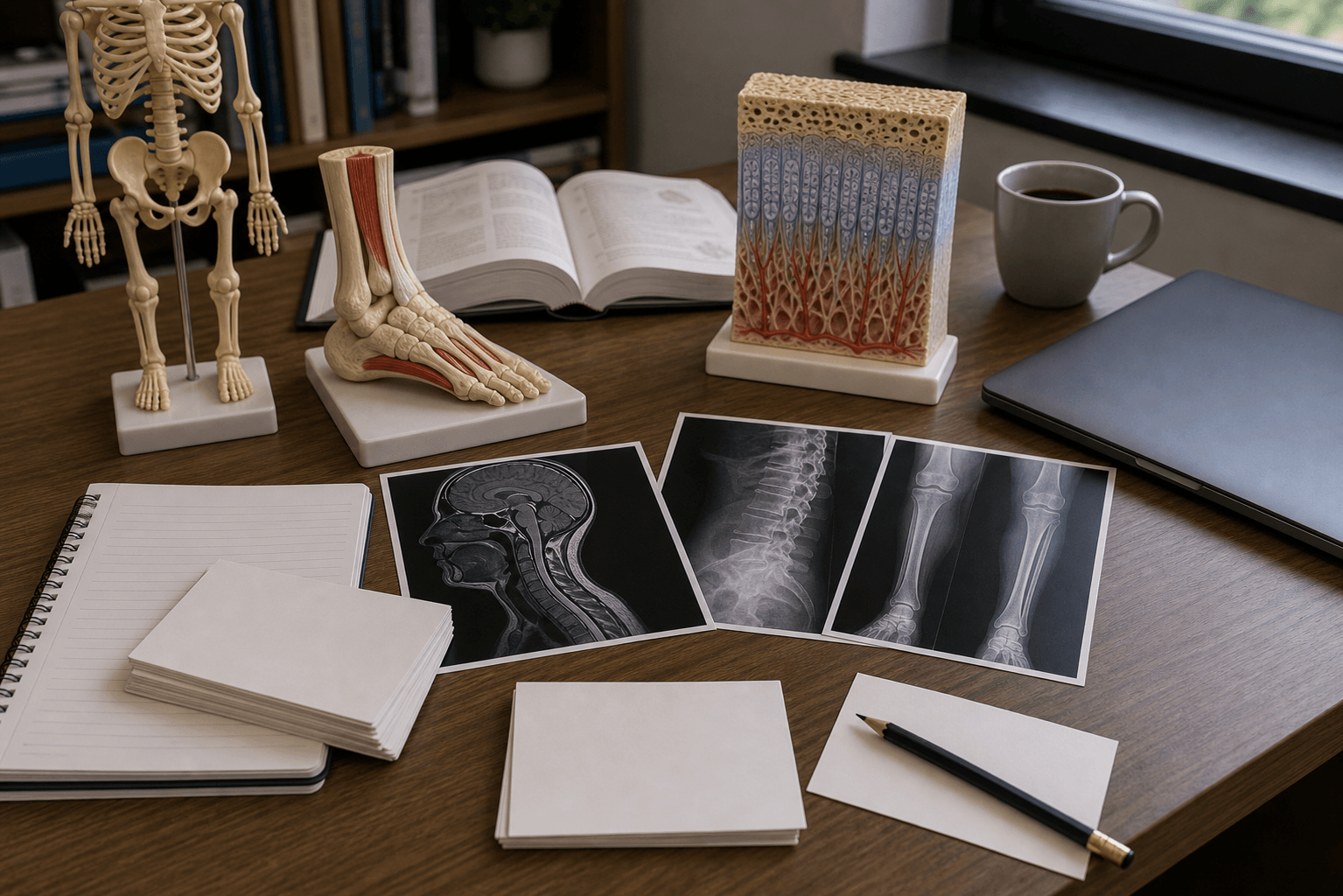
Clinical Imaging
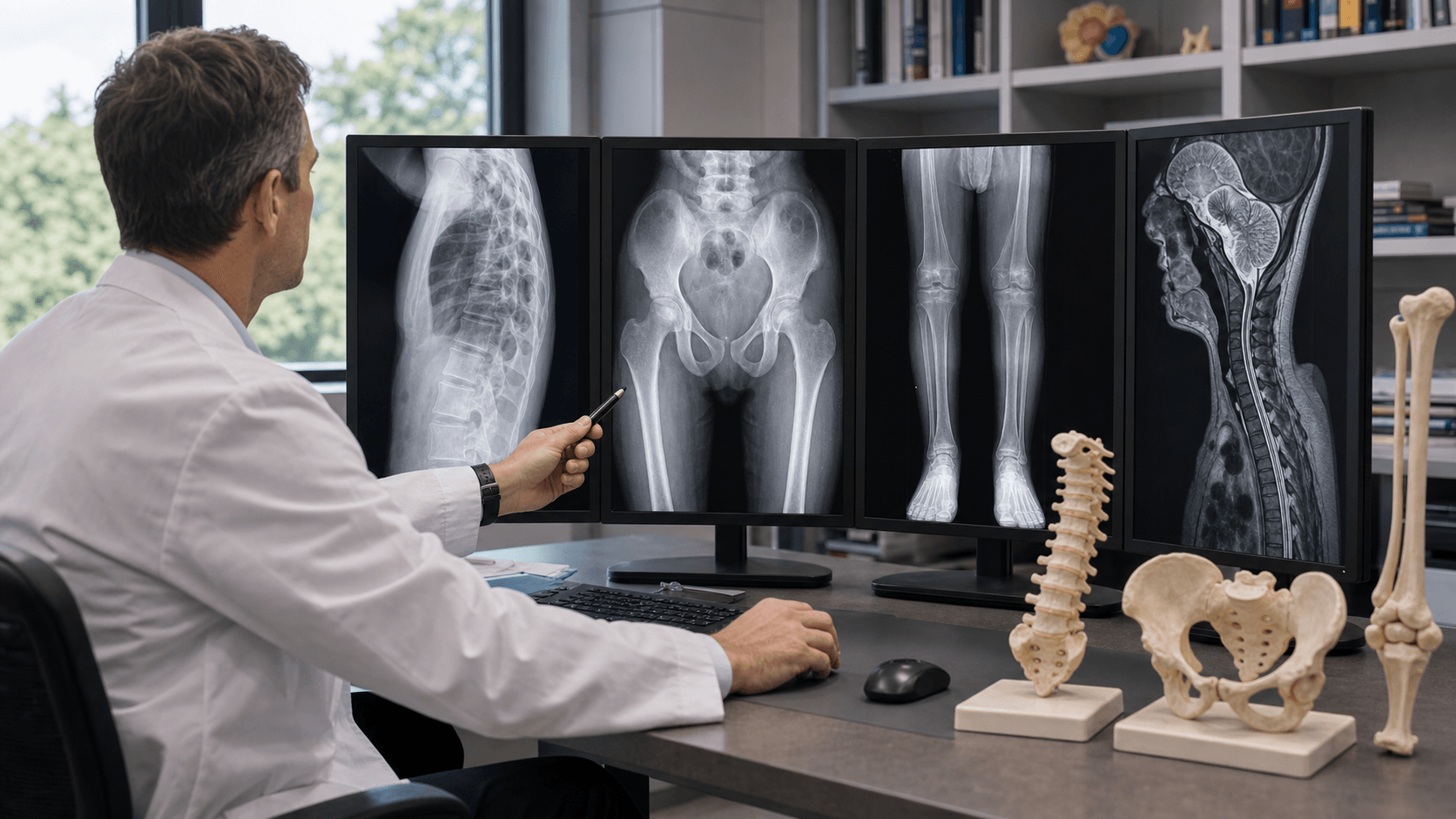
Imaging Atlas
Foramen Magnum Stenosis causes cervicomedullary compression. Can lead to central apnea and sudden infant death. Mortality is significantly higher in infancy.
Mandatory Screening: Monitor for apnea, hypotonia, feeding issues. MRI Craniocervical Junction at birth/neonatal period is essential.
| Feature | Description | Management |
|---|---|---|
| Infancy - apnea, sudden death | MRI, decompression if symptomatic | |
| Adults - claudication, neurological | Wide laminectomy | |
| Bowed legs | Osteotomy if symptomatic | |
| Infancy - usually resolves | Most observation |
FFRSAchondroplasia Features
Hook:FFRS - FGFR3, Foramen, Rhizomelic, Stenosis.
MFTLClinical Appearance
Hook:MFTL - Macro, Frontal, Trident, Lordosis.
ICASpinal Issues by Age
Hook:ICA - Infancy (foramen), Childhood (kyphosis), Adult (lumbar).
WIDESurgical Decompression
Hook:Go WIDE or go home - inadequate decompression is the main surgical pitfall!
Overview/Epidemiology
Achondroplasia is the most common skeletal dysplasia.
- Genetics: Autosomal dominant. FGFR3 (Fibroblast Growth Factor Receptor 3) mutation.
- Incidence: 1 in 20,000.
- New Mutations: 80% are new mutations (unaffected parents).
- Pathophysiology: FGFR3 is a negative regulator of bone growth. Gain-of-function mutation → reduced endochondral ossification.
Pathophysiology and Mechanisms
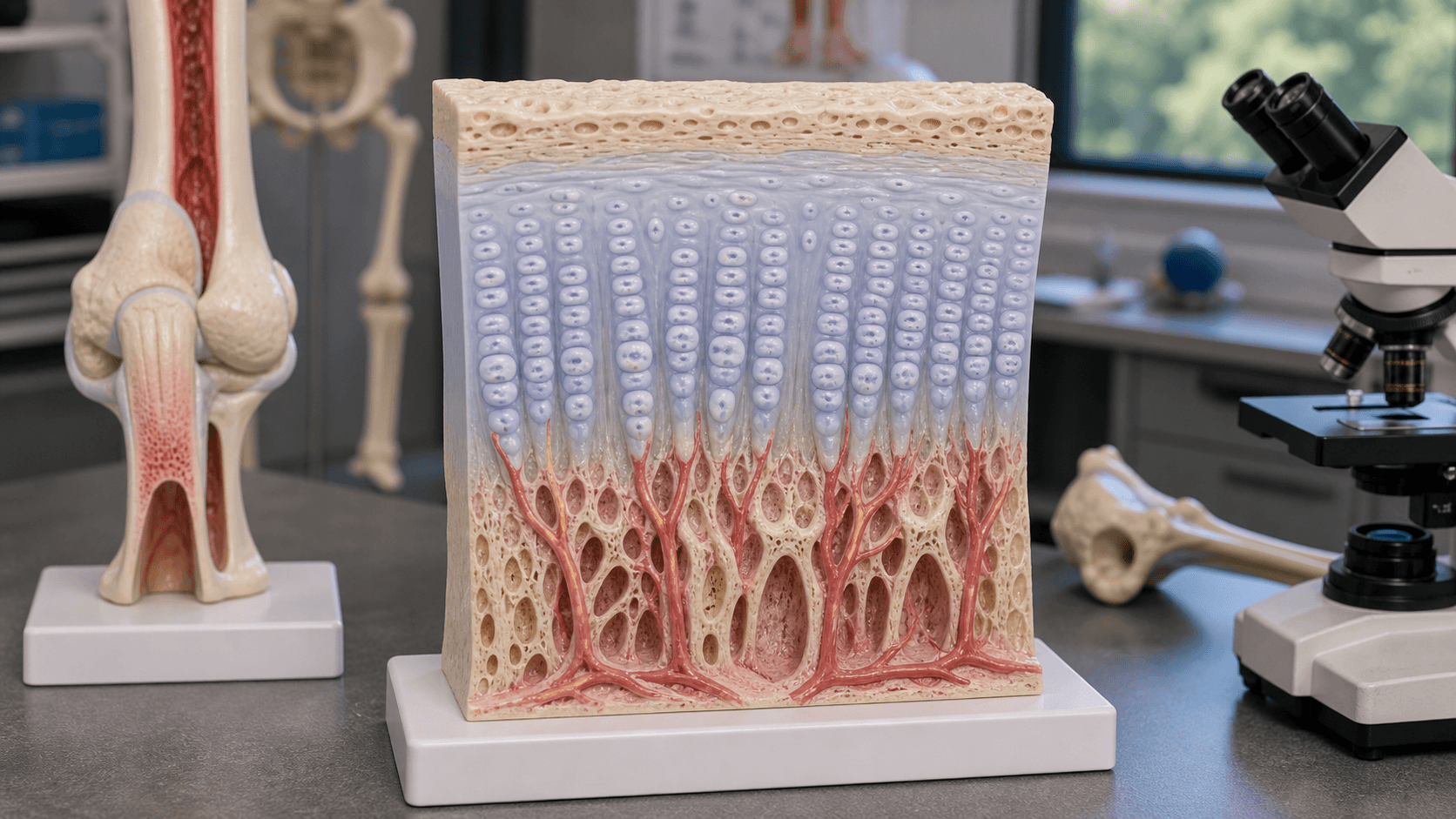
Endochondral Ossification Defect
- FGFR3 normally inhibits bone growth at the growth plate.
- Gain-of-function → excessive inhibition → short bones.
- Affects endochondral bones (limbs, skull base) more than intramembranous.
Why Spinal Stenosis Occurs
- Short pedicles → narrow spinal canal.
- Progressive symptoms in adulthood.
Classification Systems
Clinical Features
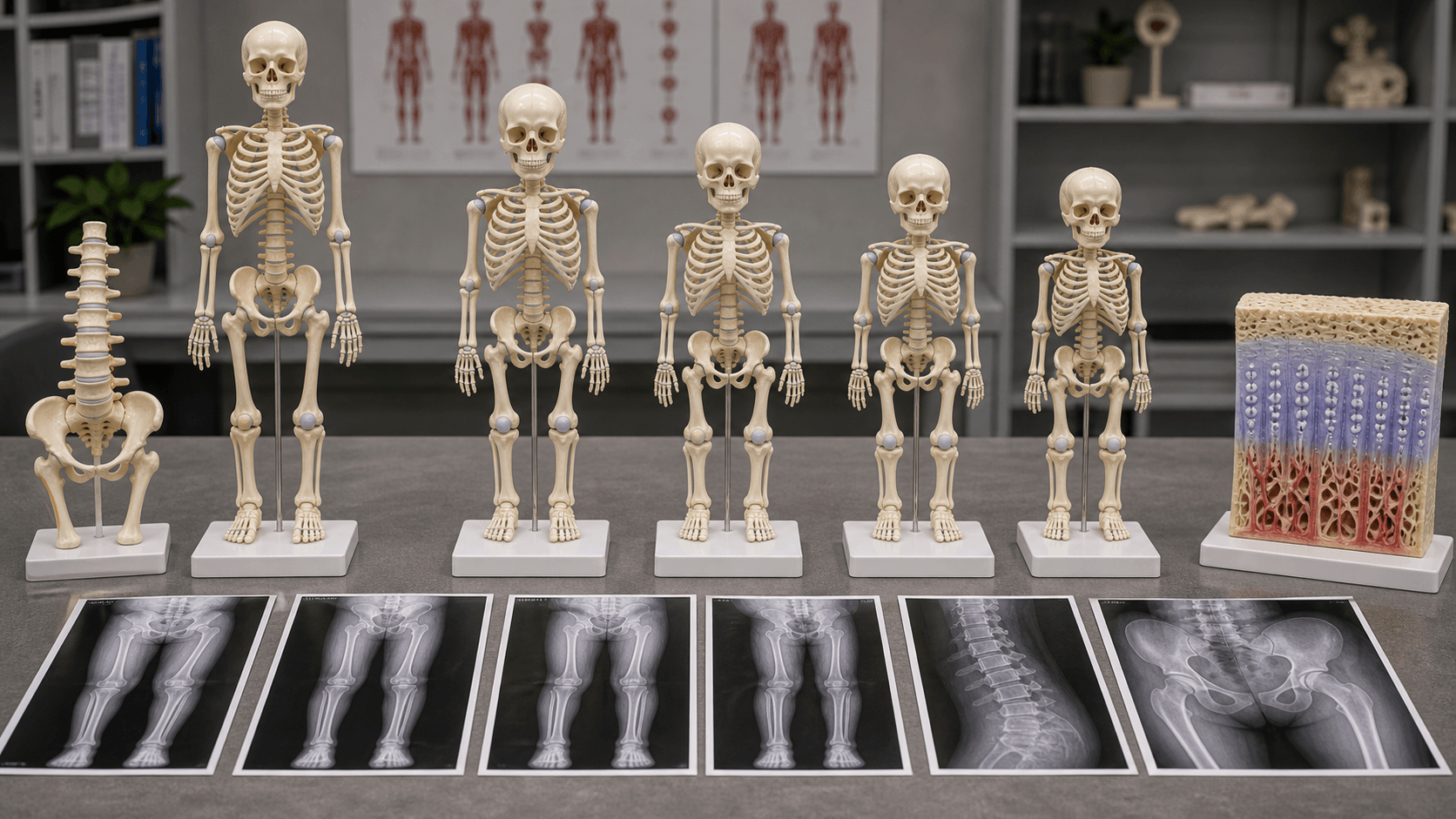
- Short Stature: Adult height 120-130cm.
- Rhizomelic Shortening: Proximal limbs (humeri, femora) shorter than distal.
- Macrocephaly: Large head with frontal bossing.
- Midface Hypoplasia: Flat nasal bridge.
- Trident Hands: Short fingers, can't approximate in extension.
- Lumbar Lordosis: Hyperlordosis.
Clinical Assessment
History:
- Developmental milestones.
- Apnea, breathing issues (foramen magnum).
- Back pain, leg pain, claudication (stenosis).
- Leg deformity concerns.
Physical Exam:
- General: Short stature, rhizomelic limbs.
- Head: Macrocephaly, frontal bossing, midface hypoplasia.
- Spine: Lordosis, kyphosis assessment.
- Legs: Genu varum, mechanical axis.
- Neurological: Lower limb reflexes, power (stenosis symptoms).
Investigations
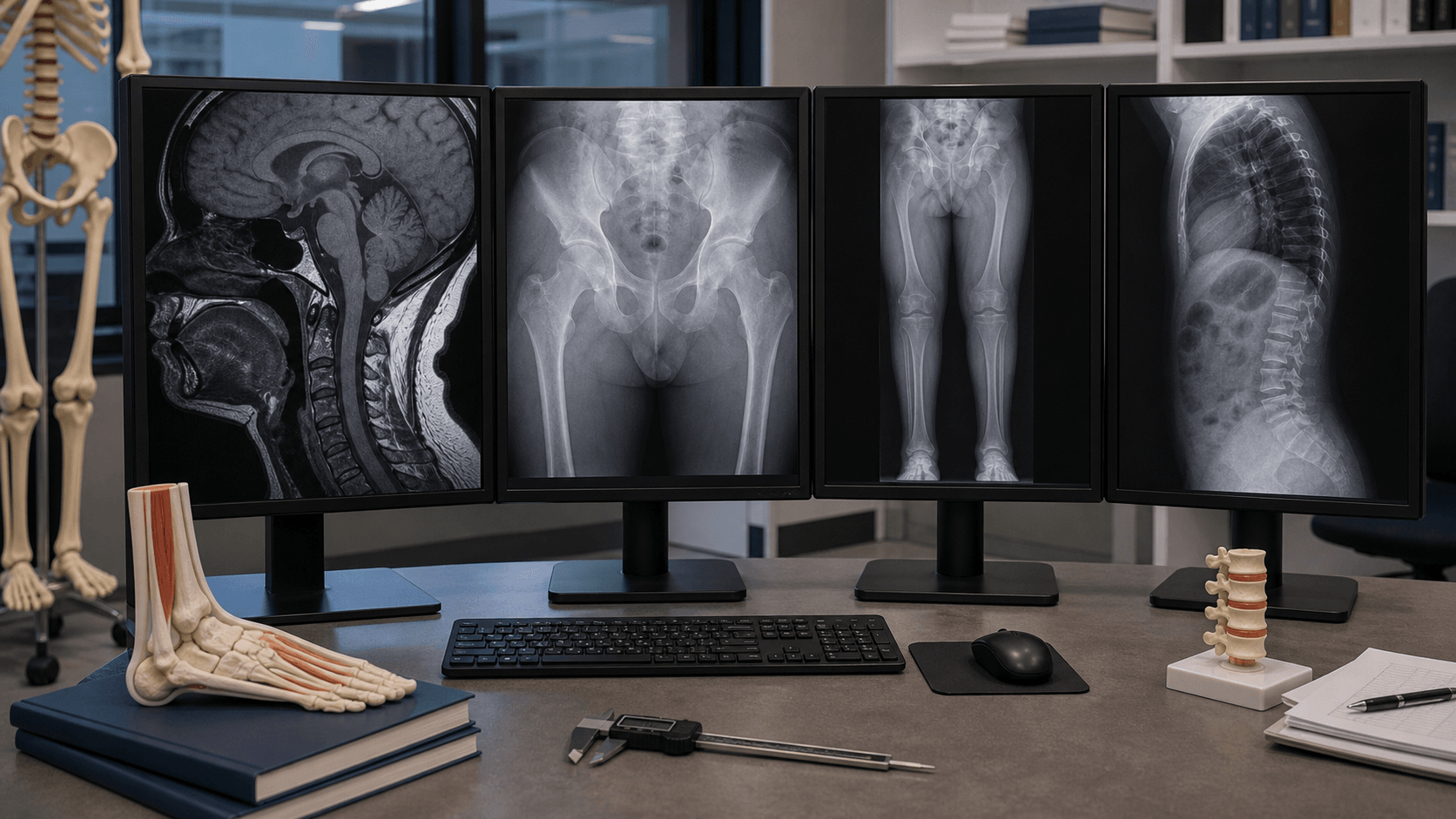
Imaging:
- MRI Craniocervical Junction: At birth/infancy for foramen magnum.
- Spine X-ray: Stenosis assessment.
- MRI Lumbar Spine: If symptomatic.
- Lower Limb X-rays: Mechanical axis.

Genetic:
- FGFR3 mutation testing (usually clinical diagnosis).
Management Algorithm
Foramen Magnum Stenosis
- Screening: MRI of craniocervical junction at birth.
- Symptomatic (apnea, neurological): Neurosurgical decompression.
- Asymptomatic with severe stenosis: Consider prophylactic decompression.
Surgical Techniques

Wide Laminectomy
Indications: Symptomatic spinal stenosis.
Technique: Wide decompression - need to go lateral to pedicles. Multi-level often needed. In the immature spine, add instrumentation/fusion to prevent post-laminectomy instability; in adults weigh fusion against preservation of motion.
Considerations: Short pedicles make surgery challenging.
Complications
Neurological Complications
- Incidence
- 5-10% symptomatic
- Risk Factors
- Small foramen magnum
- Management
- MRI screening, early decompression
- Incidence
- 2-5%
- Risk Factors
- Severe stenosis, sleep apnoea
- Management
- Polysomnography, decompression
- Incidence
- Variable
- Risk Factors
- Progressive compression
- Management
- Cervical or thoracolumbar decompression
- Incidence
- Rare
- Risk Factors
- Acute disc herniation
- Management
- Emergency decompression
- Incidence
- 20-30% adults
- Risk Factors
- Lateral recess stenosis
- Management
- Conservative or surgical decompression
Orthopaedic Complications
- Prevalence
- 30-40%
- Prevention
- Monitor with growth
- Treatment
- Guided growth or osteotomy
- Prevalence
- 90% infants
- Prevention
- Avoid early sitting
- Treatment
- Bracing, surgery if progressive
- Prevalence
- Common
- Prevention
- Physiotherapy
- Treatment
- Stretching, rarely surgical release
- Prevalence
- 10-20%
- Prevention
- Wide decompression
- Treatment
- Revision surgery
Anaesthetic and Perioperative Risks
Critical considerations for surgery in achondroplasia:
- Difficult Airway: Short neck, large head, narrow nasopharynx. Plan for difficult intubation.
- Atlantoaxial Instability: Screen with flexion-extension radiographs. Avoid neck hyperextension.
- Restrictive Lung Disease: Small thorax. Optimise respiratory function preoperatively.
- Spinal Anaesthesia: Technically difficult due to narrow canal. Consider GA instead.
- Positioning: Careful positioning to avoid pressure points and cervical injury.
Postoperative Care
Spinal Decompression Rehabilitation
- Day 1-2: Pain control, mobilisation with supervision
- Week 1-2: Walking program, stair climbing
- Week 2-6: Core strengthening, avoid heavy lifting
- Week 6+: Progressive return to activities
Lower Limb Osteotomy Recovery
- Weight Bearing: Protected weight bearing for 6-8 weeks
- Physiotherapy: Range of motion, strengthening as tolerated
- Hardware Removal: Consider after union confirmed (6-12 months)
- Long-term: Monitor for recurrence during remaining growth
Monitoring and Follow-up
- Neurological: Annual neurological examination
- Spinal: Regular MRI surveillance for stenosis progression
- Lower Limb: Monitor alignment during growth spurts
- Growth: Height velocity charts, orthopaedic review every 6-12 months
Outcomes/Prognosis
Overall Outcomes
- Life Expectancy: Near-normal with appropriate surveillance and intervention
- Functional Independence: Most patients lead independent productive lives
- Cognitive Function: Normal intelligence, no cognitive impairment
Surgical Outcomes
- Success Rate
- 90% symptom relief
- Complications
- CSF leak 5%, infection 2%
- Long-term Result
- Excellent if done early
- Success Rate
- 80% improvement
- Complications
- Dural tear 5%, recurrence 15%
- Long-term Result
- Good to excellent
- Success Rate
- 85% alignment correction
- Complications
- Delayed union 10%
- Long-term Result
- Generally durable
- Success Rate
- 10-15cm gain possible
- Complications
- Pin site infection 30%, nerve injury 5%
- Long-term Result
- Improves function
Quality of Life Considerations
- Physical Function: May have limitations but adapt well
- Social Integration: Generally good with supportive environment
- Employment: Wide range of careers possible
- Psychological: Higher rates of depression - screen and support
Evidence Base
- Identified FGFR3 as the achondroplasia gene at 4p16.3
- Same recurrent transmembrane-domain point mutation in 15/16 affected chromosomes (G1138A)
- Both observed mutations cause the same Gly380Arg substitution
- Prospective unselected series of 53 infants with achondroplasia
- 5/53 required suboccipital decompression for cervicomedullary compression
- Best predictors: lower-limb hyperreflexia/clonus, central hypopnea on polysomnography, small foramen magnum
- AAP health-supervision guideline for achondroplasia
- Anticipatory care for craniocervical compression, OSA, otitis media, kyphosis, genu varum
- Achondroplasia-specific growth and head-circumference charts
- 42-year mortality follow-up of 793 individuals with achondroplasia
- Average life expectancy reduced by ~10 years; mortality raised at all ages
- Heart-disease mortality ages 25-35 more than 10x the general population
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Newborn diagnosed with achondroplasia. What screening do you recommend?”
This infant needs **foramen magnum assessment** because stenosis at the craniocervical junction can cause apnea and sudden death. I would order an **MRI of the craniocervical junction** at birth or early infancy. If significant stenosis is present or the infant has symptoms (apnea, hypotonia, poor feeding), neurosurgical decompression is needed. I would also monitor for **thoracolumbar kyphosis** (common but usually resolves) and avoid unsupported sitting until spine matures.
“35-year-old with achondroplasia. Presents with neurogenic claudication, bilateral leg weakness.”
This patient has **lumbar spinal stenosis**, which is very common in achondroplasia. The short pedicles lead to a narrow canal. Management: **MRI lumbar spine** to confirm. If significant stenosis with neurological symptoms, surgery is indicated. I would perform **wide laminectomy** - decompression must extend lateral to the pedicles. Multi-level decompression is often needed. In adults, weigh fusion against preserving motion; in growing children, instrumentation reduces post-laminectomy instability and revision (Baca/Ain 2010).
“10-year-old with achondroplasia has progressive genu varum. How do you manage?”
Genu varum is common in achondroplasia. If **symptomatic** (pain, instability) or **progressive**, I would offer **corrective osteotomy**. This typically involves a **proximal tibial osteotomy** and possibly distal femoral osteotomy to correct mechanical axis. I would discuss with the family if they are interested in **limb lengthening** (can be combined) but counsel about high complication rates and lengthy treatment.
MCQ Practice Points
Q: What gene is mutated in achondroplasia? A: FGFR3 (gain-of-function mutation).
Q: What is the major orthopaedic issue in adults? A: Lumbar spinal stenosis.
Q: What is the dangerous issue in infancy? A: Foramen magnum stenosis (can cause sudden death).
Q: What is the pattern of limb shortening? A: Rhizomelic (proximal limbs shorter than distal).
Q: What is key to successful lumbar decompression in achondroplasia? A: Wide decompression extending lateral to the pedicles. Multi-level often needed. Short pedicles cause narrow canal.
Q: What new medical therapy is available for achondroplasia? A: Vosoritide - a C-natriuretic peptide analog that increases growth velocity by counteracting FGFR3.
Guidelines, Registries & Global Practice
Global Epidemiology
- Birth prevalence ~1 in 20,000-30,000 live births; the most common non-lethal skeletal dysplasia worldwide.
- ~80% arise as de novo mutations (unaffected average-stature parents); paternal age effect (older fathers).
- Single recurrent FGFR3 Gly380Arg mutation accounts for the vast majority of cases globally.
Side-by-Side Guidance
- Emphasis
- Age-based health supervision; craniocervical and OSA surveillance; achondroplasia-specific growth charts
- Emphasis
- Multidisciplinary skeletal-dysplasia centres; baseline craniocervical MRI plus polysomnography in infancy
- Emphasis
- Confirmatory FGFR3 testing where diagnosis uncertain; prenatal counselling for de novo and homozygous risk
- Emphasis
- Vosoritide approved for children with open growth plates; ongoing post-marketing follow-up of skeletal outcomes
Practice Variation
- High-resource settings: Neonatal craniocervical MRI, polysomnography, multidisciplinary dysplasia clinics, and access to vosoritide.
- Limited-resource settings: Diagnosis is clinical/radiographic; management is supportive, prioritising recognition of apnoea/cervicomedullary red flags and treatment of symptomatic stenosis and deformity.
- Genetic counselling and peer-support organisations (e.g. national dwarfism/little-people associations) are valuable everywhere for family planning and psychosocial support.
Controversies and Areas of Uncertainty
Prophylactic vs symptom-driven foramen magnum decompression There is no consensus threshold for operating on a radiographically small foramen magnum in an asymptomatic infant. Decisions integrate neurological signs, polysomnography (central hypopnoea), and craniocervical imaging rather than canal diameter alone.
Fusion/instrumentation with lumbar decompression in children Wide multilevel laminectomy can destabilise the immature spine. Evidence (Baca/Ain, J Pediatr Orthop 2010) favours adding instrumentation in growing children to reduce revision, but routine fusion in skeletally mature adults remains debated to preserve motion.
Limb lengthening Substantial height gain is achievable but carries high complication rates (pin-site infection, nerve injury, contracture, long treatment time). Whether lengthening is reconstructive or cosmetic is an ethical debate; many advocacy groups oppose routine lengthening for short stature alone.
Vosoritide and other FGFR3-pathway drugs Vosoritide reliably increases growth velocity, but its effect on final adult height, body proportionality, and serious complications (stenosis, foramen magnum compression) is unproven. Newer agents (e.g. CNP variants and FGFR3 inhibitors) are in trials. The aim of pharmacotherapy - height vs reduction of medical complications - is itself contested.
GENETICS
- FGFR3 Mutation
- Gain-of-function
- Autosomal Dominant
- 80% new mutations
CLINICAL
- Rhizomelic short stature
- Macrocephaly
- Trident hands
- Lumbar lordosis
SPINE
- Foramen magnum (infant)
- Lumbar stenosis (adult)
- Thoracolumbar kyphosis
- Short pedicles
LIMBS
- Genu varum
- Osteotomy if symptomatic
- Limb lengthening (controversial)
- High complication rate
FORAMEN MAGNUM
- Screen at birth (MRI)
- Apnea, sudden death risk
- Decompression if symptomatic
- Neurosurgery referral
NEW THERAPIES
- Vosoritide
- C-natriuretic peptide analog
- Increases growth velocity
- Approved (open growth plates)
Self-Assessment Quiz
Differential Diagnosis
Skeletal Dysplasias:
- Gene
- FGFR3
- Key Differentiator
- Most common, rhizomelic, foramen magnum
- Gene
- FGFR3
- Key Differentiator
- Milder form, less obvious features
- Gene
- FGFR3
- Key Differentiator
- Lethal, very short limbs
- Gene
- COMP
- Key Differentiator
- Normal face, short trunk + limbs
- Gene
- COL2A1
- Key Differentiator
- Short trunk, normal face
- Gene
- SLC26A2
- Key Differentiator
- Hitchhiker thumb, cauliflower ear
Key Distinguishing Points:
- Achondroplasia: Characteristic face (frontal bossing, midface hypoplasia)
- Pseudoachondroplasia: Normal face (distinguishes from achondroplasia)
- Thanatophoric: Lethal, telephone receiver femur
- Diastrophic: Hitchhiker thumb is pathognomonic
Additional Quiz Questions