Iliopsoas | Rectus Femoris | Athletic Population
- Rectus femoris injuries MORE COMMON than iliopsoas in athletes
- ASIS avulsion = sartorius; AIIS avulsion = rectus femoris
- Iliopsoas bursa largest in body - can communicate with hip joint
- Hip flexor weakness = antalgic gait with increased lordosis
- Return to sport based on STRENGTH not just pain resolution
- “Thomas test positive = hip flexor contracture
- “Resisted hip flexion at 90 degrees isolates iliopsoas
- “AIIS avulsions common in adolescents (apophysis open)
- “Ultrasound can assess dynamic function in real-time
Iliopsoas (iliacus + psoas major) and rectus femoris are primary hip flexors. RF crosses two joints (hip + knee) making it vulnerable during high-velocity activities like kicking and sprinting.
In adolescents, apophyseal avulsions are common. AIIS = rectus femoris, ASIS = sartorius, ischial tuberosity = hamstrings. Always get X-rays in young athletes with acute onset.
Thomas test for contracture. Resisted hip flexion at 90 degrees (patient supine) isolates iliopsoas. Resisted straight leg raise tests rectus femoris more.
Strength-based criteria - not just pain-free. Aim for greater than 90% strength compared to uninjured side. Premature return leads to high recurrence rates (30% if inadequate rehab).
- Grade
- Grade I
- Treatment
- RICE, relative rest, early mobilization
- Return Timeline
- 1-2 weeks
- Grade
- Grade II
- Treatment
- Protected activity, progressive rehab
- Return Timeline
- 4-6 weeks
- Grade
- Grade III
- Treatment
- Immobilization, consider surgery
- Return Timeline
- 3-6 months
- Grade
- Avulsion
- Treatment
- X-ray, possible surgical fixation
- Return Timeline
- 6-12 weeks
PRISMHip Flexor Anatomy
Hook:PRISM of muscles bend the hip - ilioPSoas and Rectus lead the way!
AIIS ASIS ITAvulsion Fracture Sites
Hook:AIIS = INFERIOR = RECTUS (below); ASIS = SUPERIOR = SARTORIUS (above)
SPORTReturn to Sport Criteria
Hook:SPORT readiness = STRENGTH first, pain-free second!
Overview and Epidemiology
Hip flexor strains are common in sports requiring explosive hip flexion, including soccer, running, martial arts, and dance. The rectus femoris is affected more frequently than iliopsoas due to its biarticular nature, which increases eccentric loading during activities like kicking.
Rectus femoris: Eccentric loading during kicking, sprinting (leg deceleration phase). Iliopsoas: Forceful hip flexion against resistance. The dual innervation (femoral nerve for RF, lumbar plexus for iliopsoas) has implications for recovery.
- Previous strain (strongest predictor)
- Inadequate warm-up
- Muscle fatigue
- Inflexibility/contracture
- Strength imbalance
- Soccer (kicking sports)
- Running/sprinting
- Martial arts
- Dance/gymnastics
- Australian Rules Football
Pathophysiology and Mechanisms
The iliopsoas is the most powerful hip flexor, composed of psoas major (T12-L5 vertebral bodies) and iliacus (iliac fossa), uniting to insert on the lesser trochanter. The rectus femoris has two heads (straight from AIIS, reflected from acetabular rim) and is the only quadriceps component that crosses the hip.
- Origin
- T12-L5 + Iliac fossa
- Insertion
- Lesser trochanter
- Innervation
- Femoral nerve + L1-3
- Clinical Note
- Strongest flexor, deep location
- Origin
- AIIS (straight) + Acetabulum (reflected)
- Insertion
- Tibial tuberosity via patella
- Innervation
- Femoral nerve (L2-4)
- Clinical Note
- Biarticular = high strain risk
- Origin
- ASIS
- Insertion
- Pes anserinus (tibia)
- Innervation
- Femoral nerve (L2-3)
- Clinical Note
- Longest muscle, weak flexor
- Origin
- ASIS and iliac crest
- Insertion
- ITB to Gerdy tubercle
- Innervation
- Superior gluteal nerve
- Clinical Note
- Flexion, abduction, IR
Rectus femoris crosses two joints - it is stretched maximally when the hip is extended AND knee is flexed (e.g., late swing phase of sprinting, follow-through of kick). This is when most RF strains occur.
- Largest bursa in body
- Between iliopsoas tendon and hip capsule
- Communicates with hip joint (15-20%)
- Bursitis can mimic hip flexor strain
- RF: Long fascicles, high velocity capacity
- Iliopsoas: Shorter fascicles, high force
- Pennation angle affects strain risk
- Type II fibres predominate (fast twitch)
Classification Systems
Standard Muscle Strain Classification
- Pathology
- Less than 5% fibres disrupted
- Clinical Features
- Minimal pain, no weakness, full ROM
- Imaging
- Normal or minor oedema
- Recovery
- 1-2 weeks
- Pathology
- 5-50% fibres disrupted
- Clinical Features
- Moderate pain, weakness, antalgic gait
- Imaging
- Partial tear visible, haematoma
- Recovery
- 4-6 weeks
- Pathology
- Greater than 50% or complete rupture
- Clinical Features
- Severe pain, marked weakness, defect
- Imaging
- Complete disruption, retraction
- Recovery
- 3-6 months
Grade I-II differentiation is often clinical. MRI/ultrasound helps quantify tear extent and predict recovery time. Cross-sectional area of tear on MRI correlates with return-to-play time.
This grading system guides treatment intensity and expected recovery timeline.
Clinical Assessment
- Mechanism: Explosive kick, sprint start, sudden change of direction
- Onset: Acute pop/snap vs gradual overuse
- Location: Anterior hip/groin (iliopsoas) vs anterior thigh (RF)
- Functional deficit: Stairs, running, kicking difficulty
- Gait: Antalgic, shortened stride, increased lordosis
- Inspection: Bruising (delayed), swelling
- Palpation: AIIS, lesser trochanter region, muscle belly
- ROM: Limited hip extension if contracture
- Discriminating Feature
- Acute onset, kicking/sprinting, pain on resisted flexion
- Key Test / Investigation
- Resisted hip flexion / SLR; MRI for grade
- Discriminating Feature
- Night/rest pain, female athlete triad, load-related
- Key Test / Investigation
- MRI (urgent); avoid if missed (risk of displacement)
- Discriminating Feature
- Mechanical clicking, deep groin pain, reduced IR
- Key Test / Investigation
- FADIR/impingement positive; MR arthrogram
- Discriminating Feature
- Medial groin, pain on resisted adduction
- Key Test / Investigation
- Squeeze test; Doha classification
- Discriminating Feature
- Pain worse with Valsalva, cough impulse
- Key Test / Investigation
- Dynamic ultrasound; herniography
- Discriminating Feature
- Dermatomal radiation, neurological signs
- Key Test / Investigation
- SLR (neural), lumbar MRI
Femoral neck stress fracture is the critical miss in an athlete with anterior hip/groin pain - night pain, rest pain or the female athlete triad mandate urgent MRI, as a missed tension-side fracture can displace.
- Technique
- Supine, flex opposite hip fully
- Positive Finding
- Tested hip rises off bed
- Muscle Tested
- Hip flexor contracture (general)
- Technique
- Supine, hip at 90, resist further flexion
- Positive Finding
- Pain or weakness
- Muscle Tested
- Iliopsoas (primary)
- Technique
- Supine, straight leg, resist elevation
- Positive Finding
- Pain or weakness
- Muscle Tested
- Rectus femoris (primary)
- Technique
- Prone, passive knee flexion
- Positive Finding
- Hip flexes off bed
- Muscle Tested
- Rectus femoris contracture
Iliopsoas pain is deep, anterior hip/groin, worse with resisted hip flexion at 90 degrees. Rectus femoris pain is more anterior thigh, often at AIIS or muscle belly, worse with resisted SLR or knee extension.
Investigations
Imaging Protocol
AP pelvis + frog lateral. Essential in adolescents to exclude avulsion fracture. Look for AIIS, ASIS, lesser trochanter avulsions. Often normal in pure muscle strains.
Gold standard for soft tissue assessment. Quantifies tear extent (cross-sectional area predicts recovery). Identifies location (musculotendinous junction vs muscle belly). Assesses oedema, haematoma, retraction.
Dynamic assessment possible. Real-time visualization of muscle contraction. Good for superficial muscles (RF). Operator-dependent but accessible.
Longer recovery associated with: Greater cross-sectional area of tear, involvement of central tendon (RF), proximal location (MTJ), significant retraction. MRI within 5 days is optimal for grading.
- Grade I: Feathery oedema, intact fibres
- Grade II: Partial disruption, haematoma
- Grade III: Complete disruption, gap, retraction
- Central tendon involvement = poor prognosis
- Dynamic assessment during contraction
- Guide injections (bursa, haematoma)
- Monitor healing progress
- Cost-effective, no radiation



Management Algorithm
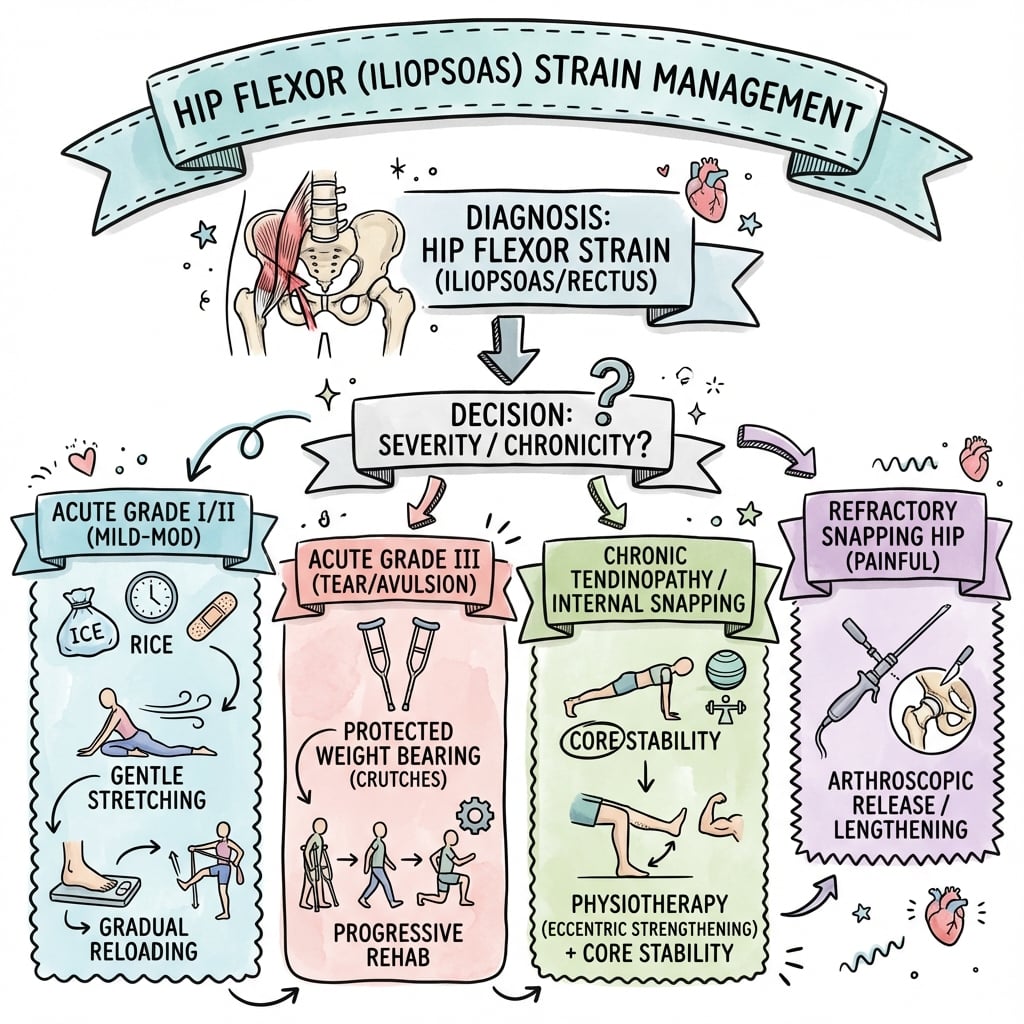
Standard Management Protocol
Goal: Pain control, restore ROM, progressive strengthening, sport-specific return.
Rehabilitation Phases
Protection and pain control: RICE principles. NSAIDs for 3-5 days. Crutches if antalgic gait. Gentle ROM as tolerated. Avoid stretching in acute phase.
ROM and isometric loading: Pain-free ROM exercises. Isometric hip flexion progressing through range. Pool therapy for unloading. Address any compensatory patterns.
Progressive resistance: Isotonic exercises. Hip flexion against bands/weights. Eccentric loading introduction. Core stability work.
Return to play preparation: Sport-specific drills. Sprinting, kicking progression. Agility and plyometrics. Meet return-to-sport criteria.
Must achieve: Greater than 90% strength vs uninjured side, pain-free sport-specific activity, full ROM without contracture, passed functional testing (hop tests, agility). Premature return = 30% recurrence rate.
Rehabilitation timeline varies with injury grade - Grade I may be 1-2 weeks, Grade II 4-6 weeks.
Surgical Technique
Rectus Femoris Avulsion Repair
Surgical Steps
Supine on radiolucent table. Bump under ipsilateral hip if needed. Prep from costal margin to mid-thigh.
Anterior approach to AIIS. Bikini incision or longitudinal over AIIS. Develop interval between sartorius (medial) and TFL (lateral).
Identify retracted tendon stump. May need to mobilize from scar. Protect lateral femoral cutaneous nerve. Identify both heads if possible.
Decorticate AIIS footprint. Create bleeding bone bed. Place suture anchors (2-3 typically).
Pass sutures through tendon. Reduce to footprint with hip in flexion to reduce tension. Secure repair. Assess stability through ROM.
Layered closure over drain if haematoma risk. Standard wound care.
Lateral femoral cutaneous nerve runs medial to ASIS, can be injured during approach. Identify and protect. Numbness is common complication if not careful.
This technique restores anatomic footprint and allows early rehabilitation.
Complications
- Incidence
- 15-30%
- Prevention
- Complete rehabilitation, strength-based RTS
- Management
- Extended conservative management
- Incidence
- 10-20% (Grade III)
- Prevention
- Early surgery if complete rupture
- Management
- Surgical repair if functional deficit
- Incidence
- Rare
- Prevention
- Avoid aggressive massage early, no heat
- Management
- Observation, excision if symptomatic
- Incidence
- 5-10%
- Prevention
- Maintain ROM during healing
- Management
- Stretching program, rarely surgical release
30% recurrence rate if return to sport before adequate rehabilitation. Key risk factors: Previous strain, premature return, inadequate strength restoration, poor flexibility. Ensure greater than 90% strength before clearance.
Iliopsoas Bursitis and Post-Arthroplasty Iliopsoas Impingement
The topic repeatedly invokes the iliopsoas bursa (the largest bursa in the body, communicating with the hip joint in roughly one in seven people) and lists bursal corticosteroid injection in the treatment menu, but the bursitis/tendinopathy entity itself is worth developing because it is the commonest mimic of a hip flexor strain and the commonest iliopsoas-related cause of chronic anterior groin pain.
- Lies between the iliopsoas musculotendinous unit and the iliopectineal eminence / anterior hip capsule
- Communicates with the joint in approximately 15% - so a hip effusion or synovitis can distend it, and an enlarged bursa can present as a groin mass or even compress the femoral vessels
- Secondary bursitis is common: hip OA, rheumatoid/inflammatory arthritis, overuse in dancers and runners
- Deep anterior groin pain, worse on resisted flexion and passive extension; often coexists with internal snapping (routed to the snapping-hip topic)
- A recognised cause of persistent groin pain after total hip arthroplasty (a small but important minority of painful THAs)
- The iliopsoas tendon is irritated by an anteriorly prominent or oversized acetabular cup, uncovered anterior component, retained cement, or a protruding screw/long-neck
- Pain on active straight-leg raise, stair climbing and rising from a chair; reproduced by resisted hip flexion
- Cross-sectional imaging (CT) quantifies anterior cup overhang relative to the native acetabular rim
An image-guided (ultrasound or fluoroscopic) injection of local anaesthetic into the iliopsoas bursa/tendon sheath is both diagnostic and therapeutic - abolition of pain confirms the iliopsoas as the pain generator. Keep the needle in the bursa, not the tendon, to avoid intratendinous steroid and tendon weakening.
For native-hip bursitis, management is conservative: activity modification, NSAIDs, stretching and eccentric loading, with a bursal injection for refractory cases. For post-THA iliopsoas impingement, escalate stepwise: activity modification and a diagnostic/therapeutic injection first; if symptoms persist, iliopsoas tenotomy (arthroscopic or open) is appropriate when the acetabular component is well positioned, whereas a malpositioned or grossly oversized/retroverted cup causing the impingement should be revised rather than simply releasing the tendon.
In an examiner's viva, do not attribute all post-arthroplasty groin pain to iliopsoas impingement - exclude infection, aseptic loosening, and adverse reaction to metal debris first. Iliopsoas impingement is a diagnosis of a well-fixed, but anteriorly prominent, component supported by a positive image-guided injection.
Iliacus/Iliopsoas Haematoma and Femoral Nerve Palsy
The topic emphasises the iliopsoas' femoral-nerve (and lumbar-plexus) innervation and describes Grade III injury with haematoma, but never develops the can't-miss neurological complication this anatomy creates: a haematoma within the tight iliacus fascial compartment can compress the femoral nerve, which runs in the groove between iliacus and its overlying fascia.
The femoral nerve is tethered against the iliacus by the unyielding iliacus fascia. Blood accumulating in this closed compartment (from a severe iliacus/psoas strain or avulsion, or spontaneously in the anticoagulated or haemophilic patient) rapidly raises pressure and produces a compressive femoral neuropathy - the iliopsoas equivalent of a compartment syndrome.
- Acute groin/iliac-fossa pain with the hip held flexed and externally rotated (this shortens the compartment and eases pain - a positive "psoas sign")
- Quadriceps weakness (loss of knee extension) and a diminished/absent patellar reflex
- Sensory loss over the anterior thigh and medial leg (saphenous distribution)
- Consider it in any anticoagulated patient with sudden groin pain and a flexed hip
- CT or ultrasound confirms and sizes the iliacus/retroperitoneal haematoma
- Check coagulation status (INR, platelets, factor levels) and reverse coagulopathy
- Most are managed conservatively - reverse anticoagulation, analgesia, observe the neurology
- Surgical or image-guided decompression/evacuation is reserved for a progressive or dense femoral nerve deficit
A femoral nerve palsy after a hip flexor injury or in an anticoagulated patient is an iliacus haematoma until proven otherwise. Early recognition, coagulopathy reversal and serial neurological assessment protect quadriceps function; delayed decompression of a progressive deficit risks permanent weakness.
Postoperative Care and Rehabilitation
Rehabilitation After Surgical Repair
Partial weight bearing with crutches. Hip flexion limited to 90 degrees. Brace if needed. Gentle passive ROM. No active hip flexion against resistance.
Progress to full weight bearing. Begin active-assisted hip flexion. Isometric strengthening. Pool therapy. Cycling.
Progressive resistance exercises. Isotonic hip flexion. Eccentric loading. Core stability. Gait normalization.
Return to play preparation. Sport-specific drills. Sprinting progression. Meet RTS criteria before clearance.
Protect the repair for 6 weeks - avoid resisted hip flexion. Rehabilitation is similar to tendon repairs elsewhere - progressive loading after initial protection phase.
Expect 3-6 months before return to competitive sport after surgical repair.
Outcomes and Prognosis
- Conservative Success
- Greater than 95%
- Surgical Success
- N/A
- Return Timeline
- 1-2 weeks
- Conservative Success
- 90-95%
- Surgical Success
- N/A
- Return Timeline
- 4-6 weeks
- Conservative Success
- 50-70%
- Surgical Success
- 85-90%
- Return Timeline
- 3-6 months
Poor prognosis: Central tendon involvement, proximal location, significant retraction, delayed treatment. Good prognosis: Muscle belly injury, minimal retraction, early appropriate management, good compliance.
Guidelines, Registries & Global Practice
Global Epidemiology
Hip flexor and iliopsoas-related injuries cluster in kicking and change-of-direction sports (soccer, Australian Rules, Gaelic football, rugby, sprinting, dance). In the UEFA Elite Club Injury Study, thigh muscle injuries (quadriceps and hamstring) are among the most common time-loss injuries in professional football. Using the Doha framework, iliopsoas-related groin pain is a recognised distinct entity, though adductor-related pain predominates and multiple causes coexist in roughly 40-45% of athletes presenting with groin pain. Apophyseal avulsions concentrate in adolescents aged 13-17 years before apophyseal fusion, with a strong male predominance.
Side-by-Side Guidance
- Region
- International
- Core Message for Hip Flexor / Muscle Injury
- Separate functional disorders from structural tears; standardise terminology
- Region
- International
- Core Message for Hip Flexor / Muscle Injury
- Classify by clinical entity (iliopsoas-, adductor-, inguinal-, pubic-, hip-related)
- Region
- UK
- Core Message for Hip Flexor / Muscle Injury
- Grade 0-4 with myofascial/musculotendinous/intratendinous (a/b/c) site modifier
- Region
- International
- Core Message for Hip Flexor / Muscle Injury
- Strength- and function-based return to sport, not pain alone
- Early MRI (within 5 days) for grading and prognosis
- Access to ultrasound-guided injection and isokinetic strength testing
- Structured criteria-based return-to-sport pathways
- Orthobiologics (PRP) available but evidence remains mixed
- Clinical grading and plain radiographs drive decisions
- Ultrasound is a cost-effective, radiation-free alternative to MRI
- Hand-held dynamometry or contralateral comparison guides return to sport
- Conservative management is appropriate for nearly all strains and avulsions
Document:
- Mechanism and grade of injury
- Explanation of recovery timeline
- Return-to-sport criteria (strength-based)
- Risks of premature return (30% recurrence)
- For adolescents: X-ray performed, avulsion excluded
Consent for surgery: Recurrence, weakness, nerve injury (LFCN), need for revision.
Controversies and Areas of Uncertainty
Platelet-rich plasma for muscle strains shows inconsistent results across trials. No robust evidence that PRP accelerates return to sport in acute hip flexor strains; it remains adjunctive at best.
Traditional Grade I-III is simple but crude. Munich and BAMIC systems add prognostic detail (functional vs structural, intratendinous involvement) but inter-rater reliability and superiority for hip flexors specifically are unproven.
The widely quoted 2cm surgical threshold is largely consensus-derived. Most avulsions (including some over 2cm) heal conservatively; the strongest predictor of nonunion in large series is displacement over 20mm and ischial tuberosity location, not muscle origin.
Whether fractional (partial) lengthening reliably preserves hip flexion strength versus complete tenotomy is debated. Reported persistent weakness varies, and routine release for snapping hip without mechanical symptoms is discouraged.
A balanced answer acknowledges that hip flexor strain management is largely evidence-poor and consensus-driven: high-level RCTs are lacking, most data are extrapolated from hamstring and quadriceps literature, and return-to-sport decisions rest on objective strength criteria rather than a single validated protocol.
MCQ Practice Points
Q: Which hip flexor is biarticular, crossing both hip and knee joints? A: Rectus femoris - It originates from AIIS (straight head) and acetabular rim (reflected head), inserting on the tibial tuberosity via the patella. This biarticular nature increases strain risk during activities like kicking.
Q: Which muscle attaches to the AIIS and avulses in adolescent athletes during kicking? A: Rectus femoris (straight head) - AIIS avulsion is common in adolescents before apophyseal fusion (16-18 years). ASIS avulsion = sartorius.
Q: What does a positive Thomas test indicate? A: Hip flexor contracture - With the patient supine and opposite hip fully flexed, if the tested hip rises off the bed, it indicates hip flexor tightness (positive Thomas test).
Q: What is the key criterion for return to sport after hip flexor strain? A: Greater than 90% strength compared to uninjured side - Strength-based criteria reduce recurrence. Pain-free activity alone is insufficient - premature return leads to 30% recurrence rate.
Q: What displacement threshold suggests surgical consideration for apophyseal avulsion? A: Greater than 2cm displacement - While most apophyseal avulsions heal conservatively, significant displacement (over 2cm) may lead to nonunion and functional deficit, particularly in high-demand athletes.
Q: What is the largest bursa in the body and where is it located? A: Iliopsoas bursa - Located between the iliopsoas tendon and hip joint capsule. Communicates with the hip joint in 15-20% of individuals. Bursitis can mimic hip flexor strain.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old male soccer player presents with acute anterior hip/groin pain after kicking during a match yesterday. He felt a sudden sharp pain and had to leave the field. Today he has an antalgic gait and pain with resisted hip flexion. What is your assessment and management?”
“A 14-year-old male sprinter presents with sudden anterior hip pain that occurred during a sprint start at athletics training. He heard a pop and couldn't continue. X-rays show a displaced AIIS avulsion fracture with 2.5cm displacement. How would you manage this?”
“A 28-year-old female dancer presents with persistent anterior hip pain for 6 months after an initial strain. She has completed physiotherapy but still has pain with dancing. Examination shows hip flexor weakness and a positive Thomas test. MRI shows chronic changes at the iliopsoas insertion. What is your differential and management?”
Key Anatomy
- Iliopsoas = psoas major + iliacus → lesser trochanter
- Rectus femoris = AIIS → tibial tuberosity (biarticular)
- AIIS avulsion = RF; ASIS avulsion = sartorius
- Iliopsoas bursa = largest bursa in body
Classification
- Grade I = under 5% fibres = 1-2 weeks
- Grade II = 5-50% fibres = 4-6 weeks
- Grade III = over 50% or complete = 3-6 months
- Apophyseal avulsion: surgery if over 2cm displacement
Clinical Tests
- Thomas test = hip flexor contracture
- Resisted hip flexion at 90 deg = iliopsoas
- Resisted SLR = rectus femoris
- Ely test = RF contracture
Return to Sport
- Greater than 90% strength vs uninjured side
- Pain-free sport-specific activity
- Full ROM, no contracture
- Premature RTS = 30% recurrence
Complications
- Recurrent strain: 15-30% (early RTS risk)
- Chronic weakness: 10-20% (Grade III)
- Myositis ossificans: rare, avoid early massage
- LFCN injury: surgical risk
Evidence Base and Key Trials
Munich Consensus: Terminology and Classification of Muscle Injuries
- Survey of 30 elite team doctors confirmed inconsistent use of the term strain
- New system separates functional muscle disorders (types 1-2) from structural injuries (types 3-4)
- Type 3 = partial tear, type 4 = (sub)total tear / tendinous avulsion
- Standardised terminology to enable comparative research
MRI Findings and Return to Play: UEFA Elite Club Injury Study
- Prospective analysis of 255 grade 1-2 hamstring injuries in elite footballers
- Radiological grade and size of oedema correlated with time to return to play
- Grade 2 lay-off longer than grade 1 (24 vs 18 days)
- Injury location and type did NOT independently predict return to play
Incomplete Intrasubstance Strains of the Rectus Femoris
- Described a distinct intrasubstance tear at the deep (indirect/reflected) head tendon
- Located more proximally than the classic distal MTJ strain
- Mechanism typically kicking or sprinting; presents as chronic thigh pain or mass
- MRI shows abnormal signal around the intramuscular tendon of the indirect head
Pelvic Apophyseal Avulsion Fractures: 228 Cases
- 225 patients, 228 avulsions, mean age 14.4 years, 76% male
- AIIS most common (49%); 50% of AIIS avulsions caused by kicking
- Displacement over 20mm increased nonunion risk 26-fold
- 97% managed conservatively; surgery indicated in only 3%
Proximal Rectus Femoris Avulsions in High-Level Athletes
- Critical analysis review of proximal RF ruptures in skeletally mature athletes
- Injury is rare, occurring in soccer and American football during kicking/sprinting
- Operative repair with suture anchors supported to restore strength and enable return to sport
- Key complications: lateral femoral cutaneous nerve injury and haematoma
Doha Agreement Applied: Causes of Groin Pain in 100 Athletes
- First clinical application of the Doha agreement classification of groin pain
- Iliopsoas-related is a defined clinical entity distinct from adductor-related groin pain
- Adductor-related most prevalent (61%); multiple causes coexisted in 44%
- Predominantly male soccer players in kicking and change-of-direction sports