SLAP Lesions | Biceps Tendinitis | Pulley Lesions | Tenotomy vs Tenodesis
- Anatomy: Intra-articular portion 3-4cm, passes through rotator interval (biceps pulley system)
- SLAP Type II most clinically significant - detachment of biceps anchor from superior labrum
- Clinical triad: Speed test (flexion resistance), Yergason (supination resistance), O'Brien (active compression)
- Age-based treatment: Under 40 = repair SLAP, over 40-50 = consider tenodesis/tenotomy
- Pulley lesions (medial sling damage) cause instability - require repair or tenodesis
- “SLAP = Superior Labrum Anterior to Posterior
- “Type II SLAP is biceps anchor detachment - most common surgical lesion
- “MRA gold standard for SLAP diagnosis (sensitivity 90%)
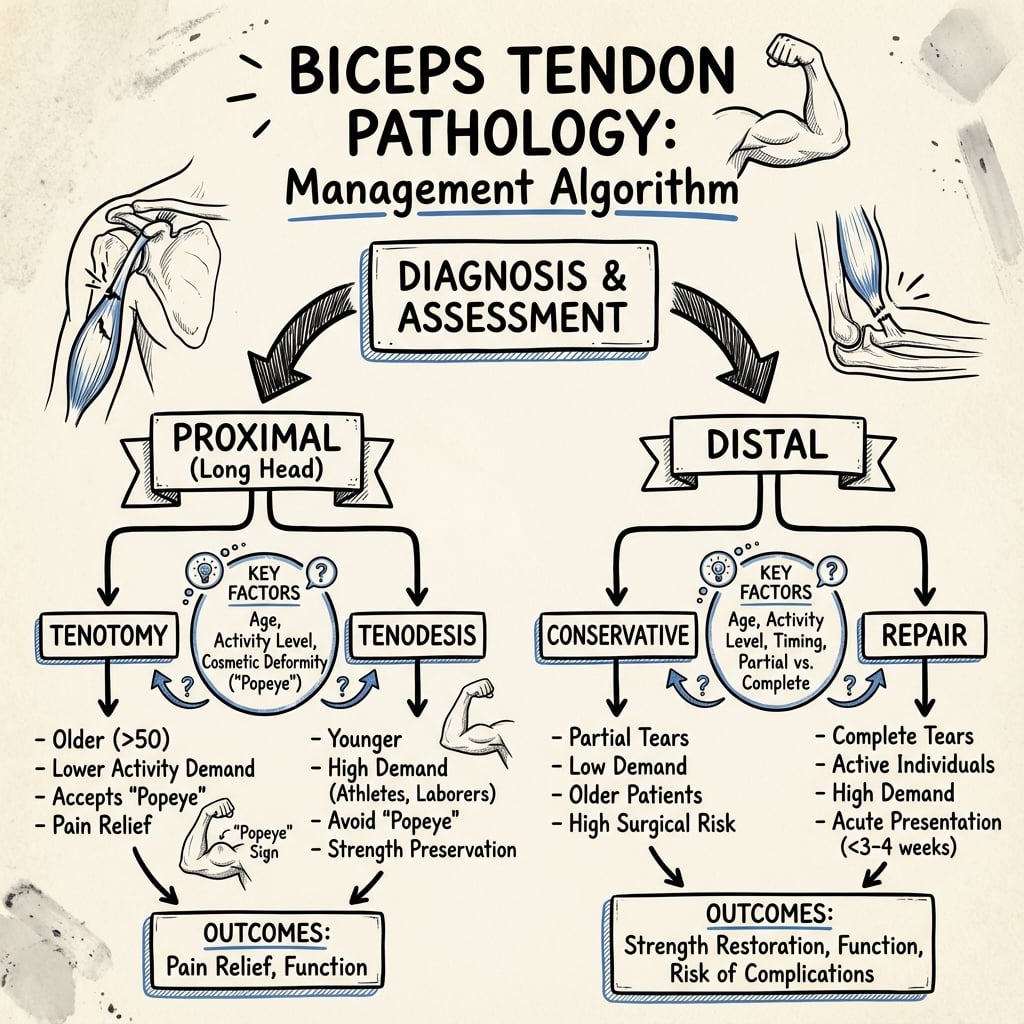
- “Tenotomy vs tenodesis: age, activity level, cosmesis are key factors
- “Associated RTC tears in 30% - always evaluate cuff in biceps pathology
Type II SLAP lesion is detachment of the biceps anchor from the superior labrum. This is the most clinically significant type requiring surgical decision-making. Younger athletes may benefit from repair, older patients from tenodesis.
Age over 40-50 years shifts treatment toward tenodesis or tenotomy rather than SLAP repair. Outcomes of SLAP repair in older patients are inferior. Consider activity level and cosmetic concerns.
The biceps pulley (SGHL, CHL, subscapularis) stabilizes the biceps in the groove. Medial subluxation occurs with pulley lesions. Look for associated subscapularis tears - these create combined instability.
30% of biceps pathology occurs with rotator cuff tears. The biceps acts as a secondary humeral head depressor. Isolated biceps symptoms may be from underlying cuff pathology - always evaluate the cuff.
- Age/Activity
- Under 40, athlete
- First-Line Treatment
- Arthroscopic SLAP repair
- Backup Options
- Tenodesis if repair fails
- Age/Activity
- Over 40-50, recreational
- First-Line Treatment
- Biceps tenodesis
- Backup Options
- Tenotomy if low demand
- Age/Activity
- Any age
- First-Line Treatment
- Conservative (NSAIDs, physio, injection)
- Backup Options
- Tenodesis if failed conservative
- Age/Activity
- Any age, active
- First-Line Treatment
- Subpectoral tenodesis
- Backup Options
- Suprapectoral if young athlete
- Age/Activity
- Any age
- First-Line Treatment
- Tenotomy or tenodesis
- Backup Options
- Debridement if under 25%
PULLEYPULLEY - Biceps Stabilizing Structures
Hook:The PULLEY system prevents medial subluxation of the biceps tendon
TENODESISTENODESIS vs TENOTOMY Decision Factors
Hook:ACTIVE decision-making balances age, cosmesis, activity level, and tissue quality
Overview and Epidemiology
Long head of biceps (LHB) pathology encompasses a spectrum of conditions affecting the intra-articular and proximal extra-articular portions of the biceps tendon. These include SLAP lesions, tendinitis, instability, and partial or complete tears.
Clinical significance:
- Common cause of anterior shoulder pain
- Often associated with rotator cuff pathology
- Can be primary or secondary to other shoulder conditions
- Treatment has evolved significantly with age-based algorithms
Biceps pathology can be primary (isolated tendinitis, SLAP tear) or secondary to rotator cuff disease, glenohumeral instability, or impingement. Secondary pathology is more common in patients over 40. Always evaluate for underlying shoulder conditions.
- SLAP lesions: Traction injury (fall on outstretched hand), repetitive overhead activity (throwing, swimming)
- Biceps tendinitis: Overuse, impingement, instability
- Pulley lesions: Trauma, subscapularis tears, chronic instability
- Overhead athletes (baseball pitchers, swimmers, tennis players)
- Repetitive lifting activities
- Age over 40 (degenerative changes)
- Shoulder instability
- Rotator cuff disease
Pathophysiology and Mechanisms

Long head of biceps anatomy:
The LHB has four distinct anatomical zones:
- Intra-articular portion (3-4 cm) - from superior labrum to bicipital groove entrance
- Extra-articular proximal - within the bicipital groove
- Musculotendinous junction - distal to groove
- Muscle belly - continues to radial tuberosity
The intra-articular portion of the LHB is unique - it is the only tendon coursing through a synovial joint without a synovial sheath in its intra-articular segment. This makes it vulnerable to inflammatory processes affecting the glenohumeral joint.
Biceps anchor and superior labrum:
- LHB originates from superior glenoid labrum (50-60% posterior, 40-50% anterior)
- Also attaches to supraglenoid tubercle of scapula
- Type of attachment varies (entirely posterior, entirely labral, or mixed)
- Normal anatomical variants can mimic SLAP lesions
The biceps pulley system:
Critical stabilizing structure preventing medial subluxation:
- Superior glenohumeral ligament (SGHL) - forms superior roof
- Coracohumeral ligament (CHL) - reinforces laterally
- Superior subscapularis fibers - forms medial sling
- Supraspinatus fibers - contributes laterally
Damage to the medial sling (superior subscapularis and SGHL) allows medial subluxation of the biceps tendon. This creates a "pseudolaxity" pattern. Look for associated subscapularis tears - these are combined pulley lesions requiring different management than isolated biceps pathology.
- Bounded by lesser tuberosity (medial) and greater tuberosity (lateral)
- Intertubercular ridge height varies (shallow groove = instability prone)
- Transverse humeral ligament - spans the groove, holds biceps
- Average depth 4-6 mm, width 9-10 mm
- Elbow flexion - primary function with short head
- Forearm supination - works with supinator
- Secondary humeral head depressor - particularly with rotator cuff deficiency
- Anterior shoulder stabilizer - controversial role in glenohumeral stability
- Anterior humeral circumflex artery - primary supply
- Tendon relatively avascular in intra-articular zone - predisposes to degeneration
- Watershed area at bicipital groove entrance - common tear location
Classification Systems
Snyder Classification of SLAP Lesions (1990, expanded to 10 types)
Original Four Types:
- Description
- Degenerative fraying, stable anchor
- Treatment
- Debridement
- Description
- Biceps anchor detachment from labrum
- Treatment
- Repair (young) or tenodesis (older)
- Description
- Bucket-handle tear, stable biceps anchor
- Treatment
- Excise unstable portion, preserve anchor
- Description
- Bucket-handle tear extending into biceps tendon
- Treatment
- Repair or tenodesis based on extent
Type II Subtypes (Morgan 1998):
- Pattern
- Anterior extension
- Clinical Significance
- May be associated with instability
- Pattern
- Posterior extension
- Clinical Significance
- Most common throwing athlete pattern
- Pattern
- Anterior and posterior
- Clinical Significance
- Complex tear, surgical challenge
SLAP Type II represents true detachment of the biceps-labral anchor. This is the most clinically significant type because it creates instability of the biceps origin. Decision between repair and tenodesis depends heavily on patient age and activity level.
Extended Types V-X (less common):
- Type V: Bankart lesion extending to SLAP
- Type VI: Unstable labral flap
- Type VII: Extension into middle glenohumeral ligament
- Type VIII: Extension into posterior labrum
- Type IX: Circumferential labral tear
- Type X: Extension into rotator interval
These extended types are rare and primarily of academic interest.
Before calling a superior labral finding a SLAP tear, exclude the normal anatomical variants of the antero-superior labrum, because "repairing" them produces a painful, stiff shoulder. Three are classic: (1) the sublabral recess (sulcus) — a smooth, cartilage-lined cleft beneath the biceps-labral anchor that follows the glenoid contour (a true SLAP tear is irregular, extends posteriorly and shows granulation/displacement); (2) the sublabral foramen — an unattached but otherwise normal antero-superior labrum with a hole between it and the glenoid (present in roughly 10% of shoulders); and (3) the Buford complex — a cord-like middle glenohumeral ligament with congenital absence of the antero-superior labrum (around 1-2%). The danger: surgically reattaching a sublabral foramen or a Buford complex tethers the MGHL and causes marked loss of external rotation and pain. The discriminators are location (variants are antero-superior; a true SLAP is at or behind the biceps anchor), smooth versus frayed edges, and whether the "tear" follows the normal articular contour. The exam point: a Buford complex and a sublabral foramen are left alone, not repaired.
SLAPSLAP - Superior Labrum Tear Classification
Hook:SLAP describes the location and direction of the labral tear involving the biceps anchor
Clinical Presentation and Examination
History:
- Pain location: Anterior shoulder, bicipital groove tenderness
- Mechanism: Acute (fall on hand, sudden load) vs chronic (overuse)
- Occupation/sport: Overhead athletes, manual laborers
- Symptoms: Night pain, catching, popping sensation (SLAP), weakness
- Previous treatments: Injections, physiotherapy
Physical examination:
- Technique
- Shoulder flexion 90deg, elbow extended, forearm supinated. Resist forward flexion.
- Positive Finding
- Pain in bicipital groove
- Sensitivity/Notes
- Sensitivity 90%, most sensitive test
- Technique
- Elbow 90deg flexed, forearm pronated. Resist supination and elbow flexion.
- Positive Finding
- Pain in bicipital groove or biceps subluxation
- Sensitivity/Notes
- Sensitivity 43%, tests stability
- Technique
- Arm forward flexed 90deg, adducted 10deg, internally rotated (thumb down). Resist forward flexion. Repeat with forearm supinated.
- Positive Finding
- Pain with thumb down, relief with palm up
- Sensitivity/Notes
- For SLAP lesions, specificity 90%
- Technique
- Supine, shoulder abducted 90deg, elbow flexed 90deg, forearm supinated. Resist elbow flexion while externally rotating shoulder.
- Positive Finding
- Increased apprehension or pain
- Sensitivity/Notes
- For SLAP in patients with instability
- Technique
- Elbow 90deg, forearm supinated. Patient performs uppercut motion against resistance.
- Positive Finding
- Pain in bicipital groove
- Sensitivity/Notes
- Good for proximal biceps pathology
- Technique
- Direct palpation of groove with arm in 10deg internal rotation.
- Positive Finding
- Point tenderness over groove
- Sensitivity/Notes
- Simple, low specificity but useful
No single test is definitive. Combine tests for better accuracy. A positive Speed test + O'Brien test is highly suggestive of biceps-labral pathology. Add imaging (MRA) for definitive diagnosis.
- Rotator cuff testing - Jobe, external rotation lag, hornblower
- Impingement signs - Neer, Hawkins-Kennedy
- Instability testing - Apprehension, relocation, load-shift
- AC joint - cross-arm adduction
- Popeye deformity - complete LHB rupture, distal muscle belly retraction
- Audible snap/pop - biceps instability with arm movement
- Tenderness - bicipital groove, anterior shoulder
- Distinguishing Features
- Bicipital-groove tenderness, pain with overhead/throwing, catching
- Best Test / Investigation
- Speed/O'Brien tests, MR arthrography for SLAP
- Distinguishing Features
- Painful arc, weakness, night pain, positive Jobe/Hawkins; coexists in ~30%
- Best Test / Investigation
- Neer/Hawkins, cuff strength testing, MRI or ultrasound
- Distinguishing Features
- Anterior pain, increased passive external rotation, positive belly-press/lift-off, biceps medial subluxation
- Best Test / Investigation
- Belly-press and lift-off tests, MRI, arthroscopy
- Distinguishing Features
- Pain localised to AC joint, positive cross-body adduction, tenderness over AC joint
- Best Test / Investigation
- Cross-arm adduction test, AC joint injection, plain radiograph
- Distinguishing Features
- Sense of slipping, apprehension, younger patient, labral injury
- Best Test / Investigation
- Apprehension/relocation tests, MR arthrography
- Distinguishing Features
- Global loss of active AND passive ROM, especially external rotation; diabetic association
- Best Test / Investigation
- Clinical (restricted passive ROM), normal radiograph
- Distinguishing Features
- Neck pain, radiation below elbow, dermatomal sensory change, neck movement reproduces pain
- Best Test / Investigation
- Spurling test, neurological exam, cervical MRI
- Distinguishing Features
- Acute severe pain, calcium deposit in cuff or groove
- Best Test / Investigation
- Plain radiograph / ultrasound showing calcific deposit
Anterior shoulder pain is rarely isolated biceps pathology. Always exclude rotator cuff and subscapularis tears (the biceps is a secondary head depressor and frequently a co-existing pain generator), screen for adhesive capsulitis by checking passive range, and rule out cervical radiculopathy when pain radiates below the elbow or there are neurological signs.
SPEEDSPEED Test - Clinical Examination
Hook:SPEED test evaluates the long head of biceps - most sensitive clinical test for biceps tendinitis
Investigations and Imaging
Plain radiographs:
Standard shoulder series (AP, scapular Y, axillary):
- Usually normal in isolated biceps pathology
- May show calcific tendinitis in groove
- Assess for other pathology (arthritis, AC joint, fracture)
Ultrasound:
Advantages:
- Dynamic assessment - can visualize subluxation with arm movement
- Cost-effective, readily available
- Good for bicipital groove pathology
Findings:
- Tendinopathy (thickening, hypoechoic changes)
- Fluid in tendon sheath
- Partial or complete tears
- Subluxation with dynamic imaging
Ultrasound is excellent for bicipital groove pathology (tendinitis, partial tears, instability) but poor for SLAP lesions. The intra-articular biceps origin cannot be adequately assessed with ultrasound. Use MRA for suspected SLAP tears.
MRI/MRA (Magnetic Resonance Arthrography):
Gold standard for SLAP lesions and intra-articular pathology.
Standard MRI findings:
- T2 hyperintensity around biceps (tendinitis)
- Partial or complete tendon tears
- Associated rotator cuff tears
- Labral pathology
MRA (with gadolinium injection):
- Sensitivity 90% for SLAP lesions
- Specificity 95%
- Better delineation of labral detachment
- Identifies extent and type of SLAP
For suspected SLAP lesions, MRA is superior to standard MRI. The intra-articular contrast outlines the biceps anchor and labral detachment. Standard MRI has lower sensitivity (60-70%) and may miss SLAP II lesions.
MRI/MRA findings by pathology:
- MRI Finding
- Fluid signal extending under biceps anchor on coronal images
- MRI Finding
- T2 hyperintensity, tendon thickening
- MRI Finding
- Partial discontinuity, increased signal
- MRI Finding
- Empty groove, retracted tendon
- MRI Finding
- Tendon medial to lesser tuberosity
- MRI Finding
- SGHL/CHL tear, subscapularis partial tear
Diagnostic arthroscopy:
Remains the gold standard for definitive diagnosis and treatment.
Advantages:
- Direct visualization of biceps, labrum, cuff
- Dynamic assessment of stability
- Therapeutic (can debride, repair at same setting)
Findings:
- SLAP lesion type and extent
- Biceps quality (degenerative vs healthy)
- Associated cuff tears, labral tears
- Pulley integrity assessment
A common diagnostic trap is that the most symptomatic part of the long head of biceps lies in the extra-articular bicipital groove, which is NOT seen on standard intra-articular glenohumeral arthroscopy — the scope visualises only the intra-articular segment and the biceps-labral anchor. Significant groove tendinopathy, fraying, partial tearing and instability can therefore be missed if the surgeon inspects only the joint. To assess it, the extra-articular tendon must be pulled into the joint with a probe (the arthroscopic "traction" manoeuvre) to deliver the hidden groove portion for inspection, and the pulley/medial sling examined for subtle subluxation. The same point explains why bicipital-groove palpation, dynamic ultrasound and MRI of the groove add value over arthroscopy alone, and why a normal-looking intra-articular biceps does not exclude symptomatic groove disease. The exam point: think of the biceps in zones — the painful one is often the one you cannot see from inside the joint.
Management Algorithm
Indications:
- Biceps tendinitis without instability
- Partial tears under 25%
- SLAP I lesions (degenerative fraying)
- Elderly patients with low functional demands
Conservative treatment protocol:
- Rest from aggravating activities (overhead, lifting)
- NSAIDs for pain and inflammation
- Ice therapy
- Activity modification
- Gentle pendulum exercises
- Progressive ROM exercises
- Rotator cuff strengthening
- Scapular stabilization
- Posterior capsule stretching
- Eccentric biceps exercises
- Sport-specific rehabilitation
- Return to overhead activities gradually
- Maintenance strengthening program
- Ergonomic modifications for work
Corticosteroid injection:
- Can be used for bicipital groove tendinitis
- Risk of tendon rupture if repeated injections
- Avoid injection into tendon substance
- Maximum 2-3 injections with 3-month intervals
Avoid repeated steroid injections into the bicipital groove. Multiple injections increase risk of complete tendon rupture. If symptoms recur after 2 injections, consider surgical options.
Success rates:
- 40-50% resolution with conservative treatment
- Higher success in older, low-demand patients
- SLAP lesions in young athletes rarely resolve without surgery
Conservative management remains the foundation of treatment for patients over 40 years of age.
Surgical Technique
Indications:
- SLAP Type II in patients under 40
- Overhead athletes (throwing, swimming)
- Healthy labral and biceps tissue
- Failed conservative management 3-6 months
Arthroscopic technique:
Step 1: Diagnostic arthroscopy
- Standard posterior viewing portal
- Assess biceps anchor stability (probe test - peel-back sign)
- Confirm SLAP type and extent
- Evaluate associated pathology (cuff, labrum, cartilage)
Step 2: Preparation
- Debride frayed labral tissue to stable base
- Prepare superior glenoid neck (gentle burr to bleeding bone)
- Preserve biceps tendon insertion
- Create healthy tissue bed for healing
Step 3: Anchor placement
- Place 1-2 suture anchors in superior glenoid
- Position just posterior to biceps root (avoid articular surface)
- 5.5mm or 3.0mm anchors depending on bone quality
- Angle toward glenoid center to maximize pullout strength
Step 4: Suture passage and tying
- Pass sutures through labrum and biceps-labral junction
- Use penetrating devices or suture shuttles
- Simple or mattress suture configuration
- Tie with arthroscopic knots (SMC, Duncan loop)
- Confirm stable fixation with probe
The peel-back sign is pathognomonic for SLAP Type II. With the arm in abduction and external rotation (throwing position), the biceps tightens and peels the posterior-superior labrum off the glenoid. This is visible arthroscopically and confirms unstable biceps anchor.
Postoperative protocol:
- Sling immobilization 4-6 weeks
- Passive ROM only initially
- Active ROM at 6 weeks
- Strengthening at 12 weeks
- Return to throwing 6-9 months
This technique has good outcomes in carefully selected young overhead athletes.
Complications
- Incidence
- 20-30%
- Prevention/Management
- Early passive ROM, aggressive physiotherapy
- Incidence
- 10-25% in athletes over 40
- Prevention/Management
- Age-appropriate patient selection, avoid repair over 45
- Incidence
- 10-15%
- Prevention/Management
- Consider subpectoral approach, avoid hardware prominence
- Incidence
- 10-30%
- Prevention/Management
- Counsel preoperatively, use tenodesis if cosmesis important
- Incidence
- Under 1%
- Prevention/Management
- Limit bone socket size to 8mm, avoid excessive depth
- Incidence
- 2-5%
- Prevention/Management
- Adequate bone socket depth, interference screw sized appropriately
- Incidence
- 5-10%
- Prevention/Management
- More common with tenotomy, usually resolves with time
- Incidence
- 10-15%
- Prevention/Management
- Address associated pathology (cuff, labrum, impingement)
- Stiffness (most common) - prolonged immobilization, capsular reaction
- Failure to return to sport - 20-40% in overhead athletes
- Revision surgery - May need conversion to tenodesis
- Groove pain (suprapectoral) - hardware prominence, irritation
- Residual tendinitis - If diseased portion not fully excised
- Cosmetic concerns - Though less than tenotomy
- Popeye deformity - Higher in young, muscular patients
- Cramping - Transient in 5-10%
- Strength loss - Usually under 10%, not functionally significant
Failed SLAP repair in patients over 40 is common. Do not attempt revision SLAP repair - outcomes are poor. Instead, perform biceps tenodesis as a salvage procedure. Counsel patient about realistic expectations for return to overhead sport.
Postoperative Care and Rehabilitation
- Sling immobilization (remove for exercises only)
- Passive ROM only (no active ROM)
- Pendulum exercises
- Gentle scapular activation
- Elbow/wrist/hand ROM
- No lifting, pushing, pulling
- Begin active-assisted ROM
- Continue passive stretching
- Gentle isometric rotator cuff
- Progress to full passive ROM
- Light scapular strengthening
- Active ROM all planes
- Progressive resistive exercises
- Rotator cuff strengthening
- Scapular stabilization program
- Begin light functional activities
- Sport-specific training
- Plyometric exercises for overhead athletes
- Interval throwing program (pitchers)
- Progressive loading
- Full unrestricted activity
- Return to competitive throwing (if applicable)
- Maintenance strengthening program
Key restrictions:
- No active biceps contraction first 4 weeks
- No overhead lifting first 8 weeks
- No throwing until 6 months minimum
SLAP repair has the most restrictive and prolonged rehabilitation of biceps procedures.
Outcomes and Prognosis
- Young overhead athletes (under 35): 70-85% return to sport at same level
- Age 35-40: 60-70% return to sport
- Age over 40: 40-50% return to overhead sport, 20-30% revision rate
- Overall satisfaction: 70-80% in appropriate candidates
- Age (younger better)
- Sport type (throwers worse than swimmers)
- Tissue quality (degenerative labrum worse)
- Associated pathology (worse with cuff tears)
The key message for exams: SLAP repair outcomes decline significantly after age 40. This is due to degenerative labral changes and poor healing capacity. For patients over 40-45, tenodesis or tenotomy is preferred over SLAP repair in most cases.
- Overall satisfaction: 85-95%
- Pain relief: 90%
- Return to activity: 90% at 3-4 months
- Cosmetic outcome: Excellent (maintains muscle contour)
- Strength: Preserved (equivalent to normal)
- Persistent groove pain: 10-15% (suprapectoral)
- Fixation failure: 2-5%
- Reoperation rate: under 5%
- Subpectoral: Lower groove pain (5% vs 15%)
- Suprapectoral: Faster recovery, all arthroscopic
- Both: Equivalent strength and function at 1 year
- Overall satisfaction: 90-95% (in appropriate patients over 60)
- Pain relief: 95%
- Popeye deformity: 10-30% (cosmetic only)
- Strength loss: 8-10% elbow flexion, 5-10% supination (not functionally significant)
- Cramping: 10% initially, resolves in most
- Desk work: 2-4 weeks (all procedures)
- Manual labor: 3-6 months (SLAP repair), 2-3 months (tenodesis), 6-8 weeks (tenotomy)
- Overhead work: 4-6 months (SLAP), 3-4 months (tenodesis)
- SLAP repair has highest failure rate at 5-10 years (especially over 40)
- Tenodesis has excellent durability
- Tenotomy outcomes remain stable long-term
Guidelines, Registries & Global Practice
Global epidemiology. There is no dedicated arthroplasty-style registry for biceps surgery in any country; long head of biceps procedures are not separately captured by the AOANJRR (Australia), NJR (England/Wales) or AJRR (USA). Best population evidence therefore comes from national surgical databases. According to PubMed, the US National Ambulatory Surgery Sample showed SLAP repairs falling and biceps tenodeses rising year-on-year between 2016 and 2018, with SLAP repair concentrated in younger and tenodesis in older patients (Hong et al., Cureus 2022, DOI). The defining trial of practice change is Boileau et al., demonstrating superior return to sport and satisfaction with tenodesis over repair in type II SLAP lesions (Am J Sports Med 2009, DOI).
Guideline and society guidance (side-by-side). No major society publishes a single dedicated "biceps pathology" guideline; recommendations sit within broader shoulder/rotator-cuff statements and consensus work.
- Position relevant to LHB pathology
- Rotator cuff CPG addresses concomitant biceps procedures; tenotomy and tenodesis both supported when treating biceps lesions during cuff repair, no clear superiority of one over the other
- Evidence basis
- Limited/moderate strength; mirrors RCT data (Zhang 2015)
- Position relevant to LHB pathology
- No biceps-specific guidance; subacromial/shoulder pain pathways favour staged conservative care (analgesia, physiotherapy, injection) before surgical referral
- Evidence basis
- Consensus / pragmatic
- Position relevant to LHB pathology
- Shoulder pathway commentary supports conservative management first and age-appropriate surgery; tenodesis increasingly favoured over SLAP repair in the over-40s
- Evidence basis
- Expert consensus
- Position relevant to LHB pathology
- Educational consensus: SLAP repair reserved for younger athletes; tenodesis/tenotomy for degenerate or older patients; address pulley and subscapularis lesions together
- Evidence basis
- Expert consensus
Registry / database evidence. Because no registry tracks biceps surgery directly, the strongest comparative evidence is from RCTs and their meta-analyses rather than registries: tenotomy and tenodesis give equivalent function and pain relief, with tenotomy carrying a roughly three-fold higher Popeye deformity rate and tenodesis a longer operative time (Zhou et al., Medicine 2021, DOI).
Practice variation. Adoption of age-appropriate surgery is incomplete and geographically variable. Database trends confirm an evidence-driven move toward tenodesis, but SLAP repair is still performed in older patients in whom outcomes are inferior (Hong 2022). Suprapectoral versus subpectoral tenodesis location is surgeon-dependent, with equivalent 2-year validated outcomes (Werner et al., Am J Sports Med 2014, DOI).
Practice setting and resource considerations. Beyond overhead sport, manual and occupational overhead loading combined with population ageing drive both traumatic and degenerative biceps pathology internationally. Ultrasound is widely accessible and cost-effective as first-line imaging for bicipital-groove pathology, while MR arthrography for suspected SLAP lesions is typically concentrated in specialist centres. Physiotherapy is central to both conservative and postoperative care across all settings, and structured return-to-work planning with realistic timelines matters for working-age patients.
Be prepared to discuss age-based treatment algorithms for biceps pathology. Know SLAP classification, clinical tests (Speed, Yergason, O'Brien), and the decision between SLAP repair (young athlete) vs tenodesis (over 40) vs tenotomy (over 60, low demand). Understand pulley lesions and their association with subscapularis tears, and that the literature now favours tenodesis over SLAP repair in the over-40s.
MCQ Practice Points
Q: Which SLAP type represents detachment of the biceps anchor from the superior labrum? A: Type II. This is the most clinically significant SLAP type requiring surgical decision-making (repair vs tenodesis based on age). Type I is degenerative fraying, Type III is bucket-handle with stable anchor, Type IV extends into biceps.
Q: What is the most sensitive clinical test for long head of biceps tendinitis? A: Speed test (sensitivity 90%). Performed with shoulder flexion 90 degrees, elbow extended, forearm supinated, resisting forward flexion. Pain in bicipital groove is positive. Yergason tests biceps stability (supination resistance).
Q: At what age do outcomes of SLAP repair decline significantly, favoring tenodesis instead? A: Age 40-45 years. SLAP repair success rates decline dramatically over 40 due to degenerative labral changes. Tenodesis has superior outcomes in this age group and should be considered as primary treatment.
Q: What structures comprise the biceps pulley system that prevents medial subluxation? A: The pulley consists of SGHL (superior glenohumeral ligament), CHL (coracohumeral ligament), and superior subscapularis fibers. Damage to the medial sling (subscapularis and SGHL) causes medial biceps instability.
Q: A 55-year-old with biceps tendinosis and 70% partial tear needs surgical treatment. What is the most appropriate option? A: Biceps tenotomy or tenodesis. Over 50% partial thickness tears are not salvageable. At age 55, either tenotomy (simpler, faster recovery) or tenodesis (preserves strength, avoids Popeye) are appropriate. Decision based on activity level and cosmetic concerns.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old competitive baseball pitcher presents with 8 months of posterior shoulder pain, particularly during the late cocking phase of throwing. Clinical examination shows positive O'Brien test and Speed test. MRA shows a Type II SLAP lesion. He has failed 4 months of physiotherapy. How do you manage this patient?”
“A 52-year-old recreational golfer presents with anterior shoulder pain for 6 months. Examination shows positive Speed test, Yergason test, and a positive Jobe test. MRI shows biceps tendinosis with 60% partial tearing of the biceps tendon, and a full-thickness supraspinatus tear (2cm retraction). What is your treatment plan?”
“A 43-year-old patient had an arthroscopic Type II SLAP repair 18 months ago for shoulder pain. He has persistent anterior shoulder pain despite extensive physiotherapy. He cannot return to overhead work as a carpenter. Examination shows positive Speed test and bicipital groove tenderness. Repeat MRI shows intact SLAP repair but biceps tendinosis. What is your management?”
KEY ANATOMY
- Intra-articular portion 3-4cm (unique - no synovial sheath in joint)
- Origin: Superior labrum (50-60% posterior, 40-50% anterior)
- Pulley system: SGHL, CHL, superior subscapularis (prevents medial subluxation)
- Bicipital groove: lesser tuberosity (medial), greater tuberosity (lateral)
- Functions: Elbow flexion, supination, secondary humeral head depressor
SLAP CLASSIFICATION (SNYDER)
- Type I: Degenerative fraying (debridement)
- Type II: Biceps anchor detachment (MOST IMPORTANT - repair vs tenodesis)
- Type III: Bucket-handle, stable anchor (debride unstable portion)
- Type IV: Bucket-handle into biceps (repair or tenodesis)
- Types V-X: Rare variants with labral extensions
CLINICAL TESTS
- Speed test: Flexion 90deg, elbow extended, supinated - resist flexion (90% sensitive)
- Yergason: Elbow 90deg, pronated - resist supination (tests stability)
- O'Brien (Active compression): Forward flex 90deg, adduct 10deg, IR - thumb down pain (SLAP specific)
- Bicipital groove tenderness: Direct palpation with arm in 10deg IR
- Combine tests for better accuracy
AGE-BASED TREATMENT
- Under 40, athlete: SLAP repair for Type II (70-80% RTS)
- Age 40-50: Tenodesis preferred over SLAP repair (better outcomes)
- Over 50-60: Tenodesis or tenotomy based on activity/cosmesis
- Over 65, low demand: Tenotomy (simplest, fastest recovery)
- Key principle: Outcomes of SLAP repair decline significantly over 40
SURGICAL OPTIONS
- SLAP repair: Young athlete, healthy tissue, 6-9 month recovery
- Suprapectoral tenodesis: All arthroscopic, faster recovery, 10-15% groove pain
- Subpectoral tenodesis: Avoids groove, lower pain rate, preferred over 40
- Tenotomy: Simplest, no restrictions, 10-30% Popeye deformity
- Partial tear over 50%: Not salvageable, needs tenotomy or tenodesis
CRITICAL EXAM POINTS
- Type II SLAP is biceps anchor detachment - most clinically significant
- Age 40 is threshold - tenodesis over SLAP repair after this age
- MRA gold standard for SLAP (sensitivity 90%), ultrasound good for groove pathology
- 30% biceps pathology occurs with RTC tears - always assess cuff
- Pulley lesion (subscapularis tear) causes medial instability - needs tenodesis
- Failed SLAP repair: salvage with tenodesis, NOT revision SLAP repair
Evidence Base
- Original description of the SLAP lesion in 27 patients from over 700 shoulder arthroscopies. Defined the four-type classification; the injury begins posteriorly and extends anteriorly, including the biceps anchor. Compression force from a fall on an outstretched, abducted arm was the commonest mechanism, and no preoperative imaging test reliably defined the lesion.
- Cohort of 25 patients with isolated type II SLAP lesions: 10 had suture-anchor repair (mean age 37), 15 had arthroscopic interference-screw tenodesis (mean age 52). Only 20% (2 of 10) returned to previous sport after repair versus 87% (13 of 15) after tenodesis. Tenodesis satisfaction was 93% versus 60% disappointment after repair. The two groups differed in age, so findings should be confirmed by further study.
- Prospective series of 42 patients (mean age 39) undergoing open subpectoral tenodesis after a failed arthroscopic type II SLAP repair, at a military centre. Return to active duty or sport was 81%, with statistically significant improvement across ASES (68 to 89), SANE (64 to 84) and WOSI (65 to 81) scores and range of motion. One transient musculocutaneous neurapraxia was the only complication.
- Comparative cohort of 82 patients (32 arthroscopic suprapectoral, 50 open subpectoral) with minimum 2-year follow-up for isolated superior labrum or long head of biceps lesions. No significant differences in Constant-Murley, ASES, SANE, Simple Shoulder Test, or biceps-specific scores, and no significant range-of-motion or strength deficits between the two tenodesis locations.
- Pooled analysis of 9 randomised controlled trials. Tenotomy carried a substantially higher rate of Popeye deformity (risk ratio 0.33 favouring tenodesis) and tenodesis required longer operative time. There were no significant differences in ASES score, VAS pain, elbow flexion or supination strength, or cramping; the small Constant-score advantage for tenodesis was statistically significant but graded inconclusive on trial sequential analysis.
- Randomised trial of 151 patients over 55 with reparable rotator cuff tears and long head of biceps lesions (77 tenotomy, 74 tenodesis), all with arthroscopic cuff repair. No significant difference in Constant score, strength indices, Popeye sign, cramping or satisfaction at 24 months; tenotomy had shorter operative time (40 vs 50 min) and faster pain relief.
- US National Ambulatory Surgery Sample, 2016-2018: SLAP repairs fell from 29,931 to 23,451 per year while biceps tenodeses rose from 19,221 to 22,867 (both p less than 0.0001). SLAP repairs were performed on younger patients and tenodeses on older patients, but practice change lagged behind the published evidence favouring tenodesis.