Primary vs Secondary Healing | Cellular Biology | Growth Factors | Mechanical Environment
- Primary healing requires absolute stability, no callus forms, cutting cones cross fracture
- Secondary healing is natural pathway with callus formation through four phases
- Strain theory (Perren): Under 2% = bone, 2-10% = cartilage, over 10% = fibrous tissue
- Diamond concept: Cells + Scaffold + Growth factors + Mechanical environment
- MSCs differentiate to osteoblasts under BMP signaling and mechanical stimulation
- “Primary healing is Haversian remodeling across fracture (cutting cones)
- “Secondary healing uses enchondral ossification (cartilage intermediate)
- “BMP-2 and BMP-7 are osteoinductive (induce MSC differentiation to osteoblasts)
- “VEGF is critical for angiogenesis during fracture healing
- “Smoking doubles nonunion risk, NSAIDs controversial but avoid long-term use


Primary (Direct): Absolute stability (under 2% strain), compression plating, lag screws. No callus. Cutting cones (osteoclasts followed by osteoblasts) cross fracture. Haversian remodeling.
Secondary (Indirect): Relative stability (2-10% strain), IM nail, external fixator, cast. Callus formation. Four phases: inflammation, soft callus, hard callus, remodeling.
Strain = change in gap / original gap (ΔL/L). Different tissues tolerate different strain:
- Under 2%: Bone forms directly (primary healing)
- 2-10%: Cartilage forms then ossifies (secondary healing)
- Over 10%: Only fibrous tissue survives (nonunion risk)
BMPs (2, 7): Osteoinductive - induce MSC differentiation to osteoblasts. Used clinically for nonunion and spinal fusion.
VEGF: Critical for angiogenesis. New blood vessels bring cells and nutrients.
PDGF, TGF-β: Chemotactic for MSCs, promote cell proliferation.
Patient factors: Smoking (2x nonunion risk), diabetes, malnutrition, age over 60, steroids, immunosuppression.
Local factors: Open fracture, infection, bone loss, poor blood supply, inadequate fixation, excessive gap.
Medications: NSAIDs (controversial), steroids, chemotherapy.
Overview and Epidemiology
Bone healing is the complex biological process by which fractured bone regenerates and restores its original structure and function. Unlike most tissues which heal by scar formation, bone has the unique capacity for true regeneration without scar.
Why Bone Healing Biology Matters
Understanding fracture biology is essential for orthopaedic surgeons:
- Treatment selection: Choosing between absolute stability (plate) vs relative stability (IM nail) based on desired healing pathway
- Optimizing healing environment: Addressing patient factors (smoking cessation), ensuring adequate stability, considering biological augmentation
- Recognizing impaired healing: Early identification of delayed union or nonunion for timely intervention
- Using biologics appropriately: BMP use in high-risk cases (smoking, diabetes, revision surgery)
Bone is the only tissue that heals by regeneration rather than scar formation. The healed bone restores original structure and mechanical properties. This is possible because of the osteogenic cells in periosteum and bone marrow, the osteoconductive bone matrix, and the mechanical environment that guides remodeling (Wolff law).
Epidemiology of Fracture Healing
- Most fractures heal: 90-95% of closed fractures achieve union with appropriate treatment
- Nonunion rates vary: 5-10% overall, higher in specific bones (scaphoid 5-10%, femoral neck 10-30%, tibial shaft 5-15%)
- Risk factors common: Smoking (present in 30-40% of nonunions), diabetes (prevalence increasing), advanced age (population aging)
- Economic impact: Nonunion treatment costs significant healthcare resources, prolonged disability, lost productivity
Concepts and Mechanisms
Primary and Secondary Bone Healing
Primary (Direct) Bone Healing
Definition and Requirements
Primary (direct) bone healing occurs when fracture fragments are anatomically reduced and rigidly fixed with absolute stability, allowing osteoclasts and osteoblasts to cross the fracture directly without intermediate callus formation.
Absolute requirements:
- Anatomical reduction (direct bone-to-bone contact)
- Interfragmentary strain less than 2%
- Compression between fragments (lag screws, compression plates)
- Rigid fixation preventing any motion
Mechanism: Cutting Cones
The cellular mechanism of primary healing is cutting cone (osteon) remodeling:
- Osteoclast activation: Osteoclasts form at one side of the fracture and begin resorbing bone
- Cutting cone tunneling: Osteoclasts tunnel across the fracture line in a cone-shaped formation
- Osteoblast following: Osteoblasts follow behind osteoclasts, depositing new bone (lamellar bone)
- Haversian system formation: New osteons (Haversian systems) form perpendicular to the fracture, directly bridging the gap
- Remodeling completion: Multiple cutting cones cross the fracture, restoring continuity
Contact Healing (Gap under 0.01mm)
When fracture fragments are in direct contact with minimal gap (under 0.01mm or 10 micrometers):
Process:
- Lamellar bone forms directly across fracture
- Cutting cones tunnel perpendicular to fracture line
- New Haversian systems oriented longitudinally
- No intermediate woven bone stage
Timeline:
- Begins within 1-2 weeks
- Mechanical strength returns slowly over 3-6 months
- Complete remodeling takes 6-12 months
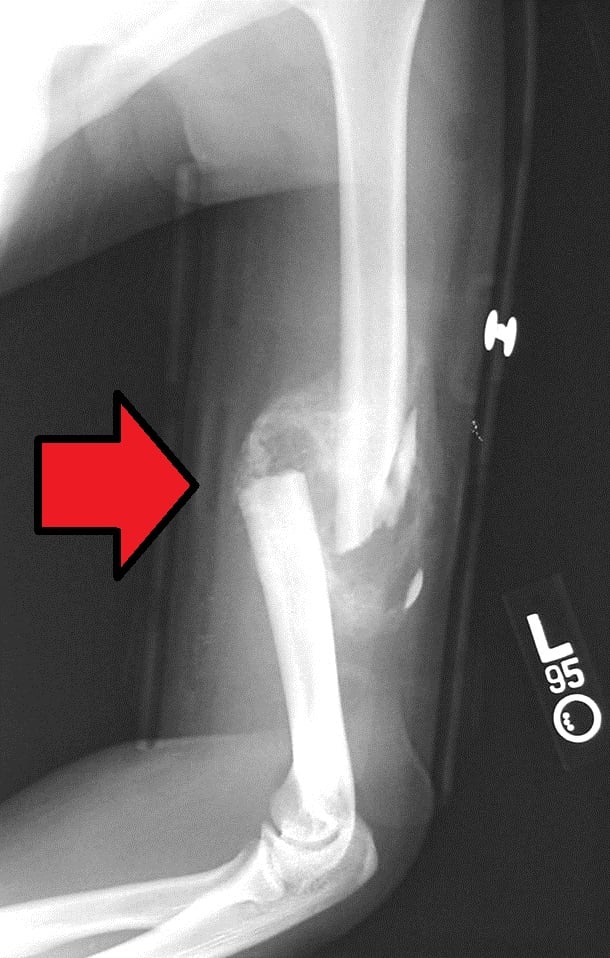
Radiographic appearance: No callus visible. Fracture line may remain visible for months even though bone is united.
This is true primary healing with direct osteonal reconstruction.
Clinical Examples and Applications
Lag screw fixation:
- Simple oblique or spiral fractures
- Compression across fracture creates absolute stability
- Common in ankle malleoli, forearm bones, scaphoid
Compression plating:
- Dynamic compression plates for forearm, clavicle
- Compression at near cortex, tension at far cortex
- Allows anatomical reduction and rigid fixation
Articular fracture fixation:
- Anatomical reduction essential for joint surface
- Lag screws through plate for compression
- Primary healing restores articular congruity
Absence of callus on radiographs indicates primary healing occurred. This is normal and expected with compression plating. The fracture line may remain visible for months even though the bone is mechanically united. Do not mistake absence of callus for absence of healing.
Advantages and Disadvantages
Advantages:
- Anatomical restoration of bone structure
- Early mechanical stability from implant
- No bulky callus to interfere with soft tissues
- Allows early joint motion (if periarticular fracture)
Disadvantages:
- Requires open reduction and internal fixation (surgical trauma)
- Extensive soft tissue dissection may impair blood supply
- Depends entirely on implant for early strength
- Stress shielding by plate may lead to bone resorption
- Slow biological healing (months for full strength)
Secondary (Indirect) Bone Healing
Definition and Characteristics
Secondary (indirect) bone healing is the natural biological response to fracture when there is relative stability allowing controlled interfragmentary motion. Callus formation bridges the fracture gap through enchondral ossification.
Key features:
- Callus forms around and between fracture fragments
- Healing occurs through four distinct phases
- Enchondral ossification (cartilage intermediate stage)
- Does not require anatomical reduction
- More biologically robust than primary healing
The Four Phases of Secondary Healing
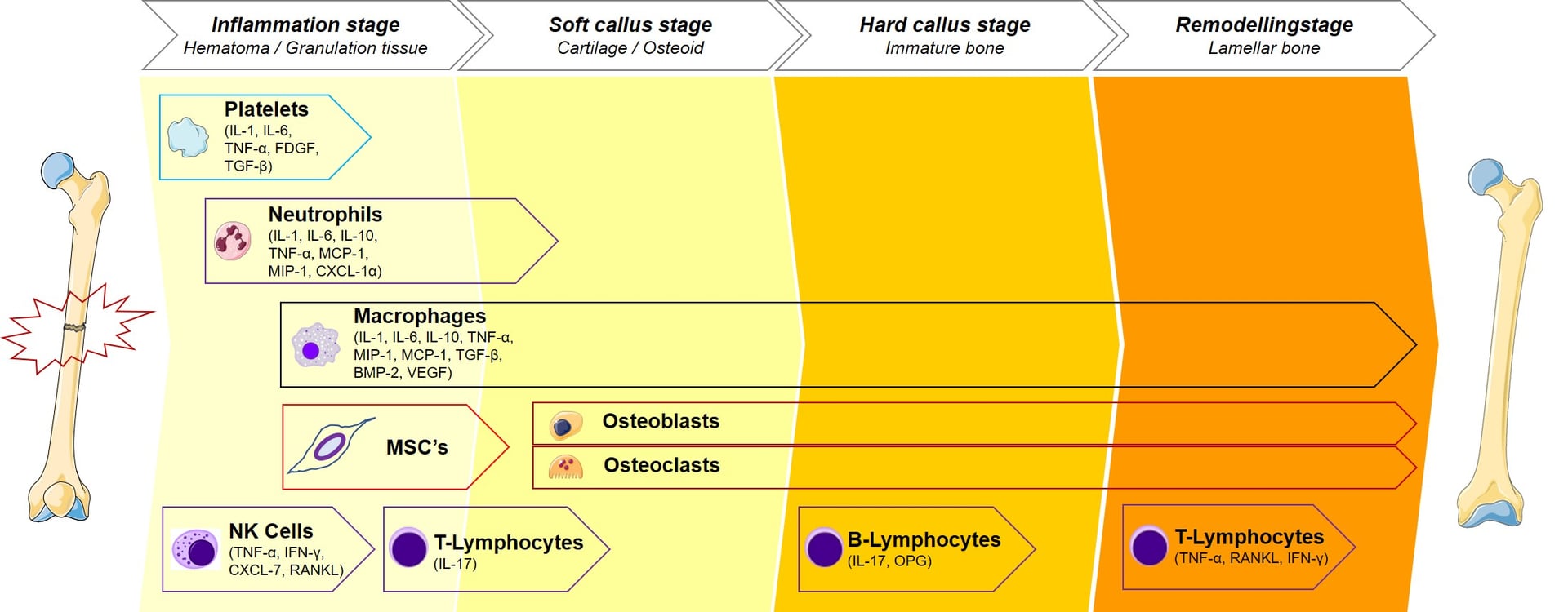
Secondary Bone Healing Timeline
Hematoma formation: Blood from torn vessels fills fracture site. Fibrin clot forms scaffold.
Inflammatory response: Neutrophils (24-48h), then macrophages arrive. Remove necrotic tissue and debris.
Cytokine release: IL-1, IL-6, TNF-α released. Recruit mesenchymal stem cells. Initiate angiogenesis.
Granulation tissue: Fibroblasts and new blood vessels form granulation tissue. Provides base for callus.
Clinical: Pain, swelling, heat at fracture site. Hematoma palpable initially.
MSC recruitment: Mesenchymal stem cells from periosteum, bone marrow, and surrounding tissues migrate to fracture.
Chondrogenesis: Low oxygen tension at fracture site promotes MSC differentiation to chondrocytes.
Fibrocartilaginous callus: Collagen type II and proteoglycans produced. Soft callus bridges fracture.
Radiolucent phase: Callus is cartilage and fibrous tissue, not yet mineralized. Appears radiolucent on X-ray.
Clinical stability: Soft callus provides limited stability. Clinical motion still present. Pain decreasing.
Enchondral ossification: Chondrocytes hypertrophy, calcify matrix, then undergo apoptosis. Blood vessels invade.
Osteoblast activity: Osteoblasts from periosteum and marrow lay down woven bone on calcified cartilage scaffold.
Mineralization: Hydroxyapatite deposition makes callus radio-opaque. Callus becomes mechanically strong.
Periosteal and endosteal callus: Callus forms externally (periosteal) and internally (endosteal), bridging fracture.
Clinical union: Fracture site becomes stable. No motion on stress. Pain minimal. Weight-bearing possible.
Woven to lamellar bone: Osteoclasts resorb woven bone. Osteoblasts deposit organized lamellar bone.
Callus resorption: Excess callus gradually resorbed. Bone returns toward original diameter.
Wolff law: Bone remodels along lines of stress. Trabeculae align with mechanical loading.
Cortical restoration: Medullary canal reconstituted. Cortical architecture restored.
Strength returns: Mechanical properties approach normal bone. Can take 6-18 months for complete strength.
Cellular Biology of Secondary Healing
Key Cells in Fracture Healing
- Origin
- Blood
- Function in Healing
- Phagocytose debris, release cytokines
- Peak Activity
- 24-48 hours
- Origin
- Blood (monocytes)
- Function in Healing
- Phagocytose debris, release growth factors
- Peak Activity
- 3-7 days
- Origin
- Periosteum, marrow, soft tissue
- Function in Healing
- Differentiate to chondrocytes and osteoblasts
- Peak Activity
- 1-3 weeks
- Origin
- MSC differentiation
- Function in Healing
- Produce cartilage matrix in soft callus
- Peak Activity
- 1-3 weeks
- Origin
- MSC differentiation
- Function in Healing
- Deposit woven bone in hard callus
- Peak Activity
- 3-8 weeks
- Origin
- Monocyte fusion
- Function in Healing
- Resorb woven bone during remodeling
- Peak Activity
- 8+ weeks
MSCs differentiate based on local environment. Low oxygen and mechanical instability favor chondrogenesis (cartilage in soft callus). Higher oxygen and stability favor osteoblastogenesis (bone in hard callus). This explains why soft callus forms first when fracture is unstable, then converts to bone as stability improves.
Understanding cell types explains the biological sequence of healing.
Clinical Examples of Secondary Healing
Intramedullary nailing:
- Femoral and tibial shaft fractures
- Relative stability allows controlled motion
- Large callus forms, providing biological bridging
- Faster clinical union than plating
External fixation:
- Open fractures, infected nonunions, distraction osteogenesis
- Allows adjustment of stability and compression
- Callus formation monitored and modulated
Cast immobilization:
- Most non-displaced or minimally displaced fractures
- Natural healing pathway
- Callus provides stability as healing progresses
The topic explains enchondral ossification in detail, but a basic-science viva expects you to know that secondary healing uses both ossification mechanisms simultaneously, and to understand the vascular response.
- Intramembranous ossification occurs subperiosteally at the fracture peripheries, away from the gap, where the environment is relatively stable and well-vascularised - osteoblasts lay down woven bone directly, with no cartilage intermediate (the peripheral "hard callus").
- Enchondral ossification occurs in the central fracture gap, which is more mobile and hypoxic - MSCs form a cartilage (soft callus) intermediate that calcifies and is then replaced by bone after vascular invasion.
- So a single healing fracture shows intramembranous bone at the edges and enchondral bone bridging the gap - the proportions shift with the local strain and oxygen tension.
- Bone has a dual blood supply: the nutrient (medullary/endosteal) artery supplies the inner two-thirds of the cortex by centrifugal (outward) flow, and the periosteal supply feeds the outer one-third by centripetal (inward) flow.
- A fracture disrupts the medullary supply, so the periosteal and extraosseous (surrounding soft-tissue) supply becomes dominant during early healing; the medullary supply is then re-established as healing progresses.
- This is the biological reason to preserve the soft-tissue envelope and avoid periosteal stripping - and why reamed nailing transiently injures the endosteal supply but the periosteal supply compensates.
Exam point: secondary healing is both intramembranous (peripheral, direct woven bone) and enchondral (central gap, cartilage-then-bone via vascular invasion); the medullary blood supply (centrifugal) is disrupted by the fracture so the periosteal/extraosseous supply (centripetal) takes over early - hence preserving periosteum and soft tissue is critical to healing.
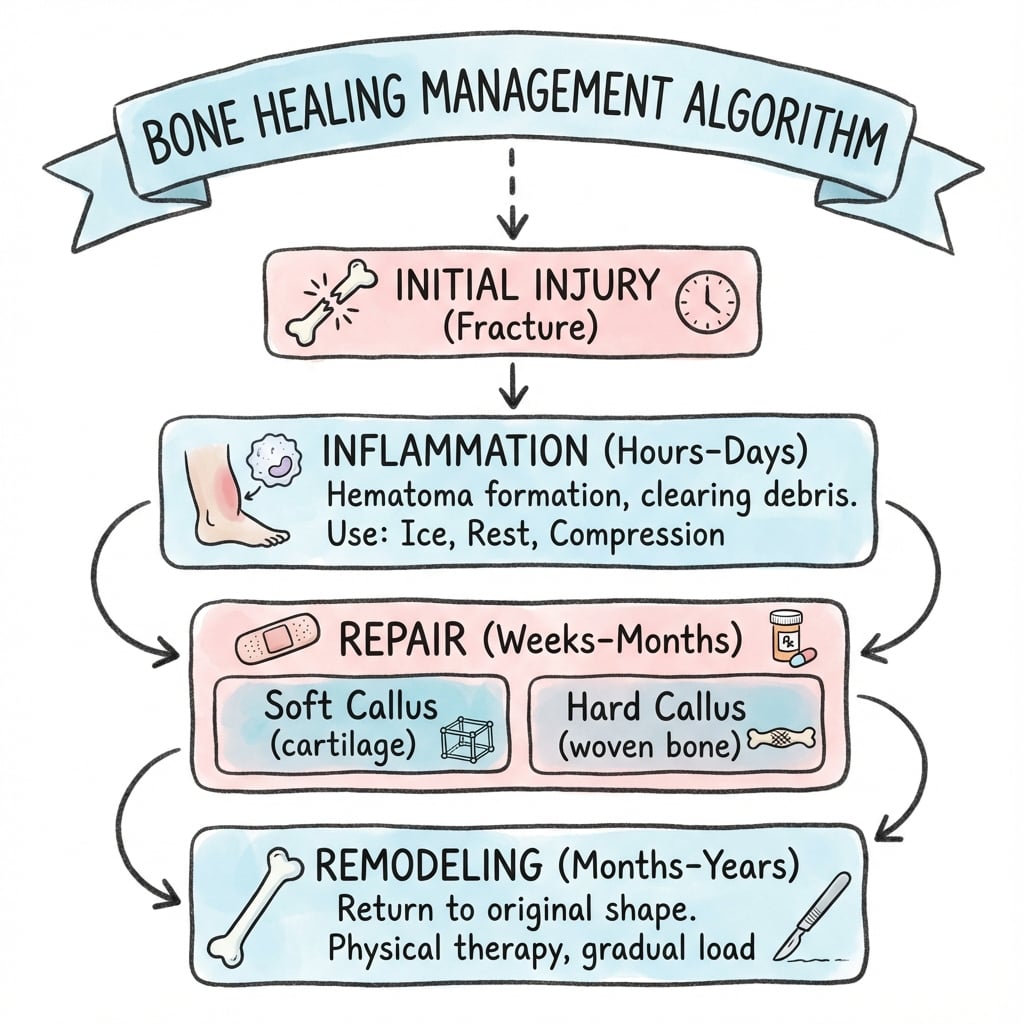
Management Algorithm
Clinical Relevance
Strain Theory and Mechanical Environment
Perren's Interfragmentary Strain Theory
Strain is defined as the change in fracture gap divided by the original gap: Strain = ΔL / L
Where:
- ΔL = change in gap width with loading
- L = original gap width
Different tissues tolerate different amounts of strain:
- Tissue That Forms
- Bone (lamellar)
- Healing Type
- Primary healing
- Clinical Example
- Compression plating with anatomical reduction
- Tissue That Forms
- Cartilage then bone
- Healing Type
- Secondary healing with callus
- Clinical Example
- Intramedullary nail, external fixator, cast
- Tissue That Forms
- Fibrous tissue
- Healing Type
- Fibrous nonunion
- Clinical Example
- Inadequate fixation, large gap, infection
Strain theory explains why different fixation methods produce different healing patterns. Compression plate (under 2% strain) produces primary healing without callus. IM nail (2-10% strain) produces secondary healing with callus. Inadequate fixation (over 10% strain) produces fibrous nonunion. Surgeon controls strain through fixation choice.
Absolute vs Relative Stability
Absolute stability (strain under 2%):
- Achieved by compression across fracture
- Requires anatomical reduction
- Methods: Lag screws, compression plates, external fixators in compression mode
- Result: Primary healing, no callus
Relative stability (strain 2-10%):
- Allows controlled interfragmentary motion
- Does not require anatomical reduction
- Methods: IM nails (locked or unlocked), bridge plating, external fixators with dynamic mode, casts
- Result: Secondary healing with callus
Optimizing Mechanical Environment
Principles for fracture fixation:
- Match stability to healing goal: Primary healing for articular fractures (need anatomical reduction), secondary healing acceptable for diaphyseal fractures
- Minimize gap: Large gaps delay or prevent healing. Bone graft if gap over 2-3mm
- Preserve biology: Minimize periosteal stripping. Indirect reduction techniques when possible
- Consider dynamization: Can reduce fixation stiffness after initial callus forms to promote remodeling
- Correct length and alignment: Malreduction impairs healing and function
Diamond Concept of Fracture Healing
The Diamond Concept (Giannoudis et al., 2007) describes four essential elements required for bone healing. Deficiency in any element increases risk of delayed union or nonunion.
1. Osteogenic Cells
Sources of osteogenic cells:
- Periosteum: Richest source of MSCs and osteoprogenitor cells
- Bone marrow: Contains hematopoietic and mesenchymal stem cells
- Endosteum: Inner lining of medullary canal
- Surrounding soft tissues: Muscle, fascia contain some MSCs
Cell requirements:
- Adequate number of viable cells
- Ability to migrate to fracture site
- Capacity to differentiate into bone-forming cells
- Survival in local environment
Clinical augmentation strategies:
- Bone marrow aspirate: Harvest from iliac crest, inject at nonunion site (contains MSCs and growth factors)
- Cancellous bone graft: Provides cells plus scaffold plus growth factors
- Demineralized bone matrix (DBM): Provides growth factors to recruit host cells
Factors depleting cells:
- Extensive periosteal stripping during surgery
- Radiation therapy (kills osteoprogenitor cells)
- Severe open fractures with soft tissue loss
- Multiple surgeries with repeat trauma
Adequate osteogenic cells are the foundation of healing.
Applying the Diamond Concept
Evaluating nonunion:
- Which element is deficient?
- Cells: Radiation, smoking, excessive stripping?
- Scaffold: Large gap, bone loss?
- Growth factors: Avascular tissue, diabetes?
- Mechanics: Inadequate fixation, persistent motion?
Treatment planning:
- Address all deficient elements
- Example for atrophic nonunion: Provide cells (bone graft), scaffold (graft or plate), growth factors (BMP or DBM), mechanics (stable fixation)
- Example for hypertrophic nonunion: Mechanics likely problem (add compression, reduce gap)
All four elements of the diamond must be present. Excellent fixation (mechanics) will not overcome absent cells or growth factors. Abundant growth factors cannot compensate for instability. This is why simple replating of infected nonunion often fails - must also address infection (kills cells) and biology (add graft).
Differential Diagnosis: Impaired Fracture Healing
A fracture that is not progressing must be characterised precisely, because each pattern has a different deficient diamond element and therefore a different treatment. Delayed union and the three nonunion subtypes are the core differential.
- Defining Feature
- Union slower than expected for site, but still progressing
- Typical Deficient Element
- Often mechanics or biology (modifiable)
- Radiographic Clue
- Some callus, fracture line persists
- Primary Treatment
- Optimise biology/stability, allow more time
- Defining Feature
- Abundant 'elephant-foot' callus, no bridging; biology intact
- Typical Deficient Element
- Mechanics (instability/motion)
- Radiographic Clue
- Exuberant callus, persistent gap
- Primary Treatment
- Improve stability/compression (e.g. nail, plate)
- Defining Feature
- Absent callus, sclerotic/resorbed ends; biology failed
- Typical Deficient Element
- Cells + scaffold + growth factors
- Radiographic Clue
- No callus, tapered/rounded bone ends
- Primary Treatment
- Biological augment (graft/BMP) plus stable fixation
- Defining Feature
- Nonunion with sepsis (sinus, raised inflammatory markers)
- Typical Deficient Element
- Cells (infection-impaired) + mechanics
- Radiographic Clue
- Lucency, sequestrum, loosening
- Primary Treatment
- Debridement, antibiotics, staged reconstruction
- Defining Feature
- Established false joint with synovial-lined cavity
- Typical Deficient Element
- Mechanics + biology (chronic)
- Radiographic Clue
- Smooth sclerotic ends, mobile gap
- Primary Treatment
- Resection of fibrous tissue, graft, stable fixation
Factors Affecting Bone Healing
Patient factors (systemic)
- Effect on Healing
- Doubles nonunion risk
- Mechanism
- Nicotine vasoconstriction impairs blood supply, CO decreases oxygen delivery
- Clinical Management
- Cessation essential - even 4 weeks helps
- Effect on Healing
- Delayed healing, increased infection
- Mechanism
- Hyperglycemia impairs cell function, neuropathy and vasculopathy
- Clinical Management
- Optimize glucose control (HbA1c under 7%)
- Effect on Healing
- Slower healing
- Mechanism
- Reduced cell number and function, comorbidities
- Clinical Management
- Optimize nutrition, consider augmentation
- Effect on Healing
- Impaired healing
- Mechanism
- Protein deficiency impairs collagen synthesis, vitamin deficiencies
- Clinical Management
- Nutritional supplementation, vitamin D, calcium
- Effect on Healing
- Inhibit healing
- Mechanism
- Suppress inflammation, reduce osteoblast function, increase osteoclast activity
- Clinical Management
- Minimize dose if possible, consider augmentation
- Effect on Healing
- Increased infection risk
- Mechanism
- Reduced immune surveillance, impaired inflammatory phase
- Clinical Management
- Prophylactic antibiotics, careful monitoring
- Effect on Healing
- Delayed healing
- Mechanism
- Reduced metabolic rate, decreased bone turnover
- Clinical Management
- Thyroid replacement therapy
Smoking increases nonunion risk approximately 2-fold (Bhandari meta-analysis, 2012). Risk is dose-dependent - heavy smokers (over 1 pack/day) have higher risk than light smokers. Even 4 weeks of cessation before surgery improves healing. Counsel all fracture patients to quit.
Local factors (fracture-specific)
- Effect
- Higher nonunion and infection risk
- Why It Matters
- Soft tissue damage, contamination, impaired blood supply
- Management
- Debridement, antibiotics, staged fixation
- Effect
- Delayed union risk
- Why It Matters
- Bone loss, difficulty achieving stability, periosteal stripping
- Management
- Bridge plating, bone graft, consider IM nail
- Effect
- Nonunion if over 2-3mm
- Why It Matters
- Cells cannot bridge large gap, inadequate scaffold
- Management
- Bone graft, Masquelet technique, bone transport
- Effect
- Impaired healing
- Why It Matters
- Inadequate oxygen and nutrients, reduced cell delivery
- Management
- Preserve soft tissue, consider vascularized graft
- Effect
- Nonunion until controlled
- Why It Matters
- Inflammatory mediators inhibit healing, biofilm prevents antibiotics
- Management
- Debridement, antibiotics, staged reconstruction
- Effect
- Varies by bone
- Why It Matters
- Scaphoid, femoral neck have poor blood supply; tibia has limited soft tissue
- Management
- Consider biology when planning treatment
Medication factors
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs):
- Controversial topic in orthopaedics
- Animal studies show impaired healing (COX-2 important for fracture healing)
- Human studies show mixed results (some show delayed union, others no effect)
- Current consensus: Avoid high-dose long-term NSAIDs (especially COX-2 selective) in high-risk fractures
- Short-term use (under 1-2 weeks) for pain likely acceptable
- Alternative analgesics: Acetaminophen, opioids (short-term), regional anesthesia
Corticosteroids:
- Inhibit osteoblast function and bone formation
- Increase osteoclast activity (bone resorption)
- Suppress inflammatory phase of healing
- Minimize dose and duration if possible
- Consider biological augmentation (BMP) in steroid-dependent patients
Other medications:
- Bisphosphonates: Reduce bone remodeling. May delay remodeling phase but do not prevent healing. Continue for osteoporosis.
- Chemotherapy: Cytotoxic agents impair cell proliferation. Delay elective surgery until after chemotherapy if possible.
- Anticoagulants: Warfarin impairs vitamin K-dependent proteins (osteocalcin). Clinical significance unclear. Continue for thromboembolic disease.
Optimization strategies
Preoperative optimization:
- Smoking cessation (minimum 4 weeks before surgery)
- Glucose control in diabetics (HbA1c under 7%)
- Nutritional supplementation (protein, vitamin D, calcium)
- Minimize steroid dose if possible
Intraoperative techniques:
- Minimize periosteal stripping (preserve blood supply)
- Adequate but not excessive stability
- Fill bone gaps with graft (under 2-3mm can heal, over needs graft)
- Consider biological augmentation in high-risk cases (BMP, bone graft)
Postoperative care:
- Avoid NSAIDs (or use short-term only)
- Early weight-bearing if fixation allows (stimulates healing)
- Monitor healing (clinical exam, radiographs)
- Early intervention if delayed union suspected
The diamond concept tells you what to optimise; a viva will also ask how to actively augment or rescue a slow-healing fracture. Three categories are high-yield and only touched on above.
- Intermittent low-dose PTH is anabolic (net osteoblast stimulation, unlike the catabolic effect of continuous PTH).
- Off-label uses to accelerate or rescue healing: delayed union/nonunion (especially osteoporotic), pelvic and sacral insufficiency fractures, stress fractures, and atypical femoral fractures (where impaired remodelling is the problem). Some RCT data (e.g. distal radius) suggest faster healing; the overall evidence is mixed, so it is an adjunct, not a guaranteed therapy.
- Cautions: avoid in the skeletally immature, Paget disease, prior skeletal radiation, or unexplained high alkaline phosphatase (osteosarcoma signal in rodents); typically limited to a ~2-year lifetime course.
- Low-intensity pulsed ultrasound (LIPUS) and pulsed electromagnetic fields (PEMF) / electrical stimulation (capacitive, inductive, or direct current) are non-invasive adjuncts proposed for delayed/nonunion.
- Evidence is mixed - the large TRUST RCT showed LIPUS did not improve tibial fracture healing - so they are selective adjuncts of uncertain benefit, never a substitute for correcting the deficient diamond element.
- Exchange (reamed) intramedullary nailing for a diaphyseal (especially hypertrophic) nonunion - reaming provides autograft and a larger, stiffer nail.
- Masquelet induced-membrane technique for segmental defects - a two-stage approach where a cement spacer induces a vascular membrane, which is later opened and packed with bone graft.
- Bone transport / distraction osteogenesis (Ilizarov) for large segmental defects.
Exam point: to augment healing, know the anabolic option (teriparatide for osteoporotic/insufficiency/stress/atypical-femoral and delayed union), the biophysical adjuncts (LIPUS/PEMF - mixed evidence, TRUST negative for LIPUS), and the nonunion operations (exchange reamed nailing, Masquelet induced-membrane, bone transport) - all applied on top of correcting the deficient diamond element.
Guidelines, Registries & Global Practice
Global Epidemiology of Fractures and Impaired Healing
Fractures are among the most common large-organ traumatic injuries worldwide, and approximately 10% fail to heal normally (Einhorn and Gerstenfeld, Nat Rev Rheumatol 2014, PMID 25266456). Global Burden of Disease modelling shows lower-limb fractures (patella, tibia/fibula, ankle) carry the highest age-standardised prevalence of all fracture sites, with falls the dominant mechanism and a projected continuing rise in fall-related fractures to 2035 (GBD 2019 analysis, PMID 39543488).
- Finding
- Approximately 10%
- Source
- Einhorn & Gerstenfeld 2014 (PMID 25266456)
- Finding
- Lower-limb (patella, tibia/fibula, ankle)
- Source
- GBD 2019 (PMID 39543488)
- Finding
- OR 2.32 (95% CI 1.76-3.06)
- Source
- Scolaro et al. 2014 (PMID 24740664)
- Finding
- OR 2.07 (95% CI 1.19-3.61)
- Source
- Wheatley et al. 2019 (PMID 30260913)
Guidance and Principles Across Jurisdictions
Bone-healing biology is governed by AO principles rather than disease-specific guidelines; the table below summarises how the major bodies frame stability and biology, with the underpinning evidence level.
- Core Guidance on Healing
- Absolute stability (lag screw/compression plate) for articular and simple fractures requiring anatomical reduction; relative stability (IM nail, bridge plating, external fixation) for comminuted/diaphyseal fractures
- Evidence Basis
- Mechanistic - Perren strain theory (PMID 376198)
- Core Guidance on Healing
- Optimise modifiable patient factors (smoking, glycaemia, nutrition); reserve osteobiologics (BMP) for high-risk/recalcitrant cases
- Evidence Basis
- RCT/meta-analysis (PMID 11314793, 24740664)
- Core Guidance on Healing
- Non-union and complex/open fractures managed in specialist (major trauma) centres; structured smoking cessation offered around surgery
- Evidence Basis
- Service standards + observational evidence
- Core Guidance on Healing
- Diamond-concept-guided management of nonunion - identify and correct the deficient element(s)
- Evidence Basis
- Expert consensus (PMID 18224731)
Registry and Surveillance Evidence
There is no dedicated international fracture-healing registry; population-level signal derives from trauma registries and Global Burden of Disease surveillance (PMID 39543488). Where biologics or implants are involved, device and adverse-event surveillance (e.g. national regulator pharmacovigilance) informs practice — for example, post-marketing signals shaped the cautious, lowest-effective-dose use of rhBMP-2/rhBMP-7 in spine and long-bone surgery.
Practice Variation
- Osteobiologic use varies markedly by funding and regulation. rhBMP use is constrained by cost in publicly funded systems; autograft remains the global default for biological augmentation.
- Smoking-cessation pathways differ but the principle (cessation around the time of surgery; structured support) is universal given the OR 2.32 nonunion signal (PMID 24740664).
- NSAID policy varies between centres given dose- and duration-dependent harm in adults but a reassuring profile in children and short courses (PMID 30260913).
- Underserved and remote populations carry compounded risk. Higher diabetes prevalence and barriers to surgery and follow-up access (including telehealth reach) worsen healing outcomes in Indigenous, remote-rural, and low-resource settings, making equitable access and culturally appropriate planning part of optimising healing globally.
Orthopaedic Examination Relevance
- Bone healing is a core basic science topic
- Primary vs secondary healing mechanisms
- Perren's strain theory (under 2%, 2-10%, over 10%)
- Diamond concept (cells, scaffold, growth factors, mechanics)
- Cutting cones and enchondral ossification
- Four phases of secondary healing (ISHR)
- Osteoinduction vs osteoconduction
- BMP and VEGF roles
- Smoking roughly doubles nonunion risk (OR 2.32)
- Fixation choice determines healing type via strain
MCQ Practice Points
Q: What is the interfragmentary strain threshold that determines whether primary or secondary bone healing occurs?
A: Under 2% strain = primary (direct) healing. 2-10% strain = secondary (indirect) healing with callus. Over 10% strain = only fibrous tissue survives (nonunion). This is Perren's strain theory: tissue survives only if local strain is less than its elongation at failure. Bone tolerates only 2%, cartilage tolerates 10%, fibrous tissue tolerates 100%.
Q: What are the four phases of secondary bone healing in correct order?
A: Inflammation → Soft callus → Hard callus → Remodeling (ISHR). Days 0-7: hematoma and inflammation. Weeks 1-3: fibrocartilaginous soft callus. Weeks 3-8: enchondral ossification to hard (woven bone) callus. Months to years: remodeling of woven to lamellar bone following Wolff's law.
Q: What is the mechanism of primary (direct) bone healing at the cellular level?
A: Cutting cones (osteoclast-led basic multicellular units) cross the fracture site directly. Osteoclasts at the leading edge resorb bone, followed by osteoblasts laying down new Haversian systems. This requires absolute stability (under 2% strain) achieved by compression plating or lag screws. No callus forms.
Q: Which growth factors are classified as osteoinductive and are used clinically to treat nonunion?
A: BMP-2 and BMP-7 (also called OP-1). They are osteoinductive because they induce mesenchymal stem cell differentiation into osteoblasts. BMP-2 is used in spinal fusion and tibial nonunion. VEGF, PDGF, and TGF-β are important for healing but are chemotactic/angiogenic rather than osteoinductive.
Q: What are the four components of the "Diamond Concept" for fracture healing?
A: (1) Osteogenic cells (MSCs, osteoblasts), (2) Osteoconductive scaffold (bone graft matrix), (3) Growth factors (BMPs, osteoinductive signals), (4) Mechanical environment (stability). All four are required for union. Nonunion management targets whichever element is deficient - atrophic needs biology, hypertrophic needs stability.
At a Glance
Bone heals via two pathways: primary (direct) healing requires absolute stability (less than 2% strain) with cutting cones crossing the fracture without callus, while secondary (indirect) healing follows four phases—Inflammation, Soft callus, Hard callus, Remodeling (ISHR)—through enchondral ossification forming visible callus. Perren's strain theory defines tissue tolerance: less than 2% = bone, 2-10% = cartilage intermediate (secondary healing), greater than 10% = fibrous tissue (nonunion risk). The Diamond Concept identifies four requirements: Cells (MSCs), Scaffold (osteoconductive matrix), Growth factors (BMPs for osteoinduction, VEGF for angiogenesis), and Mechanical environment. Key impairment factors: smoking doubles nonunion risk, diabetes, malnutrition, open fractures, infection, and poor fixation stability. Clinical union typically occurs at 6-12 weeks.
ISHRSecondary Healing Phases - ISHR
Hook:I See Hard Remodeling - the four phases of fracture healing in chronological order
CSGMDiamond Concept - CSGM
Hook:Can't See Good Mechanics = nonunion risk (all four diamond elements required)
BPTVGrowth Factors in Bone Healing - BPTV
Hook:Bone Healing Needs BPTV (like watching fracture healing on TV)
Basic Science Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An examiner presents an X-ray of a tibial shaft fracture treated with intramedullary nail showing large callus, then an X-ray of a forearm fracture treated with compression plate showing no callus. They ask you to explain the difference.”
“A 55-year-old heavy smoker presents with atrophic nonunion of the tibia 9 months after open fracture treated with external fixator. The examiner asks how you would approach treatment using the Diamond Concept.”
“Explain the role of growth factors in fracture healing, focusing on BMPs and VEGF. What is the difference between osteoinduction and osteoconduction?”
Primary Healing (Direct)
- Absolute stability required (strain under 2%)
- Compression plating, lag screws achieve this
- No callus forms - cutting cones cross fracture
- Cutting cones = osteoclasts followed by osteoblasts
- Direct Haversian remodeling across fracture
- Slower biological healing, relies on implant early
Secondary Healing (Indirect)
- Relative stability (strain 2-10%), natural pathway
- Four phases: Inflammation (0-1wk), Soft callus (1-3wk), Hard callus (3-8wk), Remodeling (months-years)
- Inflammation: hematoma, cytokines, granulation tissue
- Soft callus: MSCs → chondrocytes, cartilage forms (radiolucent)
- Hard callus: enchondral ossification, woven bone (radio-opaque)
- Remodeling: woven to lamellar bone, Wolff law
Strain Theory (Perren)
- Strain = ΔL / L (gap change / original gap)
- Under 2% strain: bone forms (primary healing)
- 2-10% strain: cartilage then bone (secondary healing)
- Over 10% strain: fibrous tissue only (nonunion)
- Explains why fixation method determines healing type
Diamond Concept (All 4 Required)
- 1. Cells: MSCs, osteoblasts from periosteum and marrow
- 2. Scaffold: Osteoconductive matrix (bone graft, hematoma)
- 3. Growth factors: BMPs (osteoinductive), VEGF (angiogenesis), PDGF, TGF-β
- 4. Mechanics: Appropriate stability for healing type
Growth Factors (Know These)
- BMP-2, BMP-7: Osteoinductive (induce MSC → osteoblast)
- VEGF: Angiogenesis (critical for enchondral ossification)
- PDGF: Chemotactic for MSCs, proliferation
- TGF-β: Regulates cell proliferation, chondrogenesis
Factors Impairing Healing
- Smoking: doubles nonunion risk (nicotine, CO, impaired angiogenesis)
- Diabetes: hyperglycemia impairs cells, neuropathy/vasculopathy
- NSAIDs: controversial, avoid long-term especially COX-2
- Steroids: inhibit osteoblasts, increase osteoclasts
- Open fracture, infection, bone loss/gap, poor blood supply
Key Concepts for Viva
- Osteoinduction = inducing MSC differentiation to osteoblasts
- Osteoconduction = scaffold for existing cells to grow on
- Enchondral ossification = cartilage intermediate, requires vessels
- Cutting cones = osteoclasts then osteoblasts (primary healing)
- Autograft = cells + scaffold + growth factors (gold standard)
Evidence Base
Strain Theory and Tissue Differentiation
- Introduced interfragmentary strain theory (ΔL/L)
- Different tissues tolerate different strain levels
- Bone tolerates under 2% strain (primary healing possible)
- Cartilage forms at 2-10% strain (secondary healing)
- Over 10% strain leads to fibrous tissue (nonunion)
- Explained why different fixation methods produce different healing patterns
Diamond Concept of Fracture Healing
- Described four essential elements for healing: cells, scaffold, growth factors, mechanical environment
- Deficiency in any element can lead to nonunion
- Framework for analyzing nonunion etiology
- Guides augmentation strategies (which element is deficient?)
Cigarette Smoking Increases Fracture Complications
- Systematic review of 19 cohort studies (7 prospective, 12 retrospective) of smoking and long-bone fracture healing
- Adjusted odds ratio for nonunion in smokers vs non-smokers was 2.32 (95% CI 1.76-3.06, p under 0.001)
- Increased nonunion in smokers with tibial fractures (OR 2.16) and open fractures (OR 1.95)
- Mean time to union longer in smokers (30.2 vs 24.1 weeks)
- Non-significant trends toward more superficial and deep wound infection in smokers
rhBMP-7 (OP-1) for Tibial Nonunion
- Prospective randomised controlled trial (124 tibial nonunions) of rhOP-1 (BMP-7) with collagen carrier vs fresh autogenous bone graft, all with intramedullary fixation
- At 9 months, clinical success 81% (BMP-7) vs 85% (autograft) (p=0.524); radiographic union 75% vs 84% (p=0.218) - no significant difference
- Avoided donor-site morbidity: over 20% of autograft patients had chronic donor-site pain
- Supported regulatory approval of BMP-7 (OP-1) for recalcitrant tibial nonunion
Fracture Healing: Mechanisms and Interventions (Landmark Review)
- Authoritative review framing fracture repair as a postnatal regenerative process recapitulating embryonic skeletal development
- Approximately 10% of fractures do not heal normally
- Integrates the tissue, cellular and molecular sequence (inflammation, endochondral and intramembranous ossification, remodelling)
- Reviews the innate/adaptive immune contribution and the roles of fixation and vascularity
- Summarises biological interventions including rhBMPs and parathyroid hormone (teriparatide) therapy
Effect of NSAIDs on Bone Healing Rates (Meta-analysis)
- Systematic review and meta-analysis of NSAID exposure and bone healing (delayed union, nonunion, pseudarthrosis)
- NSAID exposure increased delayed union or nonunion overall (OR 2.07, 95% CI 1.19-3.61)
- No significant effect in paediatric patients (OR 0.58, 95% CI 0.27-1.21)
- No significant effect with low-dose / short-duration exposure (OR 1.68, 95% CI 0.63-4.46)
- Effect appears dose- and duration-dependent