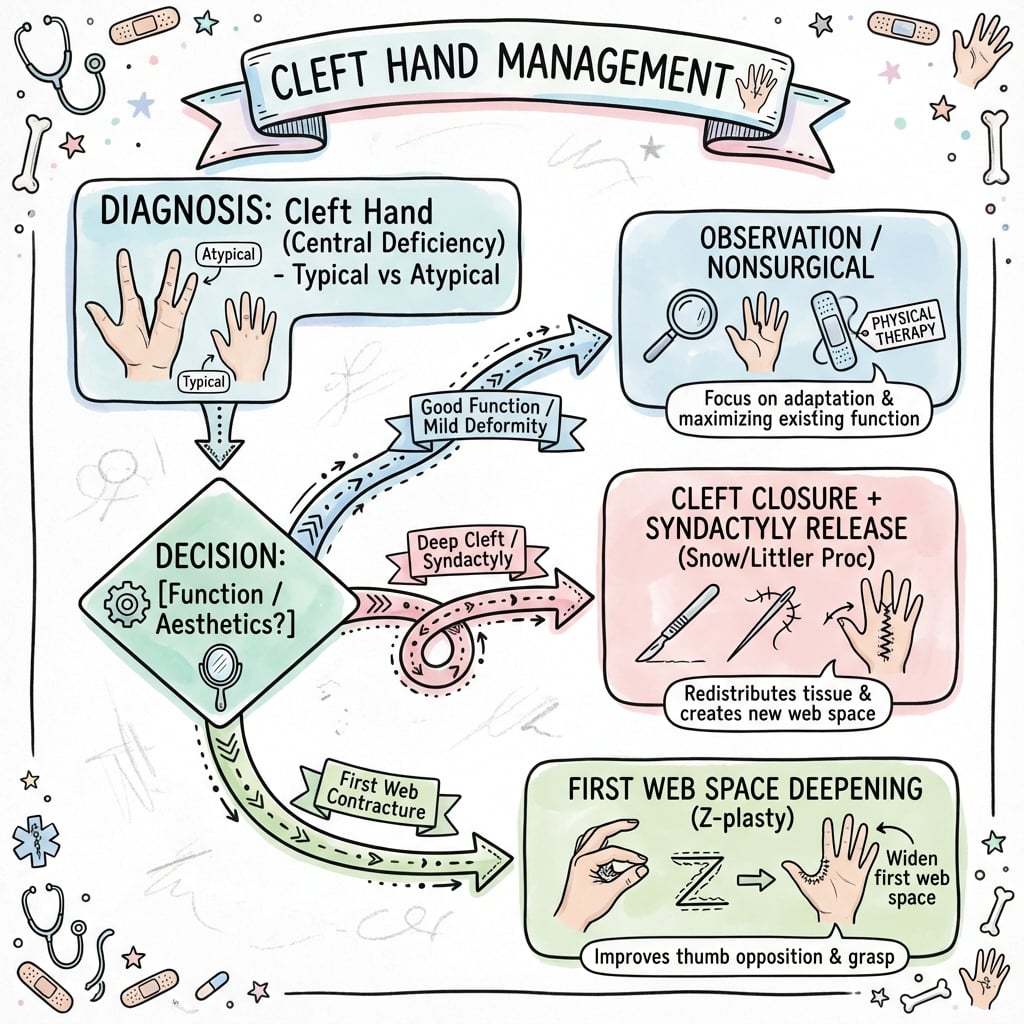
Central Ray Deficiency
- Typical Cleft: Isolated, sporadic, U-shaped, good first web, better function.
- Atypical Cleft: Syndromic, familial, V-shaped, poor first web, worse function.
- Manske-Halikis I-V: Based on thumb web (normal→suppressed) and cleft severity.
- EEC Syndrome: Ectrodactyly-Ectodermal dysplasia-Clefting - autosomal dominant.
- Surgical Goals: Close cleft, deepen first web, release syndactyly, maintain function.
- “Typical = U-shaped, good function, sporadic
- “Atypical = V-shaped, syndromic, familial
- “Snow-Littler procedure = cleft closure technique
- “EEC syndrome triad: limbs, skin/hair, facial cleft
- “First web space depth determines function
Shape: U-Shaped (Wide). First Web: Good/Normal. Inheritance: Sporadic (Non-syndromic). Function: Good.
Shape: V-Shaped (Deep/Narrow). First Web: Suppressed/Tight (Adducted thumb). Inheritance: Familial (Dominant) / Syndromic. Function: Poor.
EEC Syndrome: Ectrodactyly, Ectodermal dysplasia, Clefting. Prognosis: Atypical clefts = Worse functional outcome.
First Web Space: Deepening is MORE important than cleft closure for function.
Overview and Epidemiology
Cleft hand (also called ectrodactyly, split hand, or lobster claw deformity) is a congenital longitudinal deficiency characterized by the absence of one or more central rays (metacarpals and phalanges), creating a V-shaped or U-shaped cleft in the central portion of the hand.
Epidemiology
- Incidence: Split-hand/split-foot malformation (SHFM, the umbrella term encompassing cleft hand) occurs in approximately 1 in 8,500 to 1 in 25,000 newborns (Holder-Espinasse et al, Eur J Hum Genet 2019)
- Proportion of limb defects: SHFM accounts for approximately 15% of all limb reduction defects
- Bilateral: Both hands are frequently involved, and many patients have concurrent foot involvement (true split hand-split foot malformation)
- Gender: Broadly equal distribution male:female
- Typical vs Atypical: The historical typical/atypical split is descriptive; "atypical cleft hand" is now largely reclassified as symbrachydactyly (a transverse/dysplastic process) rather than a true central longitudinal deficiency
Genetics and Inheritance
- Inheritance: Most commonly autosomal dominant with incomplete penetrance; X-linked and autosomal recessive forms also occur (Holder-Espinasse et al, 2019)
- Recognised loci (SHFM1-6): SHFM1 at 7q21.2 (DLX5), SHFM2 at Xq26, SHFM3 at 10q24 duplication (the most frequently identified cause), SHFM4 at 3q27 (TP63), SHFM5 at 2q31 and SHFM6 (WNT10B, 12q13)
- EEC Syndrome: Autosomal dominant, caused by TP63 mutation (3q27 / SHFM4 locus)
Associated Syndromes
- EEC Syndrome (Ectrodactyly-Ectodermal dysplasia-Clefting): Most common
- SHFM (Split Hand-Split Foot Malformation): Isolated limb defects
- Other: Cornelia de Lange syndrome, Adams-Oliver syndrome
Embryology
- Develops during limb bud formation (4-8 weeks gestation)
- Failure of formation of central rays (index, middle, ring fingers)
- Zone of Polarizing Activity (ZPA) and Apical Ectodermal Ridge (AER) disruption
- Suppression or absence of central digital rays during differentiation
- First web space development affected in atypical forms
Anatomy and Pathophysiology
Normal Hand Development
- Digital Rays: 5 rays form from radial (thumb) to ulnar (small finger)
- Central Rays: Rays 2, 3, 4 (index, middle, ring) are central rays
- AER and ZPA: Control proximal-distal and radial-ulnar patterning
- Programmed Cell Death: Normal interdigital tissue apoptosis
Pathologic Anatomy in Cleft Hand
- Central Ray Absence: One or more of rays 2, 3, 4 are completely or partially absent
- Metacarpal Absence: May involve metacarpals, phalanges, or both
- Soft Tissue Cleft: V-shaped or U-shaped defect extends proximally
- Syndactyly: Border digits often joined (index-middle or ring-small)
- First Web Contracture: Variable suppression of thumb-index web space
Typical Cleft Anatomy
- U-Shaped Cleft: Wider, more shallow cleft
- Normal First Web: Good thumb-index web space preserved
- Central Deficiency Only: Isolated to central rays
- Better Function: Opposition and grasp relatively preserved
- Single Ray Absence: Often middle finger (ray 3) only
Atypical Cleft Anatomy
- V-Shaped Cleft: Narrow, deep cleft extending to carpus
- Suppressed First Web: Thumb-index web is tight, narrow, adducted
- Multiple Ray Absence: Often 2 or 3 central rays absent
- Transverse Bones: Abnormal transverse metacarpal elements
- Worse Function: Poor opposition and grasp
Key Anatomical Considerations
- First Web Space Depth: THE critical determinant of hand function
- Neurovascular Bundles: May have abnormal course around cleft borders
- Tendons: Extrinsic tendons may be absent or misdirected
- Thumb Position: May be radially deviated or adducted
- Border Digits: Often stiff, may have joint contractures
Classification Systems
Manske-Halikis Classification (Most Useful)
Principle: Based on first web space status - determines function and treatment.
- First Web Space
- Normal thumb web
- Cleft Description
- Central cleft only
- Function
- Good - normal pinch/grasp
- First Web Space
- Mildly narrowed
- Cleft Description
- Central cleft + mild web suppression
- Function
- Good - slightly reduced
- First Web Space
- Moderately narrowed
- Cleft Description
- Central cleft + moderate suppression
- Function
- Moderate - reduced pinch
- First Web Space
- Severely suppressed
- Cleft Description
- Deep cleft + severe web contracture
- Function
- Poor - minimal pinch
- First Web Space
- Absent (monodactyly)
- Cleft Description
- Single digit only (thumb or finger)
- Function
- Very poor - no opposition
Clinical Utility:
- Type I-II: May not require surgery (good function)
- Type III-IV: Surgery beneficial (improve function and appearance)
- Type V: Complex reconstruction or prosthetic consideration
Remember: The first web space is MORE important than the central cleft for function.
The Manske-Halikis system emphasizes functional assessment rather than just anatomic description.
Clinical Presentation
History
- Birth Presentation: Cleft visible at birth - obvious deformity
- Family History: Important to ask - atypical forms are familial
- Syndromic Features: Ask about skin/hair (ectodermal dysplasia), cleft palate
- Bilateral: Examine both hands AND both feet
- Developmental Milestones: Usually normal motor development
Physical Examination
Inspection
- Cleft Configuration: V-shaped vs U-shaped
- Number of Digits: Count present digits and identify missing rays
- First Web Space: Assess depth and width (CRITICAL for function)
- Syndactyly: Check for fusion of border digits
- Thumb Position: Assess for radial deviation or adduction contracture
Palpation
- Metacarpals: Palpate to determine which are present/absent
- Transverse Bones: Feel for abnormal transverse metacarpal elements (atypical)
- Soft Tissue: Assess tightness of first web space skin
- Neurovascular: Identify digital arteries/nerves (may be anomalous)
Functional Assessment (MOST IMPORTANT)
- Opposition: Can thumb oppose to remaining fingers?
- Pinch Strength: Assess tip pinch, key pinch, three-point pinch
- Grasp: Power grip capability with remaining digits
- First Web Span: Measure distance between thumb-finger when maximally abducted
- Activities: Can child manipulate objects, feed self, grasp toys?
Red Flags Requiring Syndrome Workup
- Sparse Hair/Teeth: Suggests ectodermal dysplasia (EEC syndrome)
- Cleft Lip/Palate: EEC syndrome
- Cleft Feet: Split hand-split foot malformation (SHFM)
- Multiple Limb Defects: Consider broader genetic syndrome
- Developmental Delay: Suggests syndromic etiology
Associated Findings
- Cleft Feet: 60% have split foot deformity
- Syndactyly: Common in border digits
- Polydactyly: May coexist with central ray absence
- Thumb Hypoplasia: May have underdeveloped thumb
- Stiffness: Border digits often have joint contractures
A classic examiner question is "should you operate, and what do you tell the parents?" - and the answer hinges on a paradox unique to the cleft hand:
- Flatt's aphorism: the typical cleft hand is famously "a functional triumph and a social disaster" - it usually works remarkably well (good opposition and grasp because the first web is preserved) but looks abnormal and attracts attention.
- Implication for surgery: in a well-functioning (Manske I-II / typical) cleft hand, surgery is largely for appearance, not function - so you are operating on a working hand, with real risk of stiffness, web contracture and neurovascular injury to functioning border digits. The decision must be a careful shared decision weighing cosmesis/social factors against the risk of making a good hand worse.
- Contrast - when function does drive surgery: this is the opposite of the atypical/severe (Manske III-V) hand, where the first web is suppressed and surgery genuinely improves function - there the indication is functional, not cosmetic.
- Counselling points: most children adapt and develop excellent compensatory function; address the family's distress and social concerns explicitly; avoid over-promising a "normal-looking" hand; and time cosmetic surgery before school-age social awareness if it is chosen.
Exam point: state Flatt's "functional triumph, social disaster" - in the typical/good-function cleft hand surgery is mainly cosmetic and optional (don't make a working hand worse), whereas in the first-web-suppressed hand surgery is functional and indicated.
Investigations
Radiographic Assessment
Plain Radiographs (Essential)
- AP and Lateral Views: Document bony anatomy
- Identify Present Rays: Determine which metacarpals/phalanges present
- Carpal Bones: May have carpal anomalies in atypical forms
- Transverse Bones: Look for abnormal transverse metacarpal elements
- Syndactyly: Assess bony vs soft tissue fusion
Findings on X-ray
- Typical: Usually absence of middle finger ray (ray 3) only
- Atypical: Multiple ray absence, transverse bones, carpal anomalies
- First Metacarpal: May be short or deviated radially
- Phalanges: May have hypoplastic or absent phalanges
Genetic Testing
- Indicated if: Familial pattern, syndromic features, bilateral involvement
- TP63 Gene: EEC syndrome mutation
- Chromosomal Microarray: Identify deletions/duplications
- Genetic Counseling: Essential for familial cases
Syndromic Workup (If Indicated)
- Skin/Hair/Teeth Assessment: Ectodermal dysplasia features
- Craniofacial Evaluation: Cleft lip/palate assessment
- Foot Examination: Look for cleft feet
- Ophthalmology: Eye anomalies in some syndromes
- Audiology: Hearing assessment if syndromic
Functional Assessment Tools
- Hand Function Tests: Age-appropriate functional testing
- Grip/Pinch Strength: Objective measurements (if child cooperative)
- Video Recording: Document baseline function before surgery


Differential Diagnosis
Cleft hand must be distinguished from other central and transverse failures of formation, because management and prognosis differ markedly. The single most important modern distinction is between true central longitudinal deficiency (cleft hand) and symbrachydactyly of the cleft/atypical type, which is a transverse/dysplastic process and follows symbrachydactyly principles.
- Pattern of deficiency
- Central rays (2-4) absent, V- or U-shaped cleft
- Distinguishing features
- Well-formed border digits, transverse metacarpal bones may be present, foot often involved
- Laterality / inheritance
- Often bilateral; frequently familial / autosomal dominant
- Pattern of deficiency
- Transverse arrest with short or absent central digits
- Distinguishing features
- Nubbins / ectodermal remnants, short fingers, no familial pattern, foot usually spared
- Laterality / inheritance
- Almost always unilateral; sporadic
- Pattern of deficiency
- Amputation-like loss distal to a transverse level
- Distinguishing features
- No proximal digital elements beyond the arrest, may have nubbins
- Laterality / inheritance
- Unilateral; sporadic
- Pattern of deficiency
- Acrosyndactyly, distal ring constrictions, irregular digit loss
- Distinguishing features
- Constriction grooves, distal fusion, lymphoedema; no metacarpal cleft
- Laterality / inheritance
- Unilateral or asymmetric; sporadic, non-genetic
- Pattern of deficiency
- Extra (not absent) central rays, often hidden within syndactyly
- Distinguishing features
- Excess rather than deficient tissue, HOXD13 in synpolydactyly
- Laterality / inheritance
- Often bilateral; autosomal dominant
The classic exam trap is calling a unilateral, sporadic, nubbin-bearing hand with a central gap a "cleft hand" — if it is unilateral, non-familial and the foot is spared, think symbrachydactyly (cleft type), not true central longitudinal deficiency.
Management Algorithm
Treatment Goals (In Order of Priority)
1. Function First
- Maximize opposition capability (thumb-finger pinch)
- Improve grasp and release
- Deepen first web space if suppressed
2. Appearance Second
- Close cleft for cosmetic improvement
- Create more normal hand contour
- Improve social acceptance
3. Growth Preservation
- Maintain growth plates during surgery
- Avoid damage to viable digits
Conservative Management
Observation (Acceptable For)
- Manske Type I: Good function, normal first web - surgery optional
- Manske Type II: Mild impairment - may not require surgery
- Unilateral with Good Bilateral Hand Function: Non-dominant hand may not need surgery
Occupational Therapy
- Adaptive Strategies: Teach compensatory techniques
- Strengthening: Maximize function of existing digits
- First Web Stretching: If mild contracture present
- ADL Training: Feeding, dressing, writing adaptations
Surgical Management Principles
Timing: 12-18 months optimal
- Early enough to integrate before fine motor development
- Late enough for safe anesthesia and tissue handling
- Before social awareness (2-3 years)
Goals of Surgery:
- Close the cleft (improve appearance, prevent trauma to cleft margins)
- Deepen first web space (improve opposition and grasp - MOST IMPORTANT)
- Release syndactyly (if present in border digits)
- Maintain viability (preserve neurovascular supply to digits)
Cleft hand is frequently part of split-hand/split-foot malformation, so the feet are commonly involved too - but the management principle is the opposite of the hand, which is a favourite exam contrast:
- The foot is usually left alone: a cleft (split) foot is generally well tolerated - children walk well and the foot is weight-bearing, not precision-manipulating, so there is no equivalent of the all-important first web to reconstruct. The default is non-operative: accommodative/extra-depth footwear, custom shoes or simple insoles.
- When the foot is operated on: surgery is reserved for shoe-fitting problems and progressive deformity - a very wide forefoot that won't fit footwear (forefoot-narrowing/cleft closure), a protruding medial ray or hallux varus, or a deep cleft with skin breakdown. The goal is a plantigrade, shoeable foot, not fine function.
- The contrast to remember: in the hand you operate to restore function (the first web) and appearance; in the foot function is rarely the problem, so you intervene mainly for footwear/cosmesis - and many cleft feet need no surgery at all.
- Screen and counsel: always examine both feet (and the contralateral hand), and use foot involvement as a prompt for genetic assessment (SHFM/EEC).
Exam point: a cleft foot is a different problem from a cleft hand - it is usually managed non-operatively (footwear), with surgery only for a foot that won't fit a shoe or has progressive deformity, because the foot bears weight rather than performing precision grip.
Surgical Techniques
Snow-Littler Cleft Closure Procedure
Classic technique for closing cleft and narrowing hand.
Indications
- Manske Type I-III cleft hand
- Wide cleft requiring closure
- Good first web space (or mild narrowing)
Contraindications
- Severe first web suppression (Manske IV-V) - first web deepening is priority
- Monodactyly (Type V) - insufficient tissue
Surgical Steps
1. Skin Incision
- Longitudinal incision along ulnar border of radial digit
- Longitudinal incision along radial border of ulnar digit
- Design opposing flaps to close cleft in zigzag fashion
2. Soft Tissue Dissection
- Identify and preserve neurovascular bundles to border digits
- Excise any rudimentary central ray tissue if present
- Preserve periosteum of metacarpals
3. Transverse Bone Resection (Key Step)
- If abnormal transverse metacarpal bone present: resect it
- Closes gap between metacarpal heads
- Allows approximation of border digits
4. First Web Deepening (If Needed)
- Release tight first web space if suppressed
- May use Z-plasty or four-flap Z-plasty
- Deepen web to at least level of metacarpal necks
5. Cleft Closure
- Approximate border digits by closing soft tissue
- Use opposing skin flaps in zigzag pattern (breaks scar contracture line)
- May need skin grafting if excessive tension
6. Syndactyly Release (If Present)
- Release fused border digits if syndactyly present
- Use zigzag incisions and skin grafts as needed
Technical Pearls
- First web FIRST: Always address first web before closing cleft
- No tension: Avoid tight closure - use skin grafts if needed
- Preserve nerves: Neurovascular bundles may have abnormal course
- Zigzag incisions: Prevent linear scar contracture
Postoperative Care
- Splint in position of function for 3-4 weeks
- Gentle range of motion exercises after splint removal
- Occupational therapy for strengthening and ADL training
This procedure is the gold standard for cleft closure in functional hands.
Complications
Intraoperative Complications
- Neurovascular Injury: Anomalous NV bundle course increases risk (1-2%)
- Excessive Bleeding: Difficult hemostasis in vascular anomalies
- Inadequate Release: Incomplete first web deepening
- Skin Flap Necrosis: Tension or poor design
Early Postoperative Complications (Less than 6 weeks)
- Flap Necrosis: 2-5% incidence - poor flap design or tension
- Infection: 1-3% - treat with antibiotics, may need debridement
- Hematoma: Rare - evacuate if compressing neurovascular structures
- Wound Dehiscence: More common if excessive tension during closure
- Skin Graft Loss: 5-10% of grafts may fail (syndactyly release)
Late Complications (More than 6 weeks)
- Web Space Contracture Recurrence: 10-20% - most common complication
- Scar Contracture: Linear scars contract - use Z-plasties to prevent
- Stiffness: Border digits may become stiff (5-10%)
- Growth Disturbance: If physis injured during surgery (rare with careful technique)
- Cold Intolerance: Vascular insufficiency in border digits
- Neuroma: If nerve transected or entrapped in scar
Functional Outcomes
Good Outcomes (Typical Cleft)
- Near-normal hand function achieved in 70-80%
- Good cosmetic result
- Improved opposition and grasp
Fair Outcomes (Atypical Cleft)
- Function improved but not normal in 50-60%
- First web space may re-contract requiring revision
- Multiple surgeries often needed
Poor Outcomes
- Severe first web contracture recurrence: 10-20% (especially atypical)
- Stiffness limiting function: 5-10%
- Neurovascular compromise: 1-2%
Revision Surgery
- Indications: Web space re-contracture, inadequate initial correction, scar contracture
- Timing: Wait at least 6-12 months for scar maturation
- Techniques: Repeat Z-plasty, skin grafting, free flap coverage
- Success: Lower success rate than primary surgery
Postoperative Care and Rehabilitation
Immediate Postoperative Period (0-2 weeks)
- Immobilization: Well-padded splint in position of function
- Thumb Position: Abducted if first web deepened
- Elevation: Keep hand elevated to reduce swelling
- Pain Management: Acetaminophen, avoid NSAIDs (may increase bleeding)
- Wound Care: Keep dressing clean and dry
- First Dressing Change: 7-10 days (or earlier if concerns)
Early Rehabilitation (2-6 weeks)
- Splint Removal: 3-4 weeks post-op
- Gentle ROM: Start passive range of motion exercises
- No Forceful Stretching: Allow tissues to heal before aggressive therapy
- Scar Massage: Begin gentle massage once incisions healed
- Occupational Therapy: Initiate therapy for hand function training
Late Rehabilitation (6 weeks - 6 months)
- Active ROM: Progress to active exercises and strengthening
- First Web Maintenance: Aggressive stretching to prevent re-contracture
- Functional Activities: Encourage use in age-appropriate play and ADLs
- Night Splinting: May use abduction splint at night for 3-6 months
- Scar Management: Silicone gel sheets, massage, moisturization
Long-Term Follow-Up
- Growth Monitoring: Annual follow-up through skeletal maturity
- Functional Assessment: Assess hand function at each visit
- Revision Planning: Identify need for further surgery as child grows
- Psychosocial Support: Address appearance concerns, school integration
Occupational Therapy Protocol
Phase 1 (Weeks 3-6)
- Gentle passive ROM
- Edema control
- Scar management initiation
Phase 2 (Weeks 6-12)
- Active ROM exercises
- Strengthening with therapy putty
- Fine motor skill development
Phase 3 (Months 3-12)
- Advanced strengthening
- Bilateral hand coordination activities
- Writing/drawing skills (age-appropriate)
- Adaptive equipment trial if needed
Guidelines, Registries & Global Practice
Global epidemiology
- Split-hand/split-foot malformation (SHFM), the umbrella entity for cleft hand, affects approximately 1 in 8,500 to 1 in 25,000 newborns and represents about 15% of all limb reduction defects (Holder-Espinasse et al, Eur J Hum Genet 2019).
- Inheritance is most often autosomal dominant with incomplete penetrance; this drives the need for genetic counselling and examination of relatives in apparently isolated cases.
- Cleft hand is a central longitudinal deficiency in the IFSSH-endorsed OMT classification (Tonkin et al, J Hand Surg Am 2013).
Guidance and standards, side by side
There are no disease-specific randomised guidelines for cleft hand; practice is built on classification systems and specialist consensus. Standards that genuinely shape practice are summarised below.
- Position relevant to cleft hand
- Cleft hand classified as central longitudinal deficiency; standard global nomenclature
- Evidence basis
- Consensus + reliability study, 101 patients (Level IV)
- Position relevant to cleft hand
- Treatment driven by thumb-web status (types I-V); web reconstruction prioritised over cleft closure
- Evidence basis
- Original cohort of 46 hands (Level IV)
- Position relevant to cleft hand
- Surgery individualised to function; first-web deepening, cleft closure and syndactyly release typically 1-2 years of age; non-operative care acceptable when function is good
- Evidence basis
- Expert consensus / case series (Level IV-V)
- Position relevant to cleft hand
- Offer TP63 / chromosomal microarray testing and counselling for familial, bilateral or syndromic (EEC, SHFM) presentations
- Evidence basis
- Guideline-level genetic practice
Registry evidence
There is no dedicated international cleft-hand registry, and joint-replacement registries (NJR, AJRR, AOANJRR, SHAR) do not apply. Population-level data derive instead from congenital anomaly surveillance networks (for example EUROCAT in Europe and the ICBDSR international clearinghouse), which capture SHFM among limb reduction defects and underpin the 1 in 8,500-25,000 incidence figure.
Global practice variation
- High-resource settings: early multidisciplinary assessment (hand surgery, plastics, genetics, occupational therapy), functional surgery individualised to thumb-web status, and access to four-flap Z-plasty, microsurgical toe-to-hand transfer and pollicization for severe cases.
- Limited-resource settings: emphasis on the highest-yield functional interventions (first-web deepening, syndactyly release) with less reliance on microsurgical reconstruction; genetic testing and prosthetics may be unavailable.
- Across all settings the shared principle is constant: function is governed by the thumb web, so web reconstruction takes priority over cosmetic cleft closure.
Manske-Halikis Classification: Surgical Classification of Central Deficiency by Thumb Web
OMT (Oberg-Manske-Tonkin) Classification of Congenital Upper Limb Anomalies
EEC Syndrome: Clinical Spectrum in 24 Cases
Genetics of Split-Hand/Foot Malformation (SHFM): Loci and Inheritance
Snow-Littler Procedure: Clinical Experience and Outcomes
At a Glance
Cleft hand (ectrodactyly) is a central longitudinal deficiency characterized by absence of one or more central rays, creating a V-shaped cleft. Classified as typical (sporadic, U-shaped cleft, good first web, better function) or atypical (syndromic/familial, V-shaped cleft, poor first web, worse function). Manske-Halikis classification (I-V) grades severity based on thumb web status and central defect. Associated with EEC syndrome (ectrodactyly-ectodermal dysplasia-clefting). Treatment focuses on functional reconstruction: cleft closure (Snow-Littler procedure), first web deepening, and syndactyly release at 12-18 months. First web space depth is the key determinant of function.
- First Web Status
- Normal thumb web
- Treatment Priority
- Cleft closure only (if desired)
- Timing
- 12-18 months
- First Web Status
- Mild narrowing
- Treatment Priority
- Cleft closure + web release
- Timing
- 12-18 months
- First Web Status
- Moderate suppression
- Treatment Priority
- First web deepening priority
- Timing
- 12-18 months
- First Web Status
- Severe suppression
- Treatment Priority
- Complex reconstruction required
- Timing
- Staged procedures
- First Web Status
- Absent (monodactyly)
- Treatment Priority
- Consider pollicization vs prosthesis
- Timing
- 18-24 months
CLEFTCLEFT Hand Features
Hook:CLEFT: Central ray absent in Longitudinal deficiency, EEC syndrome association, First web critical, Typical better than atypical
TYPICALTYPICAL Cleft Features (Better)
Hook:TYPICAL = Type better, U-shaped, Preserved web, Isolated, Chance (sporadic), Alone
EECEEC Syndrome Triad
Hook:EEC: Ectrodactyly (limbs), Ectodermal dysplasia (skin/hair/teeth), Clefting (facial)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 15-month-old child is referred with unilateral cleft hand. On examination, there is a U-shaped cleft with absence of the middle finger. The first web space is normal depth. The thumb and index finger are separate, and the ring and small fingers show simple syndactyly. X-ray confirms isolated absence of ray 3. Parents are asking about treatment options.”
“An 18-month-old presents with bilateral cleft hands. Both hands show V-shaped clefts extending to the carpus with absence of rays 2, 3, and 4. The first web spaces are severely narrowed with the thumbs held in adduction. The child cannot oppose the thumbs to the small fingers. The child also has sparse hair and bilateral cleft lip. X-rays show multiple central ray absence and abnormal transverse metacarpal bones. What is your assessment and management?”
“A 2-year-old child has a cleft hand with only a single central digit present (small finger). The thumb and all other rays are absent. X-ray confirms single 5th ray only. The parents are distressed and asking if the child will be able to use the hand. How would you manage this case?”
Classification
- Typical (70%): U-shaped, sporadic, normal first web, good function
- Atypical (30%): V-shaped, familial/syndromic, poor first web, worse function
- Manske I: Normal first web - surgery optional
- Manske II: Mild narrowing - good prognosis
- Manske III: Moderate suppression - surgery beneficial
- Manske IV: Severe suppression - complex reconstruction
- Manske V: Monodactyly - pollicization vs observation
Key Anatomy
- Central ray absence (rays 2, 3, 4) - index, middle, ring fingers
- First web depth = MOST important functional determinant
- Transverse metacarpal bones in atypical forms
- Neurovascular bundles may have anomalous course
- Border digits often have syndactyly
EEC Syndrome
- Ectrodactyly (cleft hand/foot) - 90% have limb defects
- Ectodermal dysplasia (sparse hair, absent teeth, dry skin)
- Clefting (cleft lip/palate)
- TP63 gene mutation - autosomal dominant
- Multidisciplinary care essential
Surgical Principles
- Timing: 12-18 months optimal (before fine motor development)
- FIRST WEB DEEPENING is more important than cleft closure for function
- Snow-Littler: classic cleft closure technique
- Four-flap Z-plasty: gold standard for first web deepening
- Syndactyly release: separate fused border digits
Key Numbers
- Incidence: approximately 1 in 8,500-25,000 (SHFM, Holder-Espinasse 2019)
- Bilateral: hands frequently both involved
- Cleft feet: 60% also have split foot
- Surgery timing: 12-18 months
- Good outcomes: 70-80% typical, 50-60% atypical
Complications
- Web contracture recurrence: 10-20% (most common, especially atypical)
- Flap necrosis: 2-5% (tension, poor design)
- Neurovascular injury: 1-2% (anomalous anatomy)
- Stiffness: 5-10% of border digits
- Revision surgery: needed in 15-20% of atypical clefts
VIVA ESSENTIALS
- Typical vs Atypical FIRST - determines prognosis and approach
- First web depth determines function - prioritize this over cleft closure
- Screen for EEC syndrome: sparse hair, cleft palate, dry skin, absent teeth
- Manske Type I-II may not need surgery - counsel about optional nature
- Atypical clefts: first web deepening BEFORE cleft closure
- Bilateral cases: stage procedures 3-6 months apart
References
-
Tonkin MA, Tolerton SK, Quick TJ, et al. Classification of congenital anomalies of the hand and upper limb: development and assessment of a new system. J Hand Surg Am. 2013;38(9):1845-1853.
-
Manske PR, Halikis MN. Surgical classification of central deficiency according to the thumb web. J Hand Surg Am. 1995;20(4):687-697.
-
Buss PW, Hughes HE, Clarke A. Twenty-four cases of the EEC syndrome: clinical presentation and management. J Med Genet. 1995;32(9):716-723.
-
Barsky AJ. Cleft hand: classification, incidence, and treatment. Review of 149 cases. J Bone Joint Surg Am. 1964;46:1707-1720.
-
Miura T, Nakamura R, Tamura Y. Long-term follow-up of cleft hands: a review of 40 clefts in 25 patients. J Hand Surg Am. 1990;15(5):739-743.
-
Ogino T, Minami A, Fukuda K, et al. Congenital anomalies of the upper limb among the Japanese in Sapporo. J Hand Surg Br. 1986;11(3):364-371.
-
Nutt JN, Flatt AE. Congenital central hand deficiency: a classification based on anatomical patterns and treatment. J Hand Surg Br. 1981;6(1):48-58.
-
Blauth W, Borisch N. Cleft hands: classification and incidence. Handchir Mikrochir Plast Chir. 1990;22(1):2-7.
-
Bouvet JP, Lemerle P, Lortat-Jacob A. Le traitement des mains botes centrales (central deficiency). Ann Chir Plast. 1980;25(3):240-247.
-
Al-Qattan MM, Al-Thunayan A, De Cordier M, et al. Classification of the typical form of symbrachydactyly. J Hand Surg Br. 1998;23(6):801-804.
-
Snow JW, Littler JW. Surgical treatment of cleft hand. Plast Reconstr Surg. 1967;40(5):413-418.
-
Buck-Gramcko D. Pollicization of the index finger: method and results in aplasia and hypoplasia of the thumb. J Bone Joint Surg Am. 1971;53(8):1605-1617.
-
Flatt AE. The Care of Congenital Hand Anomalies. 2nd ed. St Louis: Quality Medical Publishing; 1994.
-
Oberg KC, Feenstra JM, Manske PR, et al. Developmental biology and classification of congenital anomalies of the hand and upper extremity. J Hand Surg Am. 2010;35(12):2066-2076.
-
Kay SPJ, McCombe D, Kozin SH, et al. Deformities of the hand and fingers. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, eds. Green's Operative Hand Surgery. 7th ed. Philadelphia: Elsevier; 2017:1267-1316.
-
Holder-Espinasse M, Jamsheer A, Escande F, et al. Duplication of 10q24 locus: broadening the clinical and radiological spectrum. Eur J Hum Genet. 2019;27(4):525-534. PMID: 30622331.
-
Rider MA, Grindel SI, Tonkin MA, Wood VE. An experience of the Snow-Littler procedure. J Hand Surg Br. 2000;25(4):376-381. PMID: 11058008.
-
Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009;25(2):157-170. PMID: 19380058.
Further Reading
- Tonkin MA. Failure of differentiation part II: Cleft hand. Hand Clin. 2009;25(2):195-213.
- Goldfarb CA, Manske PR, Busa R, et al. Upper-extremity phocomelia reexamined: a longitudinal dysplasia. J Bone Joint Surg Am. 2005;87(12):2639-2648.
- Elliott AM, Evans JA. Genotype-phenotype correlations in mapped split hand foot malformation (SHFM) patients. Am J Med Genet A. 2006;140(13):1419-1427.