Osteoporotic Most Common | Anterior Column Failure | Usually Non-Operative
- Osteoporotic VCFs are anterior column failures - PLC is intact, therefore stable
- Non-operative management is first-line for most compression fractures
- Kyphoplasty vs Vertebroplasty: Kyphoplasty uses balloon to restore height before cement
- Red flags: Neurological deficit, PLC injury, retropulsed bone = NOT simple compression
- INVEST trial: No benefit of vertebroplasty over sham procedure
- “Compression fractures are STABLE (anterior column only, PLC intact)
- “Kyphotic deformity greater than 30 degrees may warrant surgery
- “Pathologic fracture workup: myeloma, metastasis, lymphoma
- “Cement augmentation controversial - INVEST and VERTOS trials showed mixed results
Compression fractures are STABLE because PLC is intact. If PLC is disrupted it becomes an unstable flexion-distraction pattern, not a simple compression. Always confirm posterior column integrity.
Always exclude malignancy in compression fractures. Red flags: age under 55, weight loss, night pain, multiple levels, pedicle involvement, soft tissue mass. Order myeloma screen (serum protein electrophoresis).
Vertebroplasty vs Kyphoplasty: Both inject polymethylmethacrylate (PMMA). Kyphoplasty uses balloon to restore height first. Evidence for pain relief is controversial (INVEST trial showed no benefit vs sham).
Progressive kyphosis leads to sagittal imbalance, pain, and functional decline. Kyphotic deformity greater than 30 degrees may warrant surgical correction. Multiple adjacent VCFs create severe deformity.
- Classification
- Genant Grade 1
- Treatment
- Analgesia, early mobilization
- Key Pearl
- Avoid bed rest - increases bone loss
- Classification
- Genant Grade 2
- Treatment
- TLSO brace 6-12 weeks
- Key Pearl
- Physical therapy essential for outcomes
- Classification
- Genant Grade 3, 6 weeks conservative failed
- Treatment
- Discuss cement augmentation
- Key Pearl
- Controversial - trial of conservative care first
- Classification
- Burst or PLC injury
- Treatment
- Surgical stabilization
- Key Pearl
- This is NOT a simple compression fracture
BONESCompression Fracture Red Flags
Hook:BONES red flags suggest this may NOT be a simple osteoporotic compression fracture!
STABLEConservative Management Criteria
Hook:If STABLE, the fracture can be managed with bracing and conservative care!
CEMENTCement Augmentation Indications
Hook:Only consider CEMENT augmentation after conservative care fails - evidence is controversial!
Overview and Epidemiology
Definition
Vertebral compression fractures (VCFs) represent failure of the anterior column under compressive load, resulting in loss of vertebral body height. Unlike burst fractures, the middle and posterior columns remain intact, making these inherently stable injuries.
Etiology
Osteoporotic VCFs (75%)
- Post-menopausal women, elderly men
- Minimal trauma mechanism (bending, coughing, lifting)
- T-score less than -2.5 on DEXA scan
- Most common at thoracolumbar junction (T12-L1)
Pathologic VCFs (10-15%)
- Metastatic disease (breast, prostate, lung, renal, thyroid)
- Multiple myeloma
- Primary bone tumors
- Metabolic bone disease
Traumatic VCFs (10-15%)
- High-energy mechanism in young patients
- Fall from height, motor vehicle accident
- Often associated with other injuries
Always exclude malignancy before diagnosing osteoporotic VCF:
- Full blood count, ESR, CRP
- Serum protein electrophoresis (myeloma)
- Calcium, alkaline phosphatase
- Consider CT chest/abdomen/pelvis if red flags present
- Pedicle involvement strongly suggests malignancy (not osteoporosis)
VCFs are the most common osteoporotic fracture worldwide: roughly 1.4 million clinically diagnosed VCFs occur annually, and the lifetime risk in a 50-year-old woman approaches 16%. Crucially, around two-thirds of VCFs are never clinically recognised, being found incidentally on imaging - so prevalence vastly exceeds diagnosed incidence.
Anatomy and Biomechanics
Three-Column Model (Denis)
- Anterior longitudinal ligament (ALL)
- Anterior 2/3 of vertebral body
- Anterior annulus fibrosus
- FAILS in compression fractures
- Posterior 1/3 of vertebral body
- Posterior annulus fibrosus
- Posterior longitudinal ligament (PLL)
- INTACT in compression fractures (distinguishes from burst)
- Posterior bony arch
- Facet joints and capsules
- Posterior ligamentous complex (PLC)
- INTACT in compression fractures (key to stability)
- Compression Fracture
- Anterior only
- Burst Fracture
- Anterior + Middle
- Compression Fracture
- Intact
- Burst Fracture
- Failed (retropulsion possible)
- Compression Fracture
- Intact
- Burst Fracture
- May be intact or disrupted
- Compression Fracture
- Stable
- Burst Fracture
- Potentially unstable
- Compression Fracture
- Low
- Burst Fracture
- Higher (canal compromise)
- Compression Fracture
- 1-2 (compression)
- Burst Fracture
- 2-4 (burst morphology)
Vertebral body is 90% trabecular bone - preferentially affected by osteoporosis. Under axial compression, the anterior cortex fails first, creating the characteristic wedge deformity. The posterior cortex and middle column remain intact because the neutral axis of the spine is posterior.
Classification
Genant Semi-Quantitative Grading
Standard classification for osteoporotic VCFs based on height loss:
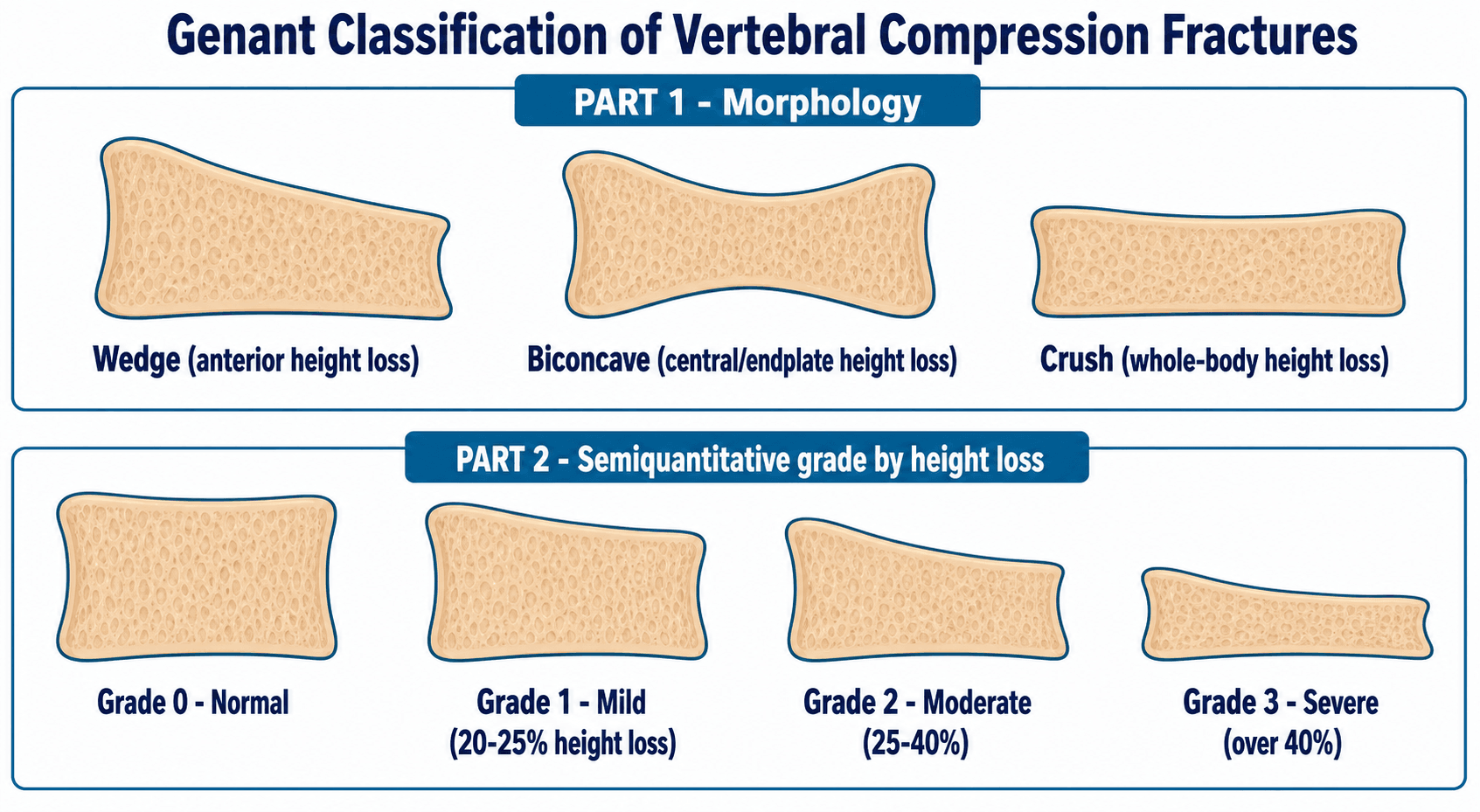
Grade 0 - Normal
- No discernible height reduction
- Intact vertebral body
Grade 1 - Mild (Wedge/Biconcave/Crush)
- 20-25% reduction in anterior, middle, or posterior height
- Mild deformity visible on lateral radiograph
Grade 2 - Moderate
- 25-40% height reduction
- Clear wedging or biconcavity
- May cause localized kyphosis
Grade 3 - Severe
- Over 40% height reduction
- Significant vertebral collapse
- Often symptomatic with localized pain
Serial imaging essential: Compare to prior imaging to determine acuity. Acute fractures show marrow edema on MRI (T2 hyperintensity, T1 hypointensity). Chronic fractures may be stable and asymptomatic despite severe height loss.
Clinical Assessment
- Mechanism: Minimal trauma? (osteoporotic) vs high-energy (traumatic)
- Pain characteristics: Localized, worse with movement
- Red flags: Night pain, weight loss, prior malignancy
- Functional status: Mobility, activities of daily living
- Osteoporosis risk factors: Age, female, smoking, steroids
- Inspection: Loss of lordosis, kyphotic posture
- Palpation: Midline tenderness at fracture level
- Percussion: Pain over spinous process
- Neurological exam: Usually normal (if not, reassess diagnosis)
- Gait: Altered stance phase due to pain
Key Clinical Findings
- Acute, localized mid-back pain
- Exacerbated by trunk flexion and rotation
- Relieved by recumbency
- May radiate to flanks (referred pain)
- Neurological deficit (suggests burst, not compression)
- Multiple levels (myeloma, metastases)
- Age under 55 without trauma
- Known history of malignancy
- Constitutional symptoms
If neurological deficit is present, this is NOT a simple compression fracture. Consider burst fracture with retropulsed bone, pathologic fracture with epidural extension, or cauda equina syndrome. Urgent MRI and surgical consultation required.
Differential Diagnosis
- Discriminating Features
- Low-energy, anterior wedge, pedicles spared, marrow edema if acute
- Key Investigation
- MRI (edema), DEXA
- Discriminating Features
- Pedicle destruction, soft-tissue mass, convex posterior wall, multiple levels
- Key Investigation
- MRI with contrast, SPEP, staging CT
- Discriminating Features
- Posterior wall involved, retropulsion, canal compromise, often higher energy
- Key Investigation
- CT (posterior wall)
- Discriminating Features
- PLC disruption, interspinous widening, seatbelt mechanism
- Key Investigation
- MRI (PLC), CT
- Discriminating Features
- Disc herniation into endplate, no acute height loss, asymptomatic
- Key Investigation
- MRI
- Discriminating Features
- Disc-centred destruction, endplate erosion, raised CRP/ESR, fever
- Key Investigation
- MRI with contrast, blood cultures
Investigations
- What to Look For
- Height loss, wedging
- Key Finding
- Greater than 20% height loss = fracture
- What to Look For
- Posterior wall
- Key Finding
- Intact posterior wall = compression (not burst)
- What to Look For
- Marrow signal
- Key Finding
- Low signal = acute or malignancy
- What to Look For
- Edema
- Key Finding
- High signal = acute fracture (within 6-8 weeks)
- What to Look For
- Enhancement pattern
- Key Finding
- Focal enhancement in pedicle = metastasis

Marrow edema on STIR/T2 indicates fracture is acute (within 6-8 weeks). This is important for cement augmentation - only effective for recent, symptomatic fractures. Chronic healed fractures without edema will not benefit from vertebroplasty.
Management Algorithm

Management
Non-Operative Treatment (First-Line for Most VCFs)
- Adequate analgesia (paracetamol, NSAIDs, short-term opioids)
- Avoid prolonged bed rest (accelerates bone loss)
- Gentle mobilization as tolerated
- Physical therapy assessment
- TLSO or Jewett brace for comfort (if needed)
- Progressive mobilization program
- Physical therapy for core strengthening
- Falls prevention assessment
- Gradual return to normal activities
- Ongoing physical therapy
- Weight-bearing exercise program
- Osteoporosis treatment initiation (bisphosphonates/denosumab)
Bed rest accelerates bone loss at 1-2% per week. The goal is early mobilization to maintain bone density and prevent deconditioning. Bracing is for comfort, not essential for healing of stable fractures.
Surgical Technique
Vertebroplasty/Kyphoplasty Technique
- Prone on radiolucent table
- Bolsters under chest and pelvis (for lordosis)
- Arms forward, face in padded rest
- Biplanar fluoroscopy required
- Transpedicular or parapedicular
- 11-gauge or 13-gauge trocar
- Local anesthesia with sedation or GA
- AP view: Align pedicle at lateral edge of vertebral body
- Lateral view: Ensure trocar tip in anterior 1/3 of body
- For kyphoplasty: Inflate balloon, restore height
- Mix PMMA, allow partial polymerization (toothpaste consistency)
- Inject under live fluoroscopy (monitor for extravasation)
- Inject 2-4ml per side (typically bilateral approach)
PMMA extravasation (10-30%), adjacent level fracture (15-20% at 1 year), pulmonary embolism (rare but serious), and infection (less than 1%).

Complications
- Incidence
- 15-25% at 1 year
- Prevention/Management
- Optimize osteoporosis treatment, monitor kyphosis
- Incidence
- 10-30%
- Prevention/Management
- Inject under live fluoro, appropriate cement viscosity
- Incidence
- 5-10%
- Prevention/Management
- Serial imaging, consider fusion if progressing
- Incidence
- 20-30%
- Prevention/Management
- Multimodal pain management, physical therapy
- Incidence
- Rare (less than 1%)
- Prevention/Management
- Monitor viscosity, small volume injection
15-25% of patients will sustain another vertebral fracture within 1 year. Controversial whether cement augmentation increases this risk (altered load transfer) or if it represents the natural history of osteoporosis. Treat the underlying osteoporosis aggressively.
Postoperative Care
After Cement Augmentation
Treating the fracture without treating osteoporosis is incomplete care. Initiate bisphosphonates or denosumab, ensure calcium/vitamin D supplementation, and coordinate with endocrinology or geriatrician. 25% will have another VCF within 1 year if osteoporosis untreated.
Outcomes and Prognosis
Natural History
- 90% of compression fractures heal with conservative management
- Pain typically improves significantly by 6-12 weeks
- Residual deformity common but often asymptomatic
- 25% will sustain another VCF within 1 year (osteoporotic cascade)
- 4x increased mortality risk compared to age-matched controls
Prognostic Factors
- Single level involvement
- Genant Grade 1-2
- Minimal pre-fracture functional impairment
- Good compliance with osteoporosis treatment
- Access to physical therapy
- Multiple levels
- Severe kyphosis (over 30 degrees)
- Inadequate osteoporosis treatment
- Poor baseline function
- Associated medical comorbidities
VCFs significantly impact quality of life - chronic pain, reduced mobility, loss of independence, depression. Comprehensive management includes not just fracture treatment but pain management, physical therapy, falls prevention, and psychological support.
Guidelines, Registries & Global Practice
- VCFs are the most common osteoporotic fracture worldwide
- Lifetime risk approaches 16% in women, 5% in men over 50
- Around two-thirds are never clinically diagnosed (incidental on imaging)
- A prevalent VCF roughly doubles the risk of further vertebral and hip fracture
- Fracture Liaison Services (FLS) improve assessment and treatment rates internationally (IOF "Capture the Fracture" programme)
- First-line: oral/IV bisphosphonate or denosumab, plus calcium and vitamin D
- Anabolic agents (teriparatide, romosozumab) reserved for very high risk
- DEXA and 10-year risk tools (FRAX) guide therapy globally
- Position on Vertebroplasty/Kyphoplasty
- Recommends AGAINST routine vertebroplasty; kyphoplasty an option (limited evidence)
- Emphasis
- Strong skepticism after sham trials
- Position on Vertebroplasty/Kyphoplasty
- Option for severe ongoing pain despite optimal analgesia after recent VCF
- Emphasis
- Selective use, pain-driven
- Position on Vertebroplasty/Kyphoplasty
- Reasonable option in carefully selected acute, painful fractures
- Emphasis
- Patient selection central
- Position on Vertebroplasty/Kyphoplasty
- Focus on anti-osteoporosis therapy; augmentation secondary
- Emphasis
- Treat the bone, not just the fracture
- Ready access to MRI for acuity, DEXA, and FLS pathways
- Cement augmentation and anabolic agents available where selected
- Multidisciplinary metabolic bone and spine services
- Diagnosis often on plain radiographs alone; MRI/DEXA may be scarce
- Generic oral bisphosphonates and calcium/vitamin D are the affordable, high-value backbone
- Early mobilisation, simple analgesia, and falls prevention remain universally applicable and low-cost
Key documentation requirements (transferable across health systems):
- Document the neurological examination thoroughly at presentation and follow-up
- Record discussion and initiation of osteoporosis treatment
- For cement augmentation, document counseling about the controversial evidence and the risks below
- Document referral to a Fracture Liaison Service or primary care for ongoing bone health
Specific risks to discuss: PMMA extravasation, adjacent level fracture (15-25% at 1 year), no guarantee of pain relief (INVEST and Buchbinder sham trials), pulmonary cement embolism (rare), infection. Explain that the evidence is controversial and conservative management works for most patients.
Controversies and Areas of Uncertainty
The two 2009 blinded sham trials (INVEST, Buchbinder) found no benefit over placebo, yet VAPOUR (2016), the only blinded trial restricted to acute fractures under 6 weeks with severe pain and adequate cement fill, was positive. The unresolved question is whether earlier intervention and better technique, rather than a true class effect, explain the difference.
Adjacent-level fractures occur in 15-25% within a year. Whether the stiffer cemented segment alters load transfer to neighbours, or whether this simply reflects the natural osteoporotic cascade, remains debated. Either way, aggressive bone-health treatment is the agreed response.
Kyphoplasty restores some height and lowers cement-leak rates, but no robust trial shows superior pain outcomes over vertebroplasty, and it costs more. Choice is often institutional rather than evidence-driven.
TLSO/Jewett braces are widely used for comfort, but evidence that bracing improves healing or alignment in stable VCFs is weak, and prolonged rigid bracing may worsen deconditioning. The trend is toward early mobilisation with brief, symptom-led brace use.
MCQ Practice Points
Q: Why are vertebral compression fractures classified as stable injuries? A: The posterior ligamentous complex (PLC) is intact. Compression fractures involve anterior column failure only. If PLC is disrupted, it becomes a flexion-distraction injury requiring different treatment.
Q: What did the INVEST trial (NEJM 2009) demonstrate regarding vertebroplasty? A: No significant difference in pain or disability between vertebroplasty and sham procedure at any time point. This is frequently tested - vertebroplasty evidence is controversial.
Q: What is the risk of subsequent vertebral fracture after an osteoporotic VCF? A: 25% within 1 year (osteoporotic cascade). This emphasizes that treating the underlying osteoporosis is as important as treating the fracture itself.
Q: What MRI finding indicates an acute vs chronic compression fracture? A: Marrow edema on STIR/T2 indicates acute fracture (within 6-8 weeks). Fat signal suggests chronic healed fracture. Only acute fractures with edema may benefit from cement augmentation.
Q: What imaging finding suggests metastatic rather than osteoporotic VCF? A: Pedicle involvement. Osteoporosis affects trabecular bone of the vertebral body; cortical pedicles are relatively spared. Pedicle loss = malignancy until proven otherwise.
Q: What percentage height loss defines a Grade 2 VCF on the Genant classification? A: 26-40% height loss. Grade 1 is 20-25%, Grade 2 is 26-40%, Grade 3 is greater than 40%. Grade 2-3 fractures may warrant closer monitoring.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman presents with acute mid-back pain after bending to pick up groceries. Lateral X-ray shows 30% height loss at T12. She is neurologically intact. How would you manage this patient?”
“A 58-year-old man with known prostate cancer presents with new thoracolumbar pain and imaging showing multiple vertebral compression fractures at T10, T11, and L2. Discuss your approach.”
“Discuss the evidence for and against vertebroplasty in osteoporotic compression fractures.”
Key Anatomy
- Anterior column ONLY involved - stable fracture
- PLC intact (distinguishes from burst/distraction)
- Vertebral body is 90% trabecular bone - osteoporosis target
- T12-L1 most common level (thoracolumbar junction)
Genant Classification
- Grade 1 (Mild): 20-25% height loss
- Grade 2 (Moderate): 25-40% height loss
- Grade 3 (Severe): Over 40% height loss
- MRI determines acuity (edema = acute)
Treatment Algorithm
- Most (90%) heal with conservative care
- Avoid bed rest - early mobilization essential
- Cement augmentation if 6 weeks conservative fails
- Surgery rare - reassess diagnosis if considering
Key Evidence
- INVEST trial: Vertebroplasty = sham procedure
- VERTOS II: Short-term benefit only
- VAPOUR: Acute fractures may benefit
- Adjacent level fracture 15-25% at 1 year
Red Flags for Malignancy
- Pedicle involvement (not just body)
- Multiple levels without trauma
- Age under 55 without mechanism
- Night pain, weight loss, known cancer
Global Practice & Guidelines
- AAOS advises against routine vertebroplasty; NICE allows it for severe refractory pain
- Bisphosphonates/denosumab for secondary prevention (FREEDOM, VERT)
- Fracture Liaison Services improve treatment rates worldwide
- 25% will have another VCF within 1 year if osteoporosis untreated
Evidence and Guidelines
- Multicenter, blinded RCT: 131 patients with 1-3 painful osteoporotic VCFs
- Vertebroplasty vs simulated (sham) procedure without cement
- No significant difference in Roland-Morris disability or pain at 1 month
- Higher crossover to vertebroplasty in the control group by 3 months (51% vs 13%)
- Open-label RCT: 202 patients with acute VCF (under 6 weeks, marrow edema on MRI, persistent pain)
- Vertebroplasty vs conservative care
- Significant pain relief favoring vertebroplasty (VAS difference 2.6 at 1 month)
- Benefit attenuated but still significant at 12 months (VAS difference 2.0)
- Multicenter RCT across 8 countries: 300 patients with acute VCF
- Balloon kyphoplasty vs non-surgical care (open-label)
- SF-36 physical component improved 5.2 points more with kyphoplasty at 1 month (p<0.0001)
- Quality-of-life benefit maintained at 12 months
- Multicentre, double-blind, placebo-controlled RCT: 120 patients with acute VCF (under 6 weeks) and severe pain (NRS 7 or more)
- Vertebroplasty (adequate-fill technique) vs simulated placebo procedure
- Primary outcome met: 44% reached NRS pain under 4 at 14 days vs 21% with placebo (difference 23 percentage points, p=0.011)
- Suggests timing and adequate cement fill are critical - acute fractures benefit
- Multicentre, double-blind, placebo-controlled RCT: 78 patients with painful unhealed VCF (under 12 months, MRI-confirmed)
- Vertebroplasty vs sham procedure (needle without cement)
- No significant advantage in any outcome at 1 week or 1, 3, 6 months
- At 3 months mean pain fell 2.6 (vertebroplasty) vs 1.9 (sham), no significant difference