ATFL Primary | CFL Secondary | Mechanical + Functional
- ATFL is weakest and most commonly injured lateral ligament
- CFL is EXTRA-ARTICULAR - injured with increasing inversion force
- Anterior drawer tests ATFL; Talar tilt tests CFL
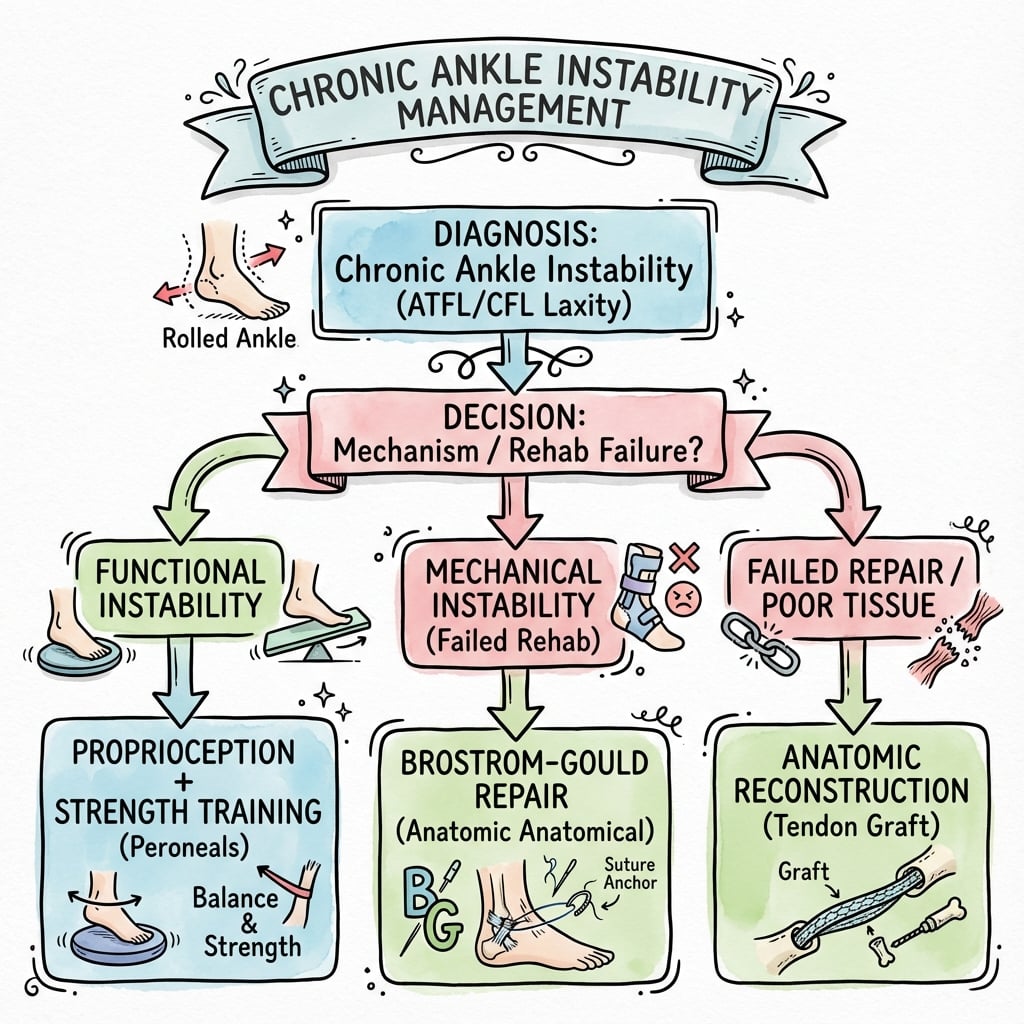
- Conservative treatment fails in 20-40% of patients
- Brostrom-Gould is gold standard surgical treatment
- “ATFL: resists anterolateral translation in plantarflexion
- “CFL: resists inversion throughout ROM (crosses subtalar joint)
- “Functional instability = proprioceptive deficit, peroneal weakness
- “Always exclude subtalar instability and OLT
ATFL (anterior talofibular): weakest lateral ligament, taut in plantarflexion, resists anterior translation. CFL (calcaneofibular): extra-articular, taut in dorsiflexion, crosses subtalar joint. PTFL: rarely injured, strongest lateral ligament.
Mechanical instability = true laxity (positive anterior drawer greater than 10mm, talar tilt greater than 10 degrees). Functional instability = giving way without laxity (proprioceptive deficit, peroneal weakness). Both types can coexist.
Anterior drawer (ATFL): 90 degrees knee flexion, ankle neutral, translate talus anteriorly. Talar tilt (CFL): invert hindfoot, compare to contralateral. Compare side-to-side - absolute values less reliable.
Brostrom-Gould = anatomic repair + IER reinforcement (first line). Non-anatomic reconstruction (tenodesis) for revision, generalized laxity, or poor tissue. Graft reconstruction increasingly popular.
- Examination
- Normal drawer/tilt, weak peroneals
- Imaging
- XR normal, consider MRI
- Management
- 6 months proprioceptive rehab
- Examination
- Positive drawer, minimal tilt
- Imaging
- Stress XR equivocal
- Management
- Trial bracing + rehab first
- Examination
- Positive drawer AND tilt
- Imaging
- Stress XR positive
- Management
- Surgical stabilization
- Examination
- Positive exam, generalized laxity
- Imaging
- MRI shows tissue quality
- Management
- Graft reconstruction
ACPLateral Ligament Complex
Hook:ACP = Anterior is weakest, Calcaneofibular is Central, Posterior is strongest!
Overview and Epidemiology
Chronic ankle instability (CAI) develops in 20-40% of patients following lateral ankle sprain. It is characterized by recurrent ankle sprains, episodes of giving way, and persistent symptoms lasting greater than 12 months despite conservative treatment. Athletes and active individuals are at highest risk.
Multifactorial: (1) Incomplete ligament healing with elongation/attenuation, (2) Proprioceptive deficit from mechanoreceptor damage, (3) Peroneal muscle weakness, (4) Altered neuromuscular control. Both mechanical and functional factors contribute.
- Previous ankle sprain (strongest predictor)
- Inadequate initial treatment/rehab
- High-demand sports (basketball, soccer)
- Generalized ligamentous laxity
- Cavovarus foot alignment
- Osteochondral lesions of talus (15-25%)
- Subtalar instability
- Peroneal tendon pathology
- Anterior/posterior impingement
- Syndesmotic injury
Pathophysiology and Mechanisms
The lateral ligament complex consists of three ligaments. The ATFL originates from anterior fibula and inserts on lateral talar body - it is the primary restraint against anterior translation in plantarflexion. The CFL is extra-articular, crosses the subtalar joint, and resists inversion throughout ROM.
- Origin
- Anterior distal fibula
- Insertion
- Lateral talar body
- Injury Frequency
- 85% (most common)
- Function
- Resists anterior translation in PF
- Origin
- Distal fibula tip
- Insertion
- Lateral calcaneus
- Injury Frequency
- 50-75% combined
- Function
- Resists inversion, crosses STJ
- Origin
- Posterior fibula
- Insertion
- Posterior talus
- Injury Frequency
- Rare (5%)
- Function
- Resists posterior translation in DF

ATFL taut in plantarflexion - this is why most ankle sprains occur with plantarflexion-inversion mechanism. ATFL provides 100% of resistance to anterior talar translation at 15 degrees plantarflexion. Sectioning ATFL increases anterior drawer by 4-5mm.
- Length: 15-20mm, width: 7-8mm
- Weakest lateral ligament
- Intra-articular structure
- 3 distinct bands described
- Mean load to failure: 139N
- Length: 20-25mm, cord-like
- Extra-articular (key exam point)
- Crosses subtalar joint
- Overlapped by peroneal tendons
- Mean load to failure: 310N
PROPSCauses of Functional Instability
Hook:PROPS support the ankle - without them, it gives way!
Classification Systems
Mechanical vs Functional Classification
- Definition
- True ligamentous laxity
- Examination
- Positive drawer/tilt, stress XR abnormal
- Treatment Focus
- Surgical stabilization
- Definition
- Giving way without laxity
- Examination
- Normal exam, proprioceptive deficit
- Treatment Focus
- Proprioceptive rehabilitation
- Definition
- Both mechanical and functional
- Examination
- Laxity + neuromuscular deficit
- Treatment Focus
- Surgery + comprehensive rehab
Functional instability can exist without mechanical laxity and responds well to rehabilitation. Mechanical instability requires structural restoration. Most patients with CAI have elements of both, requiring comprehensive management.
Classification guides treatment approach and rehabilitation focus.
Clinical Assessment
- Mechanism: Index injury and subsequent events
- Symptoms: Giving way, swelling, pain, difficulty on uneven ground
- Sports/Activity level: Demands and expectations
- Previous treatment: Bracing, rehab, surgery
- Inspection: Swelling, alignment (cavovarus)
- Palpation: ATFL, CFL, peroneal tendons, sinus tarsi
- ROM: Ankle and subtalar joint
- Stress tests: Anterior drawer, talar tilt
Always assess: subtalar instability (Broden stress), peroneal tendon integrity (subluxation, tears), generalized ligamentous laxity (Beighton score), hindfoot alignment (cavovarus = higher recurrence), and contralateral ankle for comparison.
- Technique
- Stabilize tibia, translate talus anteriorly
- Positive Finding
- Greater than 10mm or greater than 3mm vs contralateral
- Structure Tested
- ATFL
- Technique
- Stabilize tibia, invert hindfoot
- Positive Finding
- Greater than 10 degrees or greater than 5 degrees asymmetry
- Structure Tested
- CFL (+ ATFL if positive)
- Technique
- Maximal inversion with ankle neutral
- Positive Finding
- Pain, apprehension, increased motion
- Structure Tested
- Lateral ligament complex
- Technique
- Resist eversion, check for subluxation
- Positive Finding
- Weakness, subluxation over malleolus
- Structure Tested
- Peroneal tendons
Absolute values are unreliable due to normal variability. Always compare to contralateral ankle. Asymmetry greater than 3mm (drawer) or greater than 5 degrees (tilt) is more significant than absolute measurements. Examine both ankles in the same position.
Differential Diagnosis of the "Giving-Way" Ankle
Recurrent giving way is NOT always lateral ligament instability. The exam favourite is the patient with normal stress tests whose true problem lies elsewhere - missing these is a classic viva trap.
- Distinguishing Features
- Positive drawer/tilt, plantarflexion-inversion mechanism
- Best Test
- Stress radiographs, MRI
- Why It Mimics CAI
- True ATFL/CFL laxity - the index diagnosis
- Distinguishing Features
- Giving way, NORMAL stress tests, peroneal weakness
- Best Test
- Balance/proprioception testing
- Why It Mimics CAI
- Neuromuscular deficit without structural laxity
- Distinguishing Features
- Sinus tarsi pain, hindfoot giving way, Broden views
- Best Test
- Broden stress views, exam under anaesthesia
- Why It Mimics CAI
- Often coexists; tilt may be falsely attributed to CFL
- Distinguishing Features
- Posterolateral pain, snapping, weak eversion
- Best Test
- Dynamic ultrasound, MRI
- Why It Mimics CAI
- Peroneals are dynamic stabilizers - failure feels like instability
- Distinguishing Features
- Deep ankle pain, catching, effusion
- Best Test
- MRI, arthroscopy
- Why It Mimics CAI
- Catching/locking misread as giving way
- Distinguishing Features
- Anterolateral pain on dorsiflexion, no laxity
- Best Test
- MRI, diagnostic arthroscopy
- Why It Mimics CAI
- Pain limits activity, mimics unstable ankle
- Distinguishing Features
- Visible varus, lateral overload, recurrent sprains
- Best Test
- Weight-bearing alignment views, Coleman block
- Why It Mimics CAI
- Structural varus drives recurrent inversion injury
Investigations
Imaging Protocol
AP, lateral, and mortise views. Assess for malalignment, OLT, talar dome changes, arthritis. Weight-bearing views essential for alignment assessment. Often normal in isolated ligament injury.
Anterior drawer stress (Telos device) and inversion stress views. Quantify mechanical instability. Drawer greater than 10mm or tilt greater than 10 degrees (or asymmetry greater than 3mm/5 degrees) indicates instability.
Assess ligament quality, associated lesions (OLT, peroneal pathology, impingement), and tissue quality for surgical planning. Identifies chronic ligament changes (thickening, discontinuity, scarring).
Anterior drawer: greater than 10mm absolute or greater than 3mm asymmetry = ATFL incompetent. Talar tilt: greater than 10 degrees absolute or greater than 5 degrees asymmetry = ATFL + CFL involved. Always compare to uninjured side.
- Stress XR: Quantify laxity
- Standard XR: Alignment, OLT, arthritis
- Broden stress: Subtalar instability
- Hindfoot alignment view: Cavovarus
- ATFL: Thickened, attenuated, absent
- CFL: Integrity, scarring
- OLT: Location, size, stability
- Peroneal tendons: Tears, subluxation

Management Algorithm
Non-Operative Management Protocol
Goal: Restore proprioception, strength, and neuromuscular control.
Rehabilitation Phases
Acute management: RICE for any acute exacerbations. Ankle bracing for activity. Begin ROM exercises. Initiate proprioceptive training (single leg stance, wobble board).
Strengthening and proprioception: Progressive peroneal strengthening. Balance training progression. Sport-specific agility introduction. Continue bracing for activity.
Return to activity: Graduated return to sport. Continue proprioceptive maintenance. Brace use as needed. Monitor for recurrent symptoms.
60-80% success rate with comprehensive rehabilitation. Better outcomes with: functional instability only, good compliance, lower demands, and adequate peroneal strength. Failure indicators: mechanical laxity, cavovarus foot, high-demand athlete.
Minimum 6 months of supervised rehabilitation before considering surgery.
Surgical Technique
Modified Brostrom Procedure (Gold Standard)
Surgical Steps
Lateral decubitus or supine with bump. Thigh tourniquet. Mark landmarks: lateral malleolus, ATFL course, peroneal tendons, sinus tarsi.
Curvilinear incision anterior and distal to lateral malleolus (following ATFL). Identify and protect superficial peroneal nerve branches. Incise IER (inferior extensor retinaculum).
Identify ATFL (often attenuated, scarred). Assess CFL through same incision or separate distal limb. Evaluate tissue quality for repair vs reconstruction decision.
Incise ATFL capsule longitudinally at its talar attachment. Prepare fibular footprint with decortication. Pass suture anchors (2-3) into anterior fibula. Pants-over-vest imbrication of ATFL with ankle in neutral.
Key step: Advance IER (inferior extensor retinaculum) over ATFL repair and secure to fibula with sutures. This provides critical reinforcement and limits anterior translation.
If CFL involved, extend incision distally. Repair CFL to calcaneus with suture anchor or directly if tissue quality permits. Tension with ankle in neutral to slight eversion.
Tension repair with ankle in neutral - avoid over-tightening (causes stiffness) or under-tightening (recurrence). IER augmentation (Gould) is critical for improved outcomes. Consider arthroscopy first for OLT assessment and treatment.
Post-repair immobilization in walking boot for 2-4 weeks, then progressive weight-bearing and rehabilitation.
BGTSurgical Options
Hook:BGT = Brostrom is Gold standard, Tenodesis for revisions!
Arthroscopic and Arthroscopic-Assisted Brostrom Repair
The open modified Brostrom-Gould remains the reference standard, but arthroscopic and arthroscopic-assisted ("all-inside") lateral ligament repair has grown rapidly because it lets the surgeon treat intra-articular pathology and repair the ligament in a single setting. As the topic's own evidence base shows (Song and Hua meta-analysis), early functional outcomes are equivalent to open repair; the trade-off is a distinct nerve-injury profile that examiners expect you to name.
- Diagnostic arthroscopy first through standard anteromedial and anterolateral portals - treat synovitis, loose bodies, anterolateral impingement and any osteochondral lesion in the same sitting
- All-inside repair: one or two suture anchors placed into the anterior fibula at the ATFL footprint under direct vision
- Sutures capture the distal ATFL remnant and the inferior extensor retinaculum, recreating the Gould reinforcement, and are tied over the retinaculum
- Arthroscopic-assisted variants use a small accessory incision to retrieve and tension the sutures
- The superficial peroneal nerve (intermediate dorsal cutaneous branch) crosses the anterolateral working zone and is the structure most often bruised or caught in a suture
- The sural nerve is at risk with more posterior, distal anchor and knot placement near the CFL
- Careful portal placement, transillumination and avoiding blind percutaneous suture passage reduce - but do not eliminate - neuritis, the commonest reported complication
Arthroscopic repair suits primary cases with good-quality remnant tissue and coexisting intra-articular pathology to address. Because it depends on that remnant, poor tissue, generalized hyperlaxity, revision surgery and significant deformity still favour open anatomic repair or graft reconstruction. Long-term durability data for the arthroscopic technique remain immature, so the pragmatic answer is to match technique to tissue quality and surgeon experience.
Complications
- Risk Factors
- Poor tissue quality, cavovarus, non-compliance
- Prevention
- Proper patient selection, address alignment
- Management
- Revision reconstruction with graft
- Risk Factors
- Over-tensioning, prolonged immobilization
- Prevention
- Appropriate tensioning, early ROM
- Management
- Physiotherapy, possible MUA
- Risk Factors
- Surgical approach
- Prevention
- Careful dissection, identify nerve
- Management
- Observation, most resolve
- Risk Factors
- Diabetes, obesity, smoking
- Prevention
- Meticulous technique, optimize health
- Management
- Wound care, possible debridement
- Risk Factors
- Non-anatomic procedures
- Prevention
- Use anatomic techniques
- Management
- PT, accept some limitation
Higher recurrence with: cavovarus foot (address surgically if significant), generalized ligamentous laxity (use graft augmentation), poor rehabilitation compliance, return to high-demand sport too early. Recurrence rate 5-15% even with modern techniques.
Cavovarus alignment places lateral ligaments at increased stress. If significant hindfoot varus present, consider calcaneal osteotomy (Dwyer) at time of ligament reconstruction to correct alignment and reduce recurrence risk.
Postoperative Care
Rehabilitation Protocol
Immobilization: Below-knee cast or controlled motion boot. Non-weight-bearing initially. Elevate, ice, wound care. Begin toe/knee ROM to prevent stiffness.
Protected mobilization: CAM boot weight-bearing as tolerated. Begin ankle ROM exercises out of boot. Avoid inversion initially. Start isometric strengthening.
Progressive loading: Wean from boot to supportive footwear. Progressive resistance training. Proprioception exercises. Gait training, stationary bike.
Return to activity: Sport-specific drills. Agility and plyometric progression. Criteria-based return to sport. Consider bracing for return.
- Greater than 90% strength vs contralateral
- Full ROM without pain
- Passed functional hop tests
- Sport-specific drills tolerated
- Typically 4-6 months post-op
- Consider brace for first 6-12 months of sport
- May use permanently for high-demand activities
- Ankle support reduces re-injury risk
- Transition to tape if preferred
Outcomes and Prognosis
- Success Rate
- 85-95%
- Recurrence
- 5-10%
- Return to Sport
- 85-90%
- Success Rate
- 80-90%
- Recurrence
- 5-15%
- Return to Sport
- 80-85%
- Success Rate
- 70-80%
- Recurrence
- 10-20%
- Return to Sport
- 70-80%
- Success Rate
- 70-85%
- Recurrence
- 15-25%
- Return to Sport
- 70-80%
Brostrom-Gould has excellent long-term outcomes with 20+ year follow-up studies showing maintained stability. Anatomic reconstruction approaches similar outcomes when properly indicated. Key to success: appropriate patient selection, address associated pathology, comprehensive rehabilitation.
Outcome Measures and Case Identification
The registry section lists several patient-reported instruments; examiners increasingly reward candidates who name a validated tool rather than relying on an eyeball assessment. These fall into two groups: case-identification questionnaires that establish whether a patient genuinely has chronic ankle instability, and outcome scores used to track results and compare studies.
- Type
- Case identification
- What It Measures
- Severity of functional instability from 9 items, scored 0 to 30 (lower = more unstable)
- Notes
- A score of 27 or below is the commonly cited threshold for instability; validated and assessed per side
- Type
- Case identification
- What It Measures
- History of the first sprain plus current giving-way episodes
- Notes
- Aligns with international consensus (Ankle Consortium) inclusion criteria
- Type
- Outcome
- What It Measures
- Ankle-instability-specific function, 0 to 100
- Notes
- Primary outcome in several instability trials (e.g. the OLT single-stage RCT)
- Type
- Outcome
- What It Measures
- Activities-of-daily-living subscale plus a Sport subscale
- Notes
- Region-specific and responsive to change
- Type
- Outcome
- What It Measures
- Pain, function and alignment, 0 to 100
- Notes
- Widely reported but criticised for limited formal validation
Saying a patient "feels unstable" is not enough - the International Ankle Consortium recommends confirming chronic ankle instability with a validated questionnaire such as the CAIT (score 27 or below out of 30), together with a documented history of recurrent sprains and giving way persisting for at least 12 months. Using a defined tool separates true instability from a vague symptom and underpins consistent research and audit.
Guidelines, Registries & Global Practice
Global Epidemiology
Lateral ankle sprain is one of the most common musculoskeletal injuries worldwide, with an estimated incidence around 2-7 per 1000 person-years in the general population and far higher in court and field sports (basketball, volleyball, football/soccer, netball, rugby). Roughly 20-40% of sprains lead to chronic ankle instability. The injury affects all regions and resource settings; the burden is concentrated in young, active populations, and women have a higher rate in indoor court sports.
Side-by-Side Guideline Comparison
- Initial Management
- Functional treatment: brace/tape PLUS supervised exercise; avoid prolonged immobilisation
- Imaging Stance
- Delayed exam at 4-5 days most reliable; imaging for refractory/atypical cases
- Surgical Position
- Reserve surgery for failure of comprehensive exercise-based rehab
- Initial Management
- Functional rehab and neuromuscular training first-line
- Imaging Stance
- Stress radiographs and MRI to confirm mechanical laxity and associated lesions before surgery
- Surgical Position
- Anatomic repair (modified Brostrom-Gould) as standard; reconstruction for revision/poor tissue
- Initial Management
- PRICE/POLICE then exercise rehab; brace for recurrent sprains
- Imaging Stance
- Selective imaging; MRI when associated pathology suspected
- Surgical Position
- Surgery for documented mechanical instability failing rehab
- Initial Management
- Conservative rehabilitation first
- Imaging Stance
- Stress imaging and MRI for surgical planning
- Surgical Position
- Anatomic repair preferred; arthroscopic management of intra-articular lesions encouraged
Across societies the message is consistent: structured exercise-based rehabilitation first, anatomic (Brostrom-type) repair as the surgical default, and reconstruction reserved for revision, hyperlaxity or poor tissue. Differences are mainly in imaging thresholds and how aggressively associated lesions are sought.
- No dedicated international ligament-repair registry exists (unlike arthroplasty); evidence comes from cohort series, RCTs and meta-analyses
- Patient-reported outcome measures used: Karlsson-Peterson, AOFAS, FAAM, CAIT (Cumberland Ankle Instability Tool) for case identification
- Reported recurrence after modern anatomic repair is roughly 5-15%
- High-resource: stress imaging, MRI, arthroscopy, suture-anchor/graft constructs, supervised return-to-sport programmes
- Limited-resource: clinical diagnosis and functional rehab predominate; bracing/taping widely used; non-anatomic tenodesis may still be performed where anchors/grafts are unavailable
- Functional rehabilitation is effective and low-cost - the global first-line everywhere
Examiners worldwide (FRCS, FRACS, EBOT, ABOS, DNB/MS, MRCS, SICOT) expect: mechanical vs functional instability, anatomy of the lateral ligament complex (ATFL taut in plantarflexion, CFL extra-articular crossing the subtalar joint), stress radiograph thresholds, the Brostrom-Gould technique, and indications for graft reconstruction in revision/hyperlaxity settings.
Controversies and Areas of Uncertainty
High-level evidence in chronic ankle instability is limited, and several questions remain genuinely unsettled - examiners reward a balanced, evidence-aware answer here.
Arthroscopic and arthroscopic-assisted repair are rising rapidly. Meta-analysis shows equivalent early functional outcomes to open repair, but long-term durability data are immature and nerve-related complications (superficial peroneal, sural) are a concern. Open remains the reference standard.
When to abandon anatomic repair for graft reconstruction is not standardised. Proposed but unvalidated triggers: generalized hyperlaxity (Beighton high), poor remnant tissue, BMI/high demand, and revision. Some advocate primary suture-tape augmentation to allow accelerated rehab - long-term superiority is unproven.
Augmenting the Brostrom with non-absorbable tape may permit earlier loading and protect the repair, but risks over-constraint, stiffness and a foreign-body construct. Evidence is mostly short-term cohort data without proven outcome benefit over standard Brostrom-Gould.
RCT data support single-stage treatment of OLT with stabilization. Subtalar instability is harder - diagnosis is unreliable (no validated stress threshold), and whether it needs specific surgical address versus a combined ATFL/CFL reconstruction remains debated.
When asked "arthroscopic or open?" or "repair or reconstruct?", state that high-quality long-term comparative data are limited, give the pragmatic indication-based answer, and acknowledge that surgeon experience and tissue quality drive the decision. Avoid dogmatic claims.
MCQ Practice Points
Q: Which ligament is the primary restraint against anterior translation of the talus in plantarflexion? A: Anterior talofibular ligament (ATFL) - The ATFL is taut in plantarflexion and provides 100% of resistance to anterior talar translation at 15 degrees plantarflexion. It is the weakest and most commonly injured lateral ligament.
Q: What unique anatomical feature of the CFL makes it important for subtalar stability? A: CFL is extra-articular and crosses the subtalar joint - Unlike the ATFL which is intra-articular, the CFL crosses both the ankle and subtalar joints, contributing to stability of both articulations.
Q: What is considered a positive anterior drawer stress test in chronic ankle instability? A: Greater than 10mm absolute OR greater than 3mm asymmetry compared to contralateral - Side-to-side comparison is more reliable than absolute values due to individual variation in ligamentous laxity.
Q: What is the gold standard first-line surgical procedure for chronic ankle instability? A: Modified Brostrom-Gould - This anatomic repair involves ATFL imbrication to the fibula with suture anchors plus reinforcement with the inferior extensor retinaculum (Gould modification), achieving 85-95% success rates.
Q: What is the purpose of the Gould modification in the Brostrom procedure? A: Reinforcement with inferior extensor retinaculum (IER) - The IER is advanced over the ATFL repair and secured to the fibula, providing additional anterior restraint and improving outcomes compared to ATFL repair alone.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old soccer player presents with recurrent ankle sprains over 2 years. He has completed 6 months of physiotherapy with bracing. Examination shows positive anterior drawer (12mm vs 6mm contralateral). He wants to return to competitive sport.”
“A 35-year-old woman had a Brostrom repair 3 years ago that failed after 18 months. She now has persistent instability, giving way episodes, and anterior drawer 14mm (vs 5mm contralateral). MRI shows attenuated ligament remnants.”
“A 28-year-old basketball player has CAI confirmed on stress XR. MRI also shows a 1.2cm medial talar dome osteochondral lesion with overlying cartilage damage. He has failed conservative treatment.”
“A 30-year-old recreational runner has recurrent giving way and ankle sprains. She has completed 3 months of physiotherapy. Examination shows negative anterior drawer and talar tilt. She has significant peroneal weakness and poor single-leg balance.”
Key Anatomy
- ATFL: weakest ligament, intra-articular, taut in PLANTARFLEXION
- CFL: EXTRA-ARTICULAR, crosses subtalar joint, taut in DF
- PTFL: strongest, rarely injured
- Anterior drawer tests ATFL; Talar tilt tests CFL
Instability Types
- MECHANICAL: true laxity (positive stress tests/XR)
- FUNCTIONAL: giving way WITHOUT laxity (proprioceptive deficit)
- Most CAI patients have BOTH components
- Surgery for mechanical; Rehab for functional
Stress Test Thresholds
- Anterior drawer: greater than 10mm OR greater than 3mm asymmetry = positive
- Talar tilt: greater than 10 degrees OR greater than 5 degrees asymmetry = ATFL + CFL
- Always COMPARE to contralateral side
- Asymmetry more reliable than absolute values
Surgical Approach
- Brostrom-Gould = GOLD STANDARD (85-95% success)
- Gould modification = IER reinforcement (critical)
- Graft reconstruction for: revision, hyperlaxity, poor tissue
- Non-anatomic tenodesis largely HISTORICAL
Exam Pearls
- 6 months conservative before surgery
- ATFL provides 100% resistance to anterior translation at 15 degrees PF
- Always assess for OLT (15-25%), peroneals, subtalar instability
- Cavovarus = higher recurrence - consider calcaneal osteotomy
Evidence Base
- In 61 patients undergoing lateral ligament reconstruction, NO ankle had isolated ligament injury. Most common associated lesions: peroneal tenosynovitis 77%, anterolateral impingement 67%, attenuated peroneal retinaculum 54%, ankle synovitis 49%, loose body 26%, peroneus brevis tear 25%, talar osteochondral lesion 23%.
- 32 ankles in young active patients (US Naval Academy) followed a mean 26.3 years. Mean ankle function 91/100; 91% rated their ankle good or excellent. Stability durable over the long term.
- Multicentre comparison (25 anatomical reconstruction vs 29 tenodesis), mean 12.3-year follow-up. Tenodesis had more positive anterior drawer, greater talar tilt and translation on stress radiographs, more medial degenerative change, and fewer excellent results. Tenodesis does NOT restore normal ligament anatomy.
- Functional treatment (tape/brace plus a supervised exercise programme) is favoured over immobilisation for acute lateral ligament rupture. Surgery is reserved for cases failing comprehensive exercise-based treatment. Bracing reduces recurrent sprains. NSAIDs may impair healing.
- 4 comparative studies (1 RCT), 207 patients. No statistically significant difference in functional outcome scores between arthroscopic and open Brostrom repair at early term; both gave favourable results, with one study showing faster return to daily activity after arthroscopy.
- RCT of 103 patients with both CLAI and osteochondral lesion of the talus. Concurrent (single-stage) microfracture plus modified Brostrom-Gould was non-inferior to staged surgery at 24 months, and gave better Karlsson-Peterson and AOFAS scores at short-term follow-up.