Lateral Column Degenerative Disease | Triple Joint Complex | Often Overlooked
- CC joint is critical for lateral column stability and load transfer
- Rarely occurs in isolation - assess talonavicular and subtalar joints
- Triple arthrodesis indicated when multiple hindfoot joints involved
- Peroneal tendon pathology commonly coexists
- Lateral approach risks sural nerve and peroneal tendons
- “CC joint contributes to lateral column length and forefoot abduction
- “Nutcracker fracture of cuboid predisposes to CC arthritis
- “Isolated CC fusion rare - usually part of triple arthrodesis
- “Sural nerve at risk with lateral approach
CC joint maintains lateral column length. Loss leads to forefoot adduction and cavovarus deformity. Critical for proper foot biomechanics.
Isolated CC arthritis is rare (5-10%). Typically occurs with talonavicular or subtalar pathology. Always perform comprehensive hindfoot assessment.
Isolated CC fusion has higher nonunion rates than TN. Triple arthrodesis more common. Lateral approach risks sural nerve.
Peroneal tendon pathology in 30-40% of cases. Assess for tears or tendinopathy during lateral approach.
Overview and Epidemiology
Calcaneocuboid arthritis represents degeneration of the articulation between the anterior process of the calcaneus and the cuboid bone. As part of the lateral column, CC joint pathology affects forefoot alignment and lateral stability. It rarely occurs in isolation and is commonly associated with adjacent joint pathology, post-traumatic changes, or inflammatory arthropathy.
- Post-traumatic: Calcaneal fractures, nutcracker injuries
- Inflammatory: Rheumatoid arthritis, seronegative arthropathy
- Degenerative: Primary osteoarthritis (rare in isolation)
- Malalignment: Hindfoot varus/valgus causing abnormal loading
- Peroneal pathology: Tendon dysfunction altering mechanics
- Calcaneal fractures: 30-40% develop CC arthritis
- Peroneal tendon tears: 30-40% coexistence
- Talonavicular arthritis: 60% have concurrent CC involvement
- Subtalar arthritis: 50% association
- Cavovarus foot: Chronic lateral column overload
Pathophysiology
The calcaneocuboid joint is a saddle-shaped articulation that forms the lateral component of the transverse tarsal (Chopart) joint. It contributes to hindfoot-forefoot power transmission and allows limited motion for terrain adaptation. The joint bears approximately 15-20% of forefoot load during stance phase.
- Saddle joint morphology: Concave-convex articulation
- Coupled motion: Functions with TN joint in transverse tarsal complex
- Load transmission: Lateral column weight transfer
- Locking mechanism: Stabilizes lateral column during toe-off
- Forefoot position: Controls abduction/adduction
The CC joint allows approximately 5-10 degrees of motion in the sagittal and transverse planes.
- Cartilage degeneration: Progressive articular surface loss
- Subchondral sclerosis: Bone stiffening response
- Osteophyte formation: Peripheral bone spurs
- Synovitis: Inflammatory capsular changes
- Lateral column shortening: Loss of joint height
Progressive arthritis leads to abnormal load transfer and compensatory forefoot adduction.
- CC Joint
- Minimal (5-10°)
- TN Joint
- Significant (50-60% hindfoot motion)
- Subtalar Joint
- Significant (50-70% hindfoot motion)
- CC Joint
- 15-20% lateral
- TN Joint
- Major medial column
- Subtalar Joint
- Full body weight
- CC Joint
- Rare (5-10%)
- TN Joint
- Common (40% midfoot OA)
- Subtalar Joint
- Common
- CC Joint
- 75-85%
- TN Joint
- 85-95%
- Subtalar Joint
- 90-95%
Following calcaneal fractures, CC arthritis develops through: (1) Direct articular damage from the injury, (2) Malunion causing abnormal joint loading, (3) Lateral column shortening altering biomechanics. The nutcracker mechanism specifically affects the CC joint through forced abduction causing cuboid compression between the calcaneus and 4th/5th metatarsal bases.
Clinical Assessment
- Pain location: Lateral midfoot, inferior to lateral malleolus
- Pain character: Dull ache, worsens with activity
- Aggravating factors: Walking on uneven ground, lateral stress
- Previous trauma: Calcaneal fracture, midfoot injury
- Footwear issues: Difficulty with narrow shoes
- Function: Reduced walking tolerance
Ask specifically about prior calcaneal fractures as 30-40% develop CC arthritis.
- Inspection: Lateral column alignment, swelling
- Palpation: CC joint tenderness, lateral foot
- Range of motion: Reduced forefoot abduction/adduction
- Peroneal assessment: Strength, tendon integrity
- Gait: Lateral foot stress pattern
- Adjacent joints: TN, subtalar examination
The single heel rise test helps assess associated tibialis posterior dysfunction.
30-40% of CC arthritis cases have coexisting peroneal tendon pathology. Perform peroneal strength testing, palpate along tendon course for tenderness or thickening, and assess for subluxation. MRI indicated if clinical suspicion high.
Differential Diagnosis of Lateral Midfoot Pain
- Key distinguishing feature
- Tenderness directly over CC joint; pain on forefoot abduction/adduction; lateral column degeneration
- Best test
- Weight-bearing radiographs; diagnostic CC injection
- Key distinguishing feature
- Tenderness along tendon course behind/below lateral malleolus; pain on resisted eversion
- Best test
- MRI; dynamic ultrasound
- Key distinguishing feature
- Acute or overuse onset; point tenderness over cuboid; history of forced abduction
- Best test
- MRI / CT; bone scan
- Key distinguishing feature
- Pain in sinus tarsi; reduced inversion/eversion; pain on hindfoot rotation
- Best test
- CT; subtalar injection
- Key distinguishing feature
- Lateral hindfoot pain and instability sensation, often post-sprain
- Best test
- MRI; diagnostic injection
- Key distinguishing feature
- Discrete tender ossicle in peroneus longus, plantar-lateral cuboid
- Best test
- Oblique radiograph; MRI
- Key distinguishing feature
- Rigid flatfoot, restricted subtalar motion, younger patient
- Best test
- Oblique radiograph; CT/MRI
- Key distinguishing feature
- Tenderness more distal at styloid; avulsion or Jones fracture history
- Best test
- AP/oblique radiographs
Clinical Examination Sequence
Assess lateral column alignment, swelling, skin changes, and overall foot posture in weight-bearing.
Localize tenderness to CC joint (anterior to lateral malleolus). Compare with TN and subtalar joint tenderness.
Assess forefoot abduction/adduction with hindfoot stabilized. Compare with contralateral side.
Single heel rise test, peroneal strength, Coleman block test if cavovarus suspected.
Systematically assess TN joint, subtalar joint, and ankle for concurrent pathology.
Investigations
Imaging Protocol
Views: AP, lateral, oblique foot radiographs standing. CC assessment: Joint space, osteophytes, sclerosis. Alignment: Lateral column length, forefoot position. Adjacent joints: Evaluate TN and subtalar joints.
Indications: Surgical planning, assess deformity. Detail: Bone stock, subchondral changes, fusion planning. Role: Identify occult fractures, coalition.
Indications: Assess peroneal tendons, cartilage, soft tissue. Findings: Tendon tears, bone marrow edema, synovitis. Role: Pre-operative planning when tendon pathology suspected.

Key radiographic findings include: joint space narrowing, subchondral sclerosis, osteophyte formation (especially dorsal), subchondral cyst formation, and lateral column shortening. Compare lateral column length with contralateral foot. On lateral view, assess for dorsal CC osteophytes impinging on extensor tendons.
Diagnostic Calcaneocuboid Injection: Confirming the Pain Generator
Because CC arthritis rarely occurs in isolation and lateral midfoot pain has many mimics (peroneal tendinopathy, sinus tarsi syndrome, subtalar arthritis, cuboid/nutcracker pathology, an os peroneum), radiographic CC degeneration does not by itself prove the CC joint is the source of a patient's symptoms. An image-guided intra-articular injection of local anaesthetic (with or without corticosteroid) is the single most useful confirmatory test before committing to an irreversible fusion. This is why the differential-diagnosis table lists a diagnostic CC injection as the definitive test, and it directly answers the commonest viva trap of missing concurrent talonavicular or subtalar disease.
- Guidance is essential: fluoroscopy or ultrasound — the CC saddle joint is small and blind injection frequently misses or spills into adjacent structures
- Small volume: approximately 1 mL of local anaesthetic keeps the response joint-specific
- Document the response: a pain diary with a defined task (walking, single-leg stance) recorded during the anaesthetic window
- Positive test: substantial, temporary pain relief during the anaesthetic window localises the pain generator to the CC joint
- Good relief supports the CC joint as the target and, with normal adjacent joints, an isolated CC fusion
- No / equivocal relief should stop you fusing the CC joint — reassess adjacent joints (a separate subtalar or TN injection) and the peroneal sheath
- A separate response pattern may redirect surgery to double or triple arthrodesis or tendon surgery
- Adds therapeutic value when corticosteroid is included in the conservative phase
Interpret the injection alongside the clinical and radiographic picture: anaesthetic can diffuse into the adjacent subtalar joint or peroneal sheath, reducing specificity, and a good anaesthetic response confirms the pain source but does not guarantee that fusion will relieve it or unite.
The single most useful test to decide between an isolated CC fusion and a more extensive fusion is a guided diagnostic CC injection: temporary pain relief confirms the CC joint as the symptomatic source, whereas absent relief should stop you fusing it and prompt a search for an adjacent (subtalar/TN) or peroneal cause.
Management
Non-Operative Treatment
Conservative Protocol
Reduce lateral column stress activities. Supportive footwear with lateral posting.
The goal is to minimize abnormal loading on the degenerative CC joint.
Custom orthoses with lateral forefoot support. Off-the-shelf lateral wedge insoles.
Orthotics redistribute load and support the lateral column.
NSAIDs for pain control. Corticosteroid injection under guidance (maximum 2-3 per year).
Fluoroscopic or ultrasound-guided injection improves accuracy.
Peroneal strengthening. Ankle stabilization exercises. Gait retraining.
Address any associated peroneal weakness or dysfunction.
Conservative management is successful in approximately 60-70% of patients with mild to moderate CC arthritis.
Surgical Technique: Isolated CC Arthrodesis
Lateral Approach to Calcaneocuboid Joint
Surgical Steps
Supine with bump under ipsilateral hip. Thigh tourniquet. C-arm for imaging.
Ensure adequate access to lateral foot with hip externally rotated.
Oblique incision over CC joint, anterior to lateral malleolus, 6-8cm length.
Follow Langer's lines to minimize scar contracture.
Identify and protect sural nerve. Elevate peroneal tendons carefully.
Sural nerve typically runs 1-2cm posterior to incision but has variable course.
Incise CC joint capsule. Expose articular surfaces. Assess peroneal tendons.
Systematically inspect peroneal tendons for tears requiring repair.
Sural nerve runs along lateral border of foot, at risk with lateral approach. Identify early in dissection and protect throughout. Injury rate 5-10% in reported series.
Complications
- Incidence
- 15-25% (higher than TN)
- Management
- Revision with bone graft and plate
- Incidence
- 5-10%
- Management
- Usually resolves; neurolysis if persistent
- Incidence
- 25-35% at 10 years
- Management
- Activity modification, possible future fusion
- Incidence
- 10-15%
- Management
- Hardware removal after union
- Incidence
- 5-8%
- Management
- Wound care, antibiotics, possible debridement
Risk factors for CC fusion nonunion include: smoking (strongest predictor), diabetes mellitus, inadequate fixation, poor bone contact, peripheral vascular disease, immunosuppression, and revision surgery. Pre-operative smoking cessation for minimum 4 weeks is recommended.
Managing the Calcaneocuboid Fusion Nonunion
Isolated CC arthrodesis carries the highest nonunion rate of the individual hindfoot/midfoot fusions (roughly 15 to 25 percent, against 10 to 15 percent for talonavicular fusion) — a point the complications table and viva follow-ups repeatedly raise but which the topic does not otherwise develop. The reasons are specific to this joint: a small cancellous contact surface, high compressive and rotational loads across the lateral column, and a frequently scarred or relatively avascular post-traumatic bed. Knowing how to salvage a failed fusion is therefore a predictable examiner question.
- Not every nonunion is symptomatic: a stable fibrous nonunion in a comfortable patient can be observed
- Symptomatic clues: persistent lateral pain, hardware loosening or lucency, progressive lateral column collapse
- CT confirms it: plain films over-call union across the small saddle joint, so CT is the reference test
- Exclude confounders: low-grade infection, and uncorrected host factors before revising
- Correct the cause: confirmed smoking cessation, optimise vitamin D/metabolic status, treat any infection
- Prepare a fresh bed: take the fibrous interface down to bleeding bone
- Restore lateral column length: structural autograft/allograft or a distraction bone-block if shortened
- Upgrade fixation: from screws alone to a rigid compression plate with or without a lag screw; add biologic/autologous graft
Where the CC joint is heavily scarred and the adjacent joints are themselves degenerating, extending the construct to a double or triple arthrodesis provides a larger, more reliable fusion surface (the technique of triple/double fusion is covered in the dedicated arthrodesis topics). Structural graft to restore lateral column length echoes the distraction-arthrodesis principle and prevents the forefoot adduction that follows lateral column shortening.
A painful CC nonunion is confirmed on CT, not plain films. Salvage means correcting host factors (smoking, metabolic status, occult infection), taking the interface down to bleeding bone, restoring lateral column length with structural graft, and converting to rigid plate compression — or extending to a double/triple fusion when adjacent joints are involved.
Guidelines, Registries & Global Practice
Global epidemiology. Symptomatic radiographic midfoot OA affects roughly 12% of community-dwelling adults over 50 (Keele Clinical Assessment Study of the Foot), rising with age, female sex, obesity and prior foot/ankle injury. Isolated CC arthritis is uncommon; most CC degeneration is post-traumatic (after calcaneal or cuboid/nutcracker fractures) or part of broader midfoot/hindfoot OA. There is no dedicated arthroplasty registry for the CC joint because management is fusion-based, not implant-based.
Side-by-side guidance. No society publishes a CC-arthritis-specific guideline; recommendations are extrapolated from foot OA and hindfoot fusion principles.
- Region
- US
- Relevant position
- Trial of orthoses, NSAIDs and activity modification before fusion; selective single/double fusion preferred over triple when feasible to preserve motion
- Region
- UK
- Relevant position
- Generic OA guidance (exercise, weight loss, analgesia) first; calcaneal-fracture BOAST stresses anatomic articular reduction to limit later subtalar/CC arthritis
- Region
- Global
- Relevant position
- Restore lateral column length and articular congruity in cuboid/calcaneal fractures; rigid compression fixation for CC fusion with bone graft if risk factors
- Region
- Europe
- Relevant position
- Subtalar-sparing (isolated/double) fusion where adjacent joints preserved; emphasises peri-operative smoking cessation to reduce nonunion
Registry and outcome evidence. Calcaneal fracture registries and the Buckley RCT show that articular malreduction (step-off over 2 mm) drives post-traumatic subtalar and CC arthritis — the dominant route to symptomatic CC disease worldwide.
High- versus limited-resource practice. In well-resourced systems, weight-bearing CT, MRI for peroneal assessment and rigid plate/screw constructs with biologics are standard. In limited-resource settings, plain weight-bearing radiographs and screw-only fixation predominate, late presentation of malunited calcaneal fractures is more common, and accommodative orthoses with footwear modification carry a larger share of definitive care. Smoking cessation for a minimum of 4 weeks before fusion is a universal, low-cost intervention that reduces nonunion.
Controversies & Areas of Uncertainty
Whether truly isolated CC arthritis exists often enough to justify isolated fusion is debated. Isolated CC fusion carries a higher nonunion rate than TN fusion, and some surgeons favour double or triple arthrodesis for more predictable union. The counter-argument is preservation of TN and subtalar motion. Evidence is limited to small retrospective series.
Interposition arthroplasty and joint-preserving distraction for early CC arthritis remain experimental with sparse, low-quality data. There is no validated implant or established role; fusion remains the reference standard for end-stage disease.
CT helical-axis work (Beimers 2012) suggests fusing the CC joint may reduce global hindfoot motion less than once feared, since the CC contributes a small share. This challenges the historical reluctance to fuse it within lateral column lengthening.
Optimal fixation (parallel screws vs plate vs combined) and whether routine autograft, allograft or orthobiologics meaningfully lower nonunion are unresolved; recommendations are extrapolated from general hindfoot fusion data rather than CC-specific trials.
MCQ Practice Points
Q: What percentage of midfoot arthritis cases involve the calcaneocuboid joint? A: 10-15% - CC arthritis is less common than talonavicular arthritis (40% of midfoot arthritis). CC typically occurs as part of triple complex pathology.
Q: What is the most common cause of calcaneocuboid arthritis? A: Post-traumatic - Calcaneal fractures lead to CC arthritis in 30-40% of cases. Nutcracker mechanism cuboid injuries also predispose.
Q: What is the nonunion rate for isolated calcaneocuboid arthrodesis? A: 15-25% - Higher than talonavicular fusion (10-15%). Risk factors include smoking, diabetes, inadequate fixation, and poor bone contact.
Q: What nerve is at risk during lateral approach to the calcaneocuboid joint? A: Sural nerve - Runs along lateral foot border. Injury incidence 5-10%. Must be identified and protected throughout surgery.
Q: What percentage of CC arthritis cases have concurrent peroneal tendon pathology? A: 30-40% - Peroneal tendons should be inspected during lateral approach and any tears addressed with repair or tenosynovectomy.
Q: What happens to the forefoot if lateral column length is not maintained during CC fusion? A: Forefoot adduction - Loss of lateral column length causes relative forefoot adduction and can lead to medial overload and cavovarus deformity.
At a Glance
Calcaneocuboid (CC) arthritis is a relatively uncommon cause of lateral midfoot pain, representing 10-15% of midfoot arthritis cases, with isolated CC arthritis rare (5-10%). The CC joint is critical for lateral column stability and forefoot alignment—degeneration leads to lateral column shortening and forefoot adduction. CC arthritis rarely occurs in isolation; always assess talonavicular and subtalar joints for concurrent pathology requiring triple arthrodesis. Nutcracker fracture of the cuboid is a common predisposing cause. Peroneal tendon pathology coexists in 30-40% of cases. Isolated CC fusion has higher nonunion rates than TN fusion; surgical approach risks the sural nerve and peroneal tendons.
COLUMNCalcaneocuboid Joint Function
Hook:The CC joint is the lateral COLUMN - essential for lateral foot stability!
TRAUMACC Arthritis Etiologies
Hook:TRAUMA causes CC arthritis - especially calcaneal fractures!
SCARECC Fusion Surgical Risks
Hook:Don't let complications SCARE you - but know them for the viva!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old presents with lateral midfoot pain 3 years after calcaneal fracture treated non-operatively. Examination shows lateral column tenderness. Weight-bearing X-rays show CC joint narrowing with sclerosis. How would you manage?”
“Walk me through your surgical technique for isolated calcaneocuboid arthrodesis.”
“A 62-year-old presents with progressive lateral and medial midfoot pain. X-rays show CC arthritis with concurrent TN arthritis. Subtalar joint appears preserved. What is your management approach?”
Key Anatomy
- CC joint = lateral column stabilizer
- Part of triple joint complex with TN and subtalar
- Maintains lateral column length and forefoot alignment
- Sural nerve runs lateral - at risk with lateral approach
Classification
- Mild = joint space narrowing, minimal osteophytes
- Moderate = significant narrowing, sclerosis
- Severe = bone-on-bone, deformity
- Rarely isolated - usually part of triple complex
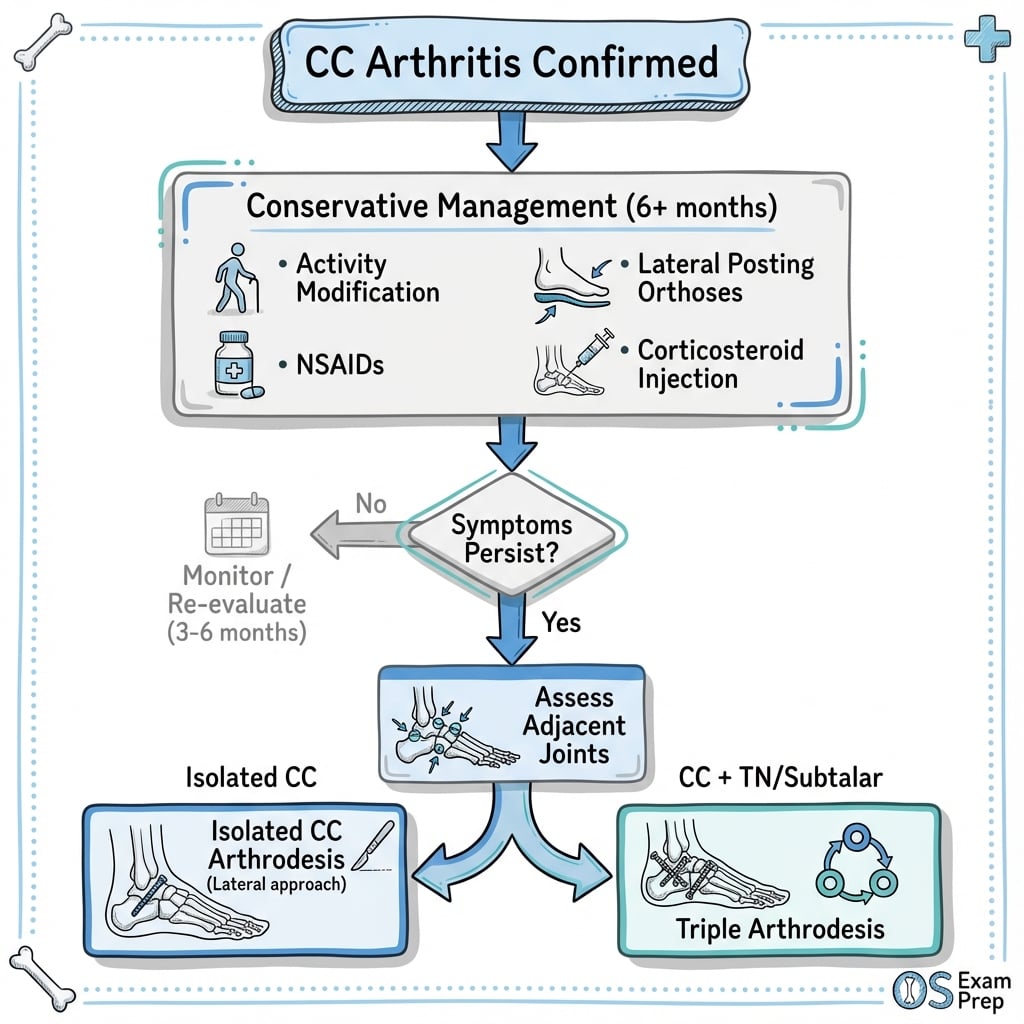
Treatment Algorithm
- Conservative: 6 months with orthoses, NSAIDs, lateral posting
- Isolated CC = isolated CC fusion (if adjacent joints normal)
- CC + TN or subtalar = triple arthrodesis
- Post-traumatic from calcaneal fracture most common
Surgical Pearls
- Lateral approach with sural nerve protection
- Two 4.0mm parallel screws standard fixation
- Consider bone graft (higher nonunion risk than TN)
- Non-weight-bearing 8 weeks minimum
- Assess peroneal tendons during approach
Complications
- Nonunion: 15-25% (higher than TN)
- Sural nerve injury: 5-10%
- Adjacent joint arthritis: 25-35% at 10 years
- Peroneal tendon pathology: 30-40% coexistence
Evidence Base
Epidemiology of Symptomatic Midfoot Osteoarthritis
- Symptomatic radiographic midfoot OA present in 12.0% of community adults aged over 50 years
- Higher in women, those over 75, obesity, prior foot/ankle injury and pain in other weight-loaded joints
- Talonavicular joint included in the validated midfoot OA scoring atlas
- Findings interpreted as consistent with mechanical (load-transmission) pathogenesis
Triple Arthrodesis: Long-Term (25 and 44 Year) Follow-Up
- 67 feet reviewed at average 25 and 44 years after triple arthrodesis
- Pseudarthrosis in 13 feet; residual but non-progressive deformity in 78%
- By second follow-up all ankles showed degenerative change, with naviculocuneiform and TMT progression
- Despite progressive adjacent-joint arthritis, 95% of patients remained satisfied
Simultaneous Calcaneocuboid and Talonavicular (Double) Fusion
- 16 feet followed mean 83 months after combined CC and TN fusion
- 12 of 16 rated excellent or good; only one asymptomatic TN nonunion
- Progressive ankle OA in 6 and naviculocuneiform OA in 7 patients
- Biomechanically superior to isolated TN fusion and a simpler alternative to triple arthrodesis
Displaced Fractures of the Cuboid (Nutcracker Injury)
- Four displaced cuboid fractures treated by open reduction, bone grafting and internal fixation
- ORIF advocated where one or more articular surfaces are appreciably displaced
- Preliminary results better than historical conservative treatment or late midtarsal fusion
- Restoration of cuboid length protects lateral column and the CC joint
Operative vs Nonoperative Treatment of Calcaneal Fractures (RCT)
- 424 patients with 471 displaced intra-articular calcaneal fractures randomized; 309 followed at least 2 years
- No overall difference in SF-36 or VAS between operative and nonoperative care
- After excluding Workers' Compensation cases, selected subgroups did better with ORIF (younger, anatomic reduction, lower workload)
- Anatomic reduction (step-off 2 mm or less) predicted better outcome
Calcaneal Malunion and Nonunion (Review)
- Calcaneal malunion produces heel widening, subfibular impingement, hindfoot varus/valgus and peroneal tendon dysfunction
- Subtalar arthrosis is a well-established consequence; CC immobilisation contributes to the low true nonunion rate
- Reconstruction is a salvage procedure with persistently lower SF-36 and AOFAS hindfoot scores
- Lateral wall decompression suffices only with minimal arthrosis and no deformity
Calcaneocuboid Distraction Arthrodesis vs Osteotomy: Hindfoot Motion
- CT helical-axis motion compared after CC distraction arthrodesis (CCDA) versus anterior calcaneal distraction osteotomy (ACDO)
- Ankle motion 49.0 deg (CCDA) versus 52.2 deg (ACDO); subtalar 24.4 deg versus 22.8 deg
- Differences were small with wide variance between the two lateral column lengthening techniques
- Concern that CCDA reduces hindfoot motion was not borne out in this cohort
Calcaneal Fracture-Dislocation and the Calcaneocuboid Joint
- 10 acute calcaneal fracture-dislocations; the calcaneocuboid joint was involved in 9 of 10
- Often overlooked at presentation; a dislocation approach over fibula to sinus tarsi to CC joint gives access
- After anatomic ORIF, Foot Function Index averaged 12.8 and EQ-5D 0.89 at mean 3 years
- No secondary subtalar fusions were required when recognised and fixed early
References
-
Thomas MJ, Peat G, Rathod T, et al. The epidemiology of symptomatic midfoot osteoarthritis in community-dwelling older adults. Arthritis Res Ther. 2015;17(1):178. PMID 26166410. doi:10.1186/s13075-015-0693-3
-
Saltzman CL, Fehrle MJ, Cooper RR, et al. Triple arthrodesis: twenty-five and forty-four-year average follow-up of the same patients. J Bone Joint Surg Am. 1999;81(10):1391-402. PMID 10535589.
-
Clain MR, Baxter DE. Simultaneous calcaneocuboid and talonavicular fusion: long-term follow-up study. J Bone Joint Surg Br. 1994;76(1):133-6. PMID 8300657.
-
Sangeorzan BJ, Swiontkowski MF. Displaced fractures of the cuboid. J Bone Joint Surg Br. 1990;72(3):376-8. PMID 2341430. doi:10.1302/0301-620X.72B3.2341430
4a. Buckley R, Tough S, McCormack R, et al. Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am. 2002;84(10):1733-44. PMID 12377902. doi:10.2106/00004623-200210000-00001
4b. Reddy V, Fukuda T, Ptaszek AJ. Calcaneus malunion and nonunion. Foot Ankle Clin. 2007;12(1):125-35. PMID 17350514. doi:10.1016/j.fcl.2006.12.004
4c. Beimers L, Louwerens JWK, Tuijthof GJM, et al. CT measurement of range of motion of ankle and subtalar joints following two lateral column lengthening procedures. Foot Ankle Int. 2012;33(5):386-93. PMID 22735280. doi:10.3113/FAI.2012.0386
4d. Rammelt S, Marx C, Swords G, Swords M. Recognition, treatment, and outcome of calcaneal fracture-dislocation. Foot Ankle Int. 2021;42(6):706-13. PMID 33478259. doi:10.1177/1071100720980012
-
Myerson MS. Adult acquired flatfoot deformity: treatment of dysfunction of the posterior tibial tendon. Instr Course Lect. 1997;46:393-405.
-
Johnson JE, Johnson KA. Dowel arthrodesis for degenerative arthritis of the tarsometatarsal (Lisfranc) joints. Foot Ankle. 1986;6(5):243-53.
-
Mann RA, Beaman DN, Horton GA. Isolated subtalar arthrodesis. Foot Ankle Int. 1998;19(8):511-9.
-
Clain MR, Baxter DE. Simultaneous calcaneocuboid and talonavicular fusion: long-term follow-up study. J Bone Joint Surg Br. 1994;76(1):133-6.
-
O'Malley MJ, Deland JT, Lee KT. Selective hindfoot arthrodesis for the treatment of adult acquired flatfoot deformity: an in vitro study. Foot Ankle Int. 1995;16(7):411-7.
-
DiGiovanni CW, Patel A, Calfee R, et al. Osteonecrosis in the foot. J Am Acad Orthop Surg. 2007;15(4):208-17.
-
Beischer AD, Brodsky JW, Pollo FE, et al. Functional outcome and gait analysis after triple or double arthrodesis. Foot Ankle Int. 1999;20(9):545-53.
-
Thordarson DB. Fusion in posttraumatic foot and ankle reconstruction. J Am Acad Orthop Surg. 2004;12(5):322-33.