Thompson Test | Complete Rupture | Surgical Repair
- Thompson test (calf squeeze) is the gold standard clinical test - absence of plantarflexion = rupture
- 80% occur 2-6cm proximal to insertion in the watershed zone of poor blood supply
- Operative vs non-operative: Similar outcomes but surgery has lower re-rupture rate (3-5% vs 10-15%)
- Early mobilization in functional bracing reduces complications in both operative and non-operative management
- Gap palpation and loss of contour are key clinical signs; delayed diagnosis common in 20-25% of cases
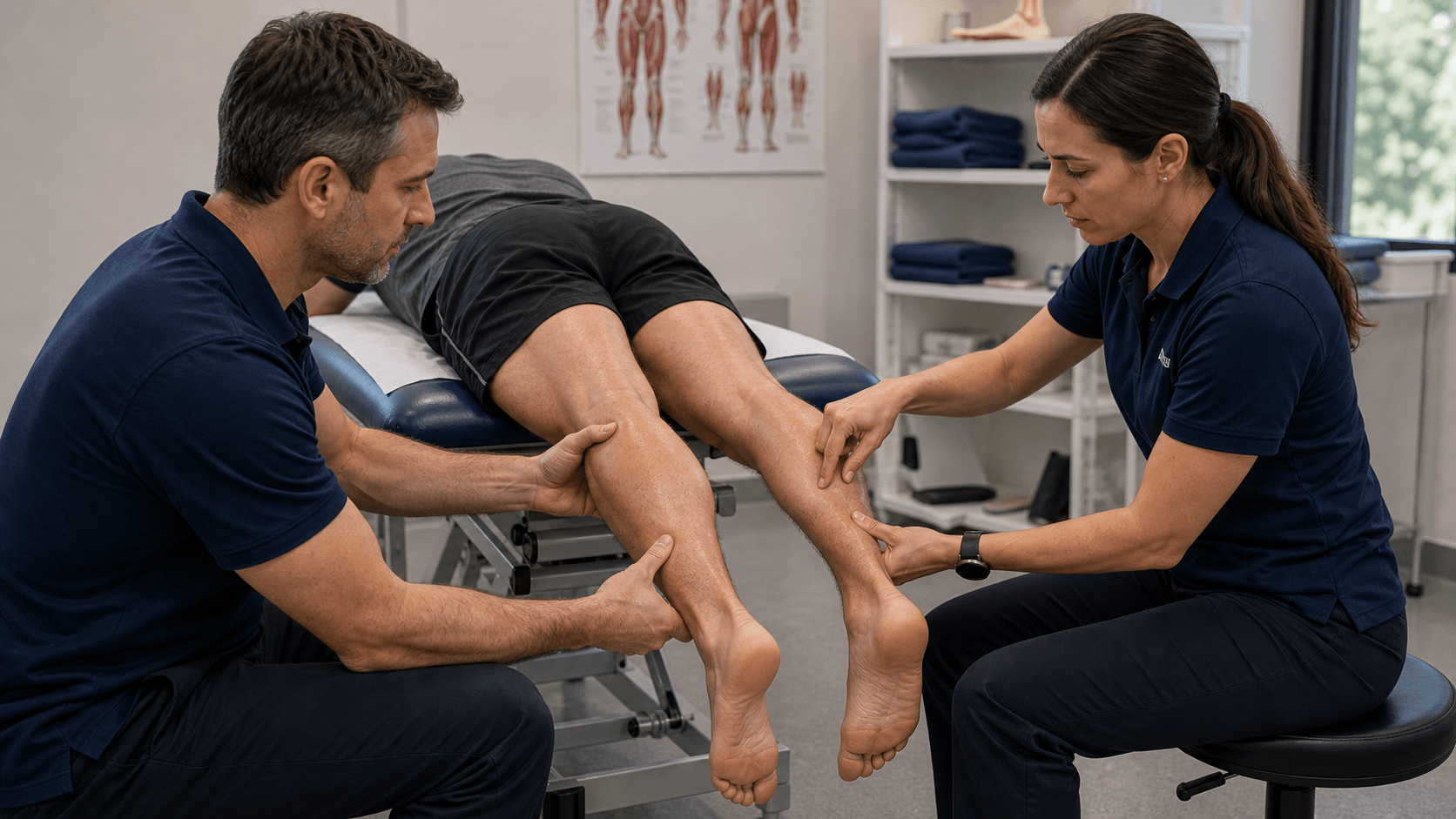
- “Describe Thompson test technique: patient prone, knee flexed 90 degrees, squeeze calf - positive if no plantarflexion
- “Know re-rupture rates: operative 3-5%, non-operative 10-15% (but functional outcomes similar)
- “Complications: Sural nerve injury (10-15%), DVT/PE risk, re-rupture
- “Weekend warrior injury: eccentric loading during push-off phase (tennis, basketball)
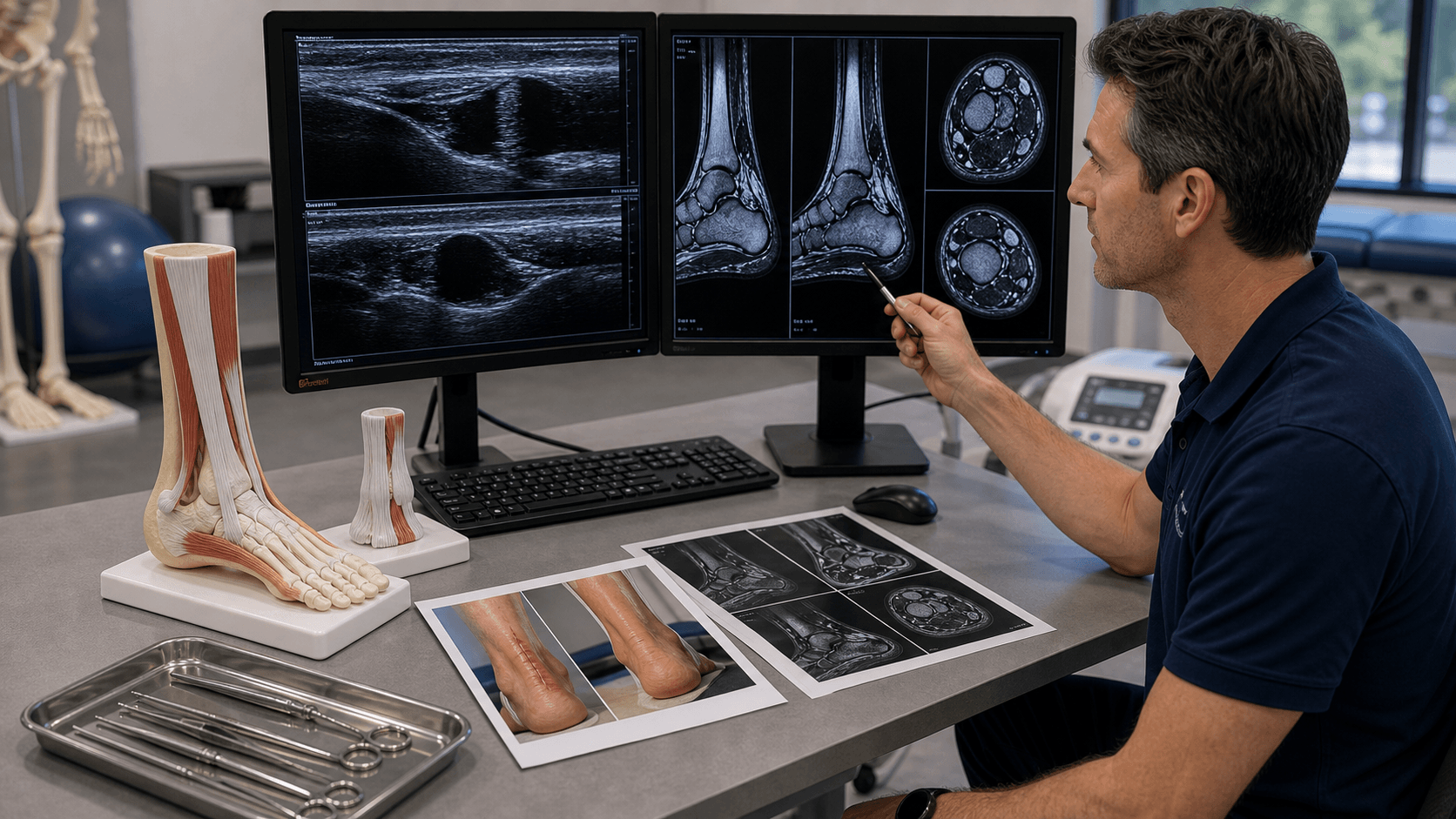
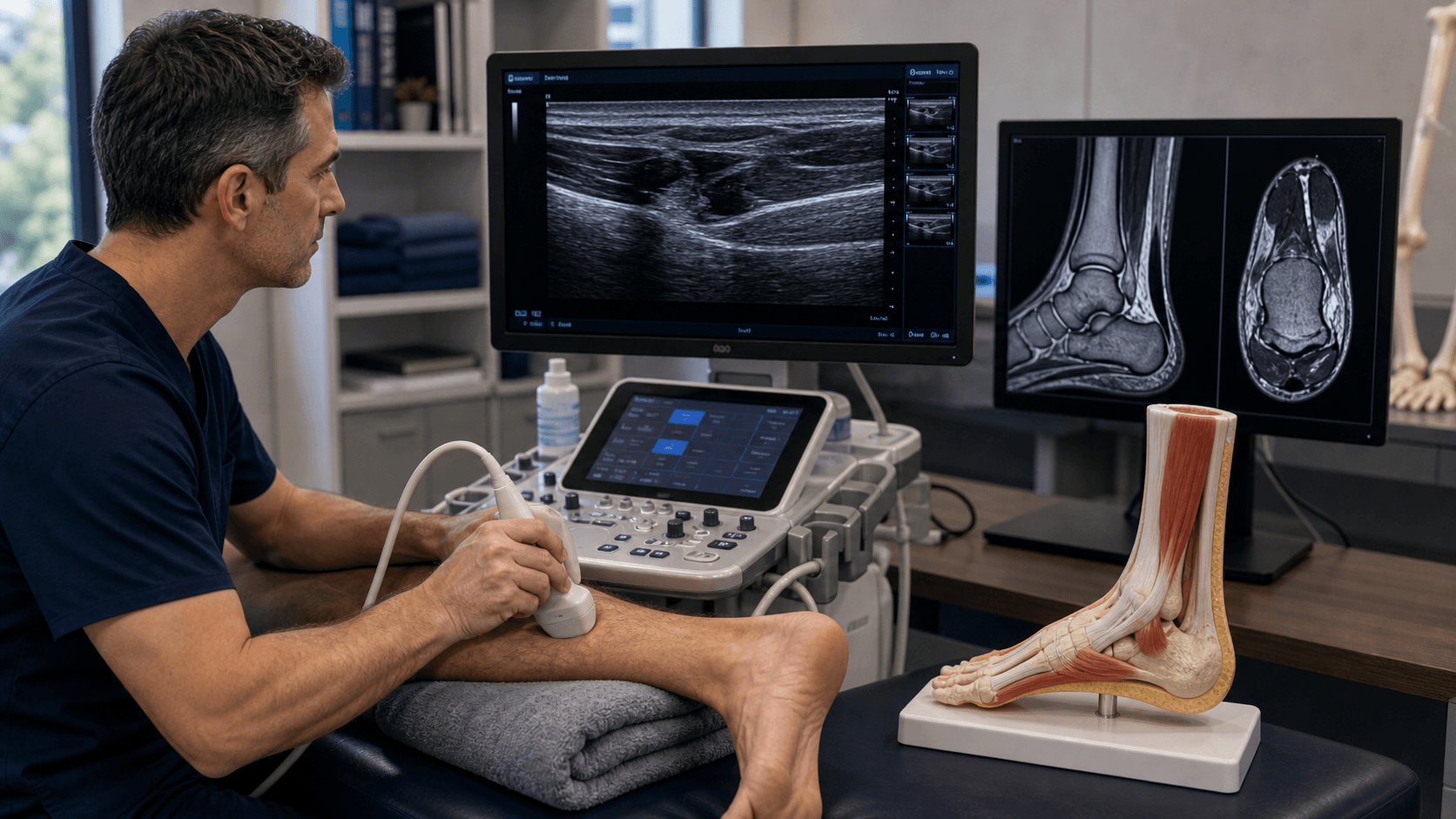
Clinical Imaging
Imaging Atlas

2-6cm proximal to insertion = poorest blood supply. Tendon receives blood from musculotendinous junction (muscle belly) and calcaneal insertion (bone). Watershed zone has relative avascularity, explaining rupture location.
Patient prone, knee flexed 90 degrees, squeeze mid-calf. Normal: ankle plantarflexes. Positive (rupture): no ankle movement. Sensitivity 96%, specificity 93%. Always compare to contralateral side.
Young active athletes: operative. Elderly sedentary: non-operative. Both need early controlled mobilization in functional brace. Operative has lower re-rupture but higher infection/nerve injury risk.
Under 4 weeks = acute (primary repair). Over 4 weeks = chronic (augmentation needed). Under 48 hours = percutaneous possible. Delayed diagnosis occurs in 20-25% - high index of suspicion needed.
| Patient | Timing | Treatment | Key Pearl |
|---|---|---|---|
| Young athlete, high demand | Acute (under 4 weeks) | Operative repair (open or percutaneous) | Lower re-rupture rate (3-5%) but nerve injury risk |
| Sedentary, low demand | Acute (under 4 weeks) | Non-operative functional bracing | Re-rupture 10-15% but avoid surgical complications |
| Delayed presentation | Chronic (over 4 weeks) | Augmented repair (FHL transfer, V-Y advancement) | Gap greater than 2cm needs augmentation |
| Insertional avulsion | Any timing | Reattachment with suture anchors | Different from mid-substance rupture |
CSAPThompson Test Components
Hook:CSAP your way to the diagnosis - Calf Squeeze shows Absent Plantarflexion in complete rupture!
QUINOLONESAchilles Rupture Risk Factors
Hook:Remember QUINOLONES - the antibiotic class most associated with Achilles rupture, plus all the other risk factors!
KRACKSurgical Repair Techniques
Hook:Don't KRACK under pressure - remember these key surgical steps for Achilles repair!
Overview and Epidemiology
Achilles tendon rupture is the most common lower extremity tendon rupture in active adults. The typical patient is a 30-50 year old male "weekend warrior" participating in sports requiring sudden acceleration or jumping (basketball, tennis, badminton). The injury occurs during eccentric loading of the plantarflexed ankle during push-off. Delayed diagnosis is common (20-25% of cases) due to patients still being able to walk and maintain some ankle plantarflexion via intact plantaris and toe flexors.
- Incidence: 11-37 per 100,000 population (increasing)
- Age: Bimodal - peak 30-50 years (sports), second peak over 60 years (degeneration)
- Gender: Male greater than female (5:1 ratio)
- Mechanism: Sudden eccentric loading during push-off phase
- Sports: Basketball, tennis, badminton, football, running
- Season: Spring and summer (return to sport after winter)
The "weekend warrior" profile is classic - sedentary lifestyle with intermittent high-intensity sports participation.
- Disability: Significant functional impairment
- Work absence: Average 3-6 months
- Sport return: 6-12 months (if return at all)
- Re-rupture: Major concern (3-15% depending on treatment)
- Missed diagnosis: 20-25% initially
- Litigation: Common when diagnosis delayed
Economic burden is substantial due to prolonged work absence and rehabilitation requirements.
Anatomy and Biomechanics
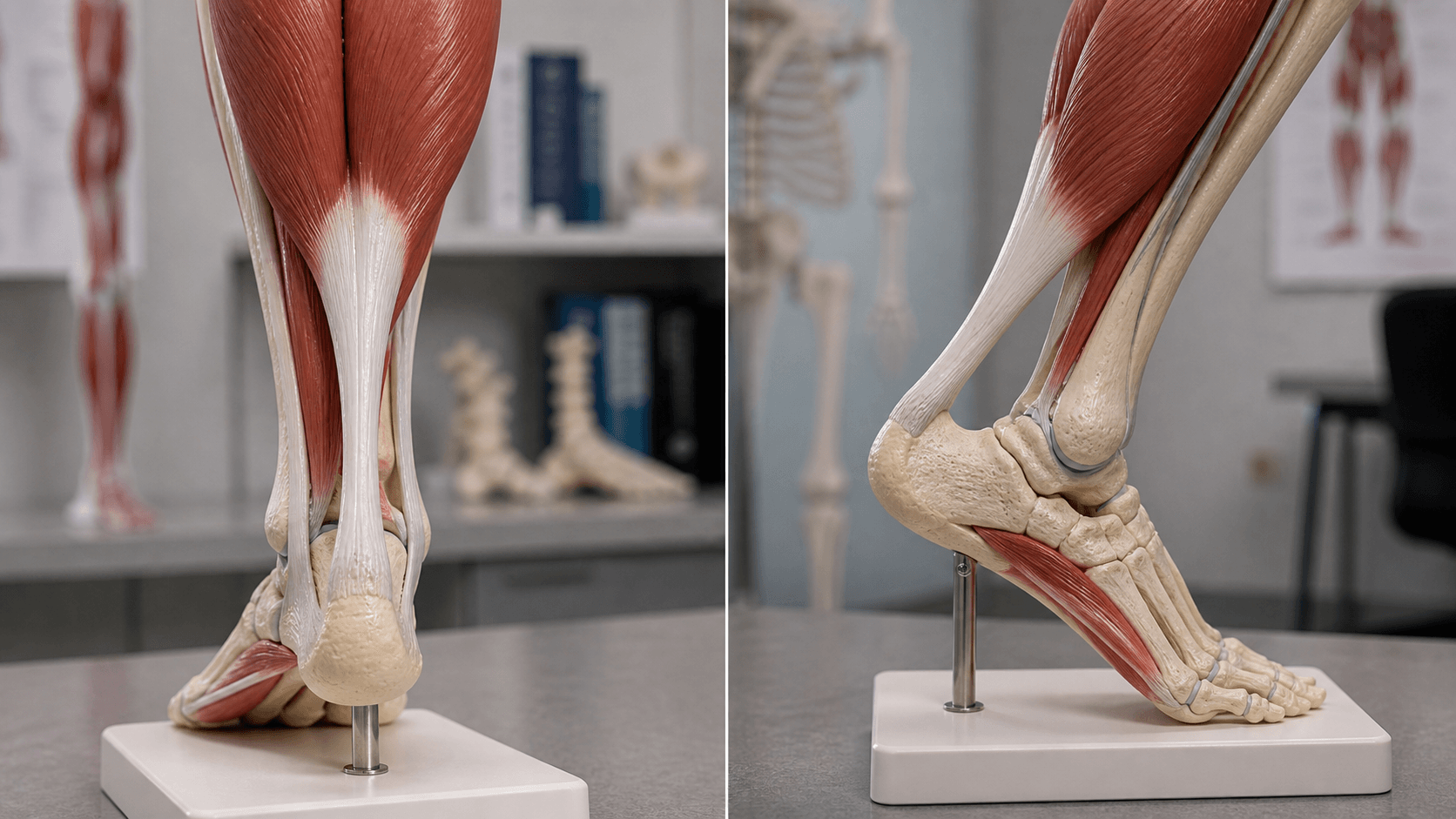
The tendon is most vulnerable 2-6cm proximal to the calcaneal insertion due to relative avascularity. Blood supply comes from:
- Proximal: Musculotendinous junction (muscle belly vessels)
- Distal: Calcaneal insertion (bone periosteum)
- Watershed zone: Area of poorest vascularization where ruptures occur
This explains why 80% of ruptures occur in this predictable location. The tendon narrows and twists in this region, creating additional mechanical stress concentration.
| Anatomical Feature | Clinical Significance | Exam Relevance |
|---|---|---|
| Tendon length 15cm | Largest and strongest tendon in body | Can generate forces up to 12 times body weight |
| Watershed zone 2-6cm proximal | Poorest blood supply | 80% of ruptures occur here |
| Gastrocnemius-soleus complex | Provides plantarflexion power | Intact toe flexors allow residual plantarflexion despite rupture |
| Plantaris tendon (medial) | May remain intact in Achilles rupture | Can confuse clinical picture - patient maintains some function |
Normal walking: 2-3 times body weight Running: 6-8 times body weight Jumping: 10-12 times body weight
Rupture occurs when force exceeds tendon strength, typically during:
- Sudden acceleration from stationary position
- Unexpected dorsiflexion of plantarflexed ankle
- Direct trauma (rare)
- Forceful dorsiflexion against resisted plantarflexion
The eccentric loading phase (deceleration while muscle contracts) generates the highest forces.
Sural nerve: Courses posterolateral to tendon
- At risk in posterolateral surgical approach (10-15% injury rate)
- Medial incision avoids this nerve
- Percutaneous repair has 2-20% nerve injury rate
Tibial nerve and vessels: Deep (anterior) to tendon
- Protected by deep fascia
- Rarely at risk unless deep dissection
Understanding nerve anatomy is crucial for surgical approach selection.
Pathophysiology and Injury Mechanism

Achilles tendon rupture occurs when the tensile load exceeds the tendon's capacity. This typically happens during eccentric contraction - when the calf muscles are contracting while the foot is dorsiflexing. Understanding pathophysiology explains why weekend warriors with pre-existing tendinopathy are at highest risk.
Mechanism of Injury
Primary Mechanisms:
- Push-off acceleration: Sudden forceful takeoff (basketball jump, tennis sprint start)
- Unexpected dorsiflexion: Landing on plantarflexed foot that forcibly dorsiflexes
- Forceful dorsiflexion against resistance: Stumbling with contracted calf muscles
- Direct trauma: Rare (under 5%), usually penetrating injury
Sequence of Events in Rupture
Most ruptures occur in tendons with subclinical degenerative changes. The tendon appears normal grossly but has areas of mucoid degeneration, decreased cellularity, and disorganized collagen fibers at a microscopic level.
During push-off or unexpected dorsiflexion, the muscle-tendon unit is loaded eccentrically (contracting while lengthening). This generates forces up to 12x body weight.
The weakest point (2-6cm proximal to insertion) with poorest blood supply fails. The tendon tears with audible pop felt like being kicked in the back of the leg.
Muscle belly recoils proximally due to loss of continuity. Gap develops immediately. Without treatment, scar tissue fills gap but lacks mechanical strength.
Why the Watershed Zone Fails
Vascular Anatomy:
- Blood supply from proximal (musculotendinous junction) and distal (calcaneal insertion)
- The 2-6cm zone has poorest perfusion
- Hypoxia contributes to degenerative changes
- Limited capacity for healing and repair
Mechanical Factors:
- Tendon narrows and rotates 90 degrees in this zone
- Concentration of stress at cross-sectional narrowing
- Cumulative microdamage from repetitive loading
The classic patient is a 30-50 year old male who is sedentary during the week but participates in high-intensity sports on weekends. The tendon has subclinical degeneration from underuse, is not conditioned for sudden loading, and fails during the first aggressive push-off. This explains why ruptures often occur early in a game or match, before adequate warm-up.
Risk Factor Pathophysiology
Fluoroquinolone Antibiotics (3x increased risk):
- Disrupt collagen synthesis and increase proteolytic activity
- Mechanism: MMPs activation, tenocyte death
- Peak risk: first 30 days of therapy
- Highest risk: ciprofloxacin, levofloxacin
Corticosteroid Injections:
- Cause focal tendon necrosis
- Weaken collagen structure
- Risk persists for weeks after injection
- NEVER inject into the tendon substance
Systemic Conditions:
- Diabetes: Glycation of collagen, neuropathy
- Renal failure: Uremic tendinopathy
- Rheumatoid arthritis: Inflammatory degradation
- Obesity: Increased mechanical load
Classification Systems
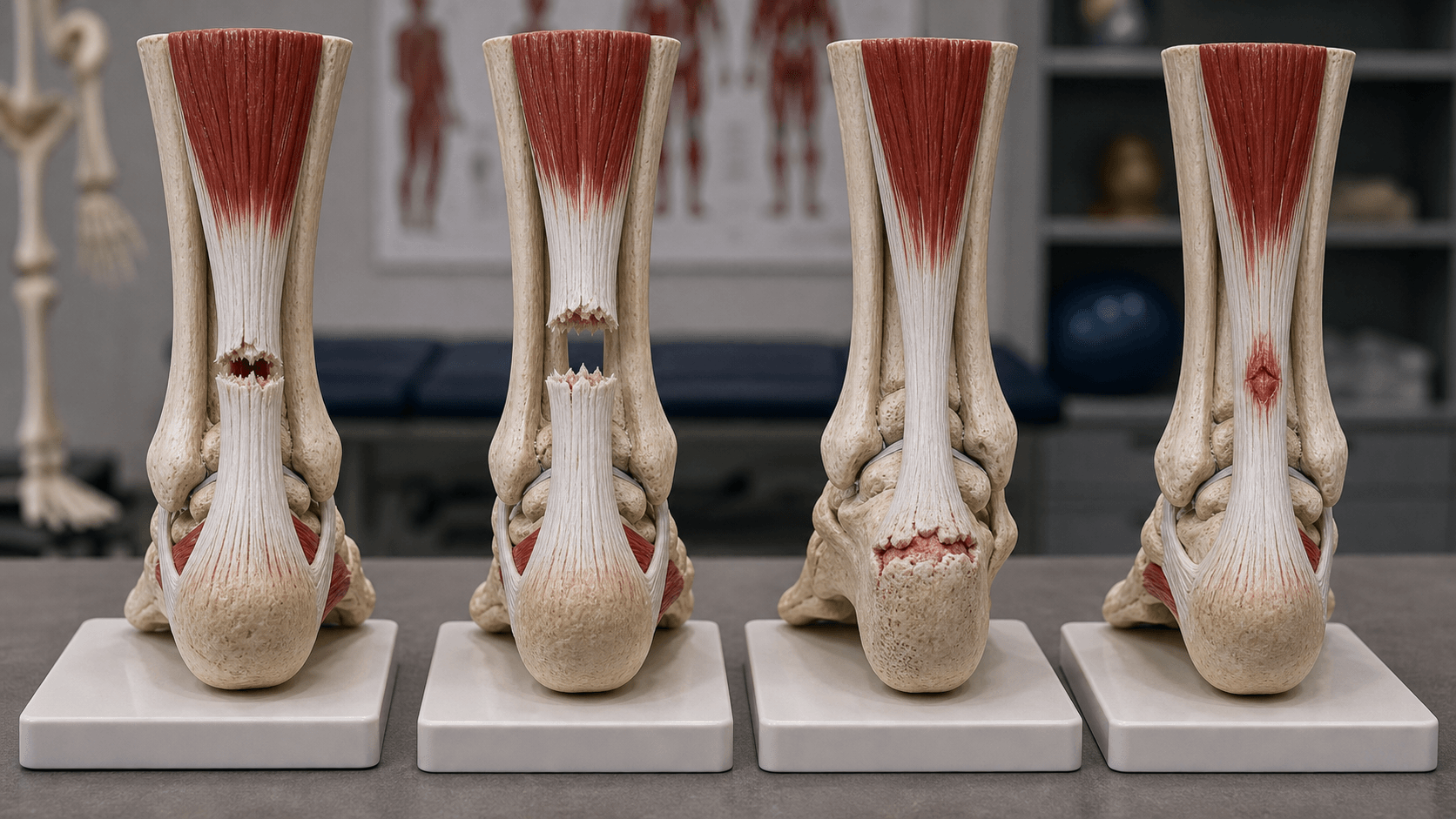
Acute vs Chronic Classification
| Type | Timeframe | Pathology | Treatment |
|---|---|---|---|
| Acute | Under 4 weeks from injury | Fresh tear, viable tissue, minimal gap | Primary end-to-end repair or conservative |
| Subacute | 4-8 weeks from injury | Early scar formation, some retraction | May need augmentation if gap over 2cm |
| Chronic | Over 8 weeks from injury | Significant retraction, poor tissue quality | Augmentation required (FHL, V-Y, turndown) |
The 4-week timepoint is when scar tissue forms and tendon ends retract significantly. Acute tears (under 4 weeks) can usually achieve end-to-end approximation with ankle in plantarflexion. Chronic tears (over 4 weeks) have a gap greater than 2cm that cannot be closed without augmentation. This fundamentally changes surgical planning.
Treatment decisions shift dramatically at this timepoint - primary repair becomes augmented reconstruction.
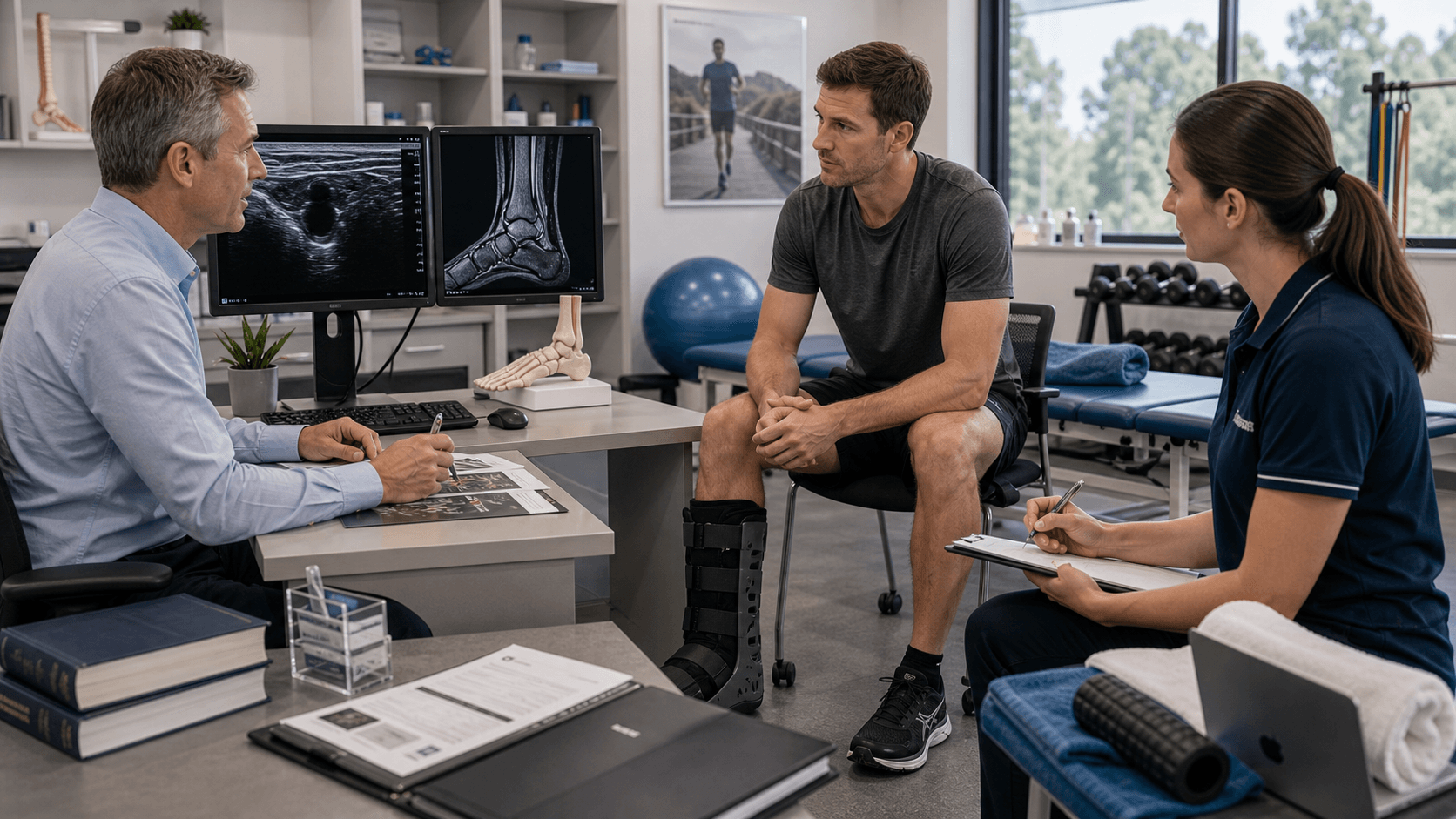
Clinical Assessment

Classic presentation:
- "Pop" or snap sensation in posterior ankle
- "Felt like someone kicked me from behind" (pathognomonic)
- Immediate pain and inability to continue activity
- Unable to stand on tiptoes
- May still walk (common - leads to missed diagnosis)
Risk factor history:
- Recent fluoroquinolone antibiotic use
- Steroid injection to tendon
- Pre-existing Achilles tendinopathy
- Weekend warrior activity pattern
- Previous contralateral rupture (10% bilateral)
Inspection:
- Visible gap or divot 2-6cm above heel
- Loss of normal tendon contour
- Swelling and ecchymosis
- Asymmetry compared to contralateral
Palpation:
- Palpable gap in tendon (pathognomonic)
- Tenderness at rupture site
- Measure gap size with ankle plantarflexed
Function:
- Cannot stand on tiptoes (single leg heel raise)
- Weak plantarflexion (but not absent - toe flexors intact)
- Increased dorsiflexion compared to normal side

20-25% of Achilles ruptures are initially missed because:
- Patient can still walk (tibialis posterior, FHL, FDL provide plantarflexion)
- Plantaris tendon may be intact
- Some swelling may obscure palpable gap
- Examiner fails to perform Thompson test
- Attributed to "ankle sprain" without proper examination
Always perform Thompson test in any posterior ankle injury. Delayed diagnosis leads to worse outcomes and potential litigation.
Differential Diagnosis
| Condition | Distinguishing Features | Thompson Test | Key Discriminator |
|---|---|---|---|
| Complete Achilles rupture | Sudden pop, palpable gap, cannot single-leg heel raise | Positive (no plantarflexion) | Palpable gap plus positive Thompson test |
| Partial Achilles tear | Pain and swelling, often able to weight bear and heel raise | Negative (plantarflexion preserved) | Continuity on ultrasound/MRI; no full gap |
| Achilles tendinopathy | Chronic gradual pain, morning stiffness, fusiform thickening | Negative | No acute event; degenerative thickening not gap |
| Gastrocnemius (medial head) tear - tennis leg | Sharp medial calf pain on push-off, bruising tracks distally | Negative | Tenderness at musculotendinous junction, not tendon; intact Achilles |
| Deep vein thrombosis | Calf swelling/tenderness, often no clear trauma, risk factors | Negative | Doppler ultrasound; consider as both differential and complication |
| Ankle sprain | Lateral/medial ankle pain, malleolar tenderness | Negative | Pain localises to ligaments, tendon intact - common misdiagnosis |
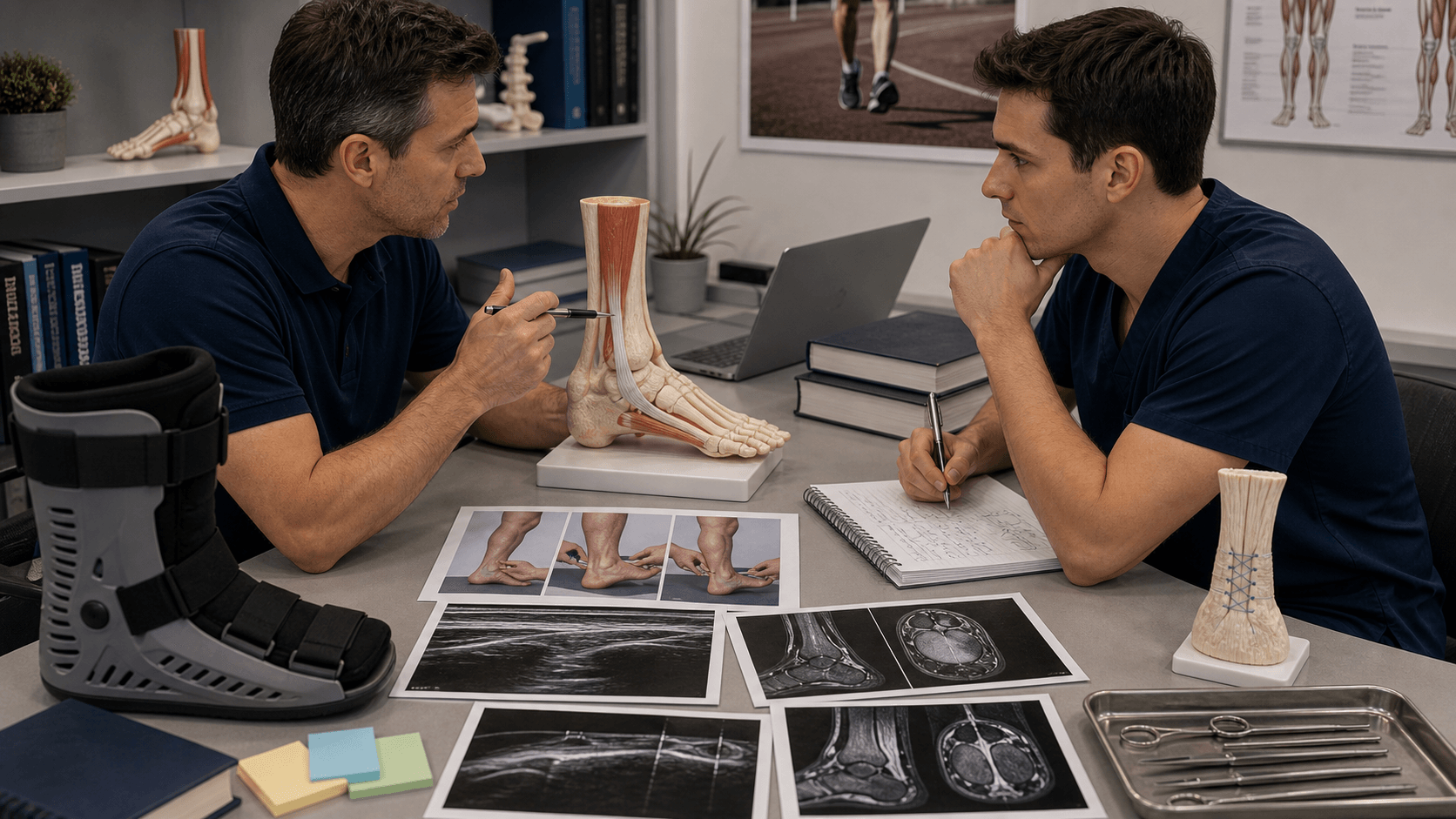
Thompson Test (Simmonds Test)

Thompson Test Technique
Patient prone on examination table
- Knee flexed to 90 degrees
- Ankle hanging off edge of table
- Both legs tested for comparison
- Patient relaxed (not actively plantarflexing)
Squeeze mid-calf firmly
- Grasp gastrocnemius muscle belly
- Firm squeeze (not just light touch)
- Observe ankle movement
- No verbal cues to patient (avoid voluntary movement)
Normal (negative test):
- Ankle plantarflexes when calf squeezed
- Indicates intact Achilles tendon
Abnormal (positive test):
- No ankle plantarflexion = rupture
- Or significantly reduced plantarflexion compared to normal side
- Sensitivity 96%, specificity 93%
False negatives can occur if:
- Partial rupture (rare)
- Plantaris intact and confused for Achilles
- Patient voluntarily plantarflexes (improper technique)
- Chronic rupture with scar bridging gap
Always correlate with:
- Palpable gap
- Inability to single leg heel raise
- Imaging if any doubt
The Thompson test is the most reliable clinical test but must be performed correctly with proper patient positioning and examiner technique.
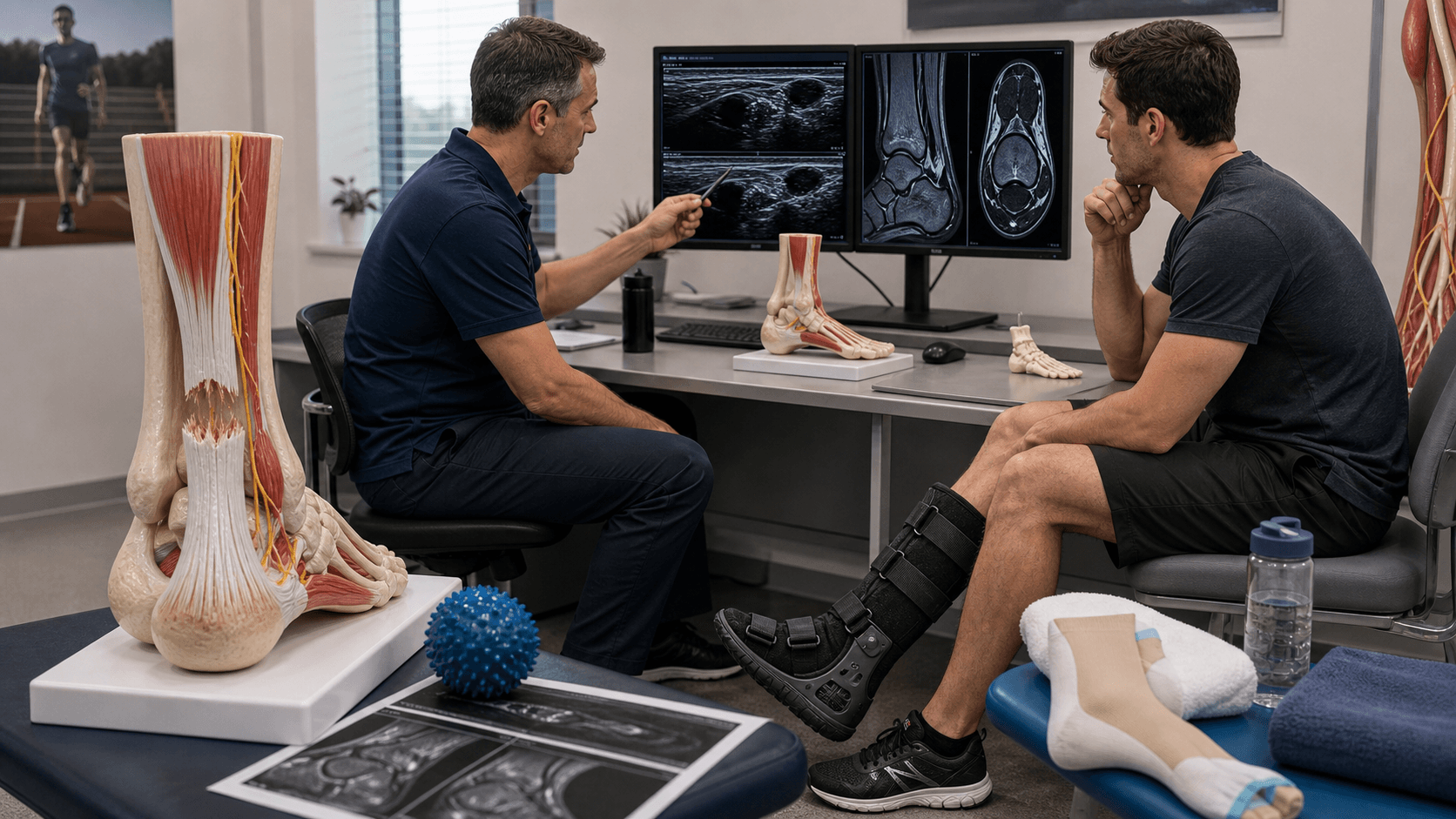
Investigations
Imaging Protocol
Achilles rupture is primarily a clinical diagnosis
- History and mechanism
- Palpable gap
- Positive Thompson test
Imaging confirms diagnosis and guides treatment planning:
- Identifies exact rupture location
- Measures gap size
- Rules out partial rupture
- Detects associated pathology
Advantages:
- Dynamic assessment (ankle in different positions)
- Measure gap with ankle plantarflexed
- Real-time visualization
- No radiation
- Low cost
Findings:
- Hypoechoic gap at rupture site
- Tendon retraction
- Hematoma
- Can measure gap under 1cm, 1-2cm, over 2cm
Accuracy: Sensitivity 95%, specificity 93% in experienced hands
Indications:
- Chronic rupture (surgical planning)
- Partial rupture suspected
- Insertional pathology
- Pre-operative planning for chronic cases
Findings:
- High T2 signal at rupture site
- Exact gap measurement
- Tendon quality assessment (degeneration)
- Associated pathology (retrocalcaneal bursitis)
- Muscle atrophy in chronic cases
Not routinely required for acute ruptures - clinical diagnosis sufficient
Limited role:
- Kager's fat pad obliteration (indirect sign)
- Calcific insertional tendinopathy
- Avulsion fracture fragment
- Pre-operative planning
Cannot directly visualize tendon - only shows secondary signs
When to image:
- Acute, clear clinical diagnosis: No imaging needed (clinical diagnosis sufficient)
- Unclear history or examination: Ultrasound
- Chronic rupture: MRI for surgical planning
- Partial rupture suspected: MRI
- Medico-legal documentation: Ultrasound or MRI
In practice: Many surgeons obtain ultrasound or MRI for documentation and surgical planning even with clear clinical diagnosis.
Gap size determines treatment:
- Under 1cm: Conservative possible
- 1-2cm: Standard repair
- Over 2cm: Augmentation needed
Measure with ankle in maximal plantarflexion - this is the position that will be used for repair. MRI or ultrasound in neutral position will overestimate the gap.
Dynamic ultrasound allows real-time measurement with ankle positioning.
Management Algorithm
Treatment Decision Framework
Goal: Return to pre-injury function with lowest complication rate
| Factor | Favors Operative | Favors Non-Operative |
|---|---|---|
| Patient age and activity | Young (under 40), high athletic demand | Elderly (over 60), low demand, sedentary |
| Re-rupture risk tolerance | Cannot accept 10-15% re-rupture | Willing to accept higher re-rupture to avoid surgery |
| Medical comorbidities | Healthy, low surgical risk | Diabetes, PVD, smoking, high surgical risk |
| Timing | Acute (under 2 weeks) or chronic (over 4 weeks) | Acute only (2-4 weeks window) |
Meta-analyses show:
- Re-rupture rate: Operative 3-5%, Non-operative 10-15%
- Functional outcomes: Similar at 1-2 years
- Return to sport: Similar rates and timing
- Complications: Operative has infection (3-5%) and nerve injury (10-15%) risk
Modern non-operative protocols with early functional rehabilitation have narrowed the re-rupture gap (now closer to 7-8% vs 3-4%). The key is early controlled mobilization regardless of treatment choice.
Decision is individualized based on patient factors, surgeon experience, and patient preference after informed consent.
Surgical Technique
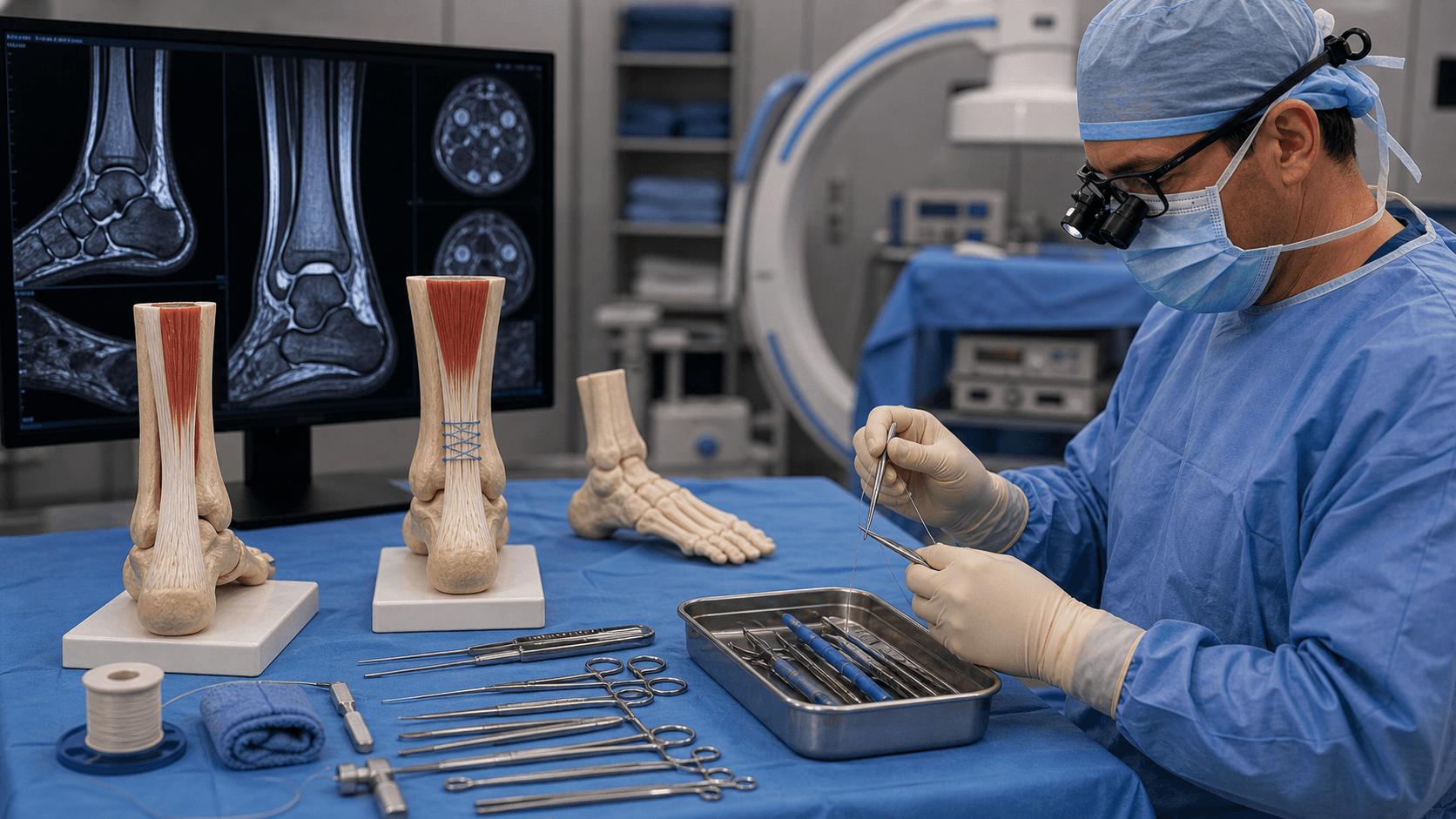
Open vs Percutaneous vs Mini-Open
| Technique | Advantages | Disadvantages | Best For |
|---|---|---|---|
| Open medial incision | Direct visualization, accurate repair, safe for sural nerve | Larger wound, infection risk 3-5% | Gold standard for most cases |
| Open posterolateral | Traditional approach | Sural nerve injury 10-15%, wound healing issues | Avoid - medial approach superior |
| Percutaneous repair | Small incisions, lower infection, cosmetic | Nerve injury 2-20%, cannot see repair quality | Acute ruptures under 48 hours, experienced surgeon |
| Mini-open | Smaller incision (3-4cm), lower infection than full open | Limited visualization, learning curve | Growing popularity, good outcomes in experienced hands |
Medial incision is now preferred over posterolateral:
- Sural nerve runs posterolateral - avoided with medial approach
- Better wound healing (not on weight-bearing surface)
- Avoid posterior midline (watershed zone for skin healing)
- Slightly more challenging exposure but safer
Technique: 1-2cm medial to tendon lateral border, avoiding posterior midline entirely.
Approach selection depends on acuity, gap size, surgeon experience, and patient factors.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Re-rupture | Operative 3-5%, Non-operative 10-15% | Non-compliance, early weight bearing, over-lengthening | Usually revision surgery with augmentation |
| Sural nerve injury | Operative 10-15% (posterolateral approach) | Posterolateral incision, percutaneous repair | Usually neuropraxia - observation. Medial approach avoids this. |
| Infection | Operative 3-5%, Non-operative under 1% | Diabetes, smoking, steroids, posterior incision | Antibiotics if superficial, debridement if deep |
| DVT/PE | Non-operative 6-8%, Operative 2-3% (on prophylaxis) | Immobilization, non-weight bearing, age over 40 | LMWH prophylaxis, early mobilization protocol |
| Wound dehiscence | Operative 2-5% | Posterior incision, tension, smoking, diabetes | Local wound care or revision closure |
| Adhesions/stiffness | Both 10-20% | Prolonged immobilization, poor rehab | Aggressive physiotherapy, rarely surgery |
| Weakness/strength deficit | Both 10-30% (subjective) | Over-lengthening, muscle atrophy, inadequate rehab | Strengthening program, usually improves to 80-90% by 1 year |
Achilles rupture has 6-8% DVT rate without prophylaxis due to prolonged immobilization and calf injury. Consider LMWH (enoxaparin 40mg daily) for:
- All non-operative patients (immobilized 4-6 weeks)
- Operative patients with risk factors (age over 40, obesity, previous DVT)
- Continue until fully weight bearing
- Early functional mobilization in boot reduces DVT risk
This is a high-risk injury for thromboembolic complications - do not overlook prophylaxis.
Re-rupture is devastating - usually occurs at 4-8 weeks when rehabilitation is progressing. Risk factors:
- Early weight bearing before healing (4-6 weeks)
- Non-compliance with boot or restrictions
- Over-lengthening at index surgery (weak repair)
- Inadequate initial repair (poor technique)
- Return to sport too early (before 6 months)
Prevention: Strict protocol adherence, weekly follow-up in first 2 months, gradual progression, consider functional brace for sport return.
Postoperative Care and Rehabilitation

Post-Surgical Rehabilitation Timeline
Standard Operative Protocol
Immobilization:
- Posterior splint in slight plantarflexion (10-15 degrees)
- Non-weight bearing with crutches
- Elevate leg (reduce swelling and DVT risk)
- Ice therapy
- DVT prophylaxis (LMWH if risk factors)
Wound care:
- Keep dry until sutures out (10-14 days)
- Monitor for infection signs
- First post-op visit 7-10 days (wound check)
Transition to boot:
- Remove splint, apply functional boot with heel wedges
- Begin early gentle ankle ROM in boot (plantarflexion only)
- Progressive weight bearing 25% to 50% to 75%
- Remove one heel wedge every 1-2 weeks
- Boot remains locked in plantarflexion initially
Rehabilitation:
- Gentle isometric exercises
- Maintain knee and hip ROM
- Upper body and core strengthening
- Pool therapy if wound healed (buoyancy assists)
Increase activity:
- Full weight bearing in boot
- All heel wedges removed (ankle at neutral)
- Unlock boot for controlled dorsiflexion
- Begin active ROM exercises
- Light resistance exercises (theraband)
Goals:
- Pain-free full weight bearing
- Dorsiflexion to neutral
- Ready to wean from boot
Wean from boot:
- Transition to supportive shoe (hiking boot, ankle brace)
- Progressive strengthening program
- Heel raise exercises (bilateral initially)
- Stationary bike, elliptical (low impact)
- Balance and proprioception training
Criteria to wean:
- Full passive dorsiflexion
- Pain-free walking
- Able to perform 10 bilateral heel raises
Sport-specific training:
- Light jogging at 3 months (if strength 70-80% of normal)
- Single leg heel raises (10-15 repetitions goal)
- Plyometric exercises (jumping, hopping)
- Sport-specific drills
- No competitive sport until 6 months minimum
Criteria for sport return:
- Single leg heel raise strength 80-90% of contralateral
- No pain with running or jumping
- Normal gait pattern
- Clearance from surgeon and physiotherapist
Ongoing maintenance:
- Continue strengthening program
- Gradual return to full sport participation
- Monitor for signs of re-rupture (pain, weakness)
- Expect continued strength gains up to 12-18 months
Long-term:
- Most patients plateau at 80-90% of pre-injury strength
- May have subjective weakness with fatigue
- Risk of contralateral rupture (10% over lifetime)
Modern trend: Early controlled mobilization
- Traditional: Immobilization 6-8 weeks in cast
- Accelerated: Functional boot with early ROM at 2 weeks
Evidence shows:
- No difference in re-rupture rates
- Faster return to work and sport with accelerated
- Less stiffness and DVT with early motion
- Requires compliant patient and close monitoring
Most surgeons now use accelerated protocols with functional bracing and early ROM.
The key is balancing early motion (to prevent stiffness) with protection (to prevent re-rupture).
Outcomes and Prognosis

| Treatment | Re-rupture Rate | Return to Sport | Complications | Patient Satisfaction |
|---|---|---|---|---|
| Operative (open) | 3-5% | 6-9 months (average 7 months) | Infection 3-5%, Nerve injury 10-15% | 85-90% satisfied |
| Non-operative (functional rehab) | 7-10% (modern protocols) | 6-9 months (similar to operative) | DVT 6-8% without prophylaxis | 80-85% satisfied |
| Non-operative (traditional cast) | 10-15% (historical) | 9-12 months (slower) | Stiffness, DVT, muscle atrophy | 70-75% satisfied |
Good prognosis factors:
- Age under 40 years
- Acute repair (under 2 weeks)
- Appropriate length restoration (not over-lengthened)
- Early functional rehabilitation
- Compliant patient
- No re-rupture
Poor prognosis factors:
- Age over 60 years
- Chronic rupture
- Over-lengthening at repair
- Prolonged immobilization
- Re-rupture
- Smoking, diabetes
The single most important factor is avoiding re-rupture - this changes a good outcome to a fair/poor outcome with chronic deficits.
Realistic counseling pre-operatively:
- Full recovery 12-18 months
- May never return to 100% of pre-injury strength
- Subjective weakness common (10-30%)
- Risk of contralateral rupture (10% lifetime)
- Re-rupture risk exists (follow protocol strictly)
Return to sport:
- 80-90% return to pre-injury sport level
- Professional athletes: 75% return to same level
- Recreational athletes: 85% return to sport
- Some change sport due to fear of re-rupture
Persistent problems (minority):
- Calf atrophy and weakness (10-20%)
- Fatigue with prolonged activity
- Occasional Achilles pain (5-10%)
- Ankle stiffness (especially if poor rehab)
- Sural nerve numbness if nerve injured
Positive aspects:
- Most return to normal daily activities
- Pain usually resolves by 6-12 months
- Continued improvement up to 2 years
- Low risk of arthritis or chronic pain
Evidence Base and Key Trials
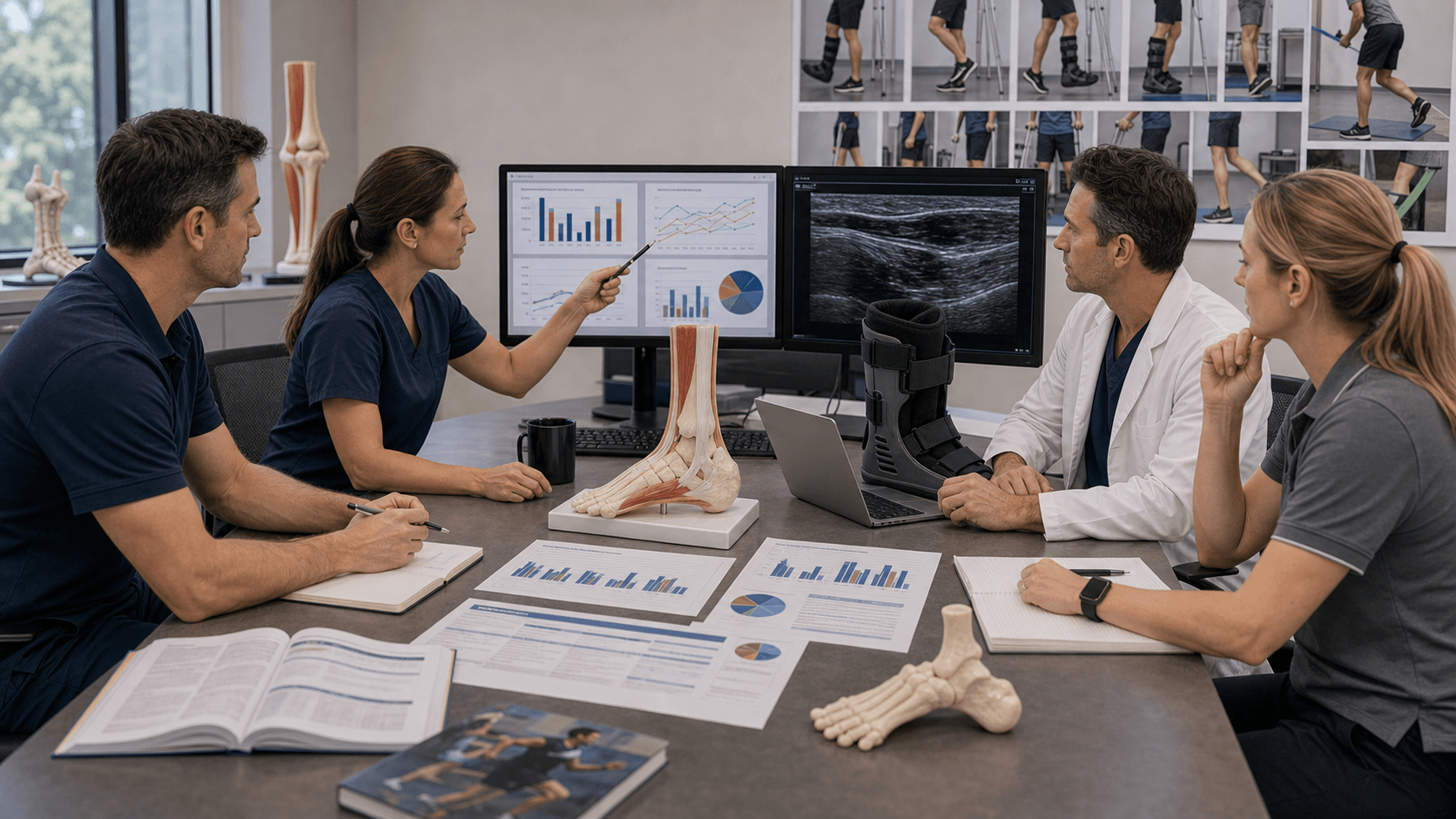
Operative vs Non-Operative Management: Quantitative Systematic Review of RCTs
- Meta-analysis of 7 level-I RCTs (677 patients)
- Re-rupture: Open repair 3.6% vs non-operative 8.8% (OR 0.425, 95% CI 0.222-0.815)
- Deep infection, sural nerve sensory disturbance and non-cosmetic scar complaints all significantly higher with surgery
- Strength measurements not standardised, so could not be pooled
Operative vs Non-Operative with Accelerated Functional Rehabilitation (Multicentre RCT)
- 144 patients randomised (72 operative, 72 non-operative); all underwent accelerated rehab with early weight-bearing and early range of motion
- Re-rupture: 2/72 operative vs 3/72 non-operative (no significant difference)
- No clinically important difference in strength, range of motion, calf circumference or Leppilahti score
- More complications in the operative group (13 vs 6), mainly soft-tissue related
Surgical vs Non-Surgical Treatment: Meta-Analysis with Functional Rehabilitation Subgroup
- Meta-analysis of 10 randomised trials
- With early range of motion, re-rupture rates equal for surgical and non-surgical care (risk difference 1.7%, p=0.45)
- Without early motion, surgery reduced re-rupture by an absolute 8.8% (p=0.001)
- Surgery increased other complications by an absolute 15.8% and allowed return to work 19 days sooner
Percutaneous (PARS) vs Open Repair: Clinical Outcomes and Complications
- Retrospective cohort of 270 operatively treated acute ruptures (101 PARS, 169 open)
- No significant difference in re-rupture, sural neuritis, wound dehiscence, infection or reoperation
- No reruptures and no DVTs in either group
- Return to baseline activity by 5 months higher with PARS (98% vs 82%, p=0.0001); overall operative complication rate 8.5%
FHL Transfer for Chronic Achilles Rupture Reconstruction
- 11 patients with chronic Achilles rupture (mean defect 7.4cm) treated by modified FHL transfer with fibrous-stump augmentation
- Significant improvement in AOFAS score at mean 79-month follow-up; no re-rupture or major wound complication
- Isokinetic plantarflexion peak-torque deficit of 28% (30 deg/s) and 36% (120 deg/s) persisted
- Loss of hallux interphalangeal motion without functional weakness
Tendon Injury and Fluoroquinolone Use: Systematic Review
- Systematic review of 16 observational studies (8 high quality; 5 specifically on Achilles rupture)
- Increased Achilles rupture risk with fluoroquinolone exposure, odds ratios ranging from 1.1 to 7.1
- Highest risk within the first month of exposure; one study showed increased risk in those over 60 years
- Concomitant corticosteroids further increase tendon-injury risk
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old male recreational basketball player presents to emergency department after sudden onset posterior ankle pain during a game 2 hours ago. He describes a 'pop' sensation and felt like someone kicked him from behind. He can walk but with a limp. On examination there is mild swelling and ecchymosis over the posterior ankle. What is your assessment and initial management?”
“You have decided to proceed with operative repair for an acute Achilles tendon rupture in a 35-year-old professional footballer. The injury occurred 5 days ago. Walk me through your surgical approach and technique for the repair.”
“A 38-year-old patient who underwent open Achilles repair 8 weeks ago presents with sudden onset posterior ankle pain and inability to walk. He admits he removed his boot 2 weeks ago against advice and returned to jogging. Thompson test is positive. What is your assessment and management?”
MCQ Practice Points
Q: Where do 80% of Achilles tendon ruptures occur and why? A: 2-6cm proximal to the calcaneal insertion in the watershed zone. This area has the poorest blood supply as it lies between the proximal blood supply from the musculotendinous junction and the distal blood supply from the calcaneal insertion. The tendon also narrows and twists in this region, creating mechanical stress concentration.
Q: Describe the Thompson test and its interpretation. A: Patient is positioned prone with knee flexed to 90 degrees. The examiner squeezes the mid-calf (gastrocnemius muscle belly) firmly. Normal response: ankle plantarflexes. Positive test (rupture): no plantarflexion occurs. The test has 96% sensitivity and 93% specificity. Must compare to contralateral side and ensure patient is relaxed (not voluntarily plantarflexing).
Q: What are the re-rupture rates for operative versus non-operative treatment? A: Operative (open repair): 3-5% re-rupture rate. Non-operative with modern functional rehabilitation: 7-10% re-rupture rate. Traditional cast immobilization has 10-15% re-rupture. While operative has lower re-rupture, it carries infection risk (3-5%) and sural nerve injury risk (10-15%). Functional outcomes at 1-2 years are similar between operative and non-operative with modern protocols.
Q: Why is medial approach preferred over posterolateral for Achilles repair? A: The sural nerve runs posterolateral to the Achilles tendon and is at high risk (10-15% injury rate) with posterolateral approach. Medial approach (1-2cm medial to lateral tendon border) avoids the sural nerve while providing adequate exposure. Medial approach also has better wound healing as it avoids the posterior midline which is under tension with dorsiflexion.
Q: What is the DVT rate in Achilles rupture and how should it be prevented? A: 6-8% DVT rate without prophylaxis due to prolonged immobilization and calf muscle injury. Prevention strategies include: LMWH (enoxaparin 40mg daily) for high-risk patients (age over 40, obesity, previous DVT, non-operative treatment), early functional mobilization in boot rather than cast immobilization, and early weight bearing as tolerated. Continue prophylaxis until fully weight bearing (typically 4-6 weeks).
Q: What is the relationship between fluoroquinolone antibiotics and Achilles rupture? A: Fluoroquinolones are associated with an increased risk of Achilles rupture (systematic review by Stephenson et al, Drug Saf 2013 - reported odds ratios ranging from 1.1 to 7.1). Highest risk is in the first month of use, with increased risk in patients over 60 years and those on concomitant corticosteroids. Regulators (FDA and others) have issued tendon-rupture warnings for this class. The proposed mechanism involves matrix metalloproteinase upregulation leading to tendon degeneration. Consider alternative antibiotics in patients with existing tendinopathy or high activity levels.
Guidelines, Registries & Global Practice
Global Epidemiology
| Parameter | Reported Figure | Source / Evidence |
|---|---|---|
| Incidence | Approximately 27-31 per 100,000 per year (Denmark, 1994-2013) | Nationwide registry of 33,160 patients (Ganestam et al, KSSTA 2015) |
| Sex ratio and age | Male:female 3:1; mean age approximately 44-45 years | Same Danish nationwide registry |
| Trend over time | Rising overall incidence, driven by patients over 50 years | Registry data; ageing, more recreational sport |
| Treatment trend | Marked decline in surgical treatment (16.9 to 6.3 per 100,000 1994-2013) | Shift following high-quality RCTs favouring functional non-operative care |
According to PubMed, the Danish nationwide registry of 33,160 patients documented a steady decline in surgical treatment between 1994 and 2013, accelerating after 2009. This mirrors a global shift in practice driven by landmark RCTs (Willits 2010) and meta-analyses (Soroceanu 2012) showing that non-operative care with early functional rehabilitation matches surgical re-rupture rates while avoiding wound and nerve complications.
Guideline and Society Positions
| Body (region) | Position on Operative vs Non-Operative | Rehabilitation / Other | Evidence Basis |
|---|---|---|---|
| AAOS (USA) | No clear superiority of one approach; shared decision-making | Early functional rehabilitation supported | Clinical practice guideline - mostly moderate/limited strength recommendations |
| BOA / BOFAS (UK) | Non-operative functional management acceptable as default for most patients | Standardised functional rehabilitation pathways encouraged | Consensus informed by UK RCTs and meta-analyses |
| AO Foundation (international) | Operative repair reserved for selected/high-demand or open injuries | Emphasis on accurate length restoration and early motion | Expert consensus plus level-I evidence |
| Sports-medicine / elite-athlete practice (global) | Lower threshold for operative repair in high-demand athletes | Accelerated, supervised, sport-specific rehabilitation | Lower-level cohort evidence; individualised |
- No dedicated arthroplasty registry applies (AOANJRR, NJR and AJRR cover joint replacement only - Achilles rupture is not an implant procedure)
- National hospital/patient registries (e.g. Danish, Swedish, Finnish) provide the best population-level data on incidence and treatment trends
- Registry data consistently show rising incidence in older patients and a declining surgical rate as functional non-operative protocols are adopted
- High-volume / metropolitan and sports-medicine centres: higher operative rates, especially for athletes
- Regional and lower-resource settings: greater reliance on non-operative functional bracing
- Convergence point: regardless of operative or non-operative choice, early controlled mobilisation in a functional orthosis is now standard and is the single biggest driver of improved outcomes
- Thromboprophylaxis: practice varies internationally; many units use LMWH during the immobilised, non-weight-bearing phase given the documented venous thromboembolism risk
Key documentation requirements:
Missed diagnosis litigation:
- 20-25% of Achilles ruptures initially missed
- Document Thompson test performance
- Document differential diagnosis considered
- Document patient counseling about diagnosis and treatment options
Consent discussion must include:
- Re-rupture rates (operative 3-5%, non-operative 10-15%)
- Infection risk (3-5% operative)
- Sural nerve injury risk (10-15% posterolateral approach, under 5% medial approach)
- DVT/PE risk (2-8% depending on prophylaxis)
- Weakness and stiffness (10-30% subjective)
- Prolonged recovery (6-12 months to sport return)
Common litigation issues:
- Delayed diagnosis (emergency department misses - called "ankle sprain")
- Sural nerve injury (if posterolateral approach used)
- Re-rupture (if patient non-compliant or protocol not followed)
- DVT/PE (if prophylaxis not offered to high-risk non-operative patients)
Protective documentation:
- Detailed examination findings including Thompson test result
- Clear documentation of operative vs non-operative discussion
- Informed consent form signed
- Rehabilitation protocol provided in writing
- Regular follow-up with milestone assessments documented
Key Anatomy
- Largest and strongest tendon - can generate forces up to 12 times body weight
- Watershed zone 2-6cm proximal to insertion = poorest blood supply = 80% of ruptures
- Blood supply from musculotendinous junction (proximal) and calcaneal insertion (distal)
- Sural nerve runs posterolateral - at risk with posterolateral surgical approach (10-15%)
Clinical Diagnosis
- Thompson test = gold standard (sensitivity 96%, specificity 93%)
- Palpable gap 2-6cm proximal to insertion (pathognomonic)
- Pop sensation and felt kicked from behind (classic history)
- Cannot perform single leg heel raise
- 20-25% missed initially - patient can still walk (toe flexors provide residual function)
Classification and Treatment
- Acute (under 4 weeks) = primary end-to-end repair or conservative
- Chronic (over 4 weeks) = augmentation required (FHL transfer, V-Y, turndown)
- Gap under 2cm = primary repair; over 2cm = augmentation needed
- Operative vs non-operative: similar functional outcomes, operative lower re-rupture (3-5% vs 10-15%)
Surgical Pearls
- Medial approach preferred (avoids sural nerve posterolateral)
- Krackow locking whipstitch with number 2 non-absorbable braided suture
- Test passive dorsiflexion before tying (should achieve 10-15 degrees to avoid over-tightening)
- Compare to contralateral length to avoid over-lengthening (causes permanent weakness)
- FHL transfer is preferred augmentation (in-phase, good strength, low morbidity)
Complications
- Re-rupture: operative 3-5%, non-operative 10-15% (devastating if occurs)
- Sural nerve injury: 10-15% posterolateral approach, under 5% medial approach
- Infection: 3-5% operative (deep infection rare under 1%)
- DVT: 6-8% without prophylaxis (LMWH for high risk, early mobilization)
- Weakness: 10-30% subjective at 1 year (expect 80-90% strength recovery)
Key Evidence and Rehabilitation
- Early functional mobilization reduces re-rupture vs traditional cast (7% vs 15%)
- Fluoroquinolones increase rupture risk 3-fold (FDA black box warning)
- Return to sport: 6-9 months minimum (need 80% contralateral strength)
- Operative protocol: Boot at 2 weeks, full weight bearing by 6 weeks, jogging at 3 months
- Weekend warrior profile: male 30-50 years, eccentric loading during push-off (basketball, tennis)