Quadrangular & Triangular Spaces
Triangular SPACE vs INTERVAL.
- Space (Medial): Circumflex Scapular Artery. No Nerve.
- Interval (Lateral/Inferior): Radial Nerve. Profunda Artery.
- Trap: Candidates often mix up the contents.
Major is Lower.
- Teres Minor is above (a rotator cuff muscle, external rotator).
- Teres Major is below (an adductor/internal rotator).
- The long head of triceps descends between them: it passes posterior to teres minor and anterior to teres major, dividing the medial triangular space from the lateral quadrangular space.
- Shape
- Square
- Key Nerve
- Axillary
- Key Artery
- Post. Circ. Humeral
- Shape
- Triangle
- Key Nerve
- None
- Key Artery
- Circumflex Scapular
- Shape
- Triangle (Inv)
- Key Nerve
- Radial
- Key Artery
- Profunda Brachii
R-IRadial Nerve Space
Hook:Radials use Intervals, not Spaces.
A-T-D-CAxillary Nerve Branches
Hook:AC/DC rocks the shoulder.
Overview
The posterior scapulo-humeral region is organised around the intersection of teres minor (superiorly, a rotator cuff external rotator), teres major (inferiorly, an adductor/internal rotator), and the long head of triceps, which descends vertically between them. This arrangement creates three named passages that examiners repeatedly test because each carries a different neurovascular structure:
- Quadrangular (quadrilateral) space — lateral; transmits the axillary nerve and posterior circumflex humeral artery (PCHA).
- Triangular space — medial; transmits only the circumflex scapular artery (no major nerve).
- Triangular interval — inferior; transmits the radial nerve and profunda brachii artery into the spiral groove.
Mastery of these boundaries underpins safe posterior shoulder approaches, the deltoid-splitting safe zone, recognition of axillary nerve injury after dislocation or proximal humerus fracture, and the diagnosis of two uncommon but high-yield entrapment syndromes (quadrilateral space syndrome and triangular interval syndrome). The same anatomy explains the circumflex scapular pedicle used in scapular and parascapular free flaps.
Neurovascular
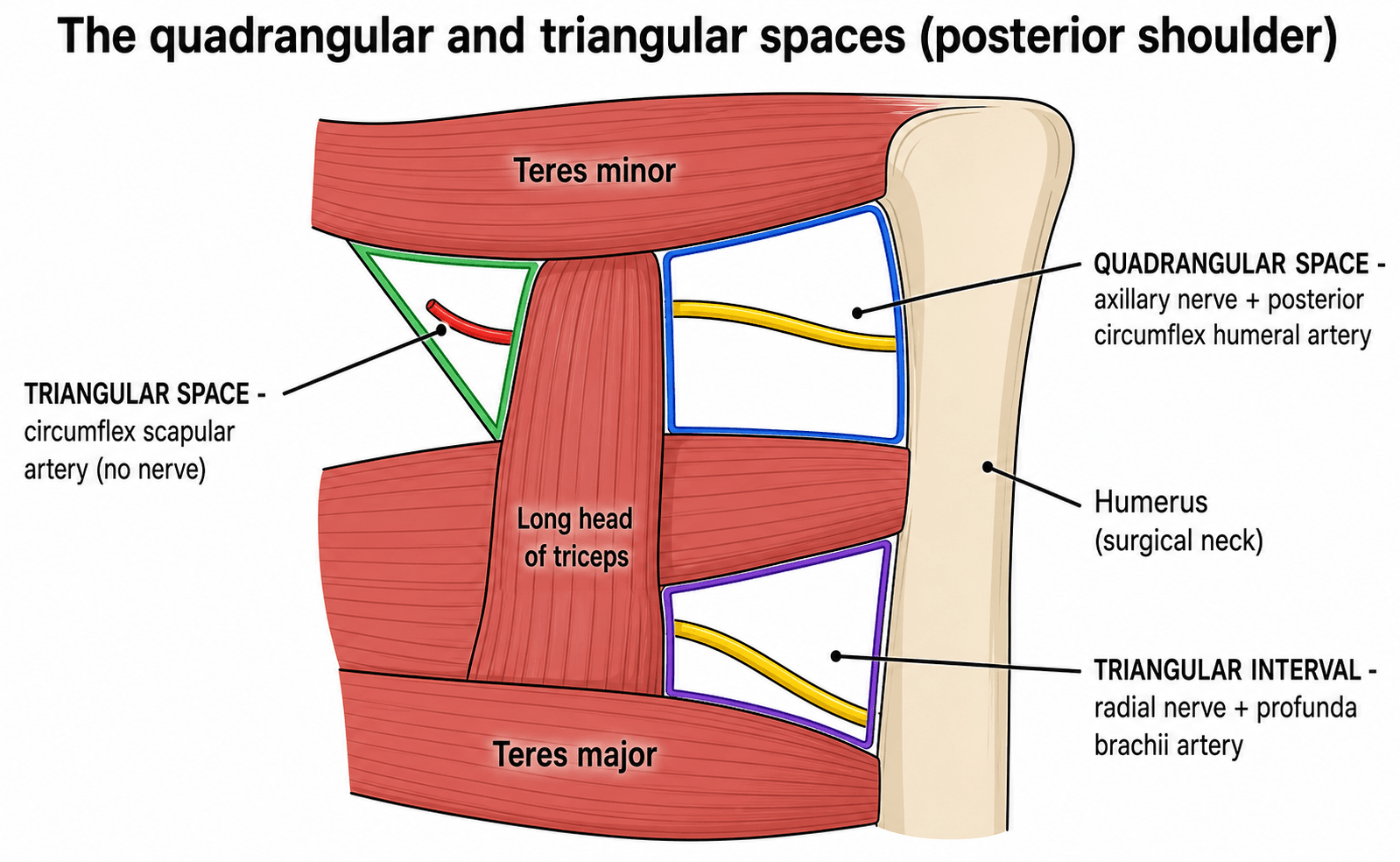
Quadrangular Space
- Superior: Teres Minor (and Subscapularis anteriorly/capsule).
- Inferior: Teres Major.
- Medial: Long Head of Triceps.
- Lateral: Surgical Neck of Humerus.
This space transmits structures from the axilla to the posterior shoulder.
Anatomy: Contents
Neurological Contents
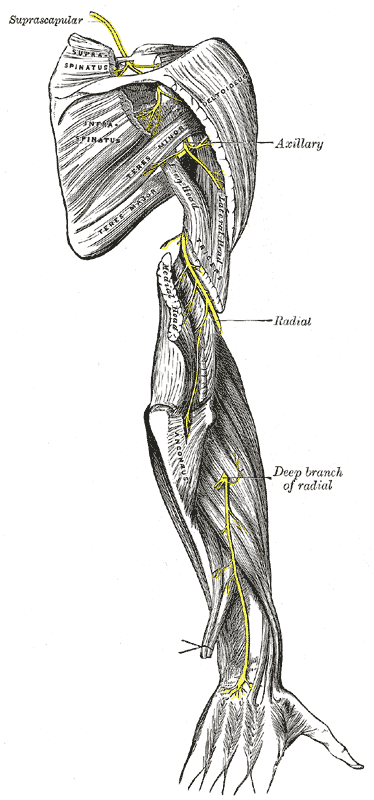
- Quadrangular: Axillary Nerve. Passes posterior to the neck of humerus. Supplies Deltoid and Teres Minor. Gives off Superior Lateral Cutaneous Nerve of Arm.
- Triangular Interval: Radial Nerve. Visible here before it passes deep to the lateral head of triceps.
- Triangular Space: No major nerve.
The axillary nerve is vulnerable in inferior dislocation.
AXEContents of Quadrangular Space
Hook:The Q-Space needs an AXE: Axillary nerve + circumfleX humeral artery, which Exit around the surgical neck.
Pathology: Atrophy
The Hallmark of QSS. Isolated fatty atrophy of the Teres Minor muscle on MRI is highly suggestive of Quadrangular Space Syndrome or isolated Axillary nerve pathology (e.g. Parsonage-Turner). Deltoid may be spared if the anterior branch is unaffected or if compression is distal to the main trunk branching (variable).
Classification Systems
Classification of Compression
- Dynamic: Functional compression (Athletes).
- Static: Structural mass (Cyst, Tumor, Osteophyte).
- Traumatic: Hematoma or Scarring post-trauma.
Most cases of QSS are Dynamic/Functional.
Clinical Assessment
Quadrangular Space Syndrome (QSS)
- Pathology: Compression of Axillary Nerve and PCHA.
- Causes: Bands, hypertrophy of muscles (Pitchers/Swimmers), paralabral cysts.
- Symptoms:
- Vague posterior shoulder pain.
- Paresthesia in "Regimental Badge" area (often absent in chronic cases).
- Weakness is subtle, fatigue-related, and provoked by sustained overhead activity.
- Vascular form: digital ischaemia, cold hand, or splinter haemorrhages from PCHA thrombus embolisation.
- Sign: Point tenderness over the quadrilateral space (lateral to scapula); symptoms reproduced by 1 minute of abduction-external rotation.
Atrophy is often the only objective sign.
Investigations
MRI Shoulder
- Sequence: T1 (Fatty Infiltration), T2/STIR (Edema/Denervation acutely).
- Look for: Paralabral cysts (inferior labrum), fibrous bands.
- Angiography (MRA/CTA): Can show occlusion of PCHA with abduction (dynamic compression).
Dynamic imaging is key for vascular compression.
Differential Diagnosis of Posterior Shoulder Pain & Teres Minor Atrophy
- Distinguishing Feature
- Overhead athlete, dynamic posterior pain
- Atrophy Pattern
- Isolated teres minor (axillary branch)
- Key Test
- Dynamic angiography / abduction-ER provocation
- Distinguishing Feature
- Acute severe pain then patchy palsy
- Atrophy Pattern
- Teres minor +/- deltoid +/- other muscles
- Key Test
- EMG: multifocal denervation
- Distinguishing Feature
- Older patient, cuff pathology on MRI
- Atrophy Pattern
- Teres minor with humeral decentering
- Key Test
- MRI cuff integrity
- Distinguishing Feature
- Spinoglenoid/paralabral cyst
- Atrophy Pattern
- Infraspinatus +/- supraspinatus (NOT teres minor)
- Key Test
- MRI cyst; EMG SSN
- Distinguishing Feature
- Neck pain, dermatomal sensory loss
- Atrophy Pattern
- Multi-muscle myotomal
- Key Test
- Spurling, cervical MRI
- Distinguishing Feature
- Posterior arm/forearm pain, radial bias
- Atrophy Pattern
- Triceps weakness, no teres minor atrophy
- Key Test
- Radial nerve tension test, no cervical provocation
Isolated teres minor atrophy points to the axillary nerve in the quadrilateral space. Isolated infraspinatus atrophy points to the suprascapular nerve at the spinoglenoid notch. Combined deltoid + teres minor denervation localises to the main axillary nerve trunk (e.g. dislocation, Parsonage-Turner).
The quadrangular-space anatomy is most often tested through trauma: the axillary nerve is the most commonly injured nerve in anterior shoulder dislocation and is frequently injured in proximal humerus fractures (and is the nerve most at risk in shoulder surgery).
- Mechanism: a traction/stretch injury as the humeral head displaces — usually a neurapraxia or axonotmesis in continuity, not a transection.
- Examine and document BEFORE and AFTER reduction: deltoid motor function (palpate the contracting muscle belly — formal abduction testing is unreliable acutely because it is painful) and sensation over the regimental-badge area (superior lateral cutaneous nerve). An axillary-nerve palsy is not a contraindication to reduction.
- Prognosis: the majority recover spontaneously over about 3 to 6 months (axonal regeneration at roughly 1 mm per day).
- When to act: a persistent complete deficit at around 3 to 6 months warrants EMG/NCS and consideration of surgical exploration with nerve grafting, or a nerve transfer (e.g. a triceps branch of the radial nerve to the axillary nerve). A complete brachial-plexus pattern, an axillary-artery injury, or an irreducible/locked dislocation raises the urgency.
Minor on TopThe Teres Sandwich
Hook:Major is heavy, so it sinks to the bottom.
Management Algorithm
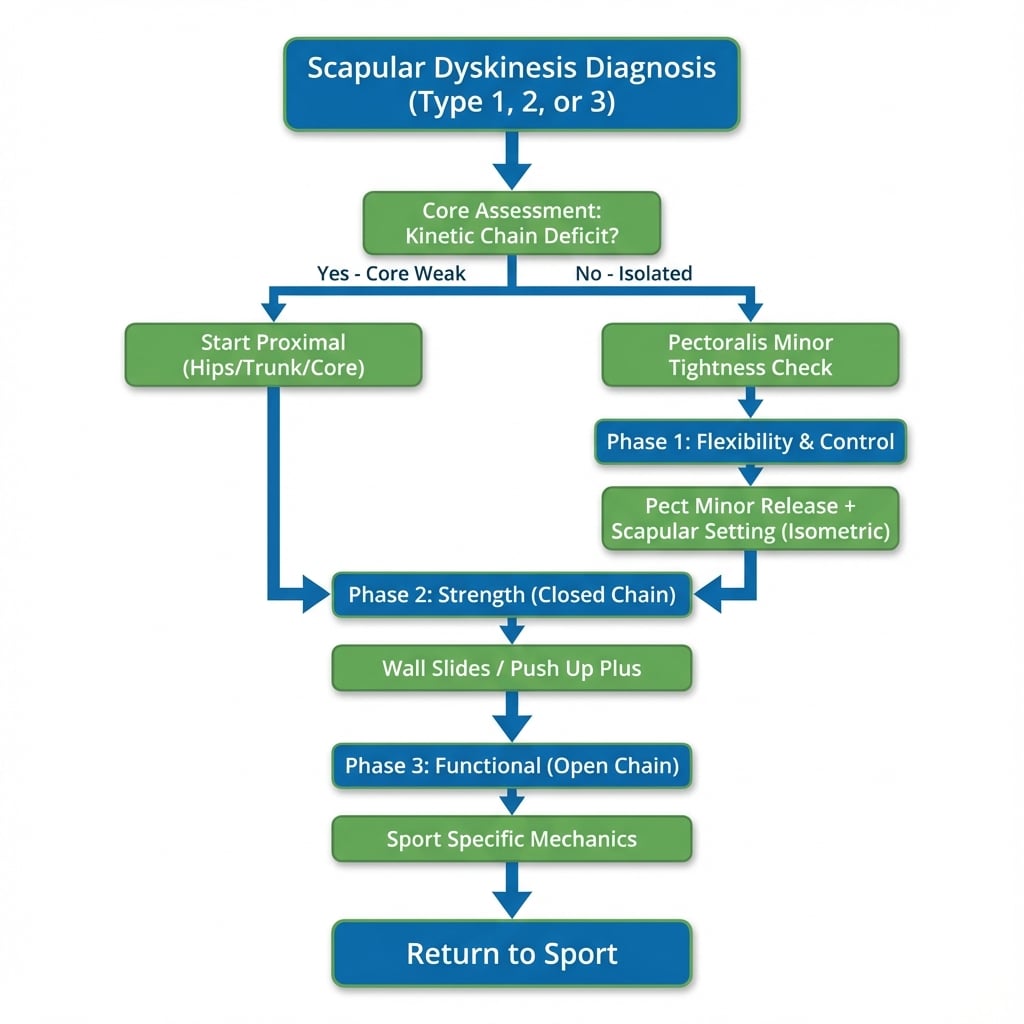
Conservative
- Indication: First line for 3-6 months.
- Therapy: Stretching (posterior capsule), Massage, Activity modification.
- Success: High for functional QSS.
Avoidance of the provoking activity (e.g. overhead throwing) is curative.
Surgical Considerations
Posterior Approach
- Interval: Between Infraspinatus and Teres Minor.
- Risk: Axillary nerve exits Q-Space below Teres Minor.
- Pearl: Stay superior.
This protects the nerve as it exits the space.
The topic's "deltoid spared if the anterior branch is unaffected" and "5–7 cm safe zone" only make sense once you know the two-branch division. After the axillary nerve (posterior cord, C5–C6) passes through the quadrangular space it splits into:
- Anterior (deep) branch — winds transversely around the surgical neck deep to the deltoid, with the posterior circumflex humeral artery, supplying the anterior and middle deltoid (plus a few sensory twigs). This is the branch endangered by the lateral deltoid-splitting approach and by surgical-neck fractures and implants.
- Posterior branch — supplies the posterior deltoid and teres minor, then continues as the superior lateral cutaneous nerve of the arm (the regimental-badge sensory area). A selective posterior-branch lesion gives isolated teres minor ± posterior deltoid denervation — exactly the quadrilateral-space-syndrome pattern.
The deltoid-split safe zone: the anterior branch runs roughly transversely 5 to 7 cm distal to the lateral/anterolateral acromion (but as close as about 3.5 cm in a small patient), so do not carry a deltoid split more than about 5 cm below the acromion, and place a transverse stay suture at the distal apex to stop the split propagating. The nerve is also at risk inferiorly in the deltopectoral approach as it crosses the subscapularis toward the inferior glenoid — palpate it ("tug test") before retracting.
Complications
- Nerve Injury: Iatrogenic injury to Axillary (during release) or Radial (during plating).
- Recurrence: Inadequate release of fibrous bands.
- Bleeding: PCHA or Circumflex Scapular artery (retraction).
- Cosmetic: Posterior scar hypertrophy.
Rehabilitation
- Early Motion: Pendular exercises immediately.
- Strengthening: Rotator cuff from 6 weeks.
- Return to Sport: 3-4 months for overhead athletes.
Prognosis
- Decompression: Good relief of pain. Atrophy may not reverse.
- Nerve Recovery: 1mm/day regeneration if axonal continuity preserved.
Guidelines, Registries & Global Practice
Global epidemiology
- Quadrilateral space syndrome is rare and there is no dedicated registry; most evidence is cadaveric or small case series. It predominates in young (20-40y) overhead athletes (volleyball, baseball/cricket bowling, swimming, tennis) and in patients with paralabral cysts.
- Symptoms of digital ischaemia from PCHA disease have been reported in up to roughly a third of elite volleyball players, underlining the vascular variant of the condition.
Society/guideline positions (no condition-specific guideline exists)
- AAOS / ASES (US) and BOA-BESS (UK): no formal guideline for QSS; consensus from upper-limb literature favours prolonged conservative management first, with surgery reserved for refractory cases or a demonstrable structural lesion.
- AO Foundation / EFORT: relevant guidance is on the axillary nerve safe zone in deltoid-splitting and posterior approaches (protect the nerve 5-7 cm distal to the acromion), rather than on QSS itself.
- IOC / sports-medicine consensus: emphasise vascular work-up (Doppler/duplex, angiography) in overhead athletes with hand ischaemia before attributing symptoms to nerve compression alone.
Imaging & practice variation
- High-resource settings: MRI (denervation signal, paralabral cysts) plus MRA/CTA or dynamic duplex ultrasound for the vascular component; arthroscopic or open decompression available.
- Limited-resource settings: diagnosis rests on clinical provocation testing and plain radiographs to exclude bony causes; ultrasound (where skilled operators exist) is a low-cost dynamic tool; management is predominantly conservative.
Controversies & Areas of Uncertainty
Cahill and Palmer's original cadaveric work did not consistently identify discrete bands, yet later dissection (McClelland and Paxinos) found bands in 14 of 16 shoulders, most often between teres major and the long head of triceps. Their pathological significance versus normal anatomical variation remains debated.
Whether QSS is primarily an axillary nerve compression or a PCHA disease (aneurysm/thrombosis with distal embolisation) is unsettled. The two may be distinct entities sharing a name, which affects whether decompression or vascular intervention is appropriate.
MRI series show isolated teres minor atrophy is far more often associated with cuff tears, humeral decentering, or idiopathic traction than with true compressive QSS, which is rare. The finding is sensitive but poorly specific.
Evidence is limited to small case series; no comparative trials define the optimal surgical technique, indications, or timing. Most authorities reserve surgery for refractory cases or a demonstrable structural lesion (paralabral cyst, mass, aneurysm).
MCQ Practice Points
Q: Which structure passes through the Quadrangular Space? A: Axillary Nerve. (And PCHA).
Q: The Triangular Interval transmits which nerve? A: Radial Nerve.
Q: The Triangular Space is bounded inferiorly by which muscle? A: Teres Major.
Q: The Circumflex Scapular Artery is found in which space? A: Triangular Space.
Q: What sensory area is supplied by the axillary nerve after exiting the Quadrangular Space? A: The 'Regimental Badge' area - lateral upper arm over the deltoid insertion. This is via the Superior Lateral Cutaneous Nerve of Arm branch.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old volleyball player presents with vague posterior shoulder pain and weakness. MRI shows isolated fatty infiltration of Teres Minor. Diagnosis?”
“During a scapular flap harvest, you identify a vessel in the Triangular Space. Which vessel is it and where does it go?”
“Trace the course of the Radial Nerve relative to the Triceps heads.”
Quadrangular Space
- Superior: Teres Minor (Subscapularis anteriorly)
- Inferior: Teres Major
- Medial: Long Head Triceps
- Lateral: Surgical Neck Humerus
- Content: Axillary Nerve
- Content: Posterior Circumflex Humeral Artery
Triangular Space
- Superior: Teres Minor
- Inferior: Teres Major
- Lateral: Long Head Triceps
- Content: Circumflex Scapular Artery
- Note: No major nerve
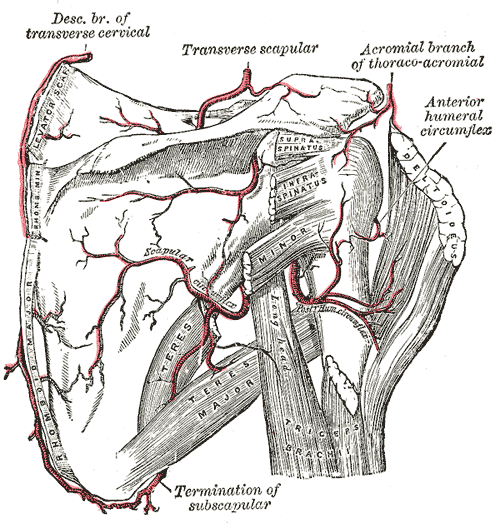
- Clinical: Scapular Anastomosis
Triangular Interval
- Superior: Teres Major
- Medial: Long Head Triceps
- Lateral: Humerus Shaft
- Content: Radial Nerve
- Content: Profunda Brachii Artery
- Clinical: Interval Syndrome (Radial palsy)
Evidence Base
Every citation below has been checked against its source record in PubMed. Cahill's 1983 paper defined the syndrome and the posterior decompression; McClelland's cadaveric study supplies the fibrous-band substrate; and the imaging series (Wilson, Cothran, Friend) consistently show that isolated teres minor atrophy is usually NOT true compressive QSS — most often it accompanies cuff/labral pathology — making the finding sensitive but not specific.
Quadrilateral space syndrome
- Landmark paper that defined the syndrome: compression of the axillary nerve and PCHA in the quadrilateral space
- Symptoms aggravated by forward flexion, abduction and external rotation; constant point tenderness posteriorly
- Subclavian arteriography showed PCHA occlusion with the arm in abduction-external rotation
- Of 18 patients operated via a posterior approach: 8 complete relief, 8 improved, 2 no improvement
The anatomy of the quadrilateral space with reference to quadrilateral space syndrome
- 16 cadaveric shoulders dissected to clarify the anatomy predisposing to QSS
- Fibrous bands present in 14 of 16 shoulders, most commonly between teres major and the long head of triceps
- Where bands were present, both internal and external rotation reduced the cross-sectional area of the quadrilateral space
Teres minor innervation in the context of isolated muscle atrophy
- Combined cadaveric (9 specimens) and radiological study of the teres minor nerve supply
- Marked anatomical variation in origin and length of the teres minor nerve(s), creating multiple potential impingement points
- Of 61 shoulder MRIs, 2 showed isolated teres minor atrophy, clinically distinct from quadrilateral space syndrome
Isolated teres minor atrophy: manifestation of quadrilateral space syndrome or traction injury to the axillary nerve?
- Prospective review of 217 consecutive shoulder MRIs
- Isolated teres minor atrophy in 12 (5.5%), mean age 60, 11 of 12 male
- 92% had associated rotator cuff or labroligamentous tears; none had a quadrilateral space mass
- True QSS appears to be a very rare cause of isolated teres minor atrophy