Midtarsal Joint | Talonavicular and Calcaneocuboid
- Definition: Injury to the midtarsal (Chopart) joint - Talonavicular (TN) and Calcaneocuboid (CC).
- Importance: Critical for foot flexibility. Missed injury leads to painful arthrosis and flatfoot.
- Mechanism: High-energy (MVA, fall). Forced abduction or adduction of forefoot.
- Treatment: Anatomic reduction essential. ORIF usually required. May need fusion if arthritic.
- Nutcracker: Lateral column compression. Cuboid crushed. Bone graft to restore length.
- “Chopart joint is the 'transverse tarsal joint' - key for midfoot motion.
- “Talonavicular is the 'keystone' of the medial longitudinal arch.
- “Nutcracker fracture = Cuboid compression. Restore lateral column length.
- “Think of Chopart any time there is significant midfoot swelling/injury.
High Index of Suspicion. Midfoot injuries are often missed. Look for widening, subluxation on X-ray/CT.
Nutcracker Cuboid. Crushed cuboid shortens lateral column. Must bone graft to restore length.
Foot Compartments. High-energy Chopart injuries can cause foot compartment syndrome. Monitor and release if needed.
Common Outcome. Even with good reduction, arthrosis is common. May need fusion.
- Chopart (Midtarsal)
- TN + CC
- Lisfranc (Tarsometatarsal)
- TMT 1-5
- Chopart (Midtarsal)
- Midfoot (Transverse Tarsal)
- Lisfranc (Tarsometatarsal)
- Midfoot (Forefoot base)
- Chopart (Midtarsal)
- Talonavicular
- Lisfranc (Tarsometatarsal)
- 2nd TMT
- Chopart (Midtarsal)
- Foot Flexibility/Adaptation
- Lisfranc (Tarsometatarsal)
- Rigid Lever for Push-off
- Chopart (Midtarsal)
- ORIF +/- Fusion
- Lisfranc (Tarsometatarsal)
- ORIF or Primary Fusion
CRUNCHNutcracker Fracture
Hook:Nutcracker Cuboid.
FLEXChopart Significance
Hook:Chopart = Foot Flexibility.
Overview and Epidemiology
Chopart joint (Midtarsal joint) injuries involve the Talonavicular (TN) and/or Calcaneocuboid (CC) joints. The Chopart joint is the boundary between the hindfoot and midfoot and is critical for foot flexibility.
Named after François Chopart (1743-1795), a French surgeon who described amputation through this joint.
- Rare: Less common than Lisfranc injuries.
- Mechanism: High-energy (MVA, motorcycle, fall from height). Occasionally low-energy (twisting).
- Pattern: Often associated with other foot injuries.
Anatomy and Pathophysiology
- Talonavicular Joint: Ball-and-socket joint. Key for inversion/eversion. Keystone of medial longitudinal arch.
- Calcaneocuboid Joint: Saddle-shaped. Less mobile. Part of lateral column.
- Ligaments: Spring Ligament (plantar calcaneonavicular), Bifurcate ligament (calcaneonavicular + calcaneocuboid), Interosseous ligaments.
- Transverse Tarsal Joint: TN + CC together. Allows midfoot motion.
- Foot Flexibility: When subtalar joint is everted, TN and CC axes are parallel, allowing flexibility. When inverted, axes diverge, creating rigidity.
- Forced Abduction/Adduction: Forefoot forced laterally or medially on fixed hindfoot.
- Axial Load: Direct force through midfoot.
- Nutcracker: Forced plantarflexion compresses cuboid between 4th/5th metatarsals and calcaneus.
Classification
Main Classification
- Injury
- TN Disruption
- Key Feature
- Navicular fracture, TN subluxation
- Injury
- Combined
- Key Feature
- TN + CC disruption
- Injury
- CC Disruption
- Key Feature
- Cuboid fracture, CC subluxation
- Injury
- Nutcracker
- Key Feature
- Cuboid compression
- Injury
- Comminuted
- Key Feature
- High-energy, multiple fragments
Often combined patterns. High-energy.
Clinical Assessment
- Mechanism: MVA? Fall? Twisting?
- Pain Location: Dorsal midfoot. Worse with walking.
- Swelling: Significant midfoot swelling.
- Tenderness: Over TN and/or CC joints.
- Deformity: May have visible abduction or adduction deformity.
- ROM: Painful midfoot motion.
- Neurovascular: Check pulses and sensation.
- Compartments: Monitor for foot compartment syndrome (especially with crush/high-energy).
Investigations
- X-ray (Foot - AP, Oblique, Lateral): Look for joint widening, subluxation, fractures.
- Weight-Bearing X-rays: If patient can tolerate. Better for subtle instability.
- CT Scan: Essential for surgical planning. Assess comminution, joint congruity.
- MRI: Rarely needed acutely. For ligamentous assessment if occult injury.
- TN Gap: Widening or incongruity of Talonavicular joint.
- CC Subluxation: Malalignment of Calcaneocuboid joint.
- Cuboid Compression: Loss of cuboid height (Nutcracker).
- Lateral Column Shortening: Compare to contralateral.



Assessing & Restoring Lateral Column Length
"Restore lateral column length" is the recurring goal of nutcracker repair throughout this topic, and a viva will ask how you actually assess it — so the method is worth setting out.
Why it matters. The lateral column (calcaneus → cuboid → 4th/5th metatarsals) must keep its length for a balanced foot. Shortening — typically from a crushed (nutcracker) cuboid — pulls the forefoot into a fixed abductus, overloads the lateral border, and drives painful gait and calcaneocuboid/midfoot arthrosis. Restoring length is therefore the central operative goal.
How to assess it:
- Compare with the contralateral (uninjured) foot. Side-by-side standing AP and lateral radiographs are the most practical reference for the patient's own normal length.
- Radiographic alignment. On the AP view the lateral column (calcaneus–cuboid–4th/5th metatarsals) should form a smooth, continuous line; loss of cuboid length and a forefoot that deviates laterally (abductus) signal shortening. Look for loss of cuboid height on the lateral/oblique view.
- Intra-operatively. Use fluoroscopic comparison with the normal side, and directly measure restored length after elevating the impacted articular surface; a lamina spreader, distractor or temporary external fixator regains and holds length before grafting and plate fixation.
The take-home: do not simply fix the cuboid — measure and restore its length against the other foot, because residual lateral column shortening leaves a fixed forefoot abductus and a poor result.
Assess lateral column length by comparing standing radiographs with the contralateral foot (the calcaneus–cuboid–4th/5th-metatarsal line should be smooth and continuous) and by intra-operative fluoroscopy and direct measurement after distracting and grafting the cuboid. Residual shortening leaves a fixed forefoot abductus, lateral overload and arthrosis — so restoring length (structural graft, with a lamina spreader / external-fixator distraction) is the core goal of nutcracker repair.
Differential Diagnosis
- Key Discriminators
- Midfoot swelling, TN/CC tenderness, joint widening or column shortening
- Confirming Test
- CT of the foot
- Key Discriminators
- Tenderness/gap at TMT bases, fleck sign, plantar ecchymosis
- Confirming Test
- Weight-bearing or stress radiographs, CT
- Key Discriminators
- Insidious dorsal midfoot pain in an athlete, no acute deformity
- Confirming Test
- MRI or CT (the 'N spot')
- Key Discriminators
- Lateral midfoot tenderness without medial column injury
- Confirming Test
- CT; assess lateral column length
- Key Discriminators
- Localised tenderness, no widening or subluxation on weight-bearing films
- Confirming Test
- Weight-bearing radiographs (stable)
Management Algorithm
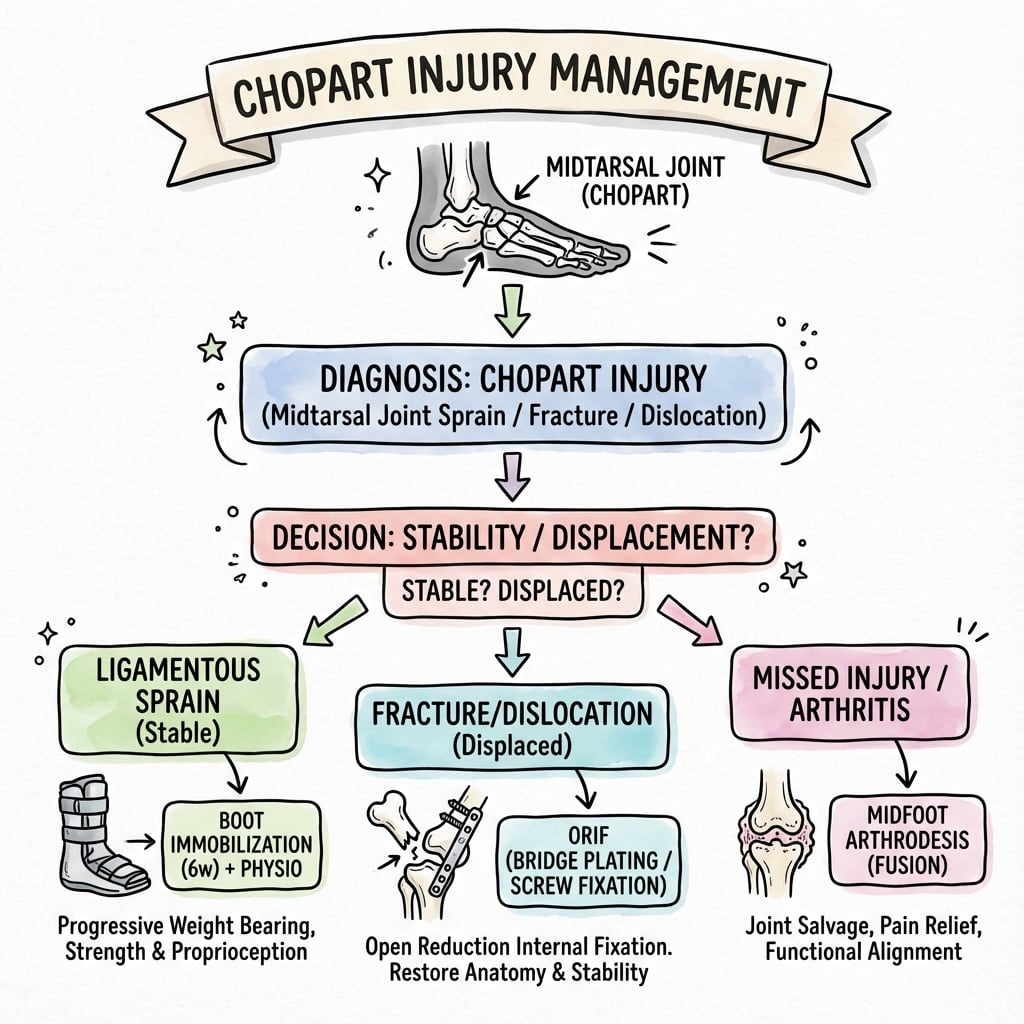
Non-Operative (Rare)
Only for Truly Stable, Non-Displaced Injuries.
- Criteria: Anatomic alignment. No subluxation. Weight-bearing X-ray stable.
- Immobilization: NWB Cast/Boot 6-8 weeks.
- Transition: PWB then FWB as tolerated.
- Follow-up: Serial X-rays to confirm no displacement.
Most Chopart injuries need surgery.
Surgical Technique
Talonavicular ORIF
- Approach: Dorsomedial incision over TN joint.
- Reduction: Reduce TN joint. Joystick with K-wire in navicular.
- Fixation:
- Screws (3.5mm Cortical or Headless) across TN.
- Bridge plate if comminuted.
- Assess Spring Ligament: Repair if disrupted.
- Closure: Layered.
TN is the key joint - must be anatomic.
Complications
- Risk Factor
- Cartilage damage
- Management
- Fusion (TN and/or CC)
- Risk Factor
- Inadequate reduction
- Management
- Osteotomy / Lengthening
- Risk Factor
- High-energy
- Management
- Fasciotomy
- Risk Factor
- Prolonged immobilization
- Management
- Physiotherapy
- Risk Factor
- Swelling
- Management
- Staged surgery if needed
Postoperative Care
- NWB: 6-12 weeks (depending on fixation stability and healing).
- Cast/Boot: Initially NWB cast, then transition to boot.
- ROM: Gentle ROM when fixation secure.
- Weight-Bearing: Progress PWB to FWB at 8-12 weeks.
- Physiotherapy: After healing. Gait training. Strengthening.
Outcomes
- Good Reduction: Better long-term outcomes.
- Post-Traumatic Arthrosis: Common even with anatomic reduction. May need fusion.
- Lateral Column Length: Critical. Shortening leads to painful abductus.
Guidelines, Registries & Global Practice
Global epidemiology
- Chopart injuries are rare, accounting for roughly 0.2 percent of all dislocations; midfoot fracture-dislocations are around five to ten times less common than Lisfranc injuries.
- Most series report a male predominance with a peak in young to middle-aged adults; high-energy mechanisms (road traffic, fall from height, crush) dominate, though a low-energy "twisting" subset exists in athletes.
- Up to a quarter present as combined Chopart-Lisfranc patterns, which carry the worst functional scores.
Side-by-side guidance
- Position on midtarsal injuries
- CT for all suspected midtarsal injuries; anatomic restoration of the medial (TN) and lateral (CC/cuboid) columns; bridge plating or temporary spanning fixation for comminution
- Position on midtarsal injuries
- Early ORIF for displaced fracture-dislocations; column-length restoration with structural graft for nutcracker cuboid; primary fusion reserved for non-reconstructable joints
- Position on midtarsal injuries
- Soft-tissue-led timing, senior decision-making, early CT, and transfer of complex foot trauma to a specialist centre
- Position on midtarsal injuries
- Reflects the Hannover (Richter) evidence: open anatomic reduction superior to closed for fracture-dislocations
Registry and evidence notes
- No dedicated national registry tracks Chopart injuries (they are not implant-arthroplasty procedures); the evidence base is single-centre series and small cohorts, so guidance is consensus- and principle-driven rather than registry-derived.
High- vs limited-resource practice variation
- Well-resourced settings: routine CT, dedicated foot-and-ankle plating systems, cuboid-specific plates, and staged soft-tissue management.
- Limited-resource settings: reliance on plain radiographs and intra-operative fluoroscopy, K-wire and external-fixator constructs to hold column length, and a lower threshold for primary fusion when implants or follow-up are constrained.
Controversies & Areas of Uncertainty
- Primary fusion vs ORIF: For severely comminuted, non-reconstructable Chopart joints (especially the talonavicular keystone), the threshold for primary arthrodesis versus attempted reconstruction is debated; no randomised data exist.
- Spanning (bridge) plate vs internal fixation: Whether to span the midtarsal joint with a temporary bridge plate or external fixator versus rigid internal fixation, and when to remove spanning hardware, remains practice-dependent.
- Nutcracker graft choice: Structural autograft (iliac crest), allograft, and synthetic wedges are all used to restore lateral column length; comparative outcome data are lacking.
- Closed reduction in pure dislocations: Richter's data support closed reduction only when truly anatomic; the durability of this approach versus routine open confirmation is uncertain.
- Weight-bearing protocol: Optimal duration of non-weight-bearing (6 vs 12 weeks) and timing of hardware removal are not standardised.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your diagnosis and management plan?”
“Explain the key differences.”
“Explain the Nutcracker mechanism.”
MCQ Practice Points
Q: Which joints make up the Chopart (Midtarsal) joint? A: Talonavicular (TN) and Calcaneocuboid (CC).
Q: What is the keystone of the medial longitudinal arch? A: The Talonavicular joint.
Q: What is a Nutcracker fracture? A: Compression fracture of the cuboid, 'nutcracked' between the bases of the 4th/5th metatarsals and the calcaneus.
Q: What is the treatment for Nutcracker fracture? A: ORIF with bone graft to restore lateral column length.
Q: What is the function of the Chopart joint? A: Allows foot flexibility and adaptation to uneven terrain.
Anatomy
- Chopart: TN + CC
- TN: Ball-Socket
- CC: Saddle
- Keystone: TN
Nutcracker
- Cuboid compressed
- Between MT bases + Calc
- Lateral column short
- Bone graft to restore
Treatment
- ORIF standard
- Anatomic reduction
- NWB 8-12 weeks
- Fusion for arthrosis
Pitfalls
- Missed injury
- Compartment syndrome
- Lateral column length
- Post-traumatic arthrosis
Evidence Base
Richter — Open vs Closed Reduction of Chopart Injuries (Landmark)
- 110 Chopart dislocations/fracture-dislocations; 65 followed for a mean of 9 years (range 2-25).
- 25% pure dislocations, 55% fracture-dislocations, 20% combined Chopart-Lisfranc; mean AOFAS midfoot 75.
- Combined Chopart-Lisfranc injuries scored significantly lower than isolated Chopart injuries.
- Initial anatomic reduction was essential for good results; open reduction outperformed closed reduction, especially in fracture-dislocations.
Sangeorzan — Navicular Fracture Classification (Classic)
- 21 displaced tarsal navicular body fractures treated with ORIF; introduced the three-type classification by fracture-line plane and foot displacement.
- Type 1 coronal (no forefoot angulation); Type 2 dorsolateral-to-plantar-medial (forefoot displaced medially); Type 3 comminuted sagittal (forefoot displaced laterally).
- Good results in 67%; both fracture type and accuracy of reduction correlated directly with outcome.
Hermel & Gershon-Cohen — Original Nutcracker Description
- First description of the cuboid 'nutcracker' fracture by indirect violence.
- Cuboid is crushed between the bases of the 4th/5th metatarsals distally and the anterior calcaneus proximally.
- Mechanism produces lateral column shortening.
Engelmann — Cuboid ORIF: Restoring Column Length
- 45 surgically managed cuboid fractures at a level 1 centre; median follow-up 67 months.
- Median AOFAS midfoot 76 (range 34-100); no infections or nonunions; secondary CC fusion in only 2 patients.
- Cuboid plate fixation was independently associated with better AOFAS scores.
van der Vliet — Functional Outcomes of Midfoot Injuries
- 40 patients (45 Lisfranc and/or Chopart injuries) after ORIF; median AOFAS midfoot 64.
- Secondary arthrodesis required in 7 of 45 injuries; higher injury severity predicted worse function.
- EQ-5D quality of life was significantly below the reference population.
Myerson & Manoli — Foot Compartment Syndrome
- Approximately 10% of calcaneal/high-energy foot injuries develop foot compartment syndrome.
- Half of those develop claw toes, stiffness or neurovascular dysfunction; calcaneal-compartment pressures confirm the diagnosis.
- Immediate fasciotomy is recommended, with delayed definitive fixation after wound closure.