Arm pain from cervical nerve root compression - C7 most common, 75-90% respond to conservative treatment
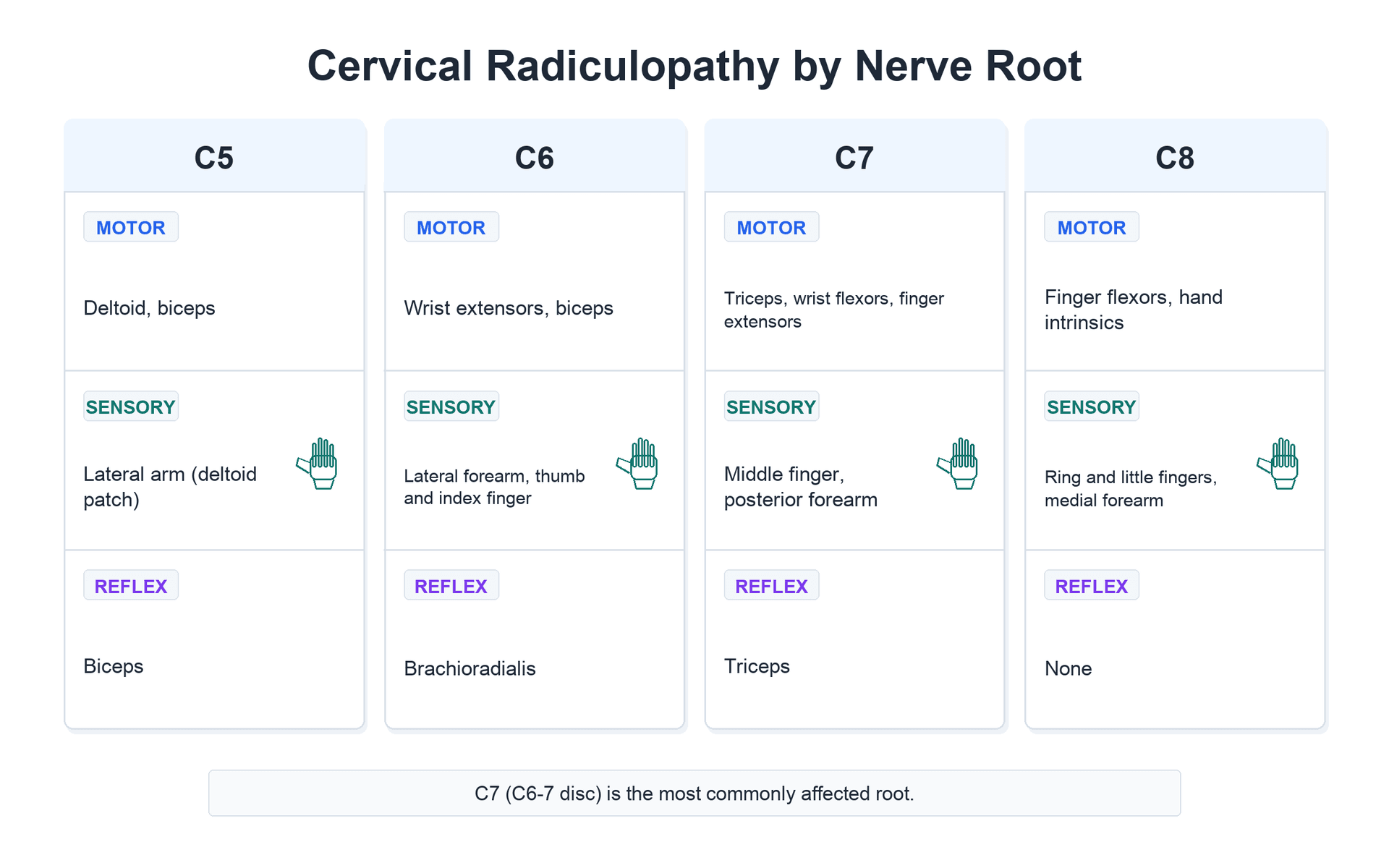
- C7 root most commonly affected (C6-7 disc) - triceps weakness, middle finger numbness
- Arm pain greater than neck pain is hallmark - if neck pain predominates, consider other diagnosis
- Spurling test: axial compression + rotation reproduces radicular symptoms
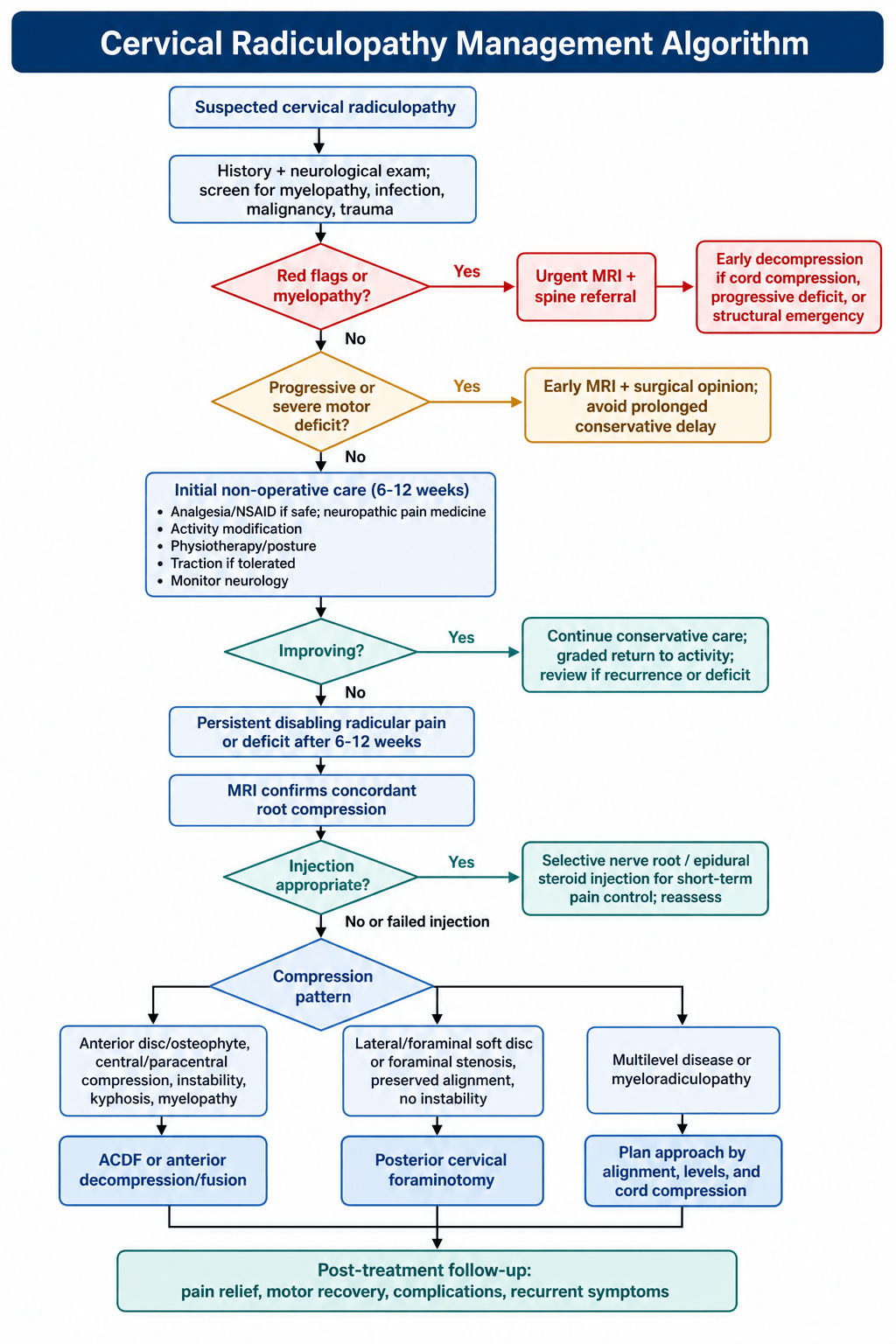
- 75-90% improve with conservative management - trial 6-12 weeks before surgery
- ACDF gold standard surgical treatment with 90-95% success rate
- “Know dermatomal and myotomal patterns for each root cold
- “C5: deltoid/biceps, C6: wrist extensors/brachioradialis, C7: triceps/wrist flexors
- “Progressive motor weakness or myelopathy are surgical indications
- “MRI is gold standard imaging - correlate with clinical findings
Cervical Radiculopathy
Arm Pain greater than Neck Pain: If neck pain predominates, question the diagnosis (think facet/muscular).
Cervical Spine: Root exits above pedicle (C6 disc hits C6 root). Lumbar Spine: Traversing root hit (L4 disc hits L5 root).
C7 Root: Most frequently affected (C6-7 disc). Triceps weakness, middle finger numbness.
Painless Weakness?: Think neurological (ALS) or tendon rupture. Radiculopathy usually HURTS.
Overview and Epidemiology
Cervical radiculopathy results from compression or inflammation of a cervical nerve root, producing a characteristic pattern of pain, sensory changes, and/or motor weakness in the distribution of that nerve root.
Epidemiology
- Value
- 83.2 per 100,000 (Rochester, Minnesota population study)
- Value
- 107.3 per 100,000 (male), 63.5 per 100,000 (female)
- Value
- 50-54 years (202.9 per 100,000); mean onset ~48 years
- Value
- C7, followed by C6
- Value
- C5-6 and C6-7
- Value
- Spondylosis/disc/both in ~68%; confirmed disc protrusion ~22%
- Value
- Only ~15% of cases
- Value
- ~32% over median 4.9-year follow-up
Risk Factors
- Occupational: Heavy manual labour, vibration exposure, prolonged neck flexion
- Smoking (accelerates disc degeneration)
- Diabetes mellitus (peripheral nerve vulnerability)
- Genetic predisposition to disc degeneration
- Prior lumbar radiculopathy (present in ~41% of patients historically)
Pathophysiology
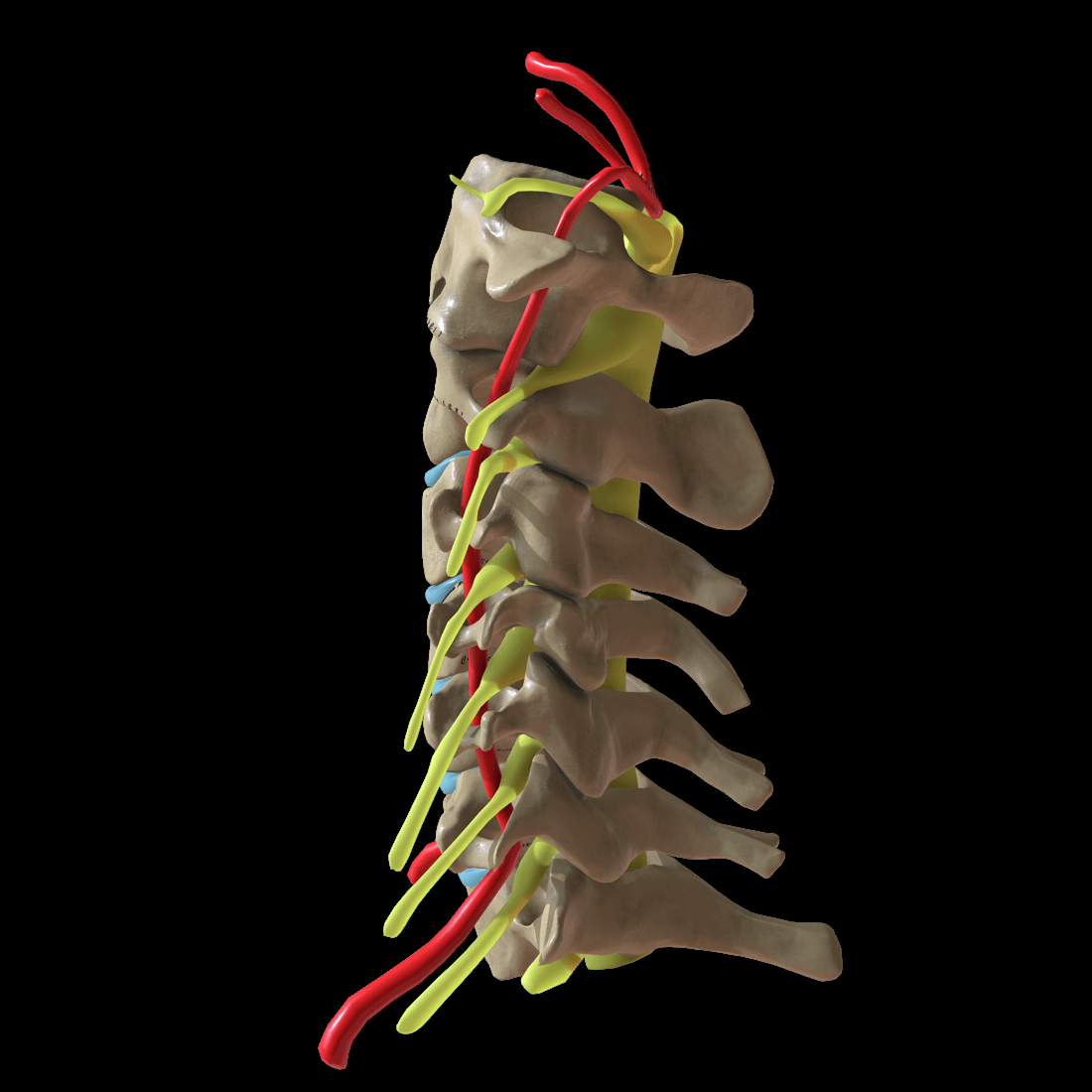
Cervical Nerve Root Anatomy
- Description
- C1-C7 exit ABOVE the corresponding pedicle; C8 exits between C7-T1
- Description
- Anterior: uncovertebral joint; posterior: facet; superior/inferior: pedicles
- Description
- ~9-10mm height, ~4-6mm width
- Description
- Occupies roughly one-third of foramen; remainder is fat and vessels
- Description
- Under 4mm foraminal diameter = high radiculopathy risk
Which Root is Affected?
- C5-6 disc affects C6 nerve root (exits at the level of the disc)
- C6-7 disc affects C7 nerve root
- This differs from the lumbar spine where an L4-5 disc typically affects L5 (the traversing root)
Critical Exam Point: In the cervical spine, the nerve root that exits AT the level of the disc is the root that is compressed. C5-6 disc = C6 root. This is opposite to the lumbar spine convention where the TRAVERSING root (one below) is usually affected.
Mechanisms of Radiculopathy
- Mechanism
- Acute nucleus pulposus herniation
- Features
- Younger patients, sudden onset, often central/centrolateral
- Mechanism
- Disc-osteophyte complex
- Features
- Older patients, insidious, foraminal stenosis
- Mechanism
- Soft + hard components
- Features
- Common presentation
- Mechanism
- Inflammatory mediators (phospholipase A2, TNF-alpha)
- Features
- Pain possible without major mechanical compression
Compression Patterns
- Posterolateral herniation: compresses the exiting nerve root (most common)
- Central herniation: may cause myelopathy
- Foraminal stenosis: chronic compression from uncovertebral/facet osteophytes
Classification
Etiological Classification
- Cause
- Acute herniation
- Age Group
- 20-40 years
- Features
- Sudden onset, may resolve spontaneously
- Cause
- Spondylotic stenosis
- Age Group
- Over 40 years
- Features
- Insidious, progressive, associated cervical spondylosis
- Cause
- Chemical radiculitis
- Age Group
- Any age
- Features
- Pain disproportionate to compression
- Cause
- Fracture, dislocation
- Age Group
- Any age
- Features
- Associated with injury
Clinical Presentation
History
- Characteristics
- Radiates from neck to shoulder, arm, forearm, hand - follows dermatomal pattern
- Characteristics
- Numbness, tingling in specific digits
- Characteristics
- Difficulty with specific motor tasks (grip, lifting)
- Characteristics
- Usually less prominent than arm pain
Key History Questions
- Onset: sudden (soft disc) vs gradual (spondylosis)
- Distribution: specific dermatome vs vague/non-anatomic
- Aggravating factors: extension/rotation (foraminal narrowing)
- Relieving factors: arm elevation (shoulder abduction sign)
- Red flags: myelopathy symptoms, trauma, weight loss, fever
Physical Examination
Dermatomal and Myotomal Patterns
- Sensory Distribution
- Lateral arm (deltoid patch)
- Motor Weakness
- Deltoid, biceps
- Reflex
- Biceps
- Sensory Distribution
- Lateral forearm, thumb, index finger
- Motor Weakness
- Wrist extensors, biceps
- Reflex
- Brachioradialis
- Sensory Distribution
- Middle finger, posterior forearm
- Motor Weakness
- Triceps, wrist flexors, finger extensors
- Reflex
- Triceps
- Sensory Distribution
- Ring and small fingers, medial forearm
- Motor Weakness
- Hand intrinsics, finger flexors
- Reflex
- Finger flexor reflex
- Sensory Distribution
- Medial arm
- Motor Weakness
- Hand intrinsics (abductor pollicis)
- Reflex
- None reliable
Special Tests
- Technique
- Extend, rotate, axially compress neck
- Positive Finding
- Reproduction of radicular arm pain
- Interpretation
- High specificity, moderate sensitivity
- Technique
- Patient places hand on head
- Positive Finding
- Relief of arm pain
- Interpretation
- Suggests radiculopathy (opens foramen)
- Technique
- Axial traction on head
- Positive Finding
- Relief of symptoms
- Interpretation
- Suggests foraminal compression
- Technique
- Bear down/cough
- Positive Finding
- Increased radicular pain
- Interpretation
- Suggests disc herniation
SPURLINGSPURLING Test
Hook:Spurling is SPURRING on the nerve!
Myelopathy Red Flags
Always screen for concurrent myelopathy:
- Hoffman sign (finger flicking causes thumb flexion)
- Ankle clonus
- Lower limb hyperreflexia
- Babinski sign
- Gait disturbance (broad-based, spastic)
- Hand clumsiness (fine motor dysfunction)
Provocative Test Accuracy and the Wainner Cluster
No single provocative test is diagnostic; combining them is far more powerful. Individually, the Spurling test has high specificity (around 90 percent) but low-to-moderate sensitivity, so it rules radiculopathy IN but cannot rule it out, whereas the upper limb tension test (ULTT-A, median-biased) is highly sensitive but not specific, so a negative ULTT-A helps rule radiculopathy OUT.
Wainner described a four-test clinical prediction rule for cervical radiculopathy:
- Positive finding
- Reproduction of radicular arm symptoms
- Property
- High specificity (rule-in)
- Positive finding
- Relief of radicular symptoms with traction
- Property
- Rule-in when positive
- Positive finding
- Less than 60 degrees to the affected side
- Property
- Reduced motion supports the diagnosis
- Positive finding
- Symptom reproduction with a side-to-side difference
- Property
- High sensitivity (rule-out)
When 3 of the 4 tests are positive the likelihood ratio for cervical radiculopathy is roughly 6 (post-test probability about 65 percent); with all 4 positive the likelihood ratio rises to roughly 30 (post-test probability about 90 percent). The ULTT-A is the upper-limb analogue of the straight-leg raise: scapular depression, shoulder abduction, forearm supination with wrist and finger extension, shoulder external rotation and elbow extension, sensitised by contralateral neck side-bending.
Spurling is specific (rule-in) but insensitive; the median-biased upper limb tension test is sensitive (rule-out). Wainner's cluster of Spurling, distraction, ipsilateral rotation under 60 degrees and a positive ULTT-A gives a likelihood ratio around 30 when all four are positive.
Investigations
Imaging Algorithm
- Investigation
- Plain X-rays
- Indication
- First-line, exclude instability, assess alignment
- Investigation
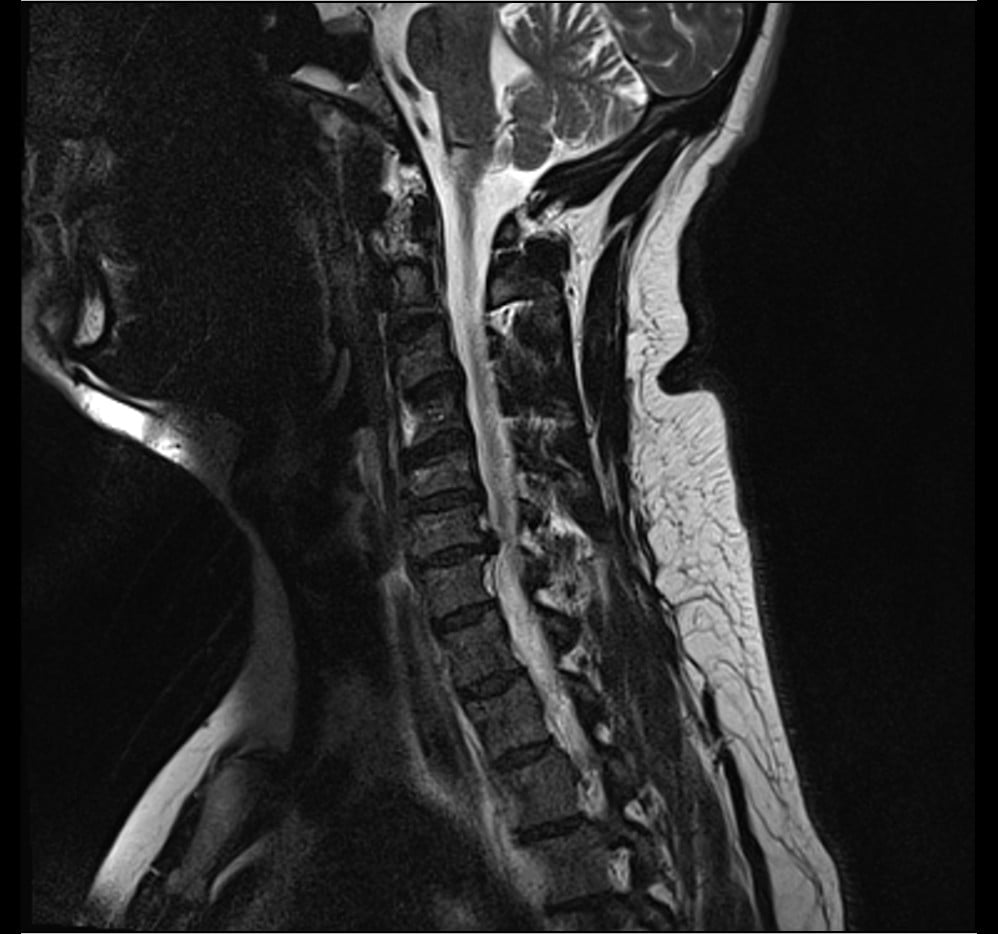
- MRI
- Indication
- Neurological symptoms, radiculopathy suspected
- Investigation
- CT
- Indication
- Osseous detail, surgical planning, MRI contraindicated
- Investigation
- CT myelogram
- Indication
- MRI contraindicated, dynamic assessment
Plain Radiographs
Key Findings: disc space narrowing, foraminal stenosis on oblique views, uncovertebral joint hypertrophy, facet arthropathy, loss of lordosis/kyphosis.
- Normal
- 9-10mm
- Abnormal
- Under 4mm = stenosis
- Normal
- 4-6mm
- Abnormal
- Under 3mm = degeneration
- Normal
- 17-18mm
- Abnormal
- Under 13mm = stenosis
MRI Findings
- Description
- Concentric expansion beyond margins
- Significance
- Common, often asymptomatic
- Description
- Focal bulge, base wider than apex
- Significance
- May cause compression
- Description
- Apex wider than base
- Significance
- Usually symptomatic
- Description
- Fragment separated from parent disc
- Significance
- May migrate, often needs surgery
- Description
- Loss of perineural fat on T1
- Significance
- Direct nerve compression
- Description
- T2 hyperintensity
- Significance
- Myelomalacia if present
MRI Interpretation: On T2-weighted sagittal images, look for "loss of CSF signal" around the cord (effacement). On axial images, assess foraminal fat signal loss on T1 and nerve root compression. Asymptomatic disc abnormalities are common, so always correlate imaging with the clinical level.
Electrodiagnostic Studies
- EMG/NCS may help localise the affected root level
- Denervation changes appear in affected muscles roughly 3+ weeks after onset
- Useful for differentiating radiculopathy from peripheral neuropathy
- Not routine, but valuable in atypical or multilevel presentations
Imaging Atlas

Differential Diagnosis
- Distinguishing Features
- Long tract signs, gait disturbance, bilateral symptoms
- Investigation
- MRI shows cord compression/signal
- Distinguishing Features
- Multiple root pattern, may follow viral illness
- Investigation
- EMG/NCS, MRI of plexus
- Distinguishing Features
- Vascular symptoms, provocation with arm positions
- Investigation
- Doppler, nerve conduction studies
- Distinguishing Features
- Distal to root, Tinel positive at compression site
- Investigation
- EMG/NCS localizes to peripheral nerve
- Distinguishing Features
- Shoulder ROM limited, rotator cuff signs
- Investigation
- Shoulder X-ray, MRI, impingement tests
- Distinguishing Features
- Exertional, risk factors, associated symptoms
- Investigation
- ECG, cardiac enzymes
- Distinguishing Features
- Horner syndrome, severe pain, T1 involvement
- Investigation
- CXR, CT chest
- Distinguishing Features
- Diffuse pain, tender points, no neurological deficit
- Investigation
- Normal investigations, clinical diagnosis
ROOTS vs CORDRadiculopathy vs Myelopathy
Hook:ROOTS for radiculopathy, CORD for myelopathy!
The Double Crush Phenomenon
Cervical radiculopathy and a distal peripheral nerve entrapment can coexist and interact. The double crush phenomenon (Upton and McComas, 1973) proposes that a proximal compression of a nerve - for example a cervical root - impairs axoplasmic transport and renders the same axons more vulnerable to a second, more distal compression, such as carpal tunnel or cubital tunnel syndrome. Each lesion may be individually subclinical yet symptomatic in combination.
- Implication
- Symptoms may not fully fit a single root or single peripheral nerve
- Implication
- Consider an unaddressed second site
- Implication
- A distal lesion can sensitise the nerve to a proximal one
- Implication
- Careful examination plus EMG/NCS to localise both levels
Clinically, suspect double crush when the pattern is atypical, when EMG shows changes at more than one level, or when symptoms persist after treating only one site. Both sites may need to be addressed, and the more symptomatic or clearly compressive lesion is usually treated first.
The double crush phenomenon explains why a cervical root compression and a distal entrapment (carpal or cubital tunnel) can coexist and reinforce each other through impaired axoplasmic flow. Persisting symptoms after decompressing one site should prompt a search for the second.
Management
Complications
Conservative Treatment Complications
- Cause
- Inadequate treatment
- Prevention/Management
- Multimodal approach
- Cause
- Prolonged use
- Prevention/Management
- PPI cover, limit duration
- Cause
- Natural history
- Prevention/Management
- Monitor closely, early surgery if progressive
- Cause
- ESI complication
- Prevention/Management
- Fluoroscopic guidance, interlaminar approach
Surgical Complications
- Rate
- 20-50% transient, 1-2% persistent
- Management
- Usually resolves over 2-4 weeks, soft diet
- Rate
- 1-2%
- Management
- Speech therapy, often recovers
- Rate
- Under 0.5%
- Management
- Primary repair if recognised, NPO
- Rate
- 0.5-1%
- Management
- Primary repair, fibrin glue, lumbar drain
- Rate
- Under 0.5%
- Management
- Avoid lateral dissection, careful burr technique
- Rate
- 3-10%
- Management
- CT assessment, revision if symptomatic
- Rate
- ~2.9% per year (cumulative)
- Management
- Surveillance, may require extension of fusion
- Rate
- 1-5% (higher posterior)
- Management
- Usually transient, recovers over ~6 months
ACDFACDF Complications
Hook:The procedure name lists the complications!
Postoperative Care
ACDF Protocol
Immediate (Day 0-2): airway monitoring (hematoma risk), swallow assessment before diet, early mobilization, soft collar if needed (not mandatory), DVT prophylaxis.
Early (Weeks 1-6): wound check at 2 weeks, soft diet if dysphagia, cervical precautions (no heavy lifting), gentle ROM from week 2, return to sedentary work 2-4 weeks.
Intermediate (Weeks 6-12): X-rays at 6 weeks, begin physiotherapy, gradual return to activities, return to manual work typically 8-12 weeks.
Late (3-12 months): fusion assessment (CT if concern), full activity by 3-6 months, monitor for adjacent segment disease.
Expected Recovery
- Milestone
- Mobilizing, oral intake
- Milestone
- Return to light activities
- Milestone
- Driving resume
- Milestone
- Return to work (most occupations)
- Milestone
- Full recovery expected
Guidelines, Registries & Global Practice
Global Epidemiology
Population-based data (Rochester, Minnesota) give an age-adjusted annual incidence of ~83 per 100,000, peaking at ~203 per 100,000 in the 50-54 year age band, with C7 the most commonly affected root. The natural history is favourable: ~90% of patients are asymptomatic or only mildly affected at long-term follow-up.
Side-by-Side Society Guidance
- Key Recommendation
- MRI is the imaging modality of choice; a trial of conservative care is appropriate before surgery in patients without progressive deficit
- Key Recommendation
- Multimodal non-operative care first-line; surgery reserved for progressive deficit, myelopathy, or failed conservative management
- Key Recommendation
- Emphasise early reassurance, activity, and physiotherapy; image only when management would change or red flags are present
- Key Recommendation
- ACDF remains the benchmark; arthroplasty for selected single/two-level disc disease; posterior foraminotomy for lateral soft disc
Registry and Trial Evidence
- Randomized data (Engquist, Spine 2013) show surgery accelerates recovery but the advantage over structured physiotherapy narrows by 2 years - supporting an initial conservative trial in non-progressive cases.
- For lateral soft-disc pathology, motion-preserving posterior foraminotomy is equivalent to ACDF at 2 years (Ruetten, Spine 2008).
- Cervical disc arthroplasty preserves index-level motion with comparable or better outcomes than ACDF at 2 years in selected single-level disease (Heller/BRYAN, Spine 2009); arthroplasty registries and IDE data show lower reoperation for adjacent-level disease at longer follow-up.
High- vs Limited-Resource Variation
- Practice Pattern
- Early MRI access, arthroplasty and navigation available, faster pathway to elective surgery
- Practice Pattern
- Greater reliance on clinical diagnosis and plain radiographs; ACDF favoured over arthroplasty on cost grounds; longer waits for elective decompression
MCQ Practice Points
High-Yield Concepts
- C7 is the most commonly affected root, typically from the C6-7 disc level
- Cervical roots exit ABOVE their corresponding vertebra (unlike the lumbar spine)
- Spurling test: high specificity, moderate sensitivity
- Arm pain greater than neck pain is the classic radiculopathy pattern
- 75-90% improve with conservative management - trial for 6-12 weeks
- Progressive motor weakness is an indication for urgent surgery
- ACDF vs foraminotomy: ACDF for central disc, foraminotomy for lateral soft disc
- Dysphagia is the most common ACDF complication (usually transient)
Common Examination Pitfalls
- Missing myelopathy signs in a radiculopathy patient
- Attributing symptoms to the wrong root level
- Not checking reflexes systematically
- Forgetting that C8 exits between C7 and T1
- Overlooking progressive weakness as a surgical emergency
- Not differentiating from peripheral entrapment
Q: Which cervical nerve root is most commonly affected by radiculopathy and what is the typical disc level?
A: C7 root from a C6-7 disc herniation. Cervical roots exit ABOVE their corresponding vertebra (unlike the lumbar spine). The C7 root exits between C6 and C7, so a C6-7 disc herniation affects C7.
Q: How do you differentiate C6 vs C7 radiculopathy on clinical examination?
A: C6 radiculopathy: weakness of biceps and wrist extension, diminished biceps and brachioradialis reflexes, sensory loss in thumb and lateral forearm. C7 radiculopathy: weakness of triceps and wrist flexion, diminished triceps reflex, sensory loss in the middle finger.
Q: How should the Spurling test be interpreted?
A: It has high specificity but only moderate sensitivity. A positive test (reproduction of radicular symptoms with extension, lateral flexion, and axial compression) strongly supports radiculopathy, but a negative test does not rule it out.
Q: What are the surgical indications for cervical radiculopathy and which procedure is most appropriate?
A: Urgent surgery: progressive motor weakness or myelopathy signs. Elective surgery: failed 6-12 weeks of conservative management with persistent symptoms. Procedure choice: ACDF for central/paracentral disc or with axial neck pain; posterior foraminotomy for lateral soft disc without instability.
At a Glance
- Key Information
- Nerve root dysfunction from compression/inflammation
- Key Information
- 50-54 years (peak incidence band)
- Key Information
- C7, then C6
- Key Information
- C5-6 and C6-7 discs
- Key Information
- Arm pain greater than neck pain
- Key Information
- Spurling test (high specificity)
- Key Information
- X-ray then MRI if neurological symptoms
- Key Information
- 75-90%
- Key Information
- Progressive weakness, refractory to 6-12 weeks conservative care
C5678Cervical Root Patterns
Hook:Count backwards for muscle strength!
Exam Day Cheat Sheet
Key Diagnosis Facts
- **Definition**: Nerve root dysfunction from compression/inflammation
- **Most common root**: C7, then C6, from the C6-7 and C5-6 levels
- **Classic pattern**: Arm pain greater than neck pain in a dermatomal distribution
Level Specifics
- **C6 pattern**: Thumb/index numbness, wrist extension weakness, brachioradialis reflex
- **C7 pattern**: Middle finger numbness, triceps weakness, triceps reflex
Management & Outcome
- **Key test**: Spurling - extension + rotation + axial load, high specificity
- **Conservative success**: 75-90% improve in 6-12 weeks
- **Surgery indication**: Progressive weakness, refractory at 6-12 weeks, severe deficit
- **ACDF success**: 90-95% for radiculopathy
- **Main complication**: Dysphagia (20-50% transient)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old office worker presents with 4 weeks of right arm pain radiating from the neck to the thumb and index finger. He has numbness in these digits and weakness of wrist extension. Examination shows reduced brachioradialis reflex.”
“A 52-year-old presents with 3 weeks of left arm pain and progressive weakness. Initially had grip weakness but now cannot lift her arm against gravity. MRI shows large C6-7 disc extrusion with severe C7 root compression.”
“A 60-year-old man has bilateral arm symptoms with C5-6 and C6-7 disc disease on MRI. He has C6 and C7 dermatomal symptoms, mild weakness of right triceps, and subtle hyperreflexia in the legs.”
Evidence Base & Outcomes
Epidemiology of Cervical Radiculopathy (Landmark Population Study)
- Population-based survey, Rochester Minnesota 1976-1990, 561 patients
- Age-adjusted annual incidence 83.2 per 100,000; peak 202.9 per 100,000 at age 50-54
- C7 monoradiculopathy most frequent, followed by C6
- Disc/spondylosis cause in ~68%; confirmed disc protrusion in ~22%
- At final follow-up 90% asymptomatic or only mildly incapacitated; recurrence ~32%
Cervical Collar or Physiotherapy vs Wait-and-See (Landmark Conservative RCT)
- RCT of 205 patients with recent-onset cervical radiculopathy (under 1 month)
- Semi-hard collar with rest or physiotherapy vs wait-and-see
- Both active treatments gave significant additional arm and neck pain reduction at 6 weeks
- Wait-and-see group still improved (arm pain fell ~19 mm over 6 weeks)
- Supports a short course of collar or physiotherapy early in the disease
Surgery (ACDF) plus Physiotherapy vs Physiotherapy Alone (Landmark Surgical RCT)
- Prospective RCT, 63 patients with cervical radiculopathy, 2-year follow-up
- ACDF plus physiotherapy vs structured physiotherapy alone
- Surgery gave faster improvement and better neck pain/global outcome at 12 months
- At 24 months between-group differences largely disappeared
- Authors conclude structured physiotherapy should be tried before surgery
References
- Radhakrishnan K, Litchy WJ, O'Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy: a population-based study from Rochester, Minnesota, 1976 through 1990. Brain 1994;117:325-35. PMID 8186959.
- Kuijper B, Tans JTJ, Beelen A, Nollet F, de Visser M. Cervical collar or physiotherapy versus wait and see policy for recent onset cervical radiculopathy: randomised trial. BMJ 2009;339:b3883. PMID 19812130.
- Engquist M, Lofgren H, Oberg B, et al. Surgery versus nonsurgical treatment of cervical radiculopathy: a prospective, randomized study. Spine 2013;38:1715-22. PMID 23778373.
- Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic cervical posterior foraminotomy for lateral disc herniations: a prospective, randomized, controlled study. Spine 2008;33:940-8. PMID 18427313.
- Heller JG, Sasso RC, Papadopoulos SM, et al. Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: a randomized, controlled trial. Spine 2009;34:101-7. PMID 19112337.
- Diwan S, Manchikanti L, Benyamin RM, et al. Effectiveness of cervical epidural injections in the management of chronic neck and upper extremity pain. Pain Physician 2012;15:E405-34. PMID 22828692.