The Sentinel of the Shoulder
- Originates from Posterior Cord (with Radial nerve)
- Passes through Quadrangular Space with PCHA
- Divides into Anterior (Motor) and Posterior (Mixed) branches
- Anterior Branch wraps horizontally around humerus (5-7cm from acromion)
- Sensory: 'Regimental Badge' area (Upper Lateral Cutaneous Nerve of Arm)
- “Most commonly injured nerve in shoulder dislocation
- “Teres Minor is the first muscle recovered (Posterior Branch)
- “Deltoid extension lag is a sign of Axillary palsy (often missed)
- “Nerve Transfer: Triceps branch to Axillary is the gold standard salvage
- Supplies
- Shoulder Joint Capsule
- Course
- Quadrangular Space
- Injury Risk
- Dislocation / QSS
- Supplies
- Deltoid (Ant/Mid)
- Course
- Winds around surgical neck
- Injury Risk
- Deltoid Splitting / #PH
- Supplies
- Teres Minor + Deltoid (Post)
- Course
- Deep to Deltoid
- Injury Risk
- Retraction injury
- Supplies
- Skin over deltoid
- Course
- Pierces deep fascia
- Injury Risk
- Sensory loss only
TAM-hum-triQuadrangular Space Boundaries
Hook:The Teres sandwich with Humerus and Triceps bread.
BADGERegimental Badge
Hook:Soldiers wear the badge where the sensation is lost.
Overview
The Axillary Nerve is a terminal branch of the Posterior Cord. It provides motor function to the Deltoid and Teres Minor, critical for shoulder abduction and external rotation. Its course around the surgical neck of the humerus makes it highly vulnerable in trauma.
Neurovascular

Origin
- Posterior Cord of Brachial Plexus (C5, C6).
- Lies posterior to the Axillary Artery.
- Located on the surface of Subscapularis.
Course
- Runs inferiorly and laterally.
- Exits axilla through the Quadrangular Space.
- Travels with the Posterior Circumflex Humeral Artery (PCHA).
- Winds posteriorly around the Surgical Neck of the Humerus.
This course explains the high risk during inferior capsule release.

SITSRotator Cuff Innervation
Hook:Axillary only supplies the MINOR Teres.
Classification Systems
Seddon Classification (1943)
- Neuropraxia: Conduction block. No structural damage. Expect full recovery.
- Axonotmesis: Axon interruption. Sheath intact. Wallerian degeneration occurs. Recovery 1mm/day.
- Neurotmesis: Complete transection. No recovery without surgery.
This system is universally used for nerve injuries.
Clinical Assessment
- Deltoid: Abduction (check greater than 90 deg, as Supraspinatus does 0-30). Also Extension (Post Deltoid).
- Teres Minor: External Rotation (Hornblower's Sign).
- Look for "Swallow Tail" sign on extension (lag of posterior deltoid).
- Regimental Badge: Area over the middle deltoid.
- Supplied by Superior Lateral Cutaneous Nerve (branch of Posterior division).
- Sensation may be preserved even with motor injury (incomplete palsy).
Differential Diagnosis
- Weakness
- Deltoid/Teres Minor
- Sensory Loss
- Regimental Badge
- Key Feature
- Hx of Trauma/Dislocation
- Weakness
- Deltoid + Biceps
- Sensory Loss
- C5 Dermatome (Thumb)
- Key Feature
- Neck Pain, Biceps Reflex loss
- Weakness
- Supraspinatus (Abd)
- Sensory Loss
- None (usually)
- Key Feature
- Painful Arc, Weak ER
- Weakness
- Patchy / Severe Pain
- Sensory Loss
- Variable
- Key Feature
- Viral prodrome, profound waste
Investigations
MRI Shoulder
- Acute: Identify edema in Deltoid/Teres Minor (denervation edema).
- Chronic: Fatty infiltration and atrophy.
- Quadrangular Space: Visualize space-occupying lesions (Paralabral cyst, Lipoma) compressing the nerve.
- Hypertrophy: Teres Minor hypertrophy is a sign of chronic rotator cuff tear (compensation), NOT axillary nerve path.
MRI is also crucial for excluding rotator cuff tears in elderly patients.
Management Algorithm

Trauma (Dislocation/#)
- Closed Injuries: 80-90% are neuropraxia and recover spontaneously.
- Protocol:
- Reduce shoulder gently.
- Re-examine nerve.
- Physio (Range of motion).
- NCS at 3-4 weeks if complete palsy.
- Repeat NCS at 3 months.
- Surgery: If no recovery by 3-6 months → Exploration / Graft / Transfer.
Timing is critical for successful re-innervation.
Treatment Summary
- Timeframe
- Day 0
- Action
- Reduce, Confirm Neuro status
- Timeframe
- Week 3-4
- Action
- EMG to baseline. Physio.
- Timeframe
- Month 3-4
- Action
- Repeat EMG. If denervation + no MUAPs → Plan Surg
- Timeframe
- Month 4-6
- Action
- Neurolysis vs Graft vs Transfer
Surgical Technique
Posterior Approach
- Incision: Vertical incision over posterior deltoid border.
- Interval: Deltoid (Axillary) and Triceps (Radial).
- Landmark: Teres Major (Inferior border of Q-Space).
- Identify: Axillary nerve emerging from Quadrangular Space.
- Action: Neurolysis (release bands) or Sural Graft.
The key landmark is the Teres Major muscle belly inferiorly.
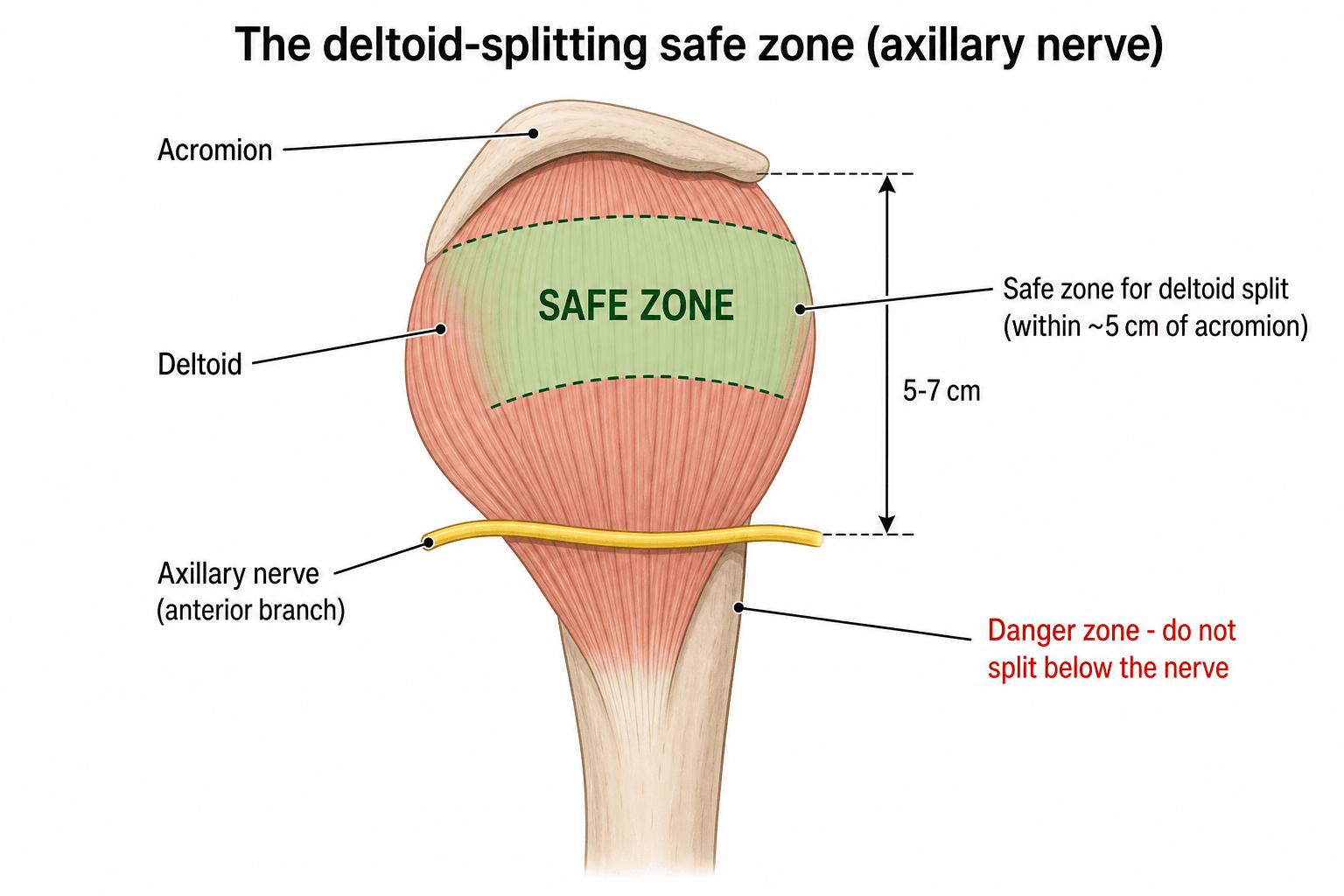
In the Deltoid Splitting Lateral Approach, the axillary nerve runs horizontally approx 5-7 cm distal to the acromion.
- Stay within 5cm of the acromion to stay safe.
- If extending distally, palpate the nerve or peel deltoid from insertion.
- The "Safe Zone" is shorter in smaller patients!
Beyond the deltoid-splitting safe zone, the axillary nerve is the structure most at risk during inferior glenohumeral surgery, because it runs immediately beneath the inferior capsule (the axillary pouch):
- The nerve lies closest to the glenoid rim at the 5- to 7-o'clock (inferior) position, only about 10 to 15 mm from the capsule/labrum — the danger zone for Bankart suture-anchor placement, inferior capsular shift and capsular release.
- Thermal / electrocautery capsulorrhaphy of the inferior capsule has caused axillary-nerve injury, as heat conducts through the thin pouch; the nerve is more vulnerable here than anywhere else arthroscopically.
- Protective measures: remember arm position changes the gap (abduction increases the capsule-to-nerve distance), stay intracapsular, place inferior anchors with care, and limit thermal energy near the 6-o'clock position.
Complications
- Shoulder stiffness: Adhesive capsulitis from prolonged immobilization.
- Fail to recover: Permanent deltoid wasting.
- Donor site morbidity: Sural nerve (numb foot), Triceps weakness (rare grade 4).
- Neuroma: Painful neuroma in continuity.
Early identification of stiffness is key.
Rehabilitation Protocol
- Timeframe
- 0-3 Weeks
- Goals
- Sling, Pendulums
- Precautions
- No Active Abduction
- Timeframe
- 3-8 Weeks
- Goals
- Gravity eliminated abduction
- Precautions
- Observe Scapular rhythm
- Timeframe
- 8+ Weeks
- Goals
- Deltoid strengthening
- Precautions
- Full ROM
Specific Exercises
- Gravity Eliminated: Lying supine or on side, sliding arm.
- Scapular Setting: Crucial to prevent "hitching" compensation.
Prognosis
- Spontaneous Recovery: 80-90% of dislocation-associated palsies recover by 3-6 months.
- Surgical Repair: Direct repair outcomes are better than graft.
- Nerve Transfer: Triceps to Axillary yields M4 strength in over 85% of patients.
- Quality of Life: Persistent deltoid weakness is well tolerated if Rotator Cuff is intact (Supraspinatus compensation).
Guidelines, Registries & Global Practice
Global Epidemiology
- Anterior glenohumeral dislocation has an incidence of roughly 15-25 per 100,000 person-years, with a bimodal distribution (young athletic males, older females after falls).
- In a prospective electrophysiological study of primary shoulder dislocations and humeral neck fractures, evidence of nerve injury was found in 45% of patients, most involving the axillary, suprascapular, radial and musculocutaneous nerves; injury was significantly more common in older patients and those with a haematoma. The axillary nerve is the single most frequently injured.
- Most lesions are traction neuropraxia or axonotmesis; the large majority recover partially or completely within four months, with persistent motor loss in a small minority.
Side-by-Side Guidance
- Emphasis
- Document neurovascular status pre- and post-reduction; baseline EMG at 3-4 weeks
- Practical Point
- Early referral for nerve transfer if no recovery by 3-6 months
- Emphasis
- Reduce promptly; structured rehab; MRI in over-40s to exclude associated cuff tear
- Practical Point
- Peripheral nerve injury MDT referral for persistent palsy
- Emphasis
- Anterolateral deltoid-splitting approach with axillary-nerve protection; stay near the acromion
- Practical Point
- Identify and protect the nerve when extending distally for plating
- Emphasis
- Neurophysiology-guided timing; reconstruction (transfer or graft) before end-plate degeneration
- Practical Point
- Favour distal nerve transfer for proximal/avulsion lesions
Registry & Resource-Setting Notes
- There is no dedicated peripheral-nerve-injury registry comparable to arthroplasty registries; outcome data come from specialist brachial-plexus and peripheral-nerve units, which concentrate volume and expertise.
- High-resource settings: access to MR neurography, high-resolution nerve ultrasound, intra-operative nerve stimulation and microsurgical transfer; earlier, protocolised decision-making.
- Limited-resource settings: diagnosis is largely clinical with EMG where available; emphasis on prompt reduction, documented serial examination and timely referral to a regional microsurgical centre, since delayed reconstruction (beyond roughly 12 months) markedly reduces the chance of useful deltoid recovery.
Special Scenarios
Quadrangular Space Syndrome
- Pathology: Compression of Axillary Nerve and PCHA in the space.
- Causes: Hypertrophy of muscles (pitchers, swimmers), Fibrous bands, Paralabral cysts.
- Presentation: Vague posterior shoulder pain, paresthesia in badge area, weakness in ER/Abd (fatigue).
- Diagnosis: MRI (atrophy), Angiogram (PCHA occlusion on abduction).
- Treatment: Surgical decompression.
Decompression involves releasing fibrous bands in the space.
The axillary nerve is the single most important nerve in shoulder replacement — above all in reverse total shoulder arthroplasty (RTSA), where the deltoid is the prime mover that substitutes for the deficient rotator cuff:
- An intact axillary nerve (a functioning deltoid) is a prerequisite for RTSA. A pre-existing axillary palsy or deltoid dysfunction is a relative contraindication, because the prosthesis depends on deltoid power and tension.
- Intra-operative risk: the nerve is vulnerable during the deltopectoral or anterosuperior approach, with inferior glenoid/humeral retraction, and from arm over-lengthening — RTSA lowers and lateralises the humerus, which stretches the nerve and is a recognised cause of post-operative neuropraxia.
- Always document deltoid / axillary function before and after shoulder arthroplasty; a new post-operative deltoid palsy after RTSA is functionally devastating, as there is no cuff to compensate.
Controversies & Areas of Uncertainty
- Timing of exploration in closed traumatic palsy. There is no Level 1 trial defining the exact cut-off. Most centres explore at 3-6 months if there is no clinical or electrophysiological recovery, applying the "1 mm/day" regeneration principle so that the motor end-plate is reached before irreversible atrophy (commonly cited as roughly 12-18 months from injury). Some advocate earlier exploration in complete high-energy injuries and avulsions, where spontaneous recovery is unlikely.
- Nerve transfer versus interpositional grafting. Distal triceps-branch-to-axillary transfer shortens regeneration distance and avoids a graft donor, and is increasingly preferred for proximal or late injuries. However, comparative data are largely retrospective Level III-IV case series; no randomised comparison exists, and graft remains valid for short, accessible gaps with a healthy proximal stump.
- Single versus double fascicular / dual neurotisation. Adding a posterior-branch (teres minor) target to the anterior-branch transfer may improve external rotation and abduction endurance, but evidence is limited and the optimal donor combination is unsettled.
- Quadrangular space syndrome diagnosis. QSS is a clinical-radiological diagnosis of exclusion. Dynamic posterior circumflex humeral artery occlusion on angiography is described in asymptomatic individuals, so a positive arteriogram is supportive rather than diagnostic; over-diagnosis and unnecessary decompression are recognised risks.
- Routine MRI / nerve ultrasound after dislocation. High-resolution ultrasound and MR neurography can demonstrate nerve continuity early, but their role in changing management before the 3-month electrophysiology window remains debated.
MCQ Practice Points
Q: What accompanies the Axillary nerve in the Quadrangular Space? A: Posterior Circumflex Humeral Artery (PCHA). The Circumflex Scapular Artery is in the Triangular Space. The Profunda Brachii is in the Triangular Interval.
Q: What is the average distance of the axillary nerve from the acromion? A: 5-7 cm. However, in shorter individuals, it can be 4cm. A safe rule of thumb is 3-4 cm.
Q: Which muscle recovers first after a proximal axillary nerve injury? A: Teres Minor. It is supplied by the posterior branch and is closer to the origin than the deltoid branches. Recovery of external rotation often precedes abduction.
Q: What does Hornblower's sign test for? A: Teres Minor dysfunction. The patient cannot externally rotate the arm in 90 degrees of abduction. The hand falls towards the mouth (like blowing a horn).
Q: Which nerve is most commonly used as a donor for Axillary Nerve reconstruction? A: Radial Nerve (Branch to Long Head Triceps). It is anatomically close, has redundant innervation to the triceps, and provides excellent motor axon match.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old male has an anterior shoulder dislocation. Reduced in ED. You see him next day. He has numbness over the deltoid. What do you do?”
“A patient had a rotator cuff repair via a mini-open lateral approach. Now has no active abduction. Cuff appears intact on Ultrasound. Diagnosis?”
“A 19-year-old elite swimmer complains of vague posterior shoulder pain and fatigue during late laps. MRI shows isolated atrophy of Teres Minor. Proximal humerus is normal.”
Anatomy High Yield
- Roots: C5-C6
- Cord: Posterior
- Space: Quadrangular
- Vessel: PCHA
Clinical Signs
- Badge: Sensory loss
- Square Shoulder: Wasting
- Swallow Tail: Post Delt Lag
- Hornblower: Teres Minor (ER)
Key Numbers
- 5.5cm: Safe zone from anterolateral acromion
- 45%: Nerve injury on EMG (dislocation/neck #)
- 3-4 weeks: Baseline EMG timing
- 1mm/day: Nerve regrowth rate
Differentials
- Rotator Cuff Tear (Pain/Weakness)
- C5 Radiculopathy (Biceps involved)
- Parsonage Turner (Pain +++)
- Frozen Shoulder (Stiffness)
Evidence Base
Triceps Long Head to Axillary Transfer - Anatomic Basis
- Cadaveric study (36 shoulder girdles) establishing the anatomic feasibility of transferring the nerve to the long head of triceps to the anterior branch of the axillary nerve via a posterior approach
- Anterior branch of axillary nerve averaged 2.1 mm diameter with ~2704 axons; nerve to long head of triceps averaged 1.1 mm with ~1233 axons
- Using the acromial angle as landmark, the combined nerve lengths exceeded the gap, allowing tension-free direct coaptation without a graft
Combined Nerve Transfers for C5-C6 Avulsion (Deltoid Outcomes)
- 15 patients with C5-C6 avulsion treated with combined transfers including nerve to long head of triceps to the anterior branch of the axillary nerve
- All patients recovered deltoid function: 13 scored M4 and 2 scored M3; mean shoulder abduction 115 degrees
- No clinical donor-nerve deficits; rapid recovery attributed to short regeneration distance without a graft
Triceps Medial Head and Anconeus to Deltoid Transfer
- 9 patients with isolated axillary nerve injury; radial branch to lower triceps medial head and anconeus transferred to the anterior division of the axillary nerve
- All recovered deltoid function and retained full elbow extension; abduction strength improved from ~40% to ~60% of the normal side
- Abduction endurance improved from ~25% to ~65% of normal, eliminating reported shoulder pain and fatigability
Nerve Lesions in Shoulder Dislocation & Humeral Neck Fracture
- Prospective clinical and EMG study of 101 patients with primary shoulder dislocation or humeral neck fracture
- Electrophysiological evidence of nerve injury in 45%, most often axillary, suprascapular, radial and musculocutaneous nerves
- Significantly more injuries in older patients and those with a haematoma; most recovered within four months, with only eight retaining persistent motor loss
Acromion-Axillary Nerve Distance & Safe Zone (Clinical)
- Intra-operative measurement in 37 patients undergoing proximal humerus plating
- Mean acromion-to-axillary-nerve distance 6.0 cm (range 5.5-6.6); nerve location predictable from arm length in only 18% of patients
- Authors recommend treating 5.5 cm from the anterolateral acromion as the safe zone in the deltoid-splitting approach
Quadrilateral (Quadrangular) Space Syndrome - Original Series
- Original description: compression of the posterior humeral circumflex artery and axillary nerve in the quadrilateral space
- Symptoms aggravated by abduction and external rotation; arteriography shows PCHA occlusion in abduction/external rotation with point tenderness over the space
- Of 18 operated patients, 8 had complete relief and 8 improved after posterior decompression
Axillary Nerve Risk in Percutaneous Proximal Humeral Plating
- Cadaveric study (20 shoulders) of the Synthes PHILOS aiming guide via a lateral deltoid-splitting approach
- The axillary nerve traversed row D in every shoulder and crossed row C in 11 and row E in 16 shoulders; closest distance to a screw was 4.5 mm
- Demonstrated for the first time that the nerve crosses row C of the plate, with left-sided screws closer to the nerve