Axial Load Injury | Middle Column Involved | Load-Sharing Score
- Burst = middle column involvement (retropulsed posterior body wall)
- PLC status determines stability more than canal compromise
- Load-sharing classification (LSC) predicts need for anterior column support
- LSC 7 or more = anterior reconstruction needed (high failure rate with posterior alone)
- Neurologically intact with intact PLC can often be managed non-operatively
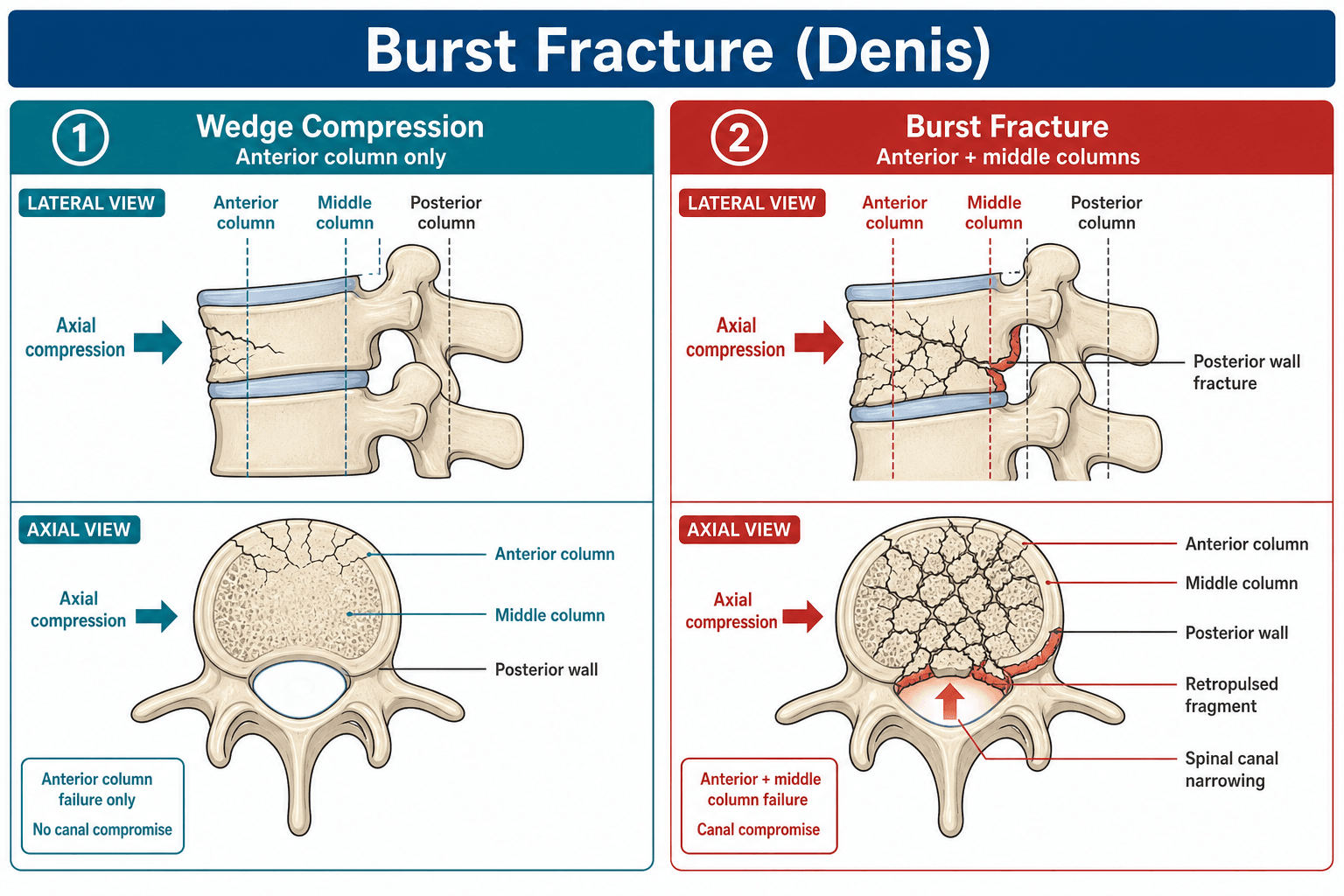
- “Burst fractures involve both anterior AND middle columns (posterior vertebral body wall)
- “Canal compromise alone does NOT mandate surgery
- “McCormack LSC: comminution + fragment apposition + kyphosis correction
- “Short segment posterior-only has a high failure rate if LSC 7 or more (36% broken screws in original McCormack series)

Posterior vertebral body wall fracture with retropulsion into canal. This is middle column involvement in Denis classification. Differentiates from simple compression fracture.
Canal compromise doesn't determine stability - PLC does. A 50% canal compromise with intact PLC can be braced. A 20% compromise with disrupted PLC needs surgery.
McCormack LSC predicts posterior-only failure: Comminution (1-3) + Apposition (1-3) + Kyphosis correction (1-3). Score 7+ = anterior column support needed.
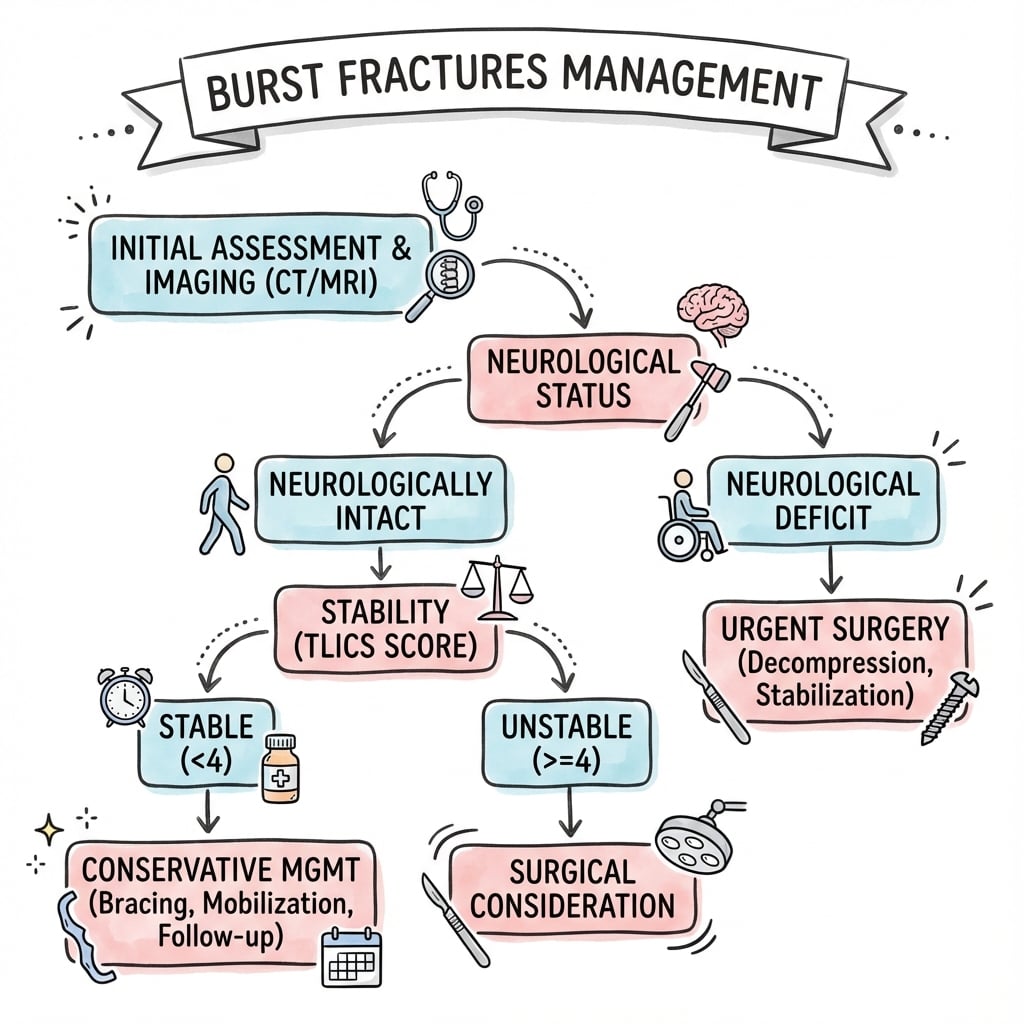
TLICS guides surgery decision. LSC guides construct choice. Stable burst (TLICS less than 4): brace. Unstable: surgery. LSC 7+: add anterior column.
- TLICS
- 2
- LSC
- N/A
- Treatment
- TLSO brace 8-12 weeks
- TLICS
- 5
- LSC
- Assess
- Treatment
- Posterior fixation +/- anterior
- TLICS
- 5+
- LSC
- 3-5
- Treatment
- Short segment posterior fixation
- TLICS
- 7+
- LSC
- 7+
- Treatment
- Anterior corpectomy + posterior fixation
CAKLoad-Sharing Score Components
Hook:CAK: Count the Comminution, Apposition, and Kyphosis - 7+ needs anterior column support!
ABUSEDenis Burst Subtypes
Hook:ABUSE: Type A-Both, B-Upper, Type C-Lower, D-Shear, E-Eccentric lateral!
7UPWhen to Add Anterior
Hook:7UP = LSC 7 or more means Unstable anterior, Posterior-only fails - need anterior column support!
Overview and Epidemiology
Burst fractures are vertebral body fractures involving both the anterior and posterior cortices with retropulsion into the spinal canal. They represent failure of both anterior and middle columns.
Epidemiology:
- Peak at thoracolumbar junction (T12-L2), especially L1
- Bimodal: young high-energy trauma, elderly osteoporotic
- MVA and falls from height most common mechanisms
- Male predominance in young age group
Compression fracture: Only anterior column (wedge shape, intact posterior wall). Burst fracture: Anterior AND middle columns (posterior wall fractured, retropulsion).
This distinction is critical because middle column involvement indicates higher instability and different treatment considerations.
Mechanism:
- Axial loading (falls from height, MVA with vertical load)
- Energy transmitted through disc into vertebral body
- Body explodes outward (hence "burst")
- Posterior wall fragment retropulses into canal
Differential diagnosis (what else produces a fractured/abnormal thoracolumbar vertebra):
- Distinguishing feature
- Anterior column only; posterior body wall intact, no retropulsion
- Key discriminator
- Intact posterior vertebral wall on CT (AO type A1/A2)
- Distinguishing feature
- Tension-band failure through bone and/or PLC; seat-belt mechanism
- Key discriminator
- Posterior element distraction, interspinous widening (AO type B)
- Distinguishing feature
- Translation/rotation, three-column failure, usually a neurological deficit
- Key discriminator
- Vertebral translation/facet dislocation (AO type C)
- Distinguishing feature
- Low energy, elderly; may still burst with canal compromise
- Key discriminator
- DEXA, low-energy mechanism, marrow oedema pattern on MRI
- Distinguishing feature
- Atypical level, pedicle/posterior-element destruction, soft-tissue mass
- Key discriminator
- Lytic lesion, pedicle erosion, abnormal marrow signal on MRI
Before calling a vertebral fracture a "burst", confirm a traumatic mechanism proportionate to the injury. A low-energy or atypical fracture demands MRI to exclude a pathological cause - posterior-element/pedicle destruction or a soft-tissue mass points to metastasis or myeloma, which changes the entire pathway (staging, biopsy, oncological MDT).
BURSTBurst Definition
Hook:BURST = Both walls fractured with Retropulsion - defines middle column involvement!
Anatomy and Biomechanics
Denis three-column concept (essential for burst understanding):
- Structures
- Anterior 2/3 vertebral body, disc, ALL
- Burst Involvement
- Always involved in burst
- Structures
- Posterior 1/3 body, posterior annulus, PLL
- Burst Involvement
- By definition involved (key feature)
- Structures
- Pedicles, facets, laminae, PLC
- Burst Involvement
- May or may not be involved
The posterior vertebral body fragment (middle column) that retropulses into the canal is the defining feature of a burst fracture. This fragment causes:
- Canal compromise
- Potential neurological injury
- Indication for decompression (if deficit present)
- Thoracolumbar junction (T12-L2) is the transition zone
- Load transfers from rigid thoracic to mobile lumbar
- Stress concentration at this level
- L1 bears significant axial load
- Burst = middle column failure
- May have intact posterior column (PLC)
- PLC status is KEY to stability
- Intact PLC = "stable burst" (can often brace)
- Disrupted PLC = "unstable burst" (surgery)
Classification Systems
McCormack Load-Sharing Classification (LSC)
Purpose: Predicts failure of posterior-only fixation by assessing anterior column load-bearing capacity.
- 1 Point
- Little (less than 30%)
- 2 Points
- Moderate (30-60%)
- 3 Points
- Severe (more than 60%)
- 1 Point
- Good (minimal displacement)
- 2 Points
- Partial (fragments still touch)
- 3 Points
- None (gross displacement)
- 1 Point
- Little (less than 3 degrees)
- 2 Points
- Moderate (4-9 degrees)
- 3 Points
- Severe (more than 9 degrees)
Score interpretation:
- 3-6: Posterior-only fixation acceptable
- 7-9: High risk of posterior-only failure → need anterior column support
LSC score of 7 or more predicts a high failure rate with short-segment posterior-only fixation. In McCormack's original series, 10 of 28 (36%) short-segment constructs developed broken screws, clustered in the most comminuted bodies. These patients need anterior column reconstruction (corpectomy + cage) OR a longer posterior construct OR a combined approach.

Clinical Assessment
History:
- Mechanism (fall height, MVA type)
- Axial loading mechanism suggests burst
- Neurological symptoms (weakness, numbness, bladder)
- Other injuries (calcaneus fractures common)
Physical examination:
- Inspection: Bruising, kyphotic deformity
- Palpation: Step-off, interspinous gap, tenderness
- Neurological: Complete lower extremity exam
- Log-roll: Examine entire spine
- Calcaneus: Fall from height mechanism
- Other spine levels: 10-15% non-contiguous
- Abdominal: Visceral injury with high-energy
- Lower extremity: Femur, pelvis
Neurological examination:
- Significance
- Good prognosis, consider non-op if stable
- Level Suggestion
- N/A
- Significance
- L1-L2 level
- Level Suggestion
- Conus/high cauda
- Significance
- L3-L4 level
- Level Suggestion
- Cauda equina
- Significance
- L4-L5 level
- Level Suggestion
- Cauda equina
- Significance
- Sacral involvement
- Level Suggestion
- Cauda equina syndrome
In burst fractures, neurological deficit is typically cauda equina (LMN) rather than cord (UMN) because most burst fractures occur below the conus (which ends L1-L2). Cauda equina syndrome (bladder/bowel dysfunction) is a surgical emergency.
Investigations
Imaging Algorithm
First-line imaging. Defines fracture morphology, canal compromise, comminution. Essential for LSC scoring. 3D reconstruction helpful.
For PLC assessment. STIR sequences show ligament injury. Also shows cord/cauda compression. Essential for TLICS scoring.
10-15% non-contiguous. CT or MRI of entire spine in high-energy trauma.
CT assessment for burst fractures:
Key measurements:
- Canal compromise percentage: (1 - fractured canal/normal canal) x 100
- Vertebral body comminution: Percentage of body involved
- Fragment apposition: Contact between fragments
- Kyphosis: Local or regional sagittal angle

Canal compromise alone does NOT mandate surgery. A patient with 60% canal compromise but intact PLC and no neurological deficit can often be managed non-operatively. The canal remodels over time with up to 50% spontaneous improvement.
MRI assessment:
- Normal
- Dark line on T2
- Abnormal
- High signal, discontinuity
- Normal
- Intermediate signal
- Abnormal
- High T2 signal, widened
- Normal
- Dark on T2
- Abnormal
- Signal change, buckling
- Normal
- Congruent joint
- Abnormal
- Widened, fluid signal
Management
Conservative Treatment
Indications:
- TLICS score 2-3 (burst, intact PLC, neurologically intact)
- Kyphosis less than 30 degrees
- No progressive neurological deficit
- Compliant patient
Protocol:
Non-Operative Protocol
Pain management, bed rest as tolerated, log-roll precautions. May begin standing with TLSO if pain controlled.
TLSO brace full-time except when supine. Serial X-rays at 2, 6, 12 weeks. Monitor for kyphosis progression.
Gradual brace weaning. Core strengthening. Return to activity based on symptoms and stability.
Monitoring:
- Serial X-rays to check for kyphosis progression
- Kyphosis increase more than 10-15 degrees = consider surgery
- Neurological deterioration = urgent surgery
The Wood et al RCT (2003) showed no significant difference in functional outcomes between operative and non-operative treatment for stable burst fractures. This supports conservative management for appropriate patients.
A neurologically injured burst fracture raises the perennial question of high-dose methylprednisolone. The NASCIS II and III trials suggested a marginal motor benefit if a 24-48 hour high-dose methylprednisolone infusion was started within 8 hours of injury - but the effect was small, derived from post-hoc subgroup analysis, and came with a real increase in complications (wound infection, pneumonia, GI bleeding, hyperglycaemia, sepsis).
On that basis most contemporary guidance (AANS/CNS, and the spinal-trauma community broadly) no longer recommends routine high-dose steroids for acute SCI; some bodies (e.g. AOSpine) regard a 24-hour infusion within 8 hours as an option to be discussed, not a standard. Exam-safe answer: steroids are not a substitute for timely decompression and stabilisation, their routine use is not recommended, any use is an individualised time-limited decision weighed against significant complication risk, and they are contraindicated in penetrating injury and the high-infection-risk polytrauma patient.
The open posterior fusion above is not the only construct. For the neurologically intact but mechanically unstable burst (e.g. AO A4/B not needing decompression), two modern options are examinable:
- Percutaneous (minimally invasive) pedicle screw fixation - the same short-segment construct placed through small stab incisions under fluoroscopy/navigation, giving less blood loss, less muscle stripping and faster mobilisation, at the cost of no formal posterolateral fusion bed.
- Fixation without fusion ("internal bracing") - posterior instrumentation stabilises the fracture while the body heals, then the implants are removed (typically around 9-12 months) to restore segmental motion and reduce adjacent-segment stress. Attractive in younger patients with good bone and a healable fracture, it avoids fusion morbidity but requires a second (removal) operation and is unsuitable when the disc is destroyed (the segment will collapse once hardware is out).
The principle: match the invasiveness and the fusion/no-fusion decision to whether decompression is needed, the bone quality, the disc integrity and the patient's age - an MIS no-fusion construct can over-treat a brace-able injury and under-treat a high-LSC one.
Surgical Technique
- Neurological injury: Less than 1% if no pre-op deficit
- Infection: 1-3%
- Hardware failure: 5-15% (higher if LSC 7+ and posterior-only)
- Need for revision: 5-10%
- Adjacent segment disease: Long-term risk
- Anterior approach: Additional risks (ileus, vascular)
- Pedicle screws: Polyaxial, appropriate lengths
- Imaging: Fluoroscopy or navigation
- Reduction tools: Lamina spreader for distraction
- If anterior: Structural cage, anterior plate
- Cell saver: For major reconstructions

Complications
- Incidence
- 5-15% (higher if LSC 7+ posterior-only)
- Prevention/Management
- Respect LSC, add anterior if 7+
- Incidence
- 10-20%
- Prevention/Management
- Index screws, cement augmentation in osteoporosis
- Incidence
- 5-10%
- Prevention/Management
- Bone graft, smoking cessation, stable fixation
- Incidence
- Up to 30% long-term
- Prevention/Management
- Short segment when appropriate
- Incidence
- Less than 1%
- Prevention/Management
- Careful technique, avoid over-distraction
- Incidence
- 10-20%
- Prevention/Management
- Gentle handling, early mobilization
- Incidence
- 1-2%
- Prevention/Management
- Vascular surgery backup, careful dissection
Ignoring the load-sharing score is a common cause of failure. Short-segment posterior-only fixation has a high broken-screw/failure rate when LSC is 7 or more (36% in the original McCormack series). Always assess LSC and plan accordingly.
Postoperative Care
Rehabilitation Timeline
DVT prophylaxis, pain management, wound care. Mobilize with physio if stable.
Continue mobilization. TLSO if additional support desired. Wound check. X-ray to confirm position.
Progressive activity. Serial X-rays. Core strengthening program. Wean brace if used.
CT at 6-12 months to confirm fusion. Return to activity based on imaging and symptoms. Long-term surveillance for adjacent disease.
Outcomes and Prognosis
- Good for stable bursts (TLICS less than 4)
- Some kyphosis progression acceptable
- Canal remodels spontaneously (up to 50%)
- Most return to normal function
- High fusion rates with adequate fixation
- LSC-appropriate constructs reduce failure
- Neurological recovery depends on initial injury
- Cauda equina has better prognosis than cord
Guidelines, Registries & Global Practice
Global epidemiology
- Burst fractures cluster at the thoracolumbar junction (T11-L2), which acts as the transition from the rigid kyphotic thoracic spine to the mobile lordotic lumbar spine; in cohorts of conservatively treated thoracolumbar fractures the junction is the commonest site and an independent risk factor for late kyphotic collapse (Guzey et al, Turk Neurosurg 2018, DOI).
- A large burst-fracture series found roughly 18% of patients were neurologically intact despite the burst, with mean canal compromise of 50% in those with a deficit versus 36% in those intact (Mohanty et al, J Orthop Surg (Hong Kong) 2008, DOI).
- Bimodal distribution: high-energy injuries (falls from height, motor-vehicle collisions) in younger men, and low-energy osteoporotic/fragility bursts in older patients - the latter behaving more like an AO type A injury at higher risk of progressive collapse.
Classification systems are the global common language - the AO Spine thoracolumbar system (type A3 incomplete / A4 complete burst) reached substantial reliability (kappa 0.72) in an international consensus study (Vaccaro et al, Spine 2013, DOI) and TLICS provides the cross-board decision threshold (operative at a score of 5 or more; Vaccaro et al, Spine 2005, DOI).
- Stance on the neurologically intact burst
- Type A3/A4 with intact PLC and no deficit: non-operative is acceptable; operative if tension-band (B) or translation (C) component
- Evidence level
- Consensus + cohort
- Stance on the neurologically intact burst
- Score 3 or less non-operative, 4 surgeon discretion, 5 or more operative; burst alone scores 2
- Evidence level
- Consensus (Level 5)
- Stance on the neurologically intact burst
- No benefit of surgery for the stable, neurologically intact burst; fewer complications without surgery
- Evidence level
- Level 1
- Stance on the neurologically intact burst
- If operating, LSC 7 or more favours anterior column support or a longer/index-screw construct
- Evidence level
- Level 4
The big international controversy is the neurologically intact burst with an indeterminate PLC. Reliance on MRI for the PLC, the weight given to canal compromise, and the threshold for early posterior-only stabilisation vary between units and resource settings. High-resource centres increasingly favour MRI-guided non-operative care (supported by the Wood RCT); limited-resource settings may stabilise earlier to allow upright mobilisation and reduce nursing burden. There is no implant registry for spinal trauma comparable to the arthroplasty joint registries (NJR, AOANJRR, AJRR), so trauma evidence rests on RCTs and cohorts rather than registry survival data.
- Complete neurological examination (and a digital rectal/perianal exam where cauda equina is possible)
- TLICS and AO Spine type with rationale
- LSC assessment when operating
- MRI for PLC integrity (especially the indeterminate PLC)
- Informed consent covering hardware failure and the option of non-operative care
failing to calculate LSC (hardware failure), inadequate consent on failure rates, not documenting PLC assessment, and missing non-contiguous fractures (10-15% of cases).
MCQ Practice Points
Q: What defines a burst fracture and differentiates it from a compression fracture? A: Involvement of the posterior vertebral body wall (middle column) with retropulsion into the canal. Compression fractures only involve the anterior column.
Q: What are the three components of the McCormack Load-Sharing Classification? A: Comminution (1-3), fragment Apposition (1-3), and Kyphosis correction needed (1-3). Score 7+ predicts posterior-only failure.
Q: At what LSC score should anterior column reconstruction be considered? A: LSC 7 or more - short segment posterior-only constructs have a high failure rate at this threshold (36% broken screws in McCormack's original series).
Q: A patient has 50% canal compromise but is neurologically intact with intact PLC. Does this require surgery? A: No - canal compromise alone does not mandate surgery. It remodels spontaneously. TLICS would be 2 (non-operative).
Q: What is the most common type of burst fracture in the Denis classification? A: Type B (superior endplate) - accounts for 70% of burst fractures.
Q: When is ligamentotaxis most effective for reducing retropulsed fragments? A: When PLL is intact and surgery is performed within 72 hours. Beyond this, fragments become adherent.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old falls from 3 meters and lands on his feet. CT shows an L1 burst fracture with 40% canal compromise. He is neurologically intact. MRI shows intact PLC. How do you manage this?”
“A 45-year-old woman falls from a roof and has an L1 burst fracture with severe comminution (more than 60%), poor fragment apposition, and 15 degrees of kyphosis. She has incomplete cauda equina syndrome. What is your surgical plan?”
“A 50-year-old male with diabetes had short segment posterior fixation (T12-L2) for an L1 burst fracture 8 weeks ago. He now presents with increasing back pain and X-rays show screw pullout with kyphosis of 30 degrees. How do you manage this failure?”
What Makes It a Burst?
- Posterior vertebral body wall fractured (middle column)
- Retropulsion of fragment into canal
- Anterior AND middle column failure
- Different from compression (anterior only)
Load-Sharing Classification
- Comminution: Little=1, Moderate=2, Severe=3
- Apposition: Good=1, Partial=2, None=3
- Kyphosis correction: Little=1, Moderate=2, Severe=3
- Score 7+ = anterior column support needed
Treatment Algorithm
- TLICS less than 4 + intact PLC: TLSO brace
- TLICS 5+: Posterior pedicle screw fixation
- LSC less than 7: Short segment (with index screws)
- LSC 7+: Anterior corpectomy + posterior
Surgical Pearls
- Index level screws reduce failure
- Ligamentotaxis works if PLL intact and less than 72h
- Canal compromise alone doesn't mandate surgery
- Cement augmentation in osteoporosis
Complications
- Hardware failure: 5-15% (much higher if LSC 7+ posterior-only; 36% in McCormack series)
- Non-union: 5-10%
- Adjacent segment disease: up to 30%
- Risk factors: diabetes, smoking, osteoporosis
Evidence Base
McCormack Load-Sharing Classification (landmark)
- Consecutive series of 28 three-column fractures fixed with short-segment Steffee screws and plates; 10 of 28 (36%) developed broken screws
- 9-point scale grading damaged vertebral body, fragment spread, and corrected traumatic kyphosis (each 1-3)
- Screw breakage clustered in patients with the greatest vertebral body comminution
- Tool to predict posterior short-segment failure and select fractures for anterior strut reconstruction
Canal Compromise vs Neurological Deficit
- 105 thoracolumbar/lumbar burst fractures; 18% were neurologically intact despite a burst
- Mean canal compromise 50% in patients with a deficit vs 36% in those intact
- Type of Denis burst did not correlate with severity of deficit (p=0.835)
- No significant overall relationship between canal compromise and deficit at L1 (p=0.42)
TLICS - Thoracolumbar Injury Classification and Severity Score (landmark)
- Consensus system scoring three characteristics: injury morphology, integrity of the posterior ligamentous complex, and neurological status
- Burst morphology scores 2; PLC scores 0 (intact), 2 (indeterminate) or 3 (injured); neurology 0-3
- A composite score stratifies to non-operative (3 or less), surgeon discretion (4), or operative (5 or more)
- Also guides the optimum operative approach for surgical patterns
AO Spine Thoracolumbar Injury Classification (landmark)
- International consensus morphological system: type A (compression), type B (tension-band disruption), type C (translation/displacement)
- Burst fractures are type A3 (incomplete, single endplate) and A4 (complete, both endplates)
- Substantial reliability for identifying the main injury type (kappa = 0.72)
- Adds neurological grade (N) and patient-specific modifiers (e.g. M1 indeterminate PLC)