The Anterior Shield of the Shoulder
- Largest and strongest of the Rotator Cuff muscles (53% of total cuff mass).
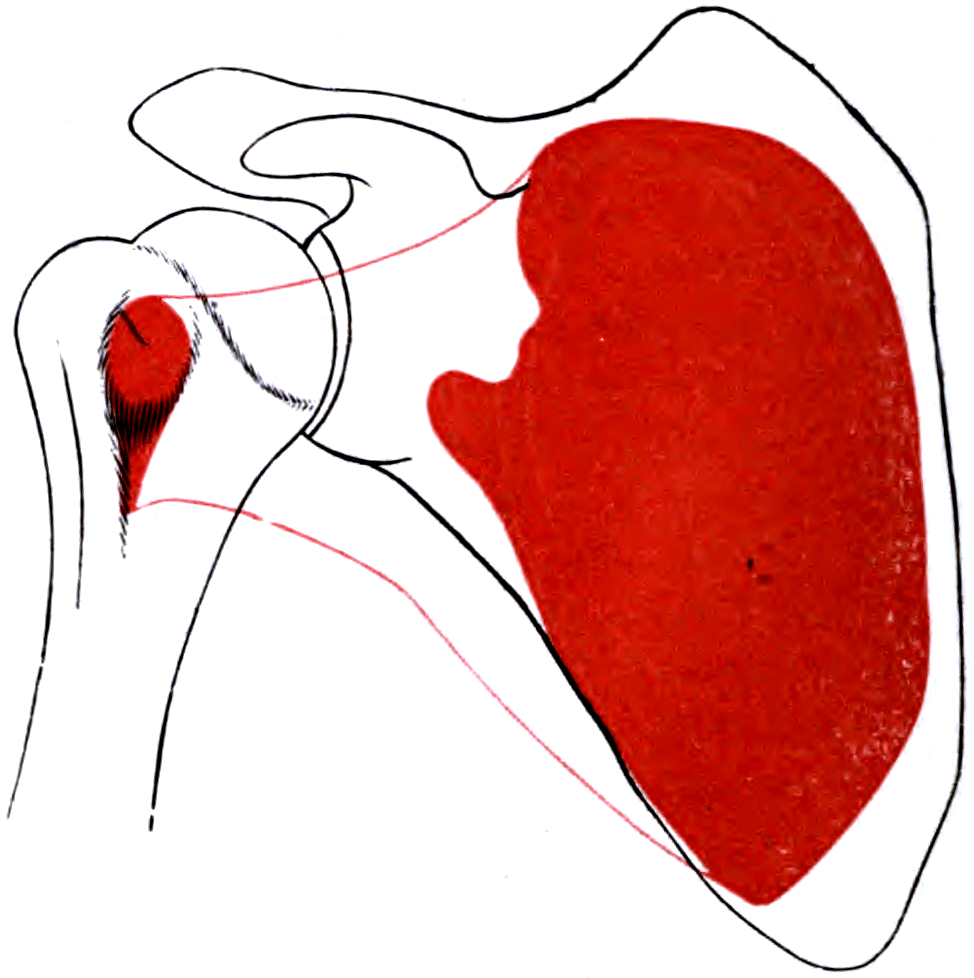
- Originates from the Subscapular Fossa (Anterior Scapula).
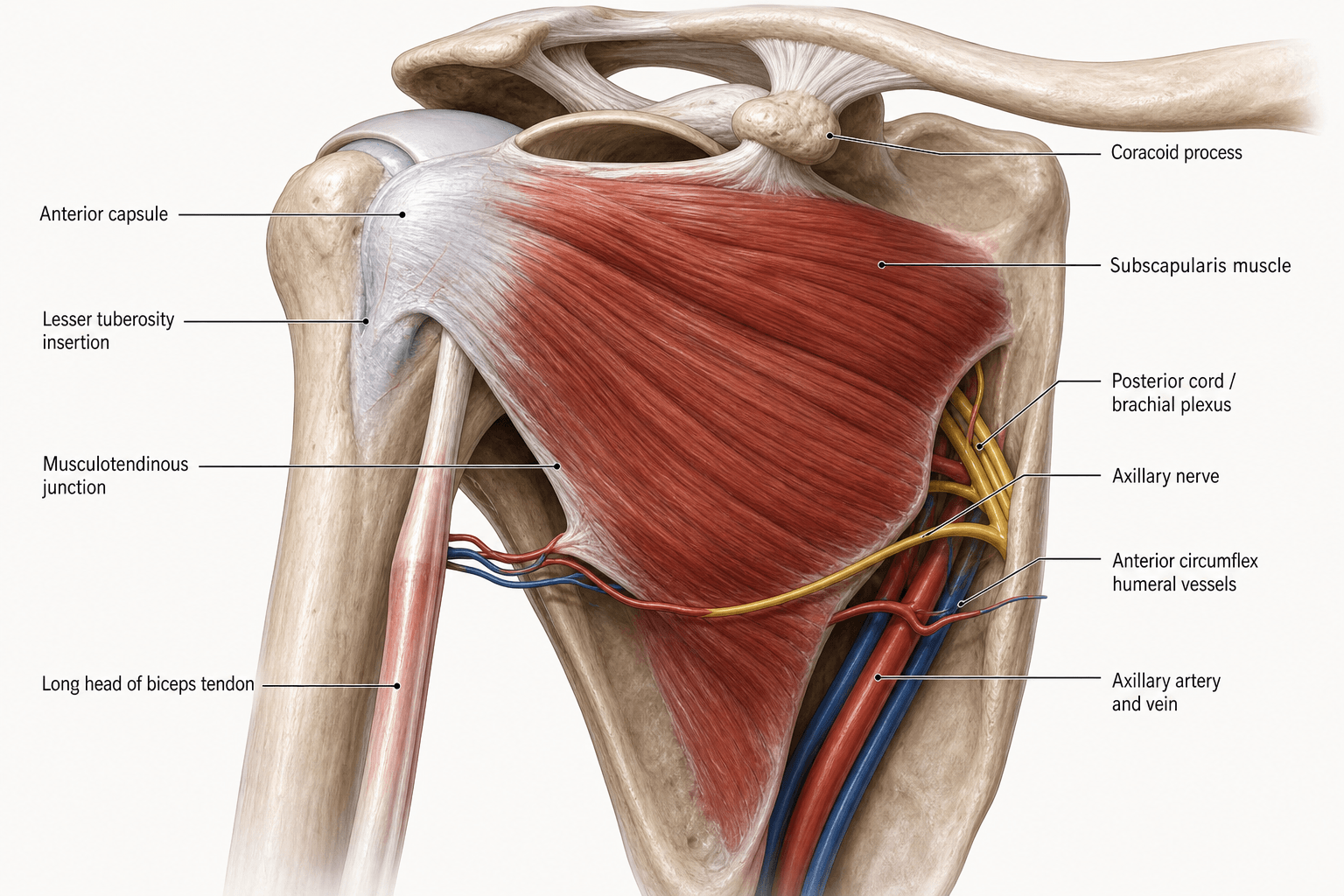
- Inserts onto the Lesser Tuberosity (Comma Sign).
- Innervated by Upper and Lower Subscapular Nerves (Posterior Cord, C5/6).
- The Lower Subscapular Nerve also innervates Teres Major.
- “The 'Comma Sign' is the confluence of the Subscapularis and the SGHL/CHL complex.
- “Isolated Subscapularis tears are rare; usually associated with Biceps pulley lesions.
- “Upper 60% of insertion is tendinous; Lower 40% is muscular (directly onto bone).
- “Roller Wringer Effect: Coracoid impingement on the subscapularis during internal rotation.
Inferior Border.
- The Axillary Nerve runs along the inferior border of the Subscapularis muscle (Quadrangular Space).
- Risk: During inferior release or 'slide', the nerve is at high risk (~1-2cm from the lower edge).
The 'Hidden' Tear.
- Subscapularis tears are often missed on MRI ("The Forgotten Cuff").
- Look for 'Subcoracoid' edema or fat effacement.
- Clinical: Increased passive External Rotation compared to normal side suggests rupture.
- Roots
- C5, C6
- Supply
- Superior Subscapularis
- Course
- Direct entry from Post Cord
- Roots
- C5, C6
- Supply
- Inf Subscapularis + Teres Major
- Course
- Descends along lateral border
- Roots
- C5, C6
- Supply
- Deltoid + Teres Minor
- Course
- Through Quadrangular Space
- Roots
- C6, C7, C8
- Supply
- Latissimus Dorsi
- Course
- Between Upper/Lower Nerves
ULTRAPosterior Cord Branches
Hook:The order of branches from the Posterior Cord.
Lift The Belly BearSubscapularis Tests
Hook:Essential clinical tests for rupture.
SITSRotator Cuff Insertion
Hook:The Subscapularis is the only anterior cuff muscle.
Overview
The Subscapularis is the largest and strongest muscle of the rotator cuff. It fills the subscapular fossa on the anterior surface of the scapula and acts as the primary anterior stabilizer of the glenohumeral joint. It provides approximately 50% of total rotator cuff muscle mass.
The subscapularis is one arm of the transverse (axial) force couple that centres the humeral head on the glenoid — a biomechanics concept examiners expect:
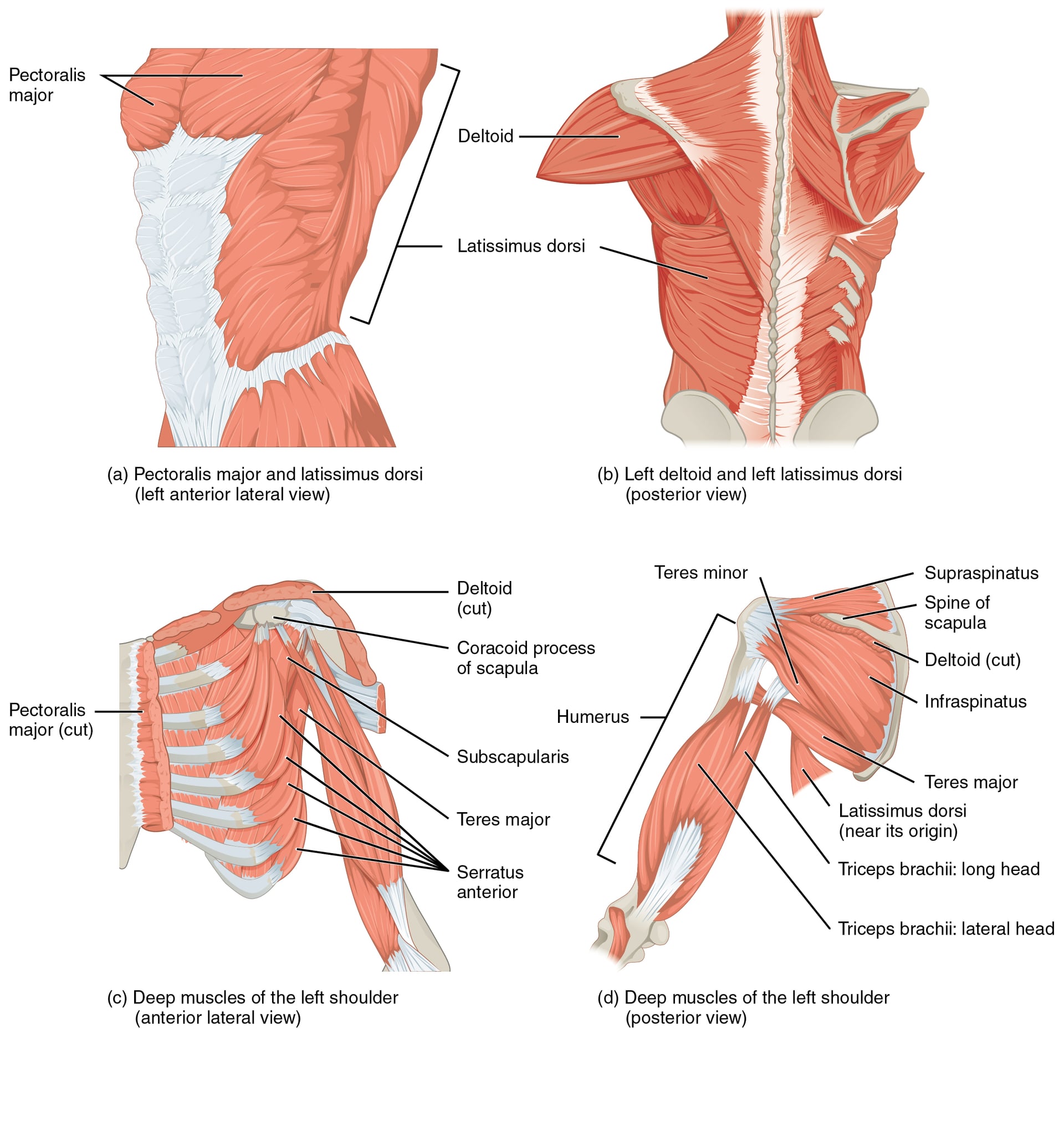
- Transverse force couple: the subscapularis anteriorly is balanced by the infraspinatus and teres minor posteriorly. Their equal and opposite pull compresses and centres the head during elevation; an intact transverse couple keeps a stable fulcrum even when the supraspinatus is torn.
- Coronal force couple: the deltoid (superiorly directed) is balanced by the inferior rotator cuff (subscapularis plus infraspinatus/teres minor), stopping the deltoid from simply shrugging the head upward.
- Why it matters: an isolated subscapularis tear unbalances the transverse couple — the unopposed posterior cuff and deltoid pull the head antero-superiorly, and large anterosuperior cuff loss produces anterosuperior escape and pseudoparalysis. This is the rationale for restoring the anterior arm of the couple (repair, pectoralis-major transfer) or changing the fulcrum (reverse arthroplasty).
Neurovascular
Origin
- Medial two-thirds of the subscapular fossa (anterior surface) of the scapula.
- Some fibers arise from tendinous intramuscular septa attached to ridges on the bone.
Insertion
- The fibers converge into a broad tendon that passes anterior to the joint capsule.
- Site: Lesser Tuberosity of the Humerus.
- Extension: The tendon extends inferiorly to the surgical neck.
- Fibrous Expansion: Some fibers extend over the bicipital groove to the Greater Tuberosity (forming the Transverse Humeral Ligament roof).
The subscapularis forms the inferior margin of the rotator interval — the triangular gap between the superior border of subscapularis (below) and the anterior border of supraspinatus (above), with the coracoid at its base. Within it lie the coracohumeral ligament (CHL), the superior glenohumeral ligament (SGHL) and the intra-articular long head of biceps.
- The biceps pulley (reflection sling) that keeps the biceps in its groove is formed by the SGHL and CHL medially, reinforced by the superior border of subscapularis (medial wall) and the supraspinatus (lateral wall).
- A subscapularis tear disrupts this medial sling, so the biceps subluxates medially — the imaging hallmark that should always trigger a search for a subscapularis tear, and the very tissue that, pulled off the humerus, becomes the arthroscopic comma sign.
- Rotator-interval laxity contributes to inferior and multidirectional instability; interval closure is a recognised adjunct in instability surgery.
Surface Anatomy
Key Surface Landmarks
- Coracoid Process: The 'Lighthouse' of the shoulder. Palpable 2cm inferior to the clavicle in the deltopectoral groove.
- Lesser Tuberosity: Palpable lateral to the coracoid when the arm is externally rotated.
- Deltopectoral Groove: The location of the cephalic vein and the interval for the open approach.
Palpation
- Axillary Approach: In abduction, the lower border of the subscapularis can be palpated in the axilla (anterior fold).
- Tendon: Difficult to palpate directly as it is deep to the coracoid and conjoined tendon.
External rotation brings the lesser tuberosity out from under the coracoid, facilitating palpation.
Classification Systems
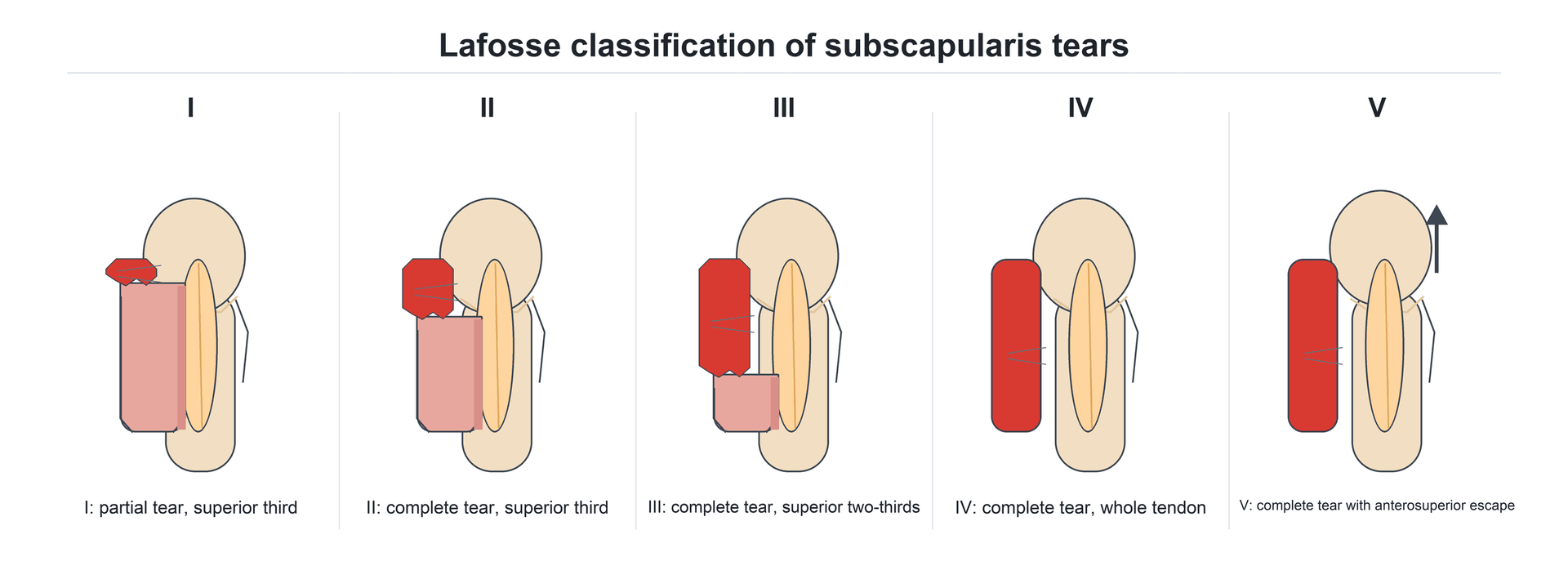
Lafosse Classification (Arthroscopic)
Based on the extent of the tear from Superior to Inferior (Rolled edge).
- Type I: Partial lesion of superior one-third (Leading edge).
- Type II: Complete lesion of superior one-third.
- Type III: Complete lesion of superior two-thirds.
- Type IV: Complete lesion of entire tendon (Head centered).
- Type V: Complete lesion with Anterosuperior Escape (Head migrates up and forward).
Implication: Type I/II can be repaired via standard portals. Type III/IV often require accessory portals or open approach. Type V needs reverse arthroplasty or complex reconstruction.
This classification guides the approach (Arthroscopic vs Open) and the rehabilitation protocol.
Clinical Assessment
Gerber's Test.
- Hand on lumbar spine (palm out).
- Patient lifts hand away from back.
- Integrity: Tests Lower Subscapularis.
- False Negative: Extension of elbow/shoulder substitution.
Napoleon Sign.
- Hand on belly, elbow forward.
- Patient presses into belly without elbow dropping back.
- Integrity: Tests Upper Subscapularis.
- Positive: Elbow drops posterior (extension) to compensate.
Additional Signs
- Bear Hug Test: Hand on opposite shoulder, resist lift-off. High sensitivity for upper tears.
- Subscapularis Lag Sign: Passive ER to near full, release. If arm springs back into IR? No, wait.
- Correction: Passive IR (Place hand behind back). If patient cannot hold the hand away (it drops back to spine), it is a lag.
- Passive External Rotation: Increased passive ER compared to the normal side is a hallmark of complete rupture.
Differential Diagnosis of Anterior Shoulder Pain / Weak Internal Rotation
- Key Discriminator
- Positive belly-press / lift-off; increased passive ER
- Confirmatory Finding
- Tendon discontinuity at lesser tuberosity on MRI; biceps medial subluxation
- Key Discriminator
- Anterior pain, click; often coexists with subscap tear
- Confirmatory Finding
- Medial biceps subluxation on axial MRI
- Key Discriminator
- Pain on adduction + internal rotation + flexion
- Confirmatory Finding
- Reduced coracohumeral distance under 6 mm
- Key Discriminator
- Apprehension in abduction-external rotation
- Confirmatory Finding
- Bankart lesion / labral tear on MRA
- Key Discriminator
- Global loss of passive AND active ER
- Confirmatory Finding
- Restricted passive motion in all planes
- Key Discriminator
- Pseudoparalysis, proximal humeral migration
- Confirmatory Finding
- High-riding head, acromiohumeral narrowing on radiograph
A key bedside discriminator: in a complete subscapularis rupture passive external rotation is increased on the affected side, whereas adhesive capsulitis reduces passive external rotation.
Investigations
MRI
- Axial View: Best for assessing the tendon insertion and retraction.
- Sagittal Oblique: "Comma Sign" evaluation.
- Findings:
- Tendon discontinuity.
- Fat infiltration (Goutallier stage) in the muscle belly (Scapular Y view).
- Biceps subluxation (medial) indicates a Subscapularis tear (pulley loss).
- Subcoracoid Stenosis: Reduced coracohumeral distance (less than 6mm) predicts impingement.
CT Scan
- CT Arthrogram: Historical gold standard. Useful if MRI is contraindicated or for bony avulsion (Lesser Tuberosity).
Ultrasound
- Dynamic assessment.
- Can visualize the "Rolling" of the tendon under the coracoid (check for impingement).
- Accuracy: Lower than for Supraspinatus, often because the insertion is deep to the coracoid.
Ideally, dynamic ultrasound should be performed by a musculoskeletal radiologist to ensure accuracy.
Subcoracoid Impingement
Anterior shoulder pain provoked by Adduction + Internal Rotation + Flexion (e.g., throwing follow-through).
- Pathology: Stenosis of the subcoracoid space (Coracohumeral distance less than 6mm on MRI).
- Effect: Abrasion of the Subscapularis tendon ('Roller-Wringer' effect).
- Test: Cross-arm adduction triggers anterior pain (distinct from AC joint).
Management Strategy
Management Algorithm
- Treatment
- Physiotherapy
- Rationale
- Compensated by Pect Major/Lat Dorsi
- Treatment
- Repair (Arthroscopic/Open)
- Rationale
- Prevents fatty atrophy (rapid in Subscap)
- Treatment
- Pect Major Transfer
- Rationale
- Restores muscle tendon unit force couple
- Treatment
- Reverse TSA
- Rationale
- Restores fulcrum
- Urgency: Subscapularis tears retract and undergo fatty atrophy FASTER than Supraspinatus tears. Early repair is advocated.
Young patients with acute tears should be prioritized for surgery within 2 weeks to optimize outcomes.
Surgical Technique
Deltopectoral Approach
- Incision: Coracoid to deltoid insertion.
- Interval: Pectoralis Major (Medial) and Deltoid (Lateral). Cephalic vein preserved (usually laterally).
- Exposure: Clavipectoral fascia incised. Conjoined tendon retracted medially.
- "The Three Sisters": Anterior Circumflex Humeral vessels (leash) mark the inferior border of the Subscapularis. must be ligated.
Tendon Management (Arthroplasty)
- Peel: Subperiosteal release (for repair).
- Tenotomy: Division 1cm from insertion (easy to close).
- Osteotomy: Lesser tuberosity osteotomy (Bone-to-bone healing, rare now).
The osteotomy has a high union rate but rehabilitation is slower due to bone healing precautions.
Complications
- Failure of Healing: Re-tear rate 5-10%.
- Nerve Injury: Axillary Nerve (inferior), Musculocutaneous (refraction of conjoined tendon).
- Stiffness: Internal Rotation loss (over-tightening).
- Biceps Pathology: Failure to address instability leads to pain.
Rehabilitation Protocol
- Phase 1 (0-6 weeks): Sling. Passive ER limited to 0 (neutral) to protect repair. Active IR prohibited.
- Phase 2 (6-12 weeks): Active assist. Full ROM goal.
- Phase 3 (3-6 months): Strengthening (Internal Rotation bands).
- Prognosis: Return to sport 6 months. High satisfaction if healed.
Prognosis
- Fatty Infiltration: Grade 3/4 (Goutallier) is irreversible and predicts failure.
- Tendon Excursion: Retraction to glenoid rim implies difficulty in mobilization.
- Outcomes: Arthroscopic results now match Open repair results for isolated tears.
Guidelines, Registries & Global Practice
Global Epidemiology
- Isolated subscapularis tears are uncommon, comprising a minority of all rotator cuff tears, and are frequently under-recognised ("the forgotten cuff").
- Tears affecting the subscapularis become more prevalent with anterosuperior cuff disease and with anterior glenohumeral instability surgery.
- Traumatic tears classically follow a forced external rotation or hyperextension injury, whereas degenerative tears accompany age-related global cuff degeneration.
Side-by-Side Guidance
- Position on Cuff/Subscapularis Tears
- Evidence-based cuff guidance supports surgical repair for acute, traumatic, full-thickness tears in active patients; shared decision-making for chronic degenerative tears.
- Position on Cuff/Subscapularis Tears
- Recommend early specialist referral for suspected acute traumatic cuff tears; structured non-operative trial appropriate for many chronic atraumatic tears.
- Position on Cuff/Subscapularis Tears
- Emphasises anatomic footprint restoration and protection of the axillary nerve at the inferior border during release.
- Position on Cuff/Subscapularis Tears
- Supports arthroscopic repair where expertise exists; tendon transfer or reverse arthroplasty reserved for irreparable tears.
Registry and Outcome Signals
- Reverse total shoulder arthroplasty (used for cuff-deficient and pseudoparalytic shoulders) shows strong implant survivorship in national joint registries (AOANJRR, NJR, AJRR), supporting its role in irreparable anterosuperior cuff insufficiency in older patients.
- Subscapularis management during anatomic shoulder arthroplasty (tenotomy vs peel vs lesser tuberosity osteotomy) remains debated, with registry and cohort data showing no single technique clearly superior for healing.
High- vs Limited-Resource Practice
- Well-resourced settings: Arthroscopic repair with 70-degree scopes, suture anchors, and routine MRI; reverse arthroplasty readily available for irreparable disease.
- Limited-resource settings: Open deltopectoral repair is a safe, reliable, equipment-light alternative; ultrasound substitutes for MRI; physiotherapy-led non-operative care is the default for low-demand chronic tears.
Instability Surgery Relevance
- The Latarjet (Bristow-Latarjet) coracoid transfer requires a subscapularis split; performing the split at the junction of the upper two-thirds and lower one-third minimises risk to the nerves entering the muscle and to the axillary nerve at the inferior border.
Controversies & Areas of Uncertainty
- Subscapularis handling in anatomic arthroplasty: Tenotomy, subscapularis peel, and lesser tuberosity osteotomy each have advocates. No technique has been shown to be clearly superior for tendon healing or functional internal rotation, and clinical relevance of imaging-detected non-healing is debated.
- Speed of fatty degeneration: It is widely taught that the subscapularis atrophies and fatty-infiltrates rapidly after rupture, motivating early repair, but the precise time-course relative to the posterosuperior cuff is not firmly established in high-level prospective data.
- Test specificity overlap: Belly-press, lift-off, and bear-hug tests each preferentially load different portions of the tendon, but they overlap and can be confounded by pain, stiffness, and substitution, so no single test reliably excludes a partial tear.
- Persistent test positivity after healing: Even with greater than 90% MRI healing, belly-press and lift-off tests frequently remain incompletely corrected, raising questions about how well tendon continuity restores true internal-rotation strength.
- Irreparable tear in younger patients: The choice between pectoralis major transfer, pectoralis minor or latissimus-based transfers, and (rarely) reverse arthroplasty in younger patients with isolated irreparable subscapularis loss remains unsettled.
MCQ Practice Points
Q: Which part of the Subscapularis tears most commonly? A: The funny thing is... It tears from Superior to Inferior. The insertion at the lesser tuberosity acts like a 'zipper'.
Q: What is the distance of the Axillary Nerve from the inferior border of Subscapularis? A: 1-2 cm. But in adduction, the nerve moves closer to the muscle significantly.
Q: Is the Subscapularis insertion tendon or muscle? A: Upper 60% = Tendoid. Lower 40% = Muscular. This is why 'footprint' repair usually focuses on the upper 2/3.
Q: On a Scapular Y view X-ray, where is the Subscapularis? A: Anterior to the scapula body. It fills the costal surface.
Q: Which structure forms the MEDIAL wall of the Biceps Pulley? A: SGHL and Subscapularis Tendon. Loss of the medial wall leads to medial subluxation of the biceps.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are performing a shoulder arthroscopy for a suspected supraspinatus tear. The posterior cuff looks fine. Biceps is frayed. How do you assess the subscapularis?”
“65M, chronic massive anterior cuff tear. Subscapularis is retracted to glenoid, Goutallier 4. He has pain and pseudoparalysis (cannot lift hand off belly). Management?”
“Patient 3 months post open Latarjet procedure. Complains they cannot tuck their shirt in behind their back. No pain. Diagnosis?”
Anatomy
- Origin: Subscap Fossa
- Insert: Lesser Tuberosity
- Nerve: Upper/Lower Subscap (Post Cord)
- Action: Internal Rotation
Clinical
- Lift-Off: Best for Lower
- Belly-Press: Best for Upper
- Bear-Hug: Sensitive
- Lag Sign: Specific
Pathology
- Comma Sign: Torn SGHL/Subscap
- Hidden Lesion: Missed on Scope
- Pulley Lesion: Biceps instability
- Goutallier: Fatty atrophy
Evidence Base
Arthroscopic Repair of Isolated Subscapularis Tears
- Prospective series of 17 patients undergoing all-arthroscopic isolated subscapularis repair
- Average relative Constant score improved from 58% to 96%
- CT arthrography showed intact repair in 15 of 17; 2 partial re-ruptures
- No progression of fatty infiltration after anatomic repair
- Mean interval from symptom onset to surgery was 24 months
Comma Sign as an Arthroscopic Guide
- The comma sign is an arc of the SGHL/CHL complex attached to the superolateral corner of the torn subscapularis
- Reliable intra-operative marker of the retracted subscapularis stump
- Especially useful in chronic tears scarred to the deltoid fascia
- Guides anatomic repair back to the lesser tuberosity footprint
Pectoralis Major Transfer for Irreparable Tears
- 30 consecutive pectoralis major transfers for irreparable subscapularis tears
- Mean relative Constant score improved from 47% to 70%
- Pain and activities-of-daily-living scores improved reliably
- Outcomes were markedly worse when an associated supraspinatus tear was also irreparable (Constant 49% vs 79%)
Arthroscopic vs Open Repair of Isolated Subscapularis Tears
- Prospective two-centre cohort: 18 arthroscopic versus 16 open single-row anchor repairs
- Constant-Murley score rose from 54 to 86 (arthroscopic) and 50 to 85 (open) at minimum 48 months
- MRI tendon healing exceeded 90% in both groups with no significant difference
- Belly-press and lift-off tests often remained incompletely corrected despite healing
Three-Dimensional Rotator Cuff Footprint Anatomy
- 28 cadaveric shoulders analysed by 3D CT reconstruction
- Five distinct tuberosity facets identified, including two on the lesser tuberosity
- Lesser tuberosity inferior facet inclined 77.8 degrees, superior facet 50.3 degrees
- Facet angular positions were highly consistent between specimens
Interdigitated Insertion of the Rotator Cuff
- 20 shoulders (16 cadaveric, 4 fresh) dissected to map cuff insertions
- Cuff tendons interdigitate into a continuous hood around the greater and lesser tuberosities
- Tendons and the joint capsule behave as one inseparable unit
- Function of one cuff muscle is influenced by its neighbours