Seatbelt Injury | Flexion-Distraction | High Association with Abdominal Injury
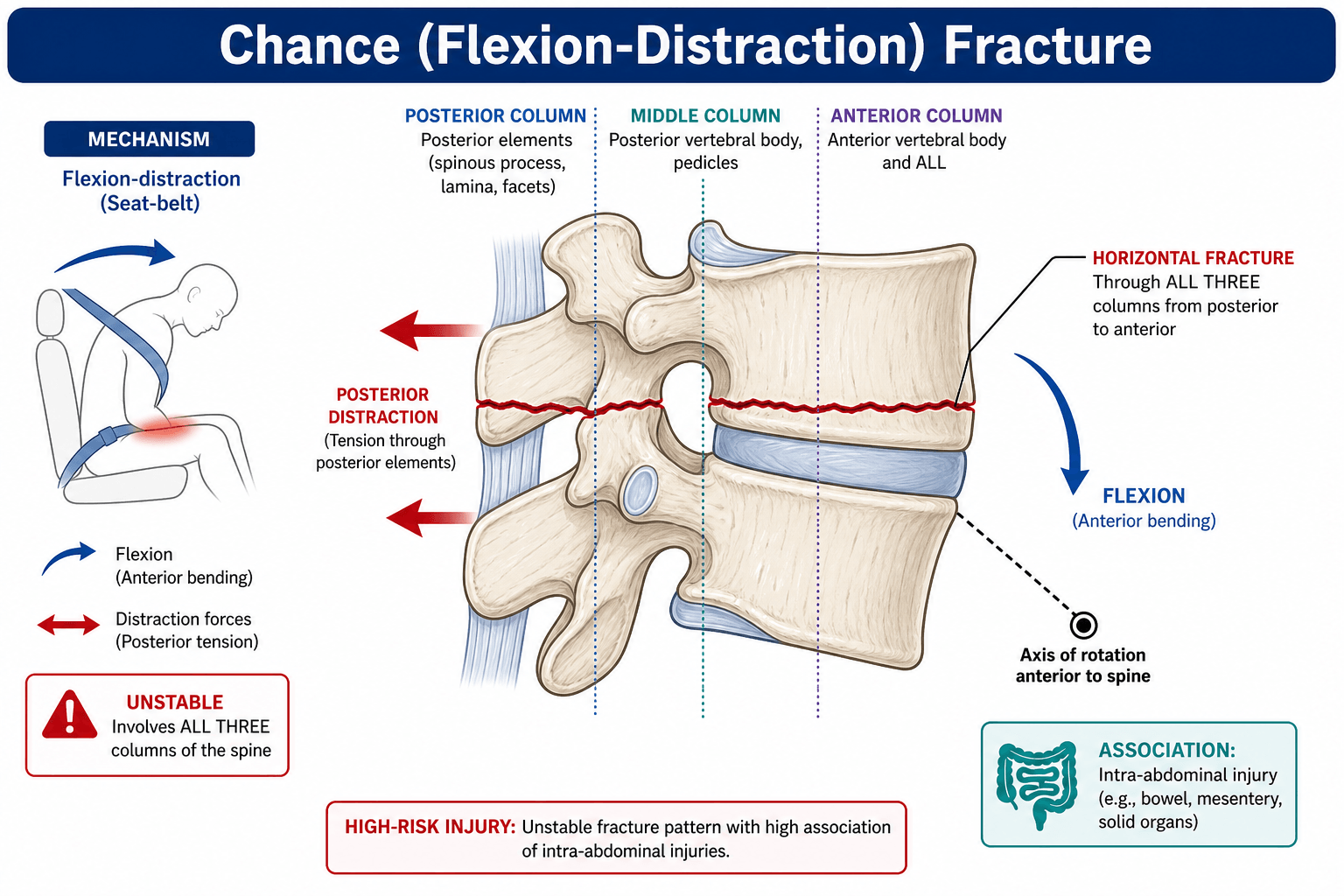
- Classic seatbelt injury = flexion around lap belt fulcrum
- 50% have intra-abdominal injury - always assess abdomen!
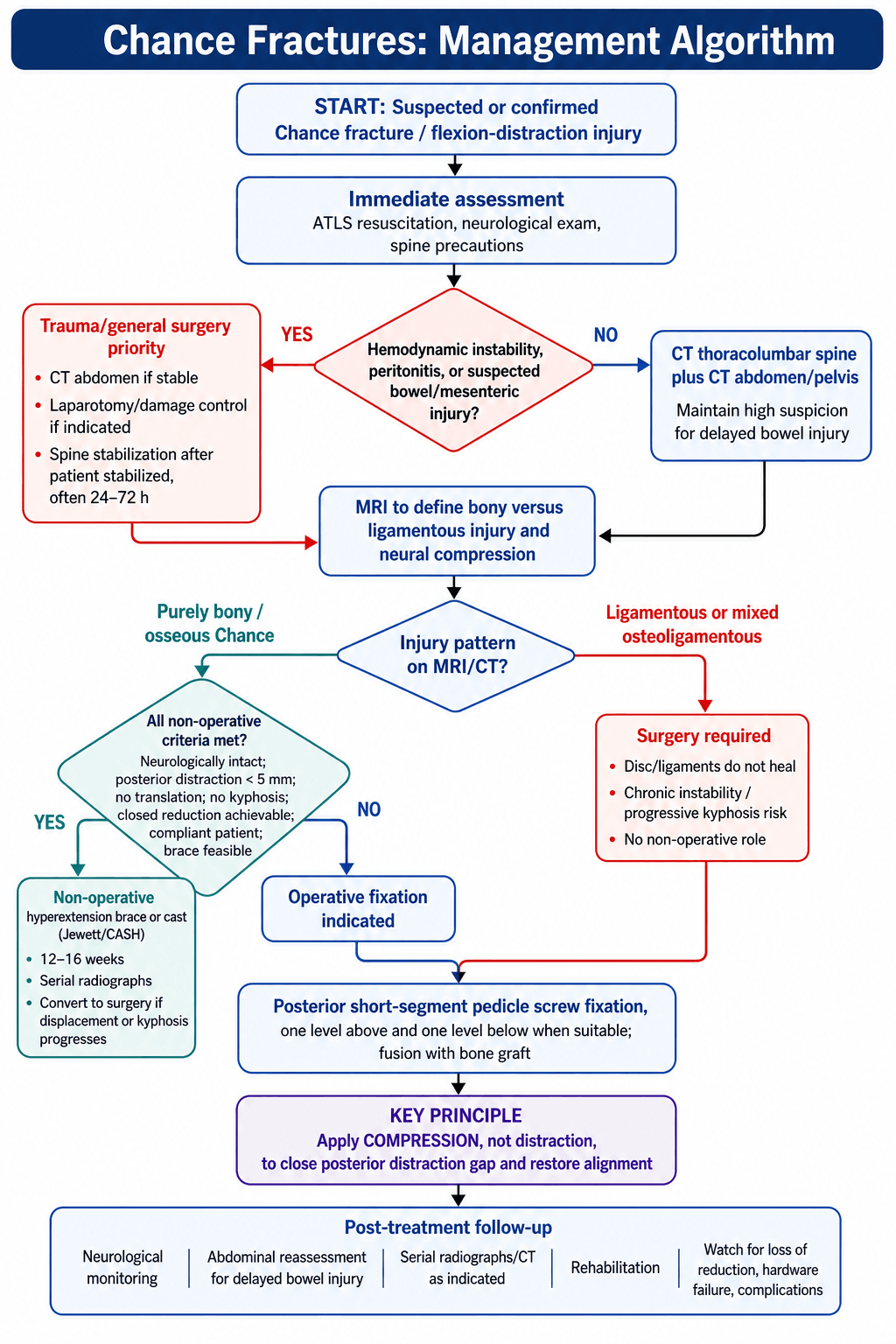
- Bony Chance may be braced if no translation and intact anterior column
- Ligamentous Chance requires surgery - soft tissue will not heal
- Use compression not distraction during posterior fixation
- “Horizontal fracture through ALL posterior elements is pathognomonic
- “Seatbelt sign on abdomen = high suspicion for Chance AND visceral injury
- “TLICS: Distraction=4, so most are surgical unless purely bony
- “Posterior surgery uses COMPRESSION to close the distraction injury
Lap belt acts as fulcrum - patient flexes over belt in MVA. Creates flexion-distraction pattern. 50% have abdominal visceral injury - bowel, mesentery, pancreas.
Bony Chance (through vertebra) heals well - may brace. Ligamentous Chance (through disc) does NOT heal - requires surgical fusion. Critical distinction for treatment.
Always CT abdomen/pelvis. Look for: bowel injury, mesenteric tear, pancreatic injury, retroperitoneal hematoma. Seatbelt bruise on abdomen = high suspicion.
Use COMPRESSION during posterior fixation - this closes the distraction injury. Opposite of burst fractures where distraction is used. Key exam point!
- Displacement
- Less than 5mm, no translation
- Treatment
- Consider hyperextension brace/cast
- Key Pearl
- Must be purely osseous - check MRI
- Displacement
- More than 5mm, kyphosis
- Treatment
- Posterior compression + fusion
- Key Pearl
- Bony heals well with fixation
- Displacement
- Any amount
- Treatment
- Posterior fusion mandatory
- Key Pearl
- Soft tissue will NOT heal
- Displacement
- Variable
- Treatment
- Posterior fusion
- Key Pearl
- Treat as ligamentous
CHANCEChance Fracture Features
Hook:CHANCE: Remember the 50% Abdominal injury rate - never miss it!
SBISeatbelt Injury Triad
Hook:SBI Triad: Seatbelt sign + Bowel injury + spinal Injury (Chance) - always look for all three!
CDCCompression Principle
Hook:In Chance: Distraction is the Disease, Compression is the Cure - opposite of burst!
Overview and Epidemiology
Chance fractures are flexion-distraction injuries of the thoracolumbar spine, classically occurring when a restrained passenger flexes over a lap seatbelt during a motor vehicle accident.
- First described by G.Q. Chance in 1948
- Originally called "seatbelt fracture"
- Classic horizontal fracture line through posterior elements
- Peak at L1-L3 (thoracolumbar junction)
- MVA with lap belt restraint most common mechanism
- Also occurs in falls with flexion
- Pediatric patients at higher risk (lap belt rides higher)
- Associated abdominal injury in approximately 50%
The lap belt acts as a fulcrum - during rapid deceleration, the upper body flexes forward while the pelvis is restrained. This creates a flexion-distraction force that opens the posterior spine while the anterior column pivots over the belt.
Anatomy and Biomechanics
Mechanism of injury:
The flexion-distraction mechanism creates a specific injury pattern:
- Force Type
- Tension (distraction)
- Result
- Horizontal fracture or ligament rupture
- Force Type
- Tension
- Result
- Fracture through body or disc rupture
- Force Type
- Compression or neutral
- Result
- Usually intact or minimal injury
Key anatomical concept:
- Fulcrum at anterior column (lap belt level)
- Posterior elements fail in tension
- Unlike burst fractures where all columns fail in compression
In a pure Chance fracture, the anterior column is intact or minimally injured. This distinguishes it from burst fractures. The injury is primarily a posterior tension failure with the anterior column acting as the fulcrum (pivot point).
- The posterior ligamentous complex is always disrupted (by definition)
- This is why most Chance fractures are considered unstable
- TLICS assigns 4 points for distraction (highest morphology score)
- Anterior column: Fulcrum, usually intact
- Middle column: Fails in tension (disc or posterior body)
- Posterior column: Fails in tension (fracture or ligament)
Classification
The Critical Treatment-Guiding Classification
- Description
- Fracture through vertebral body, pedicles, laminae, spinous process
- Treatment Implication
- Bone heals - may brace if minimal displacement
- Description
- Rupture through disc and posterior ligaments
- Treatment Implication
- Soft tissue does NOT heal - requires surgical fusion
- Description
- Combination of bone and soft tissue failure
- Treatment Implication
- Treat as ligamentous - surgery required
Bony Chance may be managed non-operatively because bone heals. Ligamentous Chance MUST be surgically fused because the disc and ligaments will NOT heal and will result in chronic instability. MRI is essential to determine the type.
Clinical Assessment
History:
- MVA details (especially restraint type - lap belt vs 3-point)
- Mechanism of impact
- Abdominal symptoms (pain, distension, vomiting)
- Neurological symptoms
Physical examination:
- Palpable gap: Widened interspinous space is classic finding
- Tenderness: Focal at fracture level
- Kyphotic deformity: May be visible or palpable
- Complete neuro exam: Lower extremities and perianal
- Seatbelt sign: Transverse bruising across abdomen
- Tenderness: Generalized or focal
- Distension: May indicate bleeding/ileus
- Peritonitis signs: Guarding, rigidity
Transverse abdominal wall bruising (seatbelt sign) should trigger:
- High suspicion for Chance fracture
- High suspicion for intra-abdominal injury
- CT thoracolumbar spine AND CT abdomen/pelvis
This is a two-cavity injury pattern - never assess just one!
Neurological examination:
- Complete lower extremity motor and sensory
- Perianal sensation (sacral sparing)
- Rectal tone
- Reflexes (may be hypo/hyperreflexic depending on level)
Investigations
Imaging Algorithm
Shows osseous injury. Look for horizontal fracture line through posterior elements. Sagittal reconstructions best to appreciate flexion-distraction pattern.
Mandatory for Chance fractures. Look for bowel wall thickening, free fluid, mesenteric hematoma, pancreatic injury. Do NOT wait for symptoms - injury may be delayed.
Determines bony vs ligamentous. Essential for treatment decision. Shows disc status, PLC injury extent, cord/cauda status.
CT findings:
Classic Chance fracture on CT:
- Horizontal fracture line through spinous process, laminae, transverse processes, pedicles, and vertebral body
- Widened interspinous space at injury level
- Empty facet sign if facets subluxed
- Minimal anterior column compression (distinguishes from burst)
- Chance Fracture
- Distraction (flexion-distraction)
- Burst Fracture
- Compression (axial)
- Chance Fracture
- Horizontal through posterior elements
- Burst Fracture
- Comminuted vertebral body
- Chance Fracture
- Fractured or widened space
- Burst Fracture
- Usually intact
- Chance Fracture
- Minimal (no retropulsion)
- Burst Fracture
- Common (retropulsed fragment)
- Chance Fracture
- Abdominal in 50%
- Burst Fracture
- Calcaneus, other spine levels
Differential Diagnosis
- Mechanism / Key feature
- Posterior tension over lap-belt fulcrum
- Distinguishing feature from Chance
- Horizontal split through posterior elements, intact/minimal anterior column
- Stability / management
- Unstable in tension - compression fixation or brace if purely bony
- Mechanism / Key feature
- Axial compression
- Distinguishing feature from Chance
- Comminuted body with retropulsion and canal compromise; posterior elements often intact
- Stability / management
- Variable - distraction/reconstruction, not compression
- Mechanism / Key feature
- Anterior column compression only
- Distinguishing feature from Chance
- Anterior wedging with intact middle/posterior columns
- Stability / management
- Usually stable - non-operative
- Mechanism / Key feature
- Translation/rotation, all columns
- Distinguishing feature from Chance
- Translation or rotational malalignment, often neurological deficit
- Stability / management
- Highly unstable - surgical stabilisation
- Mechanism / Key feature
- Low-energy, elderly
- Distinguishing feature from Chance
- Marrow oedema without high-energy mechanism; no seatbelt sign
- Stability / management
- Often non-operative or cement augmentation
- Mechanism / Key feature
- Trivial trauma on fused spine
- Distinguishing feature from Chance
- Transverse fracture through ankylosed segment, three-column unstable
- Stability / management
- Highly unstable - long-segment fixation
MRI distinguishes bony from ligamentous Chance:
- Bony: Low signal fracture line through vertebral body, bone marrow edema
- Ligamentous: High T2 signal in disc, disrupted PLC, no bone fracture through body
- Mixed: Features of both
This distinction determines whether non-operative treatment is possible.
A transverse, Chance-like fracture in a patient with ankylosing spondylitis or DISH is a different and far more dangerous entity. The rigid, often osteoporotic, fused "bamboo"/flowing-ossification spine behaves like a long bone: a trivial low-energy injury (a simple fall or even hyperextension) produces a highly unstable three-column fracture, frequently through a disc space or ankylosed segment and often an extension rather than flexion pattern. These fractures are easily missed (the line hides in the fused mass and plain films are unreliable), carry a high rate of epidural haematoma, delayed neurological deterioration and mortality, and mandate whole-spine CT and MRI. Management differs fundamentally from a typical Chance: long-segment posterior instrumentation (multiple levels above and below, not short-segment) is required because of the long rigid lever arms, and the patient must be handled in their fixed deformity, never forced to neutral.

Management
Management of Osseous Chance Fractures
- Purely bony injury (no soft tissue component on MRI)
- Minimal displacement (less than 5mm posterior distraction)
- No translation
- No kyphosis
- Neurologically intact
- Compliant patient
- Hyperextension brace or cast (Jewett or CASH brace)
- The extension posture closes the distraction injury
- Duration: 12-16 weeks
- Serial X-rays to monitor alignment
- Convert to surgery if progression
- Significant displacement (more than 5mm)
- Kyphosis
- Unable to achieve closed reduction
- Neurological deficit
- Associated injuries requiring surgery
- Unable to brace (body habitus, compliance)
The hyperextension brace works because it closes the posterior distraction injury. By extending the spine, the posterior elements approximate. This is the opposite of bracing a compression fracture where you want extension to open the compressed segment.
BLBony vs Ligamentous Treatment
Hook:Bony = Brace possible, Ligamentous = needs Locking (surgery)!
Surgical Technique Details
- Neurological injury: Less than 1% if intact pre-op
- Infection: 1-3%
- Hardware failure: Low with compression fixation
- Non-union: Rare if adequately compressed
- Adjacent segment disease: Long-term risk
- Pedicle screws: Polyaxial preferred
- Compression device: In-line compressor on rod
- Imaging: Fluoroscopy
- Bone graft: Local + allograft
- Neuromonitoring: If neurological deficit
Complications
- Incidence
- Initial 5-10%
- Prevention/Management
- High suspicion, repeat imaging if concern
- Incidence
- Less than 5%
- Prevention/Management
- Adequate compression, avoid distraction
- Incidence
- 5%
- Prevention/Management
- Bone graft, smoking cessation
- Incidence
- 5-10%
- Prevention/Management
- Adequate compression, short segment usually sufficient
- Incidence
- Less than 1%
- Prevention/Management
- Careful technique, neuromonitoring
- Incidence
- 10-20%
- Prevention/Management
- Patient education, rehabilitation
- Most dangerous early complication
- Bowel injury can present 24-48 hours after initial CT
- Maintain high suspicion
- Low threshold for repeat imaging
- Rare if surgically fused with adequate compression
- Higher risk if non-op attempted for ligamentous injury
Postoperative Care
Rehabilitation Timeline
Monitor for abdominal complications. DVT prophylaxis. Pain management. Mobilize when cleared by trauma team.
Progressive mobilization. Wound check. May use TLSO for additional support if desired.
Continue brace if used. Serial X-rays. Core strengthening. Activity progression.
CT to confirm fusion. Wean brace. Return to normal activities.
- Variable practice
- Some use TLSO 6-12 weeks for comfort/reminder
- Others rely on instrumentation alone
- Short segment fixation generally stable enough
- Monitor for adjacent segment disease (less common than burst due to short segment)
- Assess for chronic pain
- Confirm fusion on CT
Outcomes and Prognosis
- High fusion rates with adequate compression
- Low hardware failure (anterior column intact)
- Good restoration of alignment
- Most return to normal function
- Purely bony: Excellent healing with brace or surgery
- Ligamentous: Excellent with surgical fusion
- Ligamentous treated non-op: Poor (chronic instability)
- Most Chance fractures are neurologically intact
- If deficit present, prognosis depends on severity
- Cauda equina level - generally good recovery
- Associated abdominal injury increases morbidity
- May delay spine surgery
- Coordinate with general surgery team
Guidelines, Registries & Global Practice
Global Epidemiology
Flexion-distraction (Chance) injuries are a minority of thoracolumbar fractures but carry a disproportionate burden of associated visceral and neurological injury. In the original lap-belt era series, 32 of 38 restrained occupants (84%) sustained abdominal injury, with bowel or mesenteric injury in 27 of 32 (Denis et al, 1983). In a prospective cohort, abdominal injury occurred in 64% of patients with a seatbelt sign versus 8.7% without, and small-bowel perforation in 21% of those with the sign (Chandler et al, 1997). In the paediatric population, a two-decade single-centre series found abdominal visceral injury in 42% and neurological injury in 27% of children with lumbar Chance fractures, with injuries occurring even when a three-point belt was correctly worn (Louman-Gardiner et al, 2008). The shift from lap-only to three-point restraints has reduced but not eliminated these injuries, particularly in rear-seat and incorrectly restrained children.
Side-by-Side Guidance & Classification
- Key parameter for Chance injury
- Tension failure of middle and posterior columns
- Surgical threshold
- Instability when 2+ columns disrupted
- Evidence level
- Level 4 (classification)
- Key parameter for Chance injury
- Distraction morphology = 4; PLC disrupted = 3
- Surgical threshold
- TLICS greater than 4 favours surgery
- Evidence level
- Level 5 (consensus)
- Key parameter for Chance injury
- Type B (tension band / distraction) injury
- Surgical threshold
- AOSpine-TLICS greater than 5 favours surgery
- Evidence level
- Level 5 (consensus)
- Key parameter for Chance injury
- Multisystem assessment, exclude visceral injury
- Surgical threshold
- Operative for distraction/ligamentous instability
- Evidence level
- Guideline / expert
- Key parameter for Chance injury
- Whole-spine imaging, MRI if PLC/ligamentous concern
- Surgical threshold
- Surgical referral for unstable injuries
- Evidence level
- Guideline / expert
- No dedicated arthroplasty-style registry captures Chance fractures; evidence is case-series and trauma-registry based
- Managed within major trauma centre networks with combined general/spine surgery
- Paediatric trauma centres for children (higher visceral-injury rate)
- National road-trauma registries track restraint type and mechanism
- Three-point belts mandatory in most high-income countries; lap-only belts persist in older vehicles and some rear/middle seats
- Brace-versus-fixation threshold for purely bony injuries varies between units
- Short-segment posterior compression fixation is the dominant operative approach worldwide
- Child-restraint enforcement and booster-seat use differ markedly by region
restraint use and type, abdominal examination and CT findings, MRI bony-versus-ligamentous status, treatment rationale, and patient/family communication.
missed or delayed abdominal injury, failure to obtain abdominal CT initially, treating ligamentous Chance non-operatively, and not recording restraint type for road-trauma surveillance.
MCQ Practice Points
Q: What percentage of Chance fractures have associated intra-abdominal injury? A: 50% - this is the most commonly tested association. Always CT abdomen with Chance fracture.
Q: What is the mechanism of a Chance fracture? A: Flexion-distraction - the patient flexes forward over the lap belt fulcrum, creating tension failure of the posterior and middle columns.
Q: When fixing a Chance fracture posteriorly, should you use compression or distraction? A: COMPRESSION - this closes the distraction injury. This is the opposite of burst fractures.
Q: Which type of Chance fracture can be managed non-operatively? A: Bony (osseous) Chance with minimal displacement - bone heals. Ligamentous Chance MUST be fused - disc and ligaments will not heal.
Q: What is the TLICS morphology score for a Chance fracture? A: 4 points (distraction) - the highest morphology score. Combined with disrupted PLC (3), most Chance fractures score TLICS 7+.
Q: What physical exam finding on the abdomen should raise suspicion for Chance fracture? A: Transverse abdominal bruising (seatbelt sign) - indicates lap belt mechanism and high risk for both Chance fracture AND visceral injury.
Clinical Imaging
Imaging Atlas


Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old restrained back-seat passenger is brought in after an MVA. She has transverse bruising across her abdomen and tenderness at the thoracolumbar junction. CT shows a horizontal fracture through L2 spinous process, laminae, pedicles, and superior vertebral body. She is neurologically intact. How do you manage her?”
“A 40-year-old man has an L1-L2 Chance fracture. MRI shows the fracture goes through the L1-2 disc with complete disruption of the posterior ligaments. He has bilateral lower extremity weakness (4/5 throughout) and urinary retention. Describe your surgical approach.”
“A 6-year-old restrained in a booster seat is involved in an MVA. She has a seatbelt mark on her abdomen and back pain. CT shows a horizontal fracture through L3. Her abdominal CT shows free fluid. How do you manage this case?”
Definition and Mechanism
- Flexion-distraction injury (seatbelt mechanism)
- Lap belt acts as fulcrum
- Posterior elements fail in tension
- Anterior column intact (pivot point)
50% Rule - CRITICAL
- 50% have associated abdominal injury
- ALWAYS CT abdomen/pelvis
- Bowel, mesentery, pancreas most common
- Seatbelt sign = high suspicion for both
Bony vs Ligamentous
- Bony: Through vertebra, may brace if minimal displacement
- Ligamentous: Through disc/ligaments, MUST fuse
- MRI is essential to determine type
- Mixed = treat as ligamentous
Surgical Principle
- Use COMPRESSION not distraction
- This closes the posterior distraction injury
- Opposite of burst fracture management
- Short segment usually sufficient
TLICS Application
- Distraction = 4 points (highest morphology)
- PLC always disrupted = 3 points
- Most score TLICS 7+ = surgical
- Only purely bony minimal displacement may brace
Key Facts
- L1-L3 most common levels
- Horizontal fracture line is pathognomonic
- Compression during fixation closes injury
- Never miss the abdominal injury
Evidence Base
Original Description (1948)
- First description of horizontal flexion fracture of the spine
- Described the fracture line through the vertebral body and posterior arch
- Anterior column acts as fulcrum in flexion
- Established the classic imaging appearance now bearing his name
Seatbelt Syndrome - Abdominal Injury
- 32 of 38 restrained occupants (84%) had abdominal injury in this series
- 27 of 32 injured had bowel or mesenteric injury
- Highlighted the altered injury physics of lap-belt deceleration
- Established the high association between belt restraint and visceral injury
Seatbelt Sign & Bowel Injury
- Prospective study of 117 motor vehicle accident victims
- Abdominal injury in 64% of those with a seatbelt sign vs 8.7% without
- Small-bowel perforation in 21% of seatbelt-sign patients
- Seatbelt sign mandates a heightened index of suspicion