The Unique Hamstring
- Only hamstring muscle that does NOT originate from the Ischial Tuberosity.
- Only hamstring muscle that does NOT cross the Hip Joint (Knee flexor ONLY).
- Innervated by the Common Peroneal Division of the Sciatic Nerve (not Tibial).
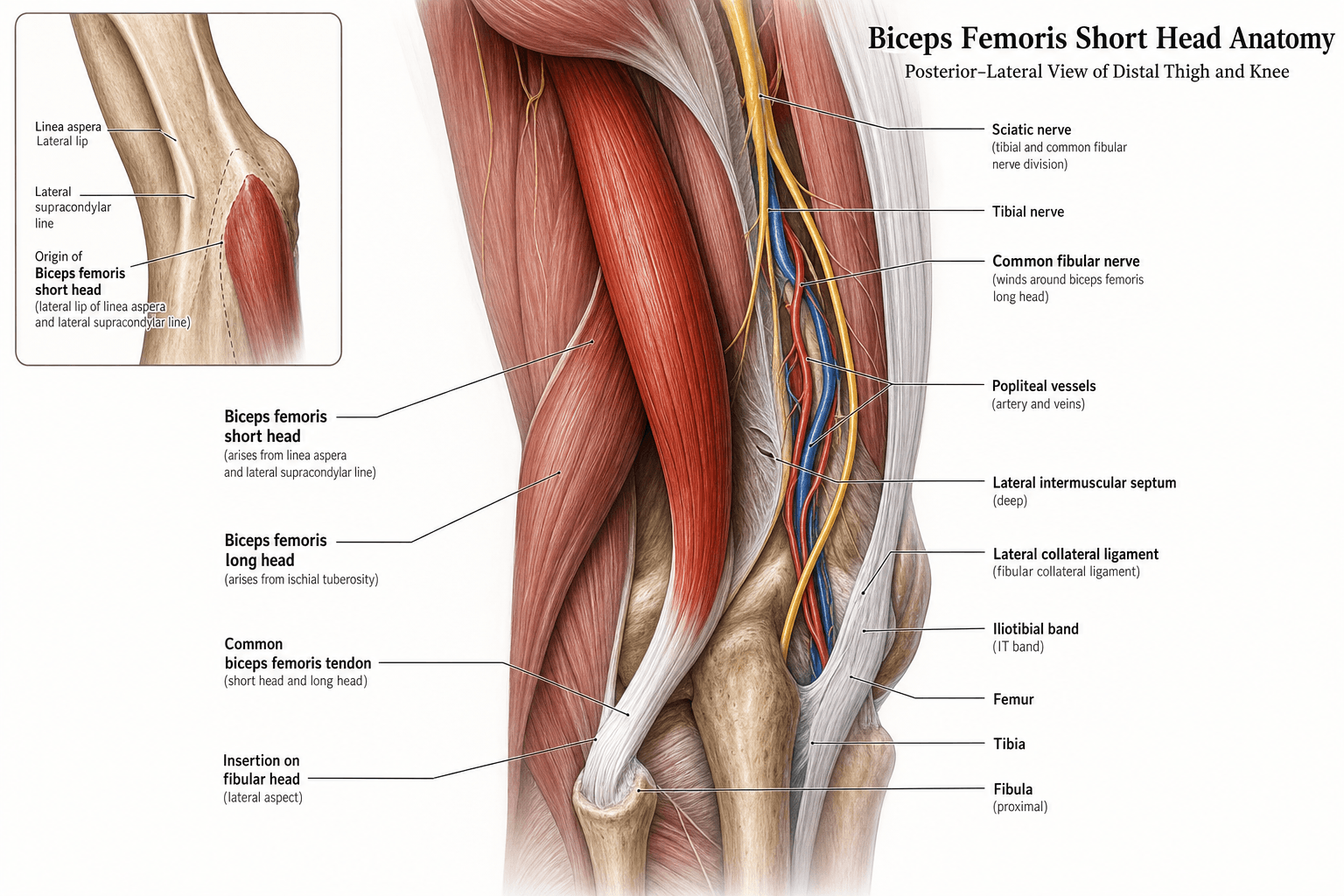
- Originates from the Linea Aspera and Lateral Supracondylar Ridge.
- Joins with Long Head BF to form common tendon inserting on Fibular Head.
- “The Short Head is the key landmark for identifying the Common Peroneal Nerve.
- “Isolated Short Head weakness suggests High Common Peroneal Nerve lesion.
- “The two heads of Biceps Femoris are embryologically different structures.
- “Sciatic Nerve bifurcation typically occurs at the level of the Short Head origin.
Intimate Relationship.
- The CPN runs along the medial border of Biceps Femoris (both heads).
- Risk: Surgical approaches (ITB release, fibular plating) can injure the nerve.
- Tethering: The nerve is tethered at the fibular neck and at the sciatic bifurcation.
- Result: Foot drop.
Variable Location.
- Usually bifurcates at mid-thigh level (near Short Head origin).
- Can occur anywhere from pelvis to popliteal fossa.
- Risk: Assuming standard anatomy during hamstring harvest or THA.
- Consequence: Inadvertent division of nerve if bifurcation is high.
- Short Head BF
- Linea Aspera
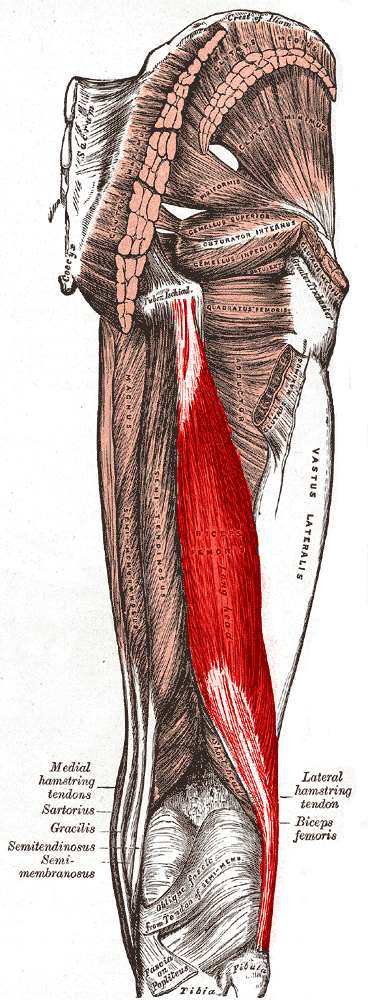
- Long Head BF
- Ischial Tuberosity
- Semitendinosus
- Ischial Tuberosity
- Short Head BF
- None
- Long Head BF
- Extension
- Semitendinosus
- Extension
- Short Head BF
- Flexion + ER
- Long Head BF
- Flexion + ER
- Semitendinosus
- Flexion + IR
- Short Head BF
- Common Peroneal
- Long Head BF
- Tibial
- Semitendinosus
- Tibial
- Short Head BF
- Fibular Head
- Long Head BF
- Fibular Head
- Semitendinosus
- Pes Anserinus
FLEX-ERBiceps Femoris Actions
Hook:Biceps Femoris = Lateral Hamstring = External Rotation.
L-I-SOrigin Difference
Hook:LIS - Short starts Low (Linea), Long from Ischium, Shared tendon.
Overview
The Short Head of Biceps Femoris is anatomically and embryologically distinct from all other hamstring muscles. Unlike the Long Head, Semitendinosus, and Semimembranosus (which all originate from the Ischial Tuberosity and cross both hip and knee), the Short Head arises from the femur itself and acts only at the knee. This distinction makes it clinically important for localizing nerve lesions and understanding hamstring biomechanics.
The muscle belly lies deep to the Long Head and is often not appreciated during superficial dissection. Its primary clinical significance relates to its intimate relationship with the Common Peroneal Nerve.
Detailed Anatomy

Origin
- Linea Aspera: Lateral lip of the linea aspera (middle third of femur).
- Lateral Supracondylar Ridge: Extends proximally along this ridge.
- Lateral Intermuscular Septum: Minor contribution from the septum.
The origin spans approximately the middle third of the femoral shaft, positioned lateral and deep to the Long Head.
Course
- Runs inferolaterally in the posterior compartment of the thigh.
- Lies deep to the Long Head for most of its course.
- Becomes visible laterally in the distal third of the thigh as it joins the Long Head.
Insertion
- Common Bicipital Tendon: Merges with Long Head tendon approximately 7-10 cm proximal to the knee.
- Fibular Head: Inserts on the lateral aspect of the fibular head.
- Expansion: Sends fascial expansion to the lateral collateral ligament and crural fascia.
The common tendon can be palpated as the prominent lateral "hamstring" tendon posterior to the knee.
Beyond flexing the knee, the biceps femoris is a primary dynamic stabiliser of the posterolateral corner (PLC) — high-yield because the PLC and the common peroneal nerve are injured together.
- Conjoined insertion: the long and short heads form a conjoined tendon with several arms — the direct arm to the fibular head, an anterior arm, and reflected/capsular expansions to the lateral collateral ligament, the posterolateral capsule and the iliotibial tract; the short head contributes to the deep capsulo-osseous layer.
- Function: it dynamises the LCL and resists varus and external-rotation (posterolateral) instability, complementing the static PLC stabilisers (LCL, popliteus, popliteofibular ligament).
- Surgical relevance: the biceps tendon is a graft/tenodesis source in PLC reconstruction; and because a PLC injury or knee dislocation tents the common peroneal nerve (tethered at the fibular neck), foot drop frequently accompanies a PLC injury — examine the short head and the peroneal nerve in every PLC case.
SHORT = CPNHamstring Innervation
Hook:SHORT receives Common Peroneal. Everything else = Tibial.
Neurovascular Supply
Nerve Supply
- Common peroneal (fibular) division of the sciatic nerve — roots L5, S1, S2.
- This is the defining feature of the short head: it is the only hamstring not supplied by the tibial division.
- The nerve enters the deep (medial) surface of the muscle in the mid-thigh; the common peroneal division then tracks along the medial border of biceps femoris toward the fibular neck.
Arterial Supply
- Proximal and middle: perforating branches of the profunda femoris artery.
- Distal: superior lateral genicular and popliteal artery branches.
- Segmental supply theoretically permits rotational flap use, though this is rarely performed.
Venous & Lymphatic
- Venous drainage follows the accompanying perforating and popliteal veins.
- Lymphatic drainage is to the deep inguinal and popliteal nodal chains.
Functional Anatomy
Primary Actions
- Knee Flexion: Prime mover (with Long Head and other hamstrings).
- Lateral (External) Rotation of Tibia: When knee is flexed, rotates tibia laterally on femur.
No Hip Action
Because the Short Head does not cross the hip joint, it has NO action on the hip. This is unique among hamstrings and explains why isolated Short Head weakness does not affect hip extension.
Functional Significance
- Knee Stability: Contributes to lateral stabilization of the knee.
- Gait: Active during terminal swing phase to decelerate knee extension.
- Posture: Minimal role compared to Long Head (no hip control).
The Short Head acts primarily as a knee flexor without the hip extension function of other hamstrings.
Pathology
Short Head Strain
- Incidence: Accounts for less than 10% of hamstring strains.
- Mechanism: Eccentric overload during terminal swing phase of sprinting.
- Location: Usually mid-belly (not proximal like Long Head).
Clinical Features
- Pain: Lateral posterior thigh pain.
- Weakness: Knee flexion weakness (subtle, as Long Head compensates).
- Palpation: Tenderness in lateral thigh (mid-level).
Differential
- Long Head strain (more common, proximal).
- ITB syndrome (lateral, not posterior).
- Lateral femoral cutaneous nerve compression (numbness, no weakness).
Short Head strains are managed conservatively like other hamstring injuries.
Clinical Significance
Diagnostic Value.
- Isolated Short Head weakness + foot drop = High Common Peroneal Nerve lesion.
- Preserved Short Head with foot drop = Low CPN lesion (fibular neck).
- Weak Short Head + weak Long Head = Sciatic Nerve lesion (or L5/S1 root).
Operative Landmark.
- CPN tracking: Runs along medial border of Biceps Femoris.
- Fibular plating: Protect nerve deep to muscle.
- Hamstring harvest: Short Head NOT harvested (too short, wrong nerve).
Injury Patterns
- Hamstring Strain: Short Head strains are LESS common than Long Head or Proximal Hamstring injuries.
- Mechanism: Usually mid-substance tears during sprinting (eccentric load).
- Presentation: Lateral thigh pain, weakness of knee flexion.
Sciatic Bifurcation Variations
- Common pattern: A single-trunk sciatic nerve exits below piriformis in ~85% of limbs; the division most often occurs distally, a mean of ~65 mm proximal to the popliteal fossa (Tomaszewski, J Orthop Res 2016).
- Anomalous course: The nerve deviates from the classic pattern in nearly 15% of limbs, including intrapelvic split with the common peroneal division piercing piriformis (~10%).
- Clinical Impact: A high or anomalous bifurcation increases common peroneal vulnerability during gluteal, posterior thigh and hip approaches.
Differential Diagnosis of Foot Drop / Lateral Thigh Symptoms
- Short Head Status
- Normal
- Discriminating Feature
- Foot drop, weak eversion, intact knee flexion; Tinel at fibular neck
- Short Head Status
- Weak
- Discriminating Feature
- Foot drop PLUS weak short head; lesion proximal to mid-thigh muscle entry
- Short Head Status
- Variable (L5 input)
- Discriminating Feature
- Weak hip abduction and EHL, back/radicular pain, paraspinal denervation on EMG
- Short Head Status
- Normal
- Discriminating Feature
- Proximal posterior thigh pain, no neurological deficit, no foot drop
- Short Head Status
- Normal
- Discriminating Feature
- Lateral knee pain on flexion-extension, no weakness, no sensory loss
- Short Head Status
- Normal
- Discriminating Feature
- Pain out of proportion, tense compartment; or central/cauda findings
Once the common peroneal (fibular) nerve passes the short head and winds round the fibular neck, it divides into two branches — knowing the split completes the foot-drop localisation the short head begins:
- Deep peroneal nerve: motor to tibialis anterior, extensor hallucis longus, extensor digitorum longus and peroneus tertius (ankle and toe dorsiflexion); sensation to the first web space. Its loss is the main cause of the foot drop.
- Superficial peroneal nerve: motor to peroneus longus and brevis (foot eversion); sensation to the lateral leg and dorsum of the foot (sparing the first web space).
- Localisation: a high lesion (proximal to the short head's mid-thigh entry) weakens the short head AND both branches; a fibular-neck lesion spares the short head; a deep-branch-predominant pattern (dorsiflexion weak, eversion relatively spared) is common in early or partial compression and can mimic an L5 radiculopathy — distinguish with the short head, hip abductors and EMG.
Investigations
Physical Examination
- Inspection: Look for muscle wasting in lateral thigh (chronic denervation).
- Palpation: Palpate for tenderness (strain) or mass (hematoma).
- Strength Testing: Resisted knee flexion with tibia externally rotated.
Specific Tests
- Knee Flexion Strength: Compare to contralateral side.
- Foot Drop Assessment: If present, indicates CPN involvement.
- L5 Radiculopathy Tests: Straight leg raise, EHL strength, ankle dorsiflexion.
Clinical examination is usually sufficient for diagnosis.
Management Strategy
Conservative Management
- Action
- RICE, analgesia, protected weight bearing
- Timeline
- Immediate
- Action
- Gentle stretching, isometric strengthening
- Timeline
- Week 1-2
- Action
- Progressive eccentric loading, running
- Timeline
- Week 2-6
- Action
- Sport-specific training, gradual return
- Timeline
- Week 6-12
- Eccentric Training: Nordic hamstring curls are the gold standard for prevention and rehabilitation.
- Criteria for RTP: Full strength, full ROM, sport-specific functional tests.
Surgery is rarely indicated for Short Head strains.
Complications
- Chronic Pain: Persistent lateral thigh pain after strain (rare, usually resolves).
- Re-injury: Higher risk if return to sport is premature (less than 6 weeks).
- Nerve Injury: CPN palsy from surgical trauma (fibular plating, knee dislocation reduction).
- Contracture: Achilles contracture if foot drop not managed with AFO.
Rehabilitation Protocol
- Phase 1 (Acute): RICE, pain control, gentle ROM.
- Phase 2 (Subacute): Progressive stretching, isometric strengthening.
- Phase 3 (Strengthening): Eccentric loading (Nordic curls), concentric exercises.
- Phase 4 (Return to Sport): Plyometrics, sport-specific drills, gradual return.
Key Exercises
- Nordic Hamstring Curl: Eccentric loading to prevent re-injury.
- Single-Leg Deadlift: Functional strengthening.
- Sprint Mechanics: Gradual return to high-speed running.
Prognosis
- Hamstring Strain: 90% return to sport within 6-12 weeks with conservative management.
- CPN Palsy: 70-80% spontaneous recovery if nerve intact (observation for 6 months).
- Surgical Nerve Repair: Variable outcomes depending on gap and timing (40-60% useful recovery).
Guidelines, Registries & Global Practice
Global Epidemiology
- Hamstring strain burden: Hamstring injury is the single most common time-loss injury in football/soccer worldwide, with biceps femoris involved in roughly 80% of strains and accounting for essentially all re-injuries (Ekstrand, Br J Sports Med 2012).
- Short head share: Isolated short head strains are uncommon relative to proximal long-head/myotendinous injuries, but the biceps femoris long-head muscle-tendon junction is the dominant strain site across all sporting populations.
- Common peroneal nerve palsy: Reported in up to 50% of knee dislocations and is a leading driver of poor functional outcome after multiligament knee injury (Cush, Sports Med Arthrosc Rev 2011).
Side-by-Side Guideline & Society Positions
- Domain
- Strain classification
- Recommendation
- MRI grading (Peetrons / British Athletics) stratifies lay-off and return-to-play; intramuscular tendon involvement extends recovery
- Domain
- Prevention
- Recommendation
- Eccentric Nordic hamstring programme endorsed as primary prevention in elite and amateur football
- Domain
- CPN palsy after knee dislocation
- Recommendation
- Early documentation, expectant management if nerve in continuity, AFO to prevent equinus; explore for laceration or no recovery
- Domain
- Foot drop rehab
- Recommendation
- Ankle-foot orthosis and supervised physiotherapy as first-line; tendon transfer for permanent palsy
Practice Variation: High vs Limited Resource
- High-resource settings: Routine MRI grading for prognosis, EMG/nerve conduction studies to localise peroneal lesions, microsurgical nerve grafting and intra-operative nerve monitoring during complex knee or hip reconstruction.
- Limited-resource settings: Diagnosis rests on clinical localisation (short head function distinguishes high from low common peroneal lesions); management centres on a low-cost ankle-foot orthosis and physiotherapy, with tendon transfer reserved for established permanent palsy where microsurgery is unavailable.
Exam Focus
- Short head anatomy and its common peroneal innervation is a classic basic-science viva question across FRCS (Tr & Orth), FRACS, EBOT/FEBOT, ABOS and DNB/MS examinations. The reliable discriminator examiners seek is the use of short head function to separate a high (proximal) from a low (fibular neck) common peroneal lesion.
Controversies & Areas of Uncertainty
- Bifurcation level is genuinely variable. Older teaching of a fixed "mid-thigh" sciatic split overstates consistency; cadaveric series place most divisions far more distally near the popliteal fossa, while others split high in the pelvis. The short head innervation point is therefore a more reliable surgical landmark than any single quoted bifurcation level.
- Timing of surgery for peroneal palsy after knee dislocation. Early exploration versus expectant management remains debated. Most palsies in nerves in continuity are observed for several months, but late intervention has a poor prognosis, so the optimal window is contested.
- Embryological "dual origin" of biceps femoris. The two heads arise from different myotomal/innervation territories (long head from the tibial-supplied flexor mass, short head from the peroneal-supplied extensor-derived mass), which underpins the split innervation. The precise developmental explanation is still discussed in the anatomical literature.
- Short head as a flap or graft. Although a segmental blood supply theoretically permits rotational use, the short head is essentially never harvested for ACL grafting (inadequate length, wrong nerve) and is rarely used as a flap; its surgical relevance is overwhelmingly as a nerve-localising landmark.
MCQ Practice Points
Q: Which nerve innervates the Short Head of Biceps Femoris? A: Common Peroneal Nerve. (All other hamstrings: Tibial Nerve)
Q: Where does the Short Head of Biceps Femoris originate? A: Linea Aspera (lateral lip) and Lateral Supracondylar Ridge. (NOT Ischial Tuberosity)
Q: Does the Short Head of Biceps Femoris extend the hip? A: No. It only crosses the knee joint, so it only flexes the knee.
Q: A patient has foot drop and weak Short Head of Biceps Femoris. Where is the lesion? A: High Common Peroneal Nerve lesion (proximal to Short Head innervation).
Q: Where does the Short Head of Biceps Femoris insert? A: Fibular Head (via common tendon with Long Head).
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Which hamstring muscle has a different nerve supply from the others, and what is that nerve?”
“What makes the Short Head of Biceps Femoris unique among the hamstring muscles?”
“A patient has foot drop. Knee flexion strength is normal. Where is the Common Peroneal Nerve lesion?”
Anatomy
- Origin: Linea Aspera
- Insert: Fibular Head
- Nerve: Common Peroneal
- Roots: L5, S1, S2
Function
- Action: Knee Flexion ONLY
- No Hip Extension
- Lateral Rotation of Tibia
- Only 1-joint hamstring
Clinical
- CPN runs medial border
- Weak + foot drop = High CPN
- Normal + foot drop = Low CPN
- Rarely injured vs Long Head
Evidence Base
Surgical Anatomy of the Sciatic Nerve: A Meta-Analysis
- Pooled analysis of 45 studies and 7068 lower limbs - the largest dataset on sciatic anatomy
- Normal Type A pattern (single trunk exiting below piriformis) in 85.2%; the nerve deviates from this course in nearly 15%
- Mean distance of bifurcation into tibial and common fibular divisions was 65.4 mm proximal to the popliteal fossa
- Type B (intrapelvic split, common peroneal piercing piriformis) in 9.8%
Sciatic Nerve Bifurcation Level: A Cadaveric Cohort
- 338 formalin-fixed limbs dissected with a reproducible bifurcation level index
- Bifurcation in the popliteal fossa (Type F) was most common at 79.6%
- No intrapelvic bifurcations (Types B and C) were observed in this cohort
- Provides a quantifiable framework for comparing bifurcation level across populations
Hamstring Injuries in Professional Football: MRI and Return to Play
- Prospective cohort of 516 hamstring injuries across 23 European professional teams
- Biceps femoris was the injured muscle in 83% of cases; every re-injury (16% of all injuries) occurred in biceps femoris
- Higher modified Peetrons MRI grade predicted longer lay-off (8, 17, 22 and 73 days for grades 0 to 3)
- 70% of injuries were grade 0 or 1 with no fibre disruption yet caused most absence days
Nordic Hamstring Exercise Prevents Acute Hamstring Injury (RCT)
- Cluster-randomised controlled trial of 942 male soccer players (50 teams)
- Eccentric Nordic hamstring training cut overall acute hamstring injuries by ~70% (rate ratio 0.29, 95% CI 0.15-0.57)
- Recurrent injuries reduced most dramatically (rate ratio 0.14); number needed to treat to prevent one recurrence was 3
- Number needed to treat to prevent any acute hamstring injury was 13 players
Nordic Hamstring Exercise in Amateur Soccer (RCT)
- Randomised controlled trial of 579 male amateur players from 40 teams
- Nordic hamstring exercise reduced injury risk (odds ratio 0.28, 95% CI 0.11-0.72; P = .005)
- Injury incidence fell from 0.8 to 0.25 per 1000 player-hours
- Programme compliance was 91%, confirming feasibility outside elite settings
Drop Foot After Knee Dislocation: Evaluation and Treatment
- Common peroneal nerve palsy incidence after knee dislocation reported as high as 50%
- Palsy is most associated with open and rotatory dislocations and posterolateral corner injury
- Late surgical nerve treatment carries a poor prognosis; early documentation and follow-up are critical
- Reconstructive options include neurolysis, repair, grafting and posterior tibial tendon transfer