Anterior-Inferior Labral Tear | Gold Standard: Arthroscopic Repair | Assess Bone Loss
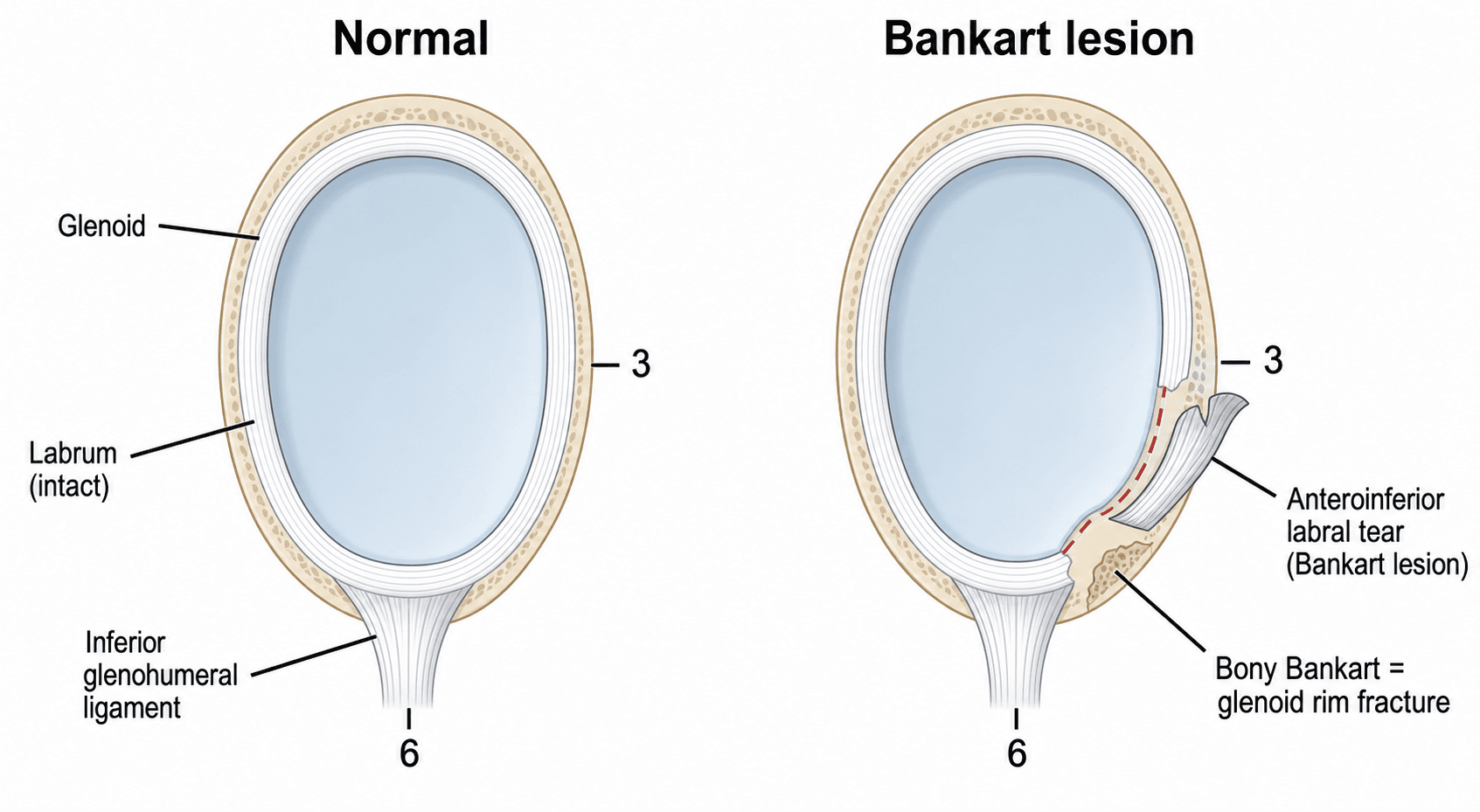
- Bankart lesion is an anterior-inferior labral tear from traumatic anterior dislocation
- 90% of anterior dislocations result in a Bankart lesion (Perthes variant if periosteum intact)
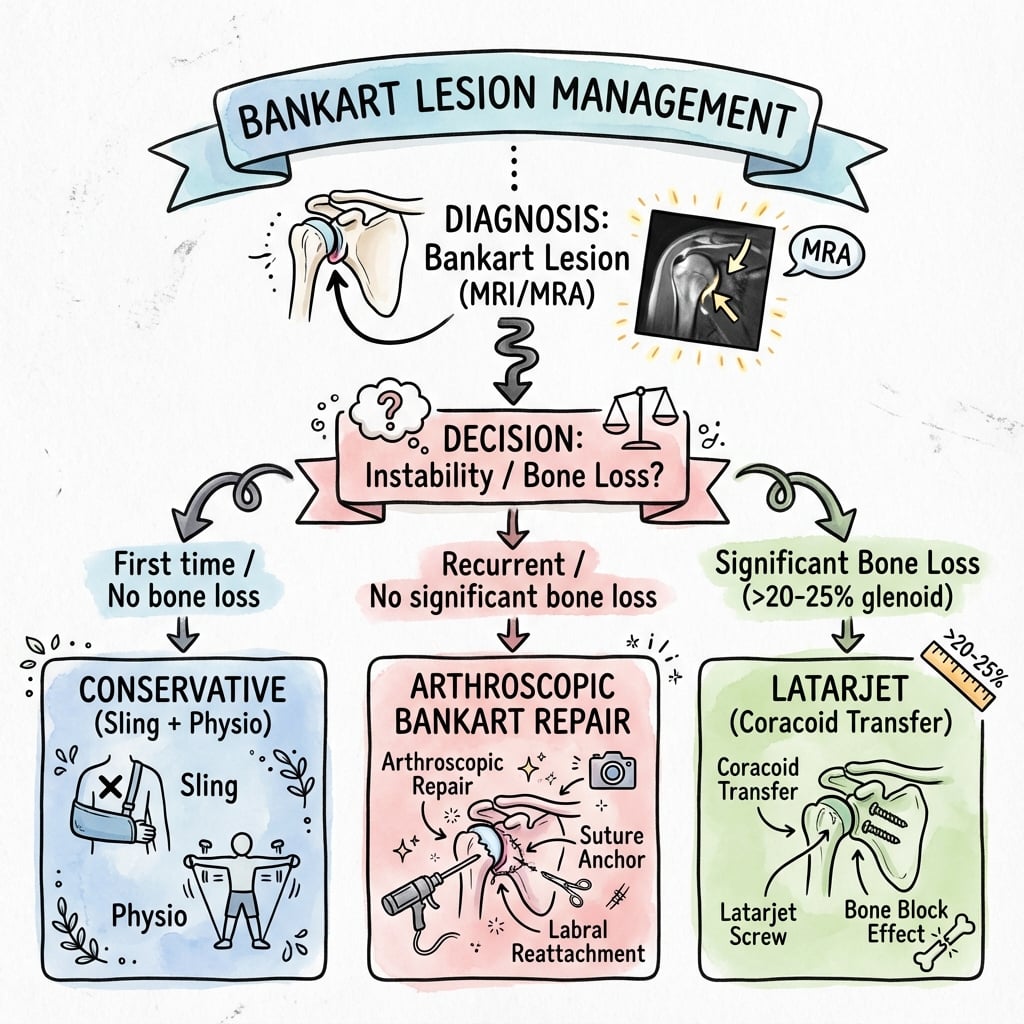
- Glenoid bone loss assessment is mandatory - over 20% (inverted pear) needs Latarjet
- ISIS score predicts instability risk: higher score = greater likelihood of failure with arthroscopic repair
- Arthroscopic repair is gold standard for soft tissue Bankart with minimal bone loss
- “Bankart = anterior-inferior labral tear from anterior dislocation
- “ALPSA = labral tear with periosteum intact but medially displaced
- “Perthes = labral tear with intact periosteum (partial Bankart)
- “Bony Bankart = greater than 20% glenoid bone loss requires bone augmentation
Always assess glenoid bone loss. Over 20% bone loss (inverted pear appearance) predicts arthroscopic failure and requires Latarjet or bone block. Use CT or MRI to measure. Engaging Hill-Sachs also critical.
Instability Severity Index Score (ISIS) predicts recurrence risk after arthroscopic repair. Score over 6 = high risk (consider Latarjet). Factors: age under 20, competitive sports, contact sports, shoulder laxity, Hill-Sachs on AP X-ray, glenoid bone loss.
First-time dislocators under 20 have up to 90% recurrence rate non-operatively. Consider early stabilization in high-risk patients. Recurrent instability is an absolute indication for surgical repair.
ALPSA lesion (Anterior Labroligamentous Periosteal Sleeve Avulsion) has intact periosteum but medially displaced labrum. Requires mobilization before repair. Diagnosis on MRI (labrum medial, intact scapular periosteum).
- Bone Loss
- Under 15%
- Patient Age/Activity
- Any age, non-contact sport
- Treatment
- Arthroscopic repair (3-4 anchors)
- Bone Loss
- 15-20% subcritical
- Patient Age/Activity
- Under 20, contact sport
- Treatment
- Consider Latarjet (ISIS over 6)
- Bone Loss
- Over 20% inverted pear
- Patient Age/Activity
- Any age, any sport
- Treatment
- Latarjet or bone block procedure
- Bone Loss
- Under 15%
- Patient Age/Activity
- Any age
- Treatment
- Arthroscopic repair after mobilization
- Bone Loss
- Minimal bone loss
- Patient Age/Activity
- Over 30, low demand
- Treatment
- Trial of non-operative (3 months rehab)
BANKARTBANKART - Essential Components
Hook:BANKART covers the key assessment and management principles for anterior shoulder instability
ISISISIS - Instability Severity Index Score
Hook:ISIS score over 6 points predicts high failure rate (over 70%) with arthroscopic repair - consider Latarjet
ALPSAALPSA - Variant Lesion Pattern
Hook:ALPSA has intact periosteum but medially displaced - like a sleeve rolling down - must mobilize back to glenoid rim
CLOCK3 CLOCK RULE - Anchor Placement
Hook:Think of a clock face on the glenoid rim - anchors at 3, 4:30, 5:30 positions restore the anterior-inferior bumper
Overview and Epidemiology
A Bankart lesion is a tear of the anterior-inferior glenoid labrum and associated inferior glenohumeral ligament (IGHL) complex. It is the essential lesion in traumatic anterior shoulder instability, occurring in over 90% of anterior dislocations.
- First described by Arthur Sidney Blundell Bankart in 1923
- He recognized the labral tear as the "essential lesion" causing recurrent anterior instability
- Initially treated with open repair (Bankart repair remains the eponym)
- Modern era dominated by arthroscopic techniques with equivalent outcomes
- Traumatic anterior dislocation is the typical mechanism
- Shoulder is forced into abduction, extension, and external rotation (ABER position)
- Anterior capsulolabral structures exceed their tensile strength
- Labrum avulses from anterior-inferior glenoid rim (typically 3-6 o'clock position)
Bankart called this the "essential lesion" because it is the pathoanatomic basis for recurrent anterior instability. Restoring the labral bumper and tensioning the anterior capsule is the goal of surgical repair.
- Incidence: 23.9 per 100,000 person-years for shoulder dislocation (US emergency-department data, Zacchilli & Owens)
- Age: Peak incidence in the 20-29 year decade (highest rate 47.8 per 100,000); 46.8% of dislocations occur between ages 15-29
- Gender: Male predominance (incidence rate ratio 2.64; 71.8% of dislocations in males)
- Sports: Almost half (48.3%) occur during sport/recreation; contact sports (rugby, Australian football), overhead sports
- Recurrence risk: Inversely related to age (up to 90% in patients under 20 years)
- First-time dislocation in young athlete: up to 90% recurrence without surgery
- First-time dislocation over age 40: approximately 20% recurrence
- Each recurrent dislocation increases risk of bone loss and cartilage damage
- Chronic instability leads to early glenohumeral arthritis
Pathophysiology and Mechanisms
Glenoid labrum anatomy:
The glenoid labrum is a fibrocartilaginous rim that:
- Deepens the glenoid socket by 50% in depth
- Increases articular surface area by up to 75%
- Serves as attachment for glenohumeral ligaments
- Acts as a "bumper" or chock-block against translation
Anterior-inferior labral complex:
- The anterior band of IGHL is the primary restraint to anterior translation in abduction and external rotation
- Inserts into the anterior-inferior labrum (3-6 o'clock position on right shoulder)
- Forms a hammock beneath the humeral head when arm is abducted
- The labrum and IGHL function as a unit - disruption of either causes instability
The inferior glenohumeral ligament (IGHL) complex and labrum function as a single unit. The IGHL inserts into the labrum, so a Bankart lesion represents both a labral tear AND a ligamentous avulsion. Repairing the labrum restores both structures.
Glenoid anatomy:
- Pear-shaped in normal state
- Anteroinferior quadrant is the critical zone for stability
- Glenoid version (normally 5-10 degrees retroversion)
- Bare area is central non-articular zone (normal finding, not pathologic)
Bankart lesion variants:
Understanding the variants is critical for surgical planning and exam discussions:
- Classic Bankart: Labral tear with avulsion from glenoid rim
- Bony Bankart: Labral tear with glenoid bone fragment (fracture)
- Perthes lesion: Labral tear but periosteum remains attached (partial Bankart)
- ALPSA: Labral avulsion with intact periosteum, medially displaced sleeve
- GLAD: Glenoid articular disruption with anterior labral tear (cartilage injury)
Not every anterior instability is a Bankart on the glenoid side. A HAGL lesion (Humeral Avulsion of the Glenohumeral Ligament) is avulsion of the IGHL from its humeral attachment rather than the glenoid. It is an important and frequently missed cause of instability and of a "failed Bankart repair" — if a labral repair is performed while a HAGL is overlooked, the shoulder stays unstable. Suspect it when the apprehension/instability pattern is present but the labrum looks intact, and look specifically for the "J sign" on the MR arthrogram: contrast leaks inferiorly where the ligament has pulled off the humerus, turning the normal U-shaped axillary pouch into a J. A bony variant (BHAGL) carries a fleck of humeral bone. Management is repair of the ligament back to the humeral neck (open or arthroscopic), not a glenoid-sided procedure. The exam point: in recurrent or atypical instability, always check both the glenoid AND the humeral attachment of the IGHL.
Pathophysiology of instability:
When the labrum is torn from the glenoid:
- Loss of the bumper effect - humeral head can translate anteriorly without resistance
- Loss of concavity-compression - labral rim normally deepens the socket
- Capsular laxity - capsule stretches with recurrent instability
- Bone loss - recurrent dislocations cause progressive glenoid erosion and Hill-Sachs lesions
- Proprioceptive deficit - loss of mechanoreceptors in labrum and capsule
Glenoid bone loss:
Critical concept for surgical decision-making:
- Under 15% - subcritical, arthroscopic repair successful
- 15-20% - borderline, consider patient factors (ISIS score)
- Over 20% - critical bone loss, "inverted pear" glenoid, high failure rate with arthroscopy alone
- Over 25% - bone augmentation (Latarjet) mandatory
Classification Systems
Classic Bankart vs Variants
- Description
- Labral tear from glenoid rim
- MRI Appearance
- Labrum detached, fluid in gap
- Treatment Implication
- Standard arthroscopic repair
- Description
- Labral tear with bone fragment
- MRI Appearance
- Bone fragment visible
- Treatment Implication
- ORIF if large, or Latarjet if over 20%
- Description
- Labral tear, periosteum intact
- MRI Appearance
- Labrum appears attached
- Treatment Implication
- May be subtle, can repair arthroscopically
- Description
- Labrum displaced medially
- MRI Appearance
- Labrum on glenoid neck, intact periosteum
- Treatment Implication
- Mobilize before repair
- Description
- Glenoid cartilage and labral tear
- MRI Appearance
- Cartilage defect visible
- Treatment Implication
- Address cartilage, may affect prognosis
ALPSA (Anterior Labroligamentous Periosteal Sleeve Avulsion) can be missed on MRI if you're not looking for it. The labrum appears to be in place but is actually displaced medially on the glenoid neck. Must mobilize before repairing to the rim.
Clinical Presentation and Assessment
- Mechanism: Traumatic anterior dislocation (ABER position)
- Number of dislocations: First-time vs recurrent
- Ease of reduction: Self-reduction suggests severe instability
- Sports and activity level: Contact sports, overhead sports
- Dominant arm: High-demand considerations
- Occupation: Overhead work, manual labor
- Psychological impact: Fear of dislocation (apprehension)
- Instability sensation (feeling of shoulder "coming out")
- Apprehension with certain positions (abduction-external rotation)
- Pain (especially early after dislocation)
- Weakness (secondary to pain or rotator cuff tear)
- Clicking or catching (labral tear, loose body)
Patients may describe a "dead arm" sensation during throwing or overhead activity. This represents a transient subluxation - the shoulder partially dislocates and immediately reduces, causing brief paralysis-like sensation and inability to complete the throwing motion.
Physical examination:
- Technique
- 90deg abduction, external rotation applied
- Positive Finding
- Patient feels shoulder will dislocate, guarding
- Technique
- Posterior force applied during apprehension
- Positive Finding
- Relief of apprehension, increased ER range
- Technique
- Release posterior force from relocation
- Positive Finding
- Return of apprehension sensation
- Technique
- Translate humeral head anteriorly with load
- Positive Finding
- Excessive anterior translation (grade 2-3)
- Technique
- Inferior traction on arm
- Positive Finding
- Inferior translation, sulcus below acromion
- Technique
- Generalized laxity assessment
- Positive Finding
- Score over 4 indicates hyperlaxity
Apprehension test is the gold standard:
- Sensitivity: 50-72%
- Specificity: 96-98%
- Most reliable test for anterior instability
Associated injuries to assess:
- Rotator cuff tear (especially in patients over 40 years)
- Greater tuberosity fracture (on initial X-rays)
- Nerve injury (axillary nerve most common, check sensation over deltoid)
- Vascular injury (rare, check pulses)
Differential diagnosis of the unstable or painful shoulder:
- Distinguishing features
- Traumatic ABER mechanism, anterior apprehension, dead-arm in throwers
- Key test / imaging
- Apprehension/relocation positive; MR arthrogram anteroinferior labral tear
- Distinguishing features
- Seizure, electrocution, axial load on adducted arm; pain in flexion-adduction
- Key test / imaging
- Jerk/Kim test positive; axillary view confirms posterior subluxation
- Distinguishing features
- Overhead athlete, deep-seated pain, clicking; no frank dislocation
- Key test / imaging
- O'Brien and biceps load tests; superior labral signal on MRA
- Distinguishing features
- Atraumatic, bilateral, generalised laxity, voluntary component
- Key test / imaging
- Positive sulcus sign, Beighton over 4; instability in 2 or more directions
- Distinguishing features
- Weakness and night pain rather than apprehension after dislocation
- Key test / imaging
- Drop-arm/Jobe; ultrasound or MRI for cuff integrity
- Distinguishing features
- Older patient, marked pain, limited movement post-reduction
- Key test / imaging
- AP and axillary radiographs; CT for fracture pattern
Investigations
Radiographic assessment:
Plain X-rays (essential first-line):
- AP view in scapular plane: Assess glenoid bone loss, Hill-Sachs
- Axillary lateral: Essential to confirm concentric reduction
- West Point axillary: Profiles anterior-inferior glenoid rim
- Stryker notch view: Profiles Hill-Sachs lesion
Never accept AP view alone. The axillary lateral is mandatory to confirm concentric reduction after dislocation and to assess posterior shoulder pathology. A missed posterior dislocation is a medicolegal disaster.
X-ray findings:
- Hill-Sachs lesion visible on AP (if large) or Stryker notch view
- Glenoid bone loss - loss of pear shape on AP, "inverted pear" if critical
- Bony Bankart fragment - small anterior-inferior glenoid fragment
- Greater tuberosity fracture - more common in older patients
MRI with intra-articular gadolinium (MR arthrogram):
Gold standard for soft tissue assessment:
- Labral tear (Bankart lesion): High signal fluid between labrum and glenoid
- ALPSA lesion: Labrum displaced medially on glenoid neck, intact periosteum
- Perthes lesion: Subtle partial detachment with periosteum intact
- Capsular stretching: Increased capsular volume
- Rotator cuff tear: Assess for concomitant injury (especially over 40 years)
- Hill-Sachs lesion: Size, depth, orientation
- Glenoid bone loss: Can measure, but CT is superior
MR arthrogram (intra-articular gadolinium) is superior to non-contrast MRI for labral tear detection. Sensitivity improves from 82% (non-contrast) to 96% (arthrogram). Always request MRA for suspected Bankart lesion.
CT scan (critical for bone loss assessment):
CT with 3D reconstruction is the gold standard for bone loss quantification:
- Glenoid bone loss percentage (best-fit circle method)
- Hill-Sachs size and location (en face view)
- On-track vs off-track calculation
- Surgical planning for Latarjet or bone grafting
- All recurrent dislocators (assess bone loss before surgery)
- Any suggestion of bony Bankart on X-ray
- ISIS score calculation (need accurate bone loss measurement)
- Preoperative planning for Latarjet procedure
- Dynamic assessment of labrum (operator-dependent)
- Limited role compared to MRI
- May detect labral tear in experienced hands

Management Algorithm
- Neurovascular examination (axillary nerve most at risk)
- X-rays (AP and axillary lateral)
- Closed reduction (multiple techniques available)
- Post-reduction X-rays (confirm concentric reduction)
- Immobilization in sling (traditionally internal rotation, but see below)
- Orthopaedic follow-up within 1-2 weeks
- Stimson technique: Prone, arm hanging with weight
- Cunningham technique: Gentle massage of shoulder girdle muscles
- Milch technique: Arm overhead abduction with gentle traction
- Traction-countertraction: Assistant holds sheet around chest
Traditional immobilization in internal rotation (sling) vs external rotation (ER brace) has been debated. Although early studies suggested an external-rotation brace might reduce recurrence, larger randomised trials and meta-analyses have not confirmed a clinically meaningful difference. Most surgeons use a standard sling for comfort, since definitive stabilisation is the key decision for high-risk patients.
The key is not immobilization position but rather identifying which patients need surgery.
Surgical Technique
Arthroscopic suture anchor repair - Gold standard for soft tissue Bankart
- Beach chair or lateral decubitus (surgeon preference)
- Beach chair: Better anatomic orientation, easier conversion to open
- Lateral: Better distraction, visualization of inferior glenoid
- Posterior portal: Viewing portal (standard, 2cm inferior and 2cm medial to posterolateral acromion)
- Anterior superior portal: Working portal (rotator interval)
- Mid-glenoid portal: Anchor placement portal (at anterior glenoid rim, 5 o'clock position for right shoulder)
- Diagnostic arthroscopy: Confirm Bankart lesion, assess for ALPSA, GLAD, Hill-Sachs
- Preparation of glenoid rim: Use shaver or rasp to create bleeding bone surface
- Mobilization (if ALPSA): Release medially displaced labrum from glenoid neck
- Anchor placement: 3-4 suture anchors at anterior-inferior glenoid rim
- 5:30 position (posteroinferior)
- 4:30-5:00 position (inferior)
- 3:00-3:30 position (anteroinferior)
- Optional 2:00 position (anterosuperior)
- Suture passing: Pass sutures through labrum and capsule
- Knot tying: Secure labrum back to glenoid rim
- Capsular shift (if needed): Plication of stretched capsule
- Closure: Close portals
Anchors must be placed on the articular margin of the glenoid (not medial on the neck). Think "bumper" restoration. If anchors are medial, the labral bumper effect is lost. Place at the 2, 3, 4:30, and 5:30 o'clock positions (right shoulder).
Number of anchors:
- Minimum 3 anchors required
- Most surgeons use 4 anchors for better coverage
- Studies show failure rate increases with fewer than 3 anchors
The systematic placement of anchors from inferior to superior ensures complete anterior-inferior stabilization.
Complications
- Incidence
- 5-10% arthroscopic, 2-5% Latarjet
- Prevention/Management
- Adequate anchor number, assess bone loss preoperatively
- Incidence
- 10-20%
- Prevention/Management
- Early motion protocol, avoid over-tensioning
- Incidence
- 1-2%
- Prevention/Management
- Careful retraction, identify anatomy
- Incidence
- 2-5%
- Prevention/Management
- Proper anchor placement on articular margin
- Incidence
- 10-20%
- Prevention/Management
- Careful repair, preserve tendon quality
- Incidence
- Under 1% arthroscopic, 2-3% open
- Prevention/Management
- Sterile technique, antibiotic prophylaxis
- Incidence
- Rare with modern devices
- Prevention/Management
- Avoid excessive thermal devices
- Most common cause of failure
- Risk factors: Young age, contact sports, inadequate bone loss recognition
- Prevention: Proper patient selection, adequate anchors, bone augmentation if needed
- Treatment: Revision surgery, consider Latarjet if failed arthroscopic repair
- More common with open repair than arthroscopic
- Risk increased with over-tensioning of capsule
- Prevention: Early motion protocol (within first week)
- Treatment: Aggressive physiotherapy, possible manipulation under anesthesia, capsular release
Suture anchor pullout is rare (under 2%) with modern all-suture or PEEK anchors. Risk factors include poor bone quality, anchor placed in glenoid neck (not rim), and inadequate number of anchors. Place anchors on the articular margin with good bone purchase.
Nerve injuries:
- Axillary nerve: At risk during anterior inferior portal creation and inferior capsular dissection
- Musculocutaneous nerve: At risk during Latarjet (in conjoint tendon)
- Prevention: Know anatomy, gentle retraction, identify nerves intraoperatively
- Most are neurapraxia and recover within 6 months
Postoperative Care and Rehabilitation
Arthroscopic Bankart repair protocol:
- Sling immobilization for 4-6 weeks (sleep in sling)
- Remove for hygiene and gentle pendulum exercises only
- No active ROM of shoulder
- Elbow, wrist, hand motion encouraged
- Pain and inflammation control
- Anchor healing phase critical
- Wean from sling at 6 weeks
- Begin passive ROM exercises with physiotherapist
- Avoid combined abduction-external rotation (ABER) position
- Progress to active-assisted ROM by week 10
- No strengthening yet
- Goal: 140 degrees forward elevation, 40 degrees ER by week 12
- Active ROM exercises
- Begin rotator cuff strengthening
- Scapular stabilization exercises
- Progressive resistance band exercises
- Avoid heavy lifting or contact sports
- Full ROM expected by week 16
- Progressive strengthening program
- Sport-specific rehabilitation
- Non-contact sports at 4 months
- Contact sports at 6 months
- Throwing athletes may need 9-12 months
- Full unrestricted activity by 6 months
Latarjet postoperative protocol:
- Sling immobilization for 6 weeks
- Passive ROM allowed after 2-3 weeks (earlier than arthroscopic)
- Bone healing phase
- No active ROM or strengthening
- Active ROM exercises
- Bone healing confirmed on X-ray
- Gentle strengthening begins week 8
- Avoid ABER position
- Progressive strengthening
- Return to non-contact sports at 3-4 months
- Return to contact sports at 6 months
- Full activities by 6 months
Key rehabilitation principles:
- Avoid ABER position for 3 months (position of injury)
- Early passive motion to prevent stiffness
- Delayed active strengthening to protect repair (wait 6 weeks)
- Gradual return to sport to prevent re-injury
- Patient compliance is critical for success
Outcomes and Prognosis
- Overall: 5-10% (modern series)
- Subcritical bone loss (under 15%): 5-8%
- Borderline bone loss (15-20%): 10-15%
- High ISIS score (over 6): 15-30%
- Return to same level of sport: 80-90%
- Patient satisfaction: 85-95%
- Improved ROM compared to open repair
- Lower complication rate than open
- Overall: 2-5% (excellent for high-risk population)
- Critical bone loss: 2-4%
- Revision cases: 5-10%
- Return to sport: 80-90%
- Patient satisfaction: over 90%
- Minimal loss of motion (5-10 degrees external rotation)
- Higher complication rate than arthroscopic (10-15%)
Latarjet has lower recurrence than arthroscopic repair in high-risk patients (young, contact sports, bone loss). For ISIS score over 6 or bone loss over 20%, Latarjet is superior. Accept the higher complication risk for better stability outcome.
- Age: Younger patients higher recurrence
- Bone loss: Critical bone loss (over 20%) needs Latarjet
- Sport level: Competitive contact sports higher risk
- Number of anchors: 3 or more reduces recurrence
- Capsular quality: Stretched capsule increases risk
- Compliance: Rehabilitation adherence critical
- Recurrent instability leads to progressive arthritis
- Early surgical stabilization may prevent arthritis
- Late repair (years after injury) has worse outcomes
- Latarjet long-term arthritis risk unclear (non-anatomic bone block)
Guidelines, Registries & Global Practice
Global epidemiology (PubMed-verified):
- Figure
- 23.9 per 100,000 person-years (US ED data)
- Source
- Zacchilli & Owens, JBJS Am 2010
- Figure
- 20-29 years (47.8 per 100,000); 46.8% aged 15-29
- Source
- Zacchilli & Owens 2010
- Figure
- Male IRR 2.64; 71.8% of dislocations in males
- Source
- Zacchilli & Owens 2010
- Figure
- 48.3% of all dislocations
- Source
- Zacchilli & Owens 2010
- Figure
- 20.7% of instability patients (Hill-Sachs 52.7%)
- Source
- MOON cohort, AJSM 2023
Anterior instability is concentrated in young active men worldwide. Contact and collision codes (rugby union/league, American/Australian football, ice hockey) and overhead/throwing sports dominate, with combat sports and falls contributing in older groups.
Guidance and decision frameworks, side by side:
- Position on first-time dislocation
- Stratify by age/activity; young athletes counselled on high recurrence and early surgical option
- Position on bone loss / recurrence
- Quantify glenoid and humeral bone loss before surgery; bony procedure for critical loss
- Evidence basis
- RCT + cohort (Bottoni/Belk)
- Position on first-time dislocation
- Reduce, confirm with axillary view, early physiotherapy; refer recurrent or high-demand for stabilisation
- Position on bone loss / recurrence
- Specialist imaging (CT/MR) and surgeon-led choice of soft-tissue vs bony repair
- Evidence basis
- Guideline + Level I evidence
- Position on first-time dislocation
- Emphasise glenoid track and ISIS-type risk stratification
- Position on bone loss / recurrence
- Off-track Hill-Sachs and critical glenoid loss favour Latarjet/bone block over isolated repair
- Evidence basis
- Yamamoto track; Burkhart
- Position on first-time dislocation
- Validated pre-op risk score
- Position on bone loss / recurrence
- ISIS over 6 contraindicates arthroscopic repair, recommend Latarjet
- Evidence basis
- JBJS Br 2007 (Level III)
There is broad international agreement on the principles (assess bone loss, risk-stratify, repair the labrum or augment bone) even where named guidelines differ in emphasis.
- The MOON Shoulder Instability prospective multicentre cohort (892 patients) shows recurrent dislocations drive progressive glenoid and humeral bone loss - each additional event raises combined-lesion odds by 95% (AJSM 2023).
- National joint registries (NJR, AOANJRR, AJRR) capture arthroplasty rather than soft-tissue stabilisation, so instability outcome data come chiefly from cohort studies and society registries rather than implant registries.
- High-resource settings: routine CT/MR arthrography, glenoid-track calculation, arthroscopic Bankart +/- remplissage, Latarjet for critical loss.
- Limited-resource settings: open Bankart and open Latarjet remain workhorse procedures where arthroscopy and 3D CT are less available; plain radiographs (AP, axillary, Stryker notch, West Point) carry more diagnostic weight.
- Collision-sport regions (Australasia, South Africa, Europe): lower threshold for early bony stabilisation in elite contact athletes given career impact and high recurrence.
Whatever board you sit, examiners reward the same reasoning chain: confirm reduction on an axillary view, quantify glenoid and humeral bone loss, apply a risk score (ISIS) and the glenoid-track concept, then choose soft-tissue repair vs bony augmentation. Name the evidence (Balg-Boileau, Burkhart, Yamamoto, Bottoni/Belk), not a single country's pathway.
MCQ Practice Points
Q: What is a Bankart lesion? A: A Bankart lesion is a tear of the anterior-inferior glenoid labrum and associated inferior glenohumeral ligament (IGHL) complex, typically occurring at the 3-6 o'clock position (right shoulder). It is the "essential lesion" in traumatic anterior shoulder instability.
Q: What percentage of glenoid bone loss is considered critical and requires bone augmentation rather than isolated arthroscopic repair? A: Over 20% glenoid bone loss is considered critical. This creates an "inverted pear" glenoid shape and predicts high failure rates (over 60%) with isolated arthroscopic Bankart repair. Latarjet or bone block procedures are indicated.
Q: What is the ISIS score and when does it predict high failure with arthroscopic Bankart repair? A: The Instability Severity Index Score (ISIS) predicts recurrence after arthroscopic Bankart based on 6 risk factors: age under 20 (2 points), competitive sports (2 points), contact/overhead sports (1 point), hyperlaxity (1 point), Hill-Sachs on AP (2 points), glenoid bone loss (2 points). Score over 6 predicts over 70% recurrence and suggests Latarjet should be considered.
Q: What is an ALPSA lesion and how does it differ from a classic Bankart? A: ALPSA (Anterior Labroligamentous Periosteal Sleeve Avulsion) is a variant where the labrum is torn but the periosteum remains intact, allowing the labrum to displace medially onto the glenoid neck. Unlike Bankart where labrum is completely avulsed, ALPSA requires mobilization of the medially displaced sleeve before repair to the glenoid rim.
Q: What is the minimum number of suture anchors recommended for arthroscopic Bankart repair? A: Minimum 3 anchors, with most surgeons using 4 anchors for better coverage of the anterior-inferior labrum. Anchors are typically placed at the 2 o'clock, 3 o'clock, 4:30, and 5:30 positions (right shoulder) to restore the labral bumper effect.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An 18-year-old rugby player presents with his third anterior shoulder dislocation. He is a competitive athlete hoping to play at university level. X-rays show a small Hill-Sachs lesion but no obvious glenoid bone loss. He wants surgery. How would you assess and manage this patient?”
“A 25-year-old recreational surfer has his first anterior shoulder dislocation. It was reduced in the ED, post-reduction X-rays show concentric reduction and a small Hill-Sachs lesion. He asks whether he needs surgery. How do you counsel him?”
“A 22-year-old patient had an arthroscopic Bankart repair 18 months ago after recurrent instability. He has now had 2 more dislocations. You obtain a CT scan showing 22% glenoid bone loss and a large engaging Hill-Sachs lesion. How do you approach this complex problem?”
DEFINITION AND KEY FACTS
- Bankart = anterior-inferior labral tear (3-6 o'clock position)
- Essential lesion in traumatic anterior instability (90% of dislocations)
- ALPSA = labrum displaced medially with intact periosteum
- Perthes = labral tear with intact periosteum (partial Bankart)
- Bony Bankart = labral tear with glenoid fracture fragment
BONE LOSS ASSESSMENT (CRITICAL)
- Under 15%: Subcritical - arthroscopic Bankart successful
- 15-20%: Borderline - use ISIS score to guide decision
- Over 20%: Critical inverted pear - Latarjet mandatory
- Over 25%: Severe bone loss - may need bulk bone graft
- CT with 3D reconstruction is gold standard for measurement
ISIS SCORE (PREDICTS RECURRENCE)
- Age under 20 years = 2 points
- Competitive sport = 2 points, contact/overhead = 1 point
- Shoulder hyperlaxity = 1 point
- Hill-Sachs on AP radiograph = 2 points
- Anterior glenoid bone loss = 2 points
- Score over 6 = over 70% recurrence with arthroscopy (consider Latarjet)
ARTHROSCOPIC BANKART REPAIR
- Gold standard for soft tissue Bankart with minimal bone loss
- 3-4 suture anchors at 2, 3, 4:30, 5:30 o'clock positions
- Anchors on articular margin (not medial on neck)
- Success rate: 85-95% in low-risk patients
- Recurrence: 5-10% overall, higher in young contact athletes
LATARJET PROCEDURE
- Indications: over 20% bone loss, ISIS over 6, failed Bankart
- Triple effect: bone block, sling effect, capsular repair
- Coracoid positioned flush with glenoid rim at equator
- Screws perpendicular to glenoid face (not parallel)
- Success: 95-98%, complications: 10-15% (nerve, hardware)
TRAPS AND PEARLS
- Always assess bone loss with CT before surgery
- ISIS score guides surgical decision in borderline cases
- ALPSA requires mobilization before repair
- Engaging Hill-Sachs needs remplissage or Latarjet
- First-time under 20 = 90% recurrence without surgery
- Apprehension test: 96-98% specificity for instability
Evidence Base
- Prospective case-control study of 131 patients undergoing arthroscopic Bankart repair with suture anchors; 14.5% recurrent instability at mean 31 months. Identified 6 pre-operative risk factors (age under 20, competitive/contact/overhead sport, hyperlaxity, Hill-Sachs on AP radiograph, loss of glenoid contour) compiled into a 10-point score. A score over 6 carried a 70% recurrence risk.
- Case series of 194 arthroscopic Bankart repairs. With no significant bone defect the recurrence rate was 4%; with an inverted-pear glenoid or engaging Hill-Sachs it rose to 67%. In contact athletes the contrast was 6.5% versus 89%. Defined the inverted-pear glenoid and the engaging Hill-Sachs as the key bony reasons for arthroscopic failure.
- Cadaveric study (9 shoulders) mapping glenoid-humeral contact in abduction and external rotation. The zone of contact (glenoid track) had a medial margin 18.4 mm from the rotator-cuff footprint, equivalent to 84% of the glenoid width. A Hill-Sachs lesion that extends medial to this margin risks engagement and dislocation (off-track).
- Prospective multicentre MOON cohort of 892 anterior-instability patients. Anterior glenoid bone loss was present in 20.7% and Hill-Sachs lesions in 52.7%. An increasing number of dislocations was the factor most strongly associated with glenoid bone loss, Hill-Sachs lesions and combined lesions - each additional dislocation raised the odds of a combined lesion by 95%.
- Prospective randomised trial in young athletes with a first-time traumatic anterior dislocation. Recurrent instability occurred in 75% (9/12) of non-operatively treated patients versus 11.1% (1/9) after early arthroscopic Bankart repair at mean 36-month follow-up.
- Meta-analysis of 5 Level-1 RCTs (259 patients) for first-time anterior dislocation. Recurrent instability was 6.3% after surgical stabilisation versus 46.6% with immobilisation; subsequent instability surgery was needed in 4.0% versus 30.8% (both p under 0.00001), at mean 60-month follow-up.
- Systematic review of 16 studies (713 shoulders) of the open Latarjet performed as a revision after failed prior stabilisation. Recurrence was 8.4% (redislocation only 0.9%), return to play 95.1%, mean Rowe score 92.7, with an 11% non-recurrence complication rate (nerve injury and infection each 2.1%).