Talus Tibia Fibula | Urgent Reduction | Associated Fractures
- Ankle dislocations = talus displaced from mortise (tibia-fibula) - usually associated with fractures, urgent reduction required
- Posterior most common - Talus displaced posteriorly, usually with posterior malleolus fracture
- Urgent reduction required - Skin tension causes necrosis, neurovascular compromise, reduce within hours
- Usually associated fractures - Ankle fractures (malleoli), talus fractures, or both
- ORIF if fractures present - After reduction, address associated fractures with ORIF
- “Posterior most common, usually with fractures
- “Urgent reduction required
- “Usually associated fractures
- “ORIF if fractures present

Urgent reduction required - Skin tension causes necrosis within hours, neurovascular compromise. Reduce within hours, do not delay for imaging. Document neurovascular status before and after reduction.
Ankle dislocations usually associated with fractures - Malleolar fractures, talus fractures, or both. After reduction, assess fractures and perform ORIF if indicated. CT scan after reduction to assess fractures.
Posterior dislocation most common - Talus displaced posteriorly, usually with posterior malleolus fracture. Reduction: traction, plantarflex, then dorsiflex. Success rate 80-85%.
ORIF if fractures present - After reduction, address associated fractures with ORIF. Malleolar fractures require ORIF if displaced. Talus fractures require ORIF if displaced. Success rate 75-85%.
- Frequency
- Most common, usually with fractures
- Treatment
- Closed reduction, ORIF
- Outcome
- 75-85% good results
- Frequency
- Rare, usually with fractures
- Treatment
- Closed reduction, ORIF
- Outcome
- 75-85% good results
- Frequency
- Rare, usually with fractures
- Treatment
- Closed reduction, ORIF
- Outcome
- 70-80% good results
- Frequency
- Rare, usually with fractures
- Treatment
- Closed reduction, ORIF
- Outcome
- 70-80% good results
FRACTUREAssociated Fractures
Hook:FRACTURE: Fractures usually associated, Reduction first, Assess fractures, CT after reduction, Treatment ORIF if needed, Urgent reduction, Reduction first, Examine fractures!
Overview and Epidemiology
Ankle dislocations are rare but serious injuries where the talus is displaced from the mortise (tibia-fibula). These dislocations are usually associated with fractures and require urgent reduction.
Definition
Ankle dislocation: Displacement of talus from mortise (tibia-fibula), which:
- Location: Tibiotalar joint
- Mechanism: High-energy trauma
- Treatment: Urgent reduction, then ORIF if fractures
- Outcome: Good with proper treatment
Types:
- Posterior: Most common, talus posterior
- Anterior: Rare, talus anterior
- Lateral: Rare, talus lateral
- Medial: Rare, talus medial
Epidemiology
- Incidence: Less than 1% of ankle injuries
- Age: Peak 20-40 years (trauma population)
- Gender: No clear predominance
- Mechanism: High-energy trauma (MVA, falls)
- Associated injuries: Ankle fractures (malleoli), talus fractures
Urgent reduction required - Skin tension causes necrosis within hours, neurovascular compromise. Reduce within hours, do not delay for imaging. Document neurovascular status before and after reduction.
Anatomy and Pathophysiology
Ankle Anatomy
Mortise:
- Tibia: Medial malleolus, plafond
- Fibula: Lateral malleolus
- Talus: Fits in mortise
- Ligaments: Deltoid, lateral ligaments, syndesmosis
Neurovascular structures:
- Posterior tibial artery: Behind medial malleolus
- Tibial nerve: With artery
- Anterior tibial artery: Anterior
- Deep peroneal nerve: With artery
Pathophysiology
Injury mechanism:
- High-energy trauma: MVA, falls from height
- Forces: Axial loading, rotation, translation
- Fractures: Usually associated (malleoli, talus)
Why urgent reduction:
- Skin tension: Causes necrosis within hours
- Neurovascular compromise: Risk of ischemia
- Soft tissue damage: Progressive with time
Why fractures usually associated:
- High-energy mechanism: Causes fractures
- Instability: Fractures contribute to instability
- ORIF required: After reduction, address fractures
Classification Systems
Direction-Based Classification

Posterior:
- Most common
- Talus posterior
- Usually with posterior malleolus fracture
- Treatment: Closed reduction, ORIF
Anterior:
- Rare
- Talus anterior
- Usually with anterior malleolus fracture
- Treatment: Closed reduction, ORIF
Lateral:
- Rare
- Talus lateral
- Usually with lateral malleolus fracture
- Treatment: Closed reduction, ORIF
Medial:
- Rare
- Talus medial
- Usually with medial malleolus fracture
- Treatment: Closed reduction, ORIF
Direction guides reduction technique.
Clinical Assessment
History
Symptoms:
- Ankle pain: Severe pain
- Deformity: Obvious deformity
- Inability to weight bear: Cannot bear weight
- Mechanism: High-energy trauma
Risk factors:
- High-energy trauma
- MVA, falls from height
- Sports injuries
Physical Examination
Inspection:
- Obvious deformity
- Swelling
- Skin tenting (urgent reduction)
- Open wound (if open)
Palpation:
- Tenderness over ankle
- Crepitus (if fractures)
- Deformity
Neurovascular:
- Document before reduction: Critical
- Pulses: Dorsalis pedis, posterior tibial
- Sensation: Dorsal and plantar foot
- Motor: Ankle dorsiflexion, plantarflexion
Range of Motion:
- Ankle ROM limited and painful
- Cannot test due to pain
Document neurovascular status before reduction - Critical for medicolegal and clinical reasons. Check pulses (dorsalis pedis, posterior tibial), sensation (dorsal and plantar foot), and motor function (ankle dorsiflexion, plantarflexion). Repeat after reduction.
The Pulseless Foot: Managing Vascular Compromise
The topic repeatedly stresses documenting the neurovascular status before and after reduction, but what to actually do about a dysvascular foot is the examinable next step.
- A dysvascular foot before reduction is an indication for immediate reduction, not a reason to wait. Gross displacement kinks, stretches or tents the anterior and posterior tibial vessels; restoring alignment is itself the first-line vascular treatment and usually returns perfusion. This is why a deformed, pulseless ankle is reduced at the point of care before definitive imaging.
- Reassess perfusion immediately after reduction - pulses (dorsalis pedis, posterior tibial), capillary refill, colour and Doppler signals. If perfusion returns, splint in the reduced position and monitor closely.
- A foot that remains pulseless or ischaemic despite confirmed anatomic reduction is a limb-threatening emergency. Do not attribute it to spasm and wait: involve vascular surgery urgently, obtain on-table angiography (or CT angiography if it will not delay revascularisation), and exclude an intimal tear, arterial entrapment or transection. Warm-ischaemia time drives the salvage window.
- Anticipate reperfusion sequelae - after a period of ischaemia or a high-energy mechanism, maintain a low threshold for leg and foot compartment syndrome and monitor accordingly.
A dysvascular deformed ankle is reduced immediately - realignment is the first vascular manoeuvre and usually restores flow. If the foot stays pulseless after anatomic reduction, treat it as a surgical emergency: urgent vascular surgery involvement, on-table/CT angiography to find an intimal tear or entrapment, and vigilance for compartment syndrome. Never wait on a persistently ischaemic foot.
Investigations
Standard X-ray Protocol
AP view:
- Shows dislocation
- Assess mortise
- Check for fractures
Lateral view:
- Shows dislocation direction
- Assess talus position
- Check for fractures
Mortise view:
- Shows mortise alignment
- Assess syndesmosis
- Check for fractures
Key point: Do not delay reduction for imaging if skin compromised.
Differential Diagnosis
The deformed, painful hindfoot has several mimics. Distinguishing them changes the reduction manoeuvre and the structure at risk.
- Key distinguishing feature
- Talus displaced within/from the mortise, malleoli usually fractured
- Imaging clue
- Talus malaligned to plafond on lateral; widened mortise
- Pitfall
- Most are fracture-dislocations - search every malleolus
- Key distinguishing feature
- Talus stays in mortise; calcaneus/navicular displaced beneath it
- Imaging clue
- Talonavicular/subtalar incongruity, normal tibiotalar joint
- Pitfall
- Beware locked medial dislocation needing open reduction
- Key distinguishing feature
- Whole talus dislocated out of all three joints, often open
- Imaging clue
- Empty talar bed
- Pitfall
- High AVN and infection risk; preserve and replant where feasible
- Key distinguishing feature
- Mortise broadly maintained, talus congruent
- Imaging clue
- Malleolar fracture without gross talar displacement
- Pitfall
- Subtle talar shift still needs anatomic reduction
- Key distinguishing feature
- Fracture line through talus; may coexist with dislocation
- Imaging clue
- Hawkins lines, fracture through talus on CT
- Pitfall
- Misreading as pure dislocation delays AVN-relevant fixation
Management Algorithm
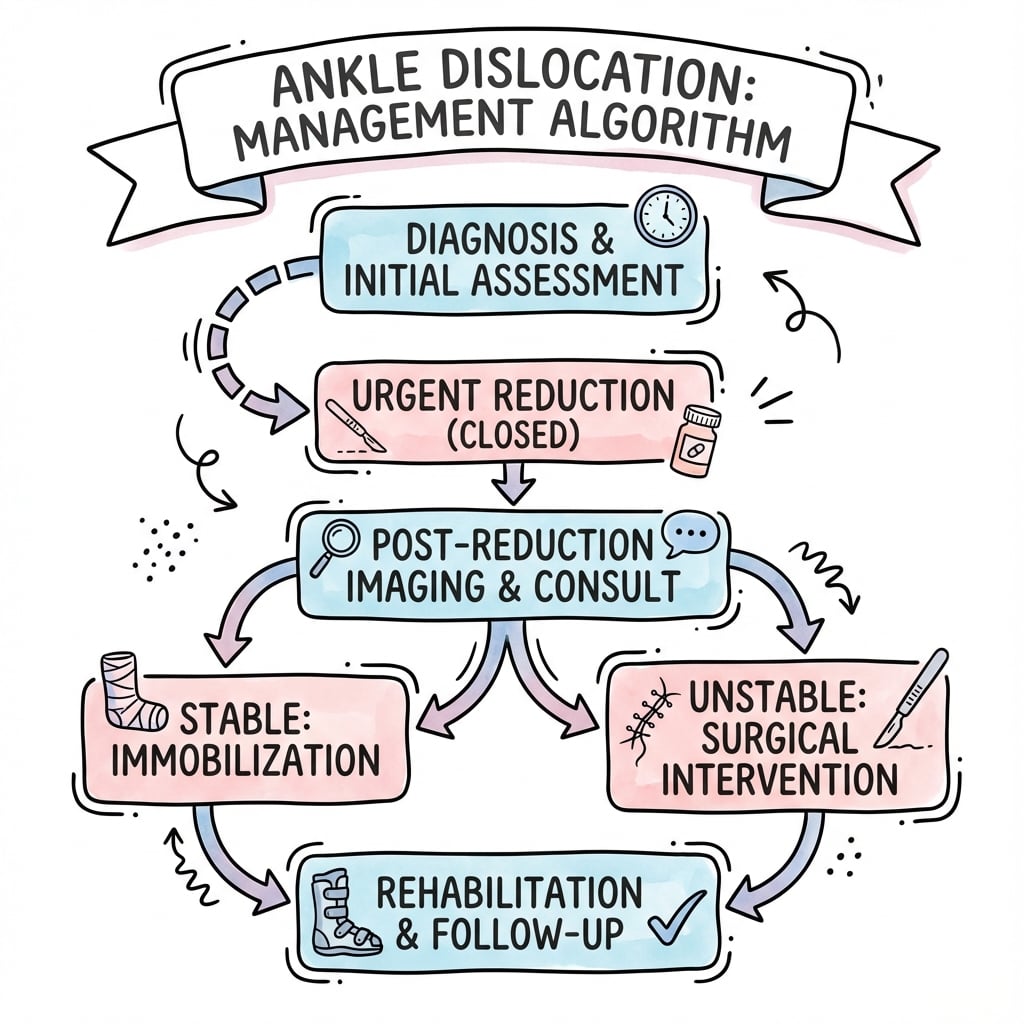
Management Pathway
Ankle Dislocation Management
Diagnose ankle dislocation clinically and radiographically. Document neurovascular status before reduction. Do not delay reduction for imaging if skin compromised. Urgent reduction required within hours.
Closed reduction under sedation or general anesthesia - Flex knee to relax gastrocnemius, traction, then reverse deformity (posterior: plantarflex then dorsiflex, anterior: dorsiflex then plantarflex). Document neurovascular status after reduction. Success rate 80-85%.
CT scan after reduction to assess associated fractures - 80-90% have associated fractures (malleoli, talus, or both). Assess displacement and plan ORIF if indicated.
ORIF if fractures present and displaced - Malleolar fractures require ORIF if displaced. Talus fractures require ORIF if displaced. Restore mortise stability. Success rate 75-85%.
Surgical Technique
Anterolateral Approach
Indication: Exposure of lateral malleolus, talus neck, and anterolateral joint.
- Incision: Longitudinal over the fibula, curving anteriorly.
- Internervous Plane: Between superficial peroneal nerve and sural nerve (distally).
- Structures at Risk: Superficial peroneal nerve, intermediate dorsal cutaneous nerve.
Posterolateral Approach
Indication: Fixation of posterior malleolus and syndesmotic stabilization.
- Incision: Midway between Achilles tendon and posterior border of fibula.
- Internervous Plane: Between peroneus brevis (S1/L5) and flexor hallucis longus (S1/L2).
- Structures at Risk: Sural nerve, small saphenous vein.

REDUCEReduction Technique
Hook:REDUCE: Reduction urgent, Emergency within hours, Document neurovascular, Urgent do not delay, CT after reduction, Examine fractures!
The Dimple Sign and the Irreducible Dislocation
The topic's own failed-reduction viva asks "what is the dimple sign?" - it is the clinical marker of an irreducible dislocation and deserves definition.
- What it is. The dimple sign is a persistent puckering or dimpling of the skin over the deformity (classically over the antero- or infero-lateral ankle) that fails to efface with longitudinal traction. It indicates that the displaced talus or its head has buttonholed through a rent in the capsule/retinaculum and tethered the invaginated overlying skin into the joint.
- Why it matters. A dimple that persists after a controlled closed attempt is a sign of an irreducible dislocation - it predicts blocked reduction and warns that continued forceful manipulation will cause pressure necrosis of the tethered skin (converting a closed injury to open) and further chondral or neurovascular damage.
- What blocks the reduction. Recognised interposed structures are the posterior tibial tendon, the flexor tendons (flexor hallucis longus / flexor digitorum longus), the deltoid ligament, or an interposed osteochondral fragment; the culprit tends to lie on the side opposite the direction of talar displacement.
- What to do. A persistent dimple or a failed single gentle attempt mandates prompt open reduction through an approach directed at the likely block, releasing the entrapped structure under direct vision - not repeated forced closed manipulation.
Q: What is the dimple sign and what does it tell you? A: A skin dimple/pucker over the deformity that does not efface with traction - the talus has buttonholed through the soft tissues and tethered the skin, signalling an irreducible dislocation. Interposed posterior tibial tendon, FHL/FDL, deltoid ligament or an osteochondral fragment blocks reduction. Proceed to open reduction; do not force, or the tethered skin will necrose.
ANKLEAnkle Dislocation Features
Hook:ANKLE: Ankle dislocation, Neurovascular check, Knee flexed, Lateral rare, Emergency reduction!
Complications
- Incidence
- 30-40%
- Risk Factors
- Displacement, inadequate reduction
- Prevention/Management
- Anatomic reduction, adequate fixation
- Incidence
- 10-15%
- Risk Factors
- Talus fractures, delayed reduction
- Prevention/Management
- Early reduction, anatomic fixation
- Incidence
- 20-30%
- Risk Factors
- Prolonged immobilization
- Prevention/Management
- Early motion, adequate fixation
- Incidence
- 5-10%
- Risk Factors
- Displacement, inadequate fixation
- Prevention/Management
- Rigid fixation
Post-Traumatic Arthritis
30-40% incidence:
- Cause: Displacement, inadequate reduction, joint damage
- Prevention: Anatomic reduction, adequate fixation
- Management: Ankle fusion or arthroplasty if severe
AVN Talus
10-15% incidence (if talus fractures):
- Cause: Talus fractures, delayed reduction, tenuous blood supply
- Prevention: Early reduction, anatomic fixation
- Management: Monitor with serial imaging, fusion if collapse
Postoperative Care

Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Ankle ROM and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- CT to confirm healing
- Cast removal if healing
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
Closed reduction (pure dislocation):
- Success rate: 80-85% (stability, pain relief)
- Functional outcomes: 75-80% return to pre-injury level
- Arthritis: 20-30% develop arthritis
ORIF (with fractures):
- Success rate: 75-85% (union, pain relief)
- Functional outcomes: 70-75% return to pre-injury level
- Arthritis: 30-40% develop arthritis
Open injuries:
- Success rate: 60-70% (union, pain relief)
- Functional outcomes: 60-70% return to pre-injury level
- Arthritis: 40-50% develop arthritis
Long-Term Prognosis
Arthritis progression:
- With proper treatment: 30-40% develop arthritis
- Without treatment: 50-60% develop arthritis
- Risk factors: Displacement, inadequate reduction, open injury
Guidelines, Registries & Global Practice
Global Epidemiology
- Pure ankle (tibiotalar) dislocation without fracture is exceptionally rare - approximately 0.46% of ankle dislocations and 0.065% of all ankle injuries (Wight et al, Injury 2017).
- High-energy talar and ankle dislocation-fractures cluster in young men (over 80% male, mean age early 30s) after motor-vehicle accidents and falls (Vosoughi et al, BMC MSD 2021).
- Around half of pure dislocations present as open injuries, reflecting the high energy and thin soft-tissue envelope.
Side-by-Side Guidance
- Emphasis
- Open fracture & soft-tissue pathways, urgent realignment
- Practical message
- Realign and splint deformed/dysvascular limbs immediately; photograph and cover open wounds, early IV antibiotics
- Emphasis
- Anatomic mortise restoration, staged fixation
- Practical message
- Span with external fixator if soft tissues are compromised; definitive ORIF once swelling settles
- Emphasis
- Ankle fracture management, syndesmosis assessment
- Practical message
- Restore fibular length/rotation and syndesmosis; intra-operative stress testing
- Emphasis
- Limb-threatening emergency
- Practical message
- Reduce a dislocated, dysvascular ankle at point of care before definitive imaging
Registry & Resource-Setting Notes
- No dedicated dislocation registry exists; long-term implant and OA data come from ankle-fracture and syndesmosis cohorts (e.g. the Oulu RCT, Lehtola et al 2021) and national fracture audits.
- High-resource settings: prompt theatre access enables early definitive ORIF; CT is routine after reduction.
- Limited-resource settings: closed reduction with splint/external fixation and delayed or definitive cast management may be the pragmatic pathway; the universal, transferable principle is immediate reduction to protect skin and the neurovascular bundle.
Ankle dislocations are a common viva topic. Know that urgent reduction is required (within hours, skin necrosis risk), that they are usually associated with fractures (most series 80-90%), that posterior displacement is most common, that ORIF follows for displaced fractures, and that neurovascular status must be documented before and after reduction. Be prepared to discuss the reduction technique and the management of associated fractures.
Controversies and Areas of Uncertainty
Whether to acutely repair the lateral/deltoid ligament complex after a pure dislocation is debated. The largest systematic review found instability was rare (2.6%) and was not reduced by acute repair, supporting functional treatment for most stable injuries.
In dislocation-fractures with a compromised soft-tissue envelope, the trade-off between spanning external fixation (protect skin, stage definitive surgery) and immediate ORIF is judgement-based, guided by skin condition and swelling rather than fixed rules.
"Reduce within hours" is universally accepted, but a precise time threshold beyond which chondral and skin injury becomes irreversible is not established by high-level human data - hence the principle of immediate point-of-care reduction.
When a talar fracture coexists, AVN risk is real but the value of restricted weight-bearing and the reliability of the Hawkins sign for predicting revascularisation remain debated; serial imaging guides decisions.
MCQ Practice Points
Q: Why is urgent reduction required for ankle dislocations? A: Skin tension causes necrosis within hours, neurovascular compromise - Reduce within hours, do not delay for imaging if skin compromised. Document neurovascular status before and after reduction.
Q: Are ankle dislocations usually associated with fractures? A: Yes, 80-90% have associated fractures - Malleolar fractures most common, talus fractures less common. After reduction, assess fractures with CT and perform ORIF if displaced.
Q: What is the most common type of ankle dislocation? A: Posterior dislocation is most common - Talus displaced posteriorly, usually with posterior malleolus fracture. Reduction: traction, plantarflex, then dorsiflex. Success rate 80-85%.
Q: What is the treatment for ankle dislocations? A: Urgent closed reduction, then ORIF if fractures present - Reduce within hours, document neurovascular status, CT after reduction to assess fractures, ORIF if displaced. Success rate 75-85% with proper treatment.
Q: What are the complications of ankle dislocations? A: Post-traumatic arthritis (30-40%), AVN talus (10-15% if talus fractures), stiffness (20-30%) - Prevent with anatomic reduction and adequate fixation. Success rate 75-85% with proper treatment.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old patient presents with ankle deformity after high-energy trauma. X-rays show posterior ankle dislocation with associated posterior malleolus fracture. Skin is tented but intact.”
“A 40-year-old patient has an open ankle dislocation with exposed talus. The examiner asks you to explain your management approach.”
“You are in the ED attempting to reduce a lateral ankle dislocation. Despite adequate sedation and correct technique, the talus will not 'clunk' back into the mortise. What are your next steps?”
Key Concepts
- Rare but serious injuries (less than 1% of ankle injuries)
- Urgent reduction required within hours (skin necrosis risk)
- Usually associated with fractures (80-90%)
- ORIF if fractures present (75-85% good results)
Classification
- Posterior: Most common, talus posterior - closed reduction (80-85% good results)
- Anterior: Rare, talus anterior - closed reduction (75-85% good results)
- Lateral: Rare, talus lateral - closed reduction (70-80% good results)
- Medial: Rare, talus medial - closed reduction (70-80% good results)
Treatment
- Urgent closed reduction: Within hours, document neurovascular status
- CT after reduction: Assess associated fractures (80-90% have fractures)
- ORIF if fractures displaced: Malleoli or talus (75-85% good results)
- Pure dislocation: Conservative if stable (80-85% good results)
Surgical Technique
- Reduction: Flex knee, traction, reverse deformity
- ORIF malleoli: Medial, lateral, or posterior approach
- ORIF talus: Anterior, medial, or lateral approach
- Verify reduction fluoroscopically
Complications
- Post-traumatic arthritis: 30-40% (prevent with anatomic reduction)
- AVN talus: 10-15% if talus fractures (prevent with early reduction)
- Stiffness: 20-30% (prevent with early motion)
- Nonunion: 5-10% (prevent with rigid fixation)
Evidence Base
Dislocation is a risk factor for poor outcome after SER ankle fractures
- 32% of operative SER IV fractures presented with dislocation
- Dislocation significantly reduced accuracy of articular reduction (p=0.003)
- Higher rates of open fracture and external fixator use in the dislocation group
- Worse ankle and subtalar ROM and FAOS scores at follow-up; infection rates not increased
Patterns and characteristics of talar injuries at two trauma centres
- 86.4% male, mean age 31.8 years - a young high-energy trauma population
- MVA (46.1%) and falls (43.3%) were the leading mechanisms
- Talar body fractures (21.9%) slightly more common than neck (19.2%)
- Medial malleolus, fibula and calcaneus were the commonest associated fractures