Location Determines Treatment | Midshaft Most Common | Displacement Key Factor
- Displacement and shortening are key surgical indications for midshaft fractures
- COTS study showed improved union rates but no functional difference at 1 year
- Type II lateral clavicle fractures are unstable - CC ligaments torn
- Floating shoulder = scapula neck + clavicle - surgical stabilization often needed
- Plate position: superior vs anteroinferior - both acceptable, different complications
- “Edinburgh study changed practice - 15% nonunion rate for displaced midshaft
- “Neer Type II lateral = CC ligament disruption = unstable = surgery
- “Shortening over 2cm correlates with poor functional outcomes
- “Medial clavicle fractures - CT for posterior displacement (vascular risk)

Shortening greater than 2cm and 100% displacement are key surgical indications. COTS/Edinburgh data showed improved union with ORIF but similar long-term function.
Neer Type II has CC ligament disruption = unstable = high nonunion rate. Type I (lateral to CC) and Type III (articular) are usually stable.
Posterior displacement is dangerous - CT essential. Risk to great vessels and trachea. Physis closes at 23-25 years - beware SC dislocation in young adults.
Clavicle + scapula neck fracture = double disruption of superior shoulder suspensory complex. Often requires clavicle fixation for stability.
- Key Finding
- Less than 100% displacement, shortening less than 2cm
- Stability
- Good prognosis
- Treatment
- Sling, early ROM, union expected
- Key Finding
- Greater than 2cm shortening, 100% displacement
- Stability
- Higher nonunion risk
- Treatment
- Discuss surgery - similar function at 1yr
- Key Finding
- CC ligament disruption, unstable fragment
- Stability
- Unstable
- Treatment
- Surgical fixation - hook plate or sutures
- Key Finding
- CT shows posterior fragment near vessels
- Stability
- Dangerous
- Treatment
- CT angiogram, likely open reduction
- Key Finding
- Clavicle + scapula neck fracture
- Stability
- Complex instability
- Treatment
- Clavicle ORIF stabilizes construct
COTSCOTS - Midshaft ORIF Benefits
Hook:COTS study showed ORIF gives better union but COmparable long-Term Score
NEERNEER - Lateral Clavicle Types
Hook:Type II = II ligaments torn (trapezoid + conoid) = Instability
2222-2-2 Rule for Midshaft Surgery
Hook:If shortening exceeds 2cm, decide within 2 weeks or double your trouble
Overview and Epidemiology
Clavicle fractures are among the most common orthopaedic injuries, representing approximately 4-5% of all fractures. The clavicle is a unique bone that serves as the only bony connection between the upper limb and the axial skeleton.
- Direct blow - fall onto the point of the shoulder (most common)
- Indirect - FOOSH (fall on outstretched hand) transmits force
- High-energy - motor vehicle accidents, sports injuries
- Young males (high-energy sports/trauma)
- Elderly (low-energy falls with osteoporosis)
The clavicle is S-shaped with the medial curve convex anteriorly and the lateral curve convex posteriorly. The junction of these curves (middle third) is the thinnest point and lacks ligamentous attachments, explaining the high fracture rate here.
Anatomy and Biomechanics
- First bone to ossify (5th week in utero)
- Last bone to fuse (medial physis closes 23-25 years)
- S-shaped: medial 2/3 convex anteriorly, lateral 1/3 convex posteriorly
- Middle third is the thinnest with no ligamentous attachments
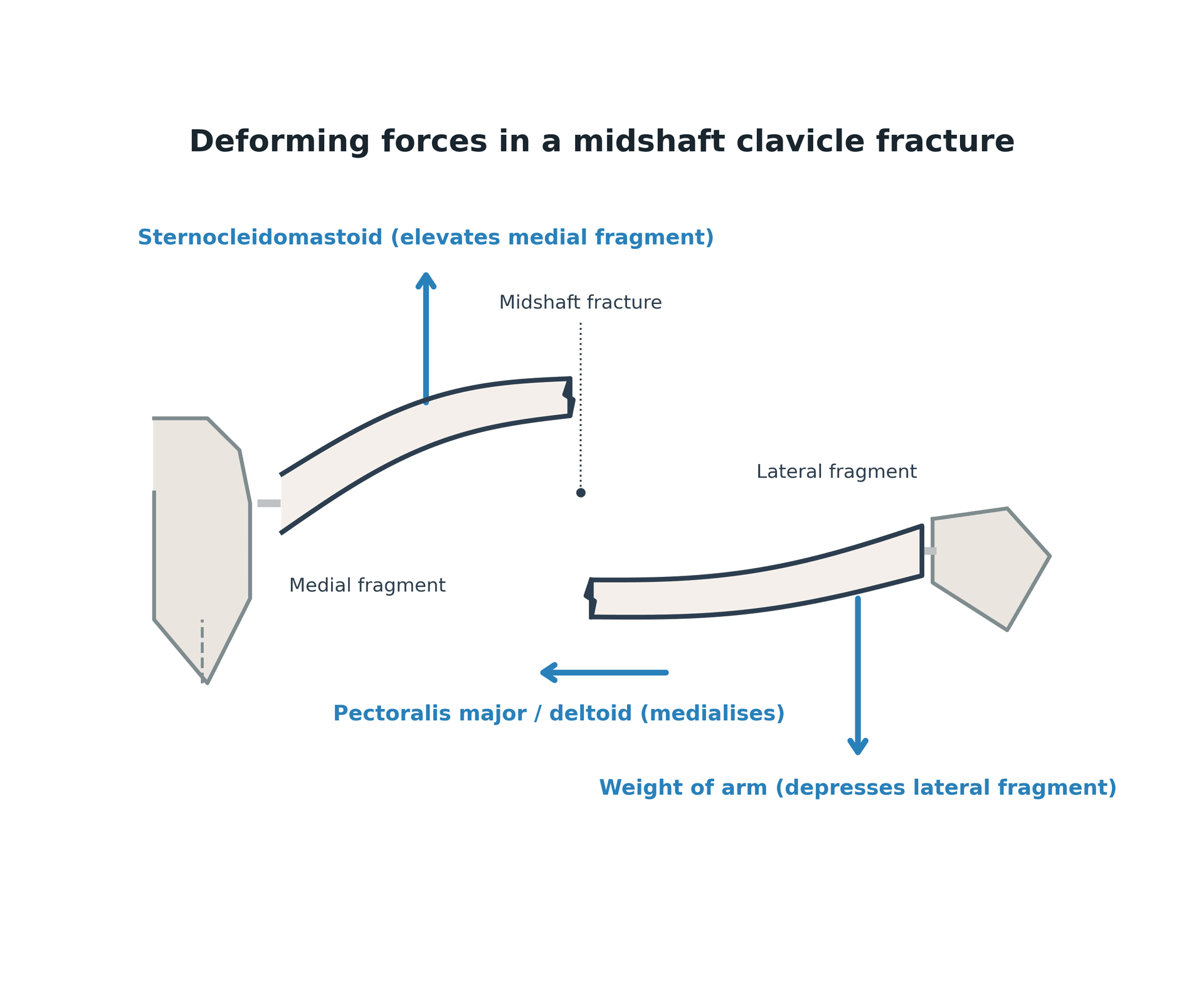
- SCM (sternocleidomastoid) - inserts medial third, elevates medial fragment
- Trapezius - inserts lateral third, may elevate lateral fragment
- Deltoid - originates from lateral third
- Pectoralis major - originates from medial third, depresses fragment
Subclavian vessels and brachial plexus pass directly posterior to the middle third. The subclavius muscle and clavipectoral fascia provide protection. Acute vascular injury rare but posterior medial displacement is dangerous.
Ligamentous structures:
- Coracoclavicular (CC) ligaments - trapezoid (lateral) and conoid (medial) - key stabilizers
- Acromioclavicular ligament - horizontal stability of AC joint
- Sternoclavicular ligaments - anchor medial clavicle
In midshaft fractures: medial fragment elevates (SCM pull) and retracts posteriorly (trapezius). Lateral fragment depresses (weight of arm) and medializes (pectoralis/deltoid). This creates the classic "step-off" deformity.
Vascular supply:
- Periosteal vessels (branches of suprascapular, thoracoacromial, internal thoracic)
- Nutrient artery enters near middle third
- Comminuted fractures disrupt blood supply - higher nonunion risk
"Floating shoulder" is best understood through Goss's superior shoulder suspensory complex (SSSC) - a bone-and-soft-tissue ring suspending the upper limb from the axial skeleton on two struts. The ring comprises the glenoid process, coracoid process, coracoclavicular ligaments, distal clavicle, acromioclavicular joint and acromion; the superior strut is the middle clavicle and the inferior strut is the lateral scapular body/spine. The clinical rule: a single disruption of the ring is usually stable and can be treated non-operatively, but a double disruption (two breaks in the ring, or a ring break plus both struts) destabilises the complex - the classic example being an ipsilateral midshaft clavicle fracture plus a scapular neck fracture ("floating shoulder"), where fixing the clavicle alone often restores enough stability to let the scapular neck heal. This framework, not the eponym, is what the examiner is after.
Classification Systems

Allman Classification (by location - most commonly used)
- Location
- Middle third
- Frequency
- 80%
- Key Features
- Between CC ligaments and costoclavicular ligament
- Location
- Lateral third
- Frequency
- 15%
- Key Features
- Lateral to CC ligaments
- Location
- Medial third
- Frequency
- 5%
- Key Features
- Medial to costoclavicular ligament
Middle third fractures occur at the junction of the two curves where the bone is thinnest and has no ligamentous attachments. This explains both the high incidence and propensity for displacement.


The adult displacement and shortening surgical thresholds do not transfer to children. The paediatric clavicle has enormous remodelling potential and a thick osteogenic periosteal sleeve, so the vast majority - including markedly displaced or shortened midshaft fractures - are treated non-operatively (sling, early motion) with reliable union and remodelling; greenstick patterns are common. Two specific entities to know: (1) the neonatal/obstetric clavicle fracture - the commonest fracture of birth (large baby, shoulder dystocia), presenting as pseudoparalysis or a lump, which must be distinguished from brachial plexus (Erb) palsy and from osteomyelitis or non-accidental injury, and which heals with simple support and no specific treatment; and (2) congenital pseudarthrosis of the clavicle - a painless, atraumatic, almost always right-sided mid-clavicular gap with rounded sclerotic bone ends and no callus, a developmental anomaly (not a fracture, and not the neurofibromatosis-associated lesion seen in the tibia) treated by excision, grafting and plating only if symptomatic. So in the child, think remodelling and recognise the two mimics rather than applying adult ORIF rules.
Clinical Presentation and Assessment
History:
- Mechanism (fall onto shoulder, direct blow, FOOSH)
- High vs low energy
- Hand dominance
- Occupation and activity level
- Associated injuries (floating shoulder, chest trauma)
Physical examination:
- Significance
- Displacement present
- Action Required
- Assess degree of shortening
- Significance
- Impending open fracture
- Action Required
- Urgent - relative surgical indication
- Significance
- Brachial plexus/vascular injury
- Action Required
- Urgent surgical exploration
- Significance
- Pneumothorax
- Action Required
- Chest X-ray, tube thoracostomy if needed
- Significance
- Floating shoulder
- Action Required
- Full shoulder girdle imaging
Neurovascular examination:
- Brachial plexus assessment (especially lateral cord - musculocutaneous, median)
- Radial, ulnar, median nerve function
- Distal pulses, capillary refill
- Signs of venous congestion
Look for floating shoulder (clavicle + scapula neck), AC joint injury, pneumothorax (especially with first rib fracture), and brachial plexus injury (particularly in high-energy trauma).
Signs of significant displacement:
- Obvious step-off deformity
- Shortening (compare to contralateral side)
- Tenting of skin
- Pain with any shoulder movement
Differential diagnosis:
- Distinguishing Features
- Tenderness over AC joint, step at the joint not the shaft, positive cross-body adduction
- Confirming Investigation
- AP and Zanca views, weighted views if needed
- Distinguishing Features
- Medial swelling, dysphagia or venous congestion if posterior
- Confirming Investigation
- CT with angiography for posterior displacement
- Distinguishing Features
- Pain and bruising over proximal humerus, restricted glenohumeral movement
- Confirming Investigation
- AP, scapular-Y and axillary radiographs
- Distinguishing Features
- High-energy mechanism, scapular tenderness, double disruption
- Confirming Investigation
- Full shoulder girdle imaging, CT
- Distinguishing Features
- Low-energy mechanism, antecedent pain, history of malignancy
- Confirming Investigation
- Radiographs for lytic lesion, staging and biopsy as indicated
- Distinguishing Features
- Age under 25 years, mimics SC dislocation as physis still open
- Confirming Investigation
- CT to differentiate from true SC dislocation
Investigations
Radiographic Examples

- 15-degree cephalic tilt provides best view
- Assess displacement, shortening, comminution
- Measure shortening by comparing to contralateral side
- Separates clavicle from overlying ribs/scapula
- Better assessment of displacement and comminution
Measure clavicle length on AP X-ray from sternal to acromial end. Compare to contralateral side. More than 2cm shortening is a key surgical threshold. CT provides more accurate measurement if needed.
When to order CT:
- Rationale
- Assess posterior displacement, vascular proximity
- Rationale
- Define CC ligament attachment, fracture pattern
- Rationale
- Define scapula fracture pattern for surgical planning
- Rationale
- Accurate shortening measurement, fragment assessment
- Indicated for medial fractures with posterior displacement
- Any concern for vascular injury (expanding hematoma, pulse deficit)
- Rule out pneumothorax
- Especially with first rib fracture or high-energy mechanism
Management

Conservative management:
Most clavicle fractures can be treated conservatively with excellent outcomes.
- Simple sling for comfort (arm sling preferred over figure-of-8)
- Ice, analgesia
- Gentle pendulum exercises when pain allows
- Wean from sling as pain allows
- Active ROM exercises below 90 degrees
- Avoid heavy lifting
- Progressive strengthening once clinical union
- Return to non-contact sports typically 8-12 weeks
- Contact sports delayed until radiographic union (12-16 weeks)
Simple arm sling is preferred over figure-of-8 brace. A Cochrane review showed no difference in outcomes, and figure-of-8 braces cause axillary discomfort and skin problems. Only advantage is cosmetic improvement of posture.
Surgical Technique
Plate and screws - gold standard for midshaft fractures
- Easier exposure
- Better cosmesis
- Plate prominence, hardware irritation common
- Less prominence
- Subcutaneous suture line
- More difficult exposure
- Protected from direct trauma
- 3.5mm reconstruction plate (can be contoured)
- Precontoured clavicle plates (anatomic)
- Locking plates for osteoporotic bone or comminution
Superior plating is most common but has higher hardware prominence. Anteroinferior plating is biomechanically similar with less prominence but technically more demanding. Both acceptable - surgeon preference.

PLATEPLATE - Surgical Indications
Hook:PLATE the clavicle when these indications are met
Complications
- Conservative Rate
- 5-15%
- Surgical Rate
- 1-2%
- Management
- Bone grafting, revision ORIF
- Conservative Rate
- Variable
- Surgical Rate
- Rare
- Management
- Accept most; osteotomy if symptomatic
- Conservative Rate
- N/A
- Surgical Rate
- 20-40%
- Management
- Hardware removal at union
- Conservative Rate
- N/A
- Surgical Rate
- 1-2%
- Management
- Antibiotics, debridement if deep
- Conservative Rate
- Rare
- Surgical Rate
- 0.5-1%
- Management
- Intraop recognition, vascular repair
- Conservative Rate
- Rare
- Surgical Rate
- 1-2%
- Management
- After hardware removal; wait 12 weeks
Nonunion:
Risk factors for nonunion:
- Displacement greater than 100%
- Shortening greater than 2cm
- Comminution
- Female sex
- Older age
- Smoking
- Refracture
Clavicle nonunion treatment: plate fixation + bone grafting (iliac crest or local autograft). Address biomechanical (length, alignment) and biological (vascularity, bone quality) factors.
Malunion:
- Shortening, angulation, and rotation
- Usually well tolerated
- Surgery only for symptomatic cases (shoulder dysfunction, cosmesis)
- Corrective osteotomy with plate fixation
Plate prominence is the most common reason for hardware removal (20-40% of patients). Counsel patients preoperatively. Anteroinferior plating may reduce this but is technically more demanding.
Postoperative Care and Rehabilitation
Post-ORIF protocol:
- Sling for comfort
- Gentle pendulum exercises
- No active elevation
- Wound care
- Wean sling
- Active assisted ROM
- Progress to active ROM as tolerated
- No lifting greater than 2-3kg
- Progressive strengthening
- Return to desk work usually possible
- No heavy lifting or contact sports
- Confirm radiographic union
- Return to full activities
- Contact sports typically 4-6 months
- Hardware removal if symptomatic (12+ months)
Key rehabilitation principles:
- Early pendulum exercises prevent stiffness
- Progressive loading only after clinical union
- Hardware removal is optional unless symptomatic
- Full sports clearance requires radiographic union
Athletes can return to non-contact sports at 8-12 weeks with clinical union and adequate ROM. Contact sports require radiographic union, typically 4-6 months. Elite athletes may have earlier return with protective padding.
Outcomes and Prognosis
Prognosis by fracture type:
- Conservative Union
- 95%+
- ORIF Union
- 98-99%
- Notes
- Conservative treatment preferred
- Conservative Union
- 85%
- ORIF Union
- 98%
- Notes
- ORIF faster union, similar function
- Conservative Union
- 90%+
- ORIF Union
- 95%+
- Notes
- Conservative preferred
- Conservative Union
- 67-78%
- ORIF Union
- 90-95%
- Notes
- ORIF strongly preferred
- Conservative Union
- 90%+
- ORIF Union
- 95%+
- Notes
- Conservative unless displaced posteriorly
Canadian Orthopaedic Trauma Society (COTS) 2007: RCT of 132 patients comparing plate fixation vs sling for completely displaced midshaft fractures. ORIF showed lower nonunion (2 of 62 vs 7 of 49), faster union (16.4 vs 28.4 weeks), and better Constant/DASH scores up to 1 year. The later network meta-analysis confirmed the functional advantage does not reach the minimal clinically important difference. Changed practice toward considering surgery for displaced fractures.
Factors affecting outcomes:
- Degree of shortening (more than 2cm worse outcomes)
- Smoking (delays union, increases complications)
- Age and bone quality
- Compliance with rehabilitation
- Patient expectations and activity demands
Guidelines, Registries & Global Practice
Global epidemiology
- Value
- Approximately 2.6-5%
- Source
- Population fracture series
- Value
- 65 of 75 injuries
- Source
- Nordqvist & Petersson 1995
- Value
- Male (sport/traffic mechanism)
- Source
- Nordqvist & Petersson 1995
- Value
- Midshaft approximately 80%, lateral approximately 15%, medial approximately 5%
- Source
- Allman / Robinson cohorts
- Value
- 6.2% (diaphyseal 4.5%, lateral 11.5%)
- Source
- Robinson 2004
The bimodal pattern - young men injured in sport or road trauma and older patients sustaining fragility injuries from low falls - is consistent across high-income population studies and shapes both management and counselling.
Guideline and society positions, side by side
- Position on displaced midshaft fractures
- Nonoperative care is the default; fixation reserved for absolute indications (open, neurovascular, skin compromise) and selected displaced fractures after shared decision-making
- Evidence basis
- RCT and meta-analysis evidence
- Position on displaced midshaft fractures
- No mandate for routine surgery; shared decision-making citing faster union and lower nonunion with surgery against hardware-related reoperation
- Evidence basis
- Level I RCTs
- Position on displaced midshaft fractures
- Predominantly nonoperative; surgery offered for high-risk displaced fractures and absolute indications, reflecting equivalence of long-term function
- Evidence basis
- Cochrane and RCT data
- Position on displaced midshaft fractures
- Individualised - operative fixation for completely displaced, shortened or comminuted fractures in active patients
- Evidence basis
- Network meta-analysis
Across all major bodies the recommendations have converged: surgery reliably improves union (number needed to treat approximately 10) and early function but does not deliver a patient-perceptible long-term functional gain, so the decision is shared and indication-led rather than mandatory.
Registry and high-level evidence
- The COTS multicentre RCT established lower nonunion and malunion with plate fixation of completely displaced fractures, but with hardware removal as the leading reoperation.
- The Axelrod network meta-analysis of 22 RCTs quantified union at 88.9% (nonoperative) versus 96.7% (operative), with functional differences below the minimal clinically important difference.
- The Nourian meta-analysis found superior and anteroinferior plating equivalent for union and function, with anteroinferior placement reducing symptomatic hardware and removal.
Global practice variation
- In high-resource settings, displaced fractures in athletes and manual workers are increasingly offered early fixation to shorten time to union and return to work, despite equivalent long-term function.
- In limited-resource settings, nonoperative management predominates given the low absolute nonunion risk and the cost, implant and theatre demands of fixation; this is an evidence-consistent choice rather than a compromise.
- Lateral Neer type II fractures attract a more uniformly operative stance worldwide because of their substantially higher nonunion risk.
MCQ Practice Points
Q: What percentage of clavicle fractures occur in the middle third? A: 80%. The middle third is the thinnest portion of the clavicle, at the junction of the two curves, and lacks ligamentous attachments - making it the most vulnerable to fracture.
Q: At what age does the medial clavicle physis close? A: 23-25 years. This is the last physis in the body to fuse. Injuries in young adults appearing as SC dislocations are often physeal fracture-separations.
Q: What shortening threshold is a key indication for ORIF of midshaft clavicle fractures? A: Greater than 2cm shortening. Along with 100% displacement, this is associated with higher nonunion rates and functional impairment.
Q: What was the key finding of the COTS study regarding operative vs non-operative treatment of displaced midshaft clavicle fractures? A: ORIF resulted in fewer nonunions (2 of 62 operative vs 7 of 49 nonoperative) and faster union, with no clinically important difference in functional scores at 1 year (the network meta-analysis confirmed the functional gain is below the MCID).
Q: Which Neer classification type of lateral clavicle fracture has the highest nonunion rate? A: Type II (22-33% nonunion). The CC ligament disruption leaves the medial fragment unstable and elevated by the trapezius.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old male cyclist presents after a fall onto his right shoulder. X-ray shows a displaced midshaft clavicle fracture with 2.5cm shortening and 100% displacement. He is a manual laborer. How would you manage this patient?”
“A 45-year-old woman presents with a lateral third clavicle fracture. X-rays show the fracture between the CC ligaments with significant displacement of the medial fragment. What is your assessment and management?”
“An 18-year-old presents with a medial clavicle injury after a rugby tackle. There is swelling at the sternoclavicular area, the patient reports difficulty swallowing, and the arm is held adducted. X-rays are difficult to interpret. What are your concerns and management?”
CLASSIFICATION
- Allman: I (80% middle), II (15% lateral), III (5% medial)
- Neer lateral: I (stable), II (unstable - CC disrupted), III (articular)
- Robinson: 2A (aligned), 2B (displaced) - key for prognosis
- Edinburgh: expanded Robinson - includes comminution assessment
KEY NUMBERS
- Greater than 2cm shortening = consider ORIF
- 15% nonunion rate for displaced midshaft (conservative)
- 22-33% nonunion for Neer Type II (lateral)
- 23-25 years = medial physis closure age
SURGICAL INDICATIONS
- Open fracture, neurovascular compromise
- Impending skin perforation (tenting)
- Shortening greater than 2cm, 100% displacement
- Neer Type II lateral fracture
- Floating shoulder (relative)
- Polytrauma needing early mobilization
COTS STUDY SUMMARY
- ORIF reduces nonunion: 2 of 62 vs 7 of 49 (COTS 2007)
- Faster union with surgery (16.4 vs 28.4 weeks)
- Better early Constant/DASH scores with ORIF
- Functional benefit below MCID - similar at 1 year (Axelrod NMA 2020)
SURGICAL OPTIONS
- Superior plate: easier exposure, more prominence
- Anteroinferior plate: less prominence, harder
- IM nail: smaller incision, migration risk
- Hook plate (lateral): needs removal at 3-6 months
TRAPS AND PEARLS
- Medial injury in less than 25yo = physeal, not SC dislocation
- Posterior medial displacement = CT angio, vascular risk
- Figure-of-8 no better than sling - sling preferred
- Floating shoulder = consider clavicle fixation
- Hook plate = plan for routine removal
Evidence Base
- Multicentre RCT of 132 patients with completely displaced midshaft fractures. Plate fixation reduced nonunion (2 of 62 operative vs 7 of 49 nonoperative) and symptomatic malunion (0 vs 9), shortened time to union (16.4 vs 28.4 weeks), and improved Constant and DASH scores at all time points up to 1 year.
- Prospective observational cohort of 868 nonoperatively treated clavicle fractures. Overall nonunion at 24 weeks was 6.2% (diaphyseal 4.5%, lateral 11.5%, medial 8.3%). Independent predictors of diaphyseal nonunion were lack of cortical apposition (displacement), comminution, female sex and advancing age.
- Network meta-analysis of 22 RCTs (1965 patients). Union at 1 year was 88.9% nonoperative versus 96.7% operative (NNT approximately 10 to avoid one nonunion). Functional gains with surgery did not reach the minimal clinically important difference for DASH; nonunion after nonoperative care was slightly above 10%.
- Meta-analysis of 34 studies (1494 patients). Union, nonunion, malunion and functional scores were equivalent for superior and anteroinferior plating, but superior plating had significantly more symptomatic hardware (17% vs 8%) and more frequent implant removal (11% vs 5%).
- Cochrane review of 3 trials (354 participants). Figure-of-eight bandage showed no functional advantage over a simple arm sling and caused more pain and discomfort; low-intensity pulsed ultrasound did not accelerate union.
- Population-based study (Malmo, Sweden) of all shoulder girdle injuries in one year. Clavicle fractures were the commonest shoulder girdle injury in children (65 of 75) and frequent in adults (67 of 181), with adult injuries significantly more common in men and predominantly caused by traffic and sport.