Guideline Development | GRADE | Implementation | Critical Appraisal
- Clinical Practice Guideline (CPG): Systematically developed statements to assist practitioner and patient decisions about appropriate care for specific clinical circumstances.
- GRADE System: Separates evidence quality (High/Moderate/Low/Very Low) from recommendation strength (Strong/Weak).
- Strong Recommendation: Clinicians should follow in most patients. Requires large benefit, high-quality evidence, or ethical imperative.
- Weak Recommendation: Different choices for different patients. Requires shared decision-making based on patient values.
- Implementation Gap: Guidelines often not followed in practice due to barriers (awareness, agreement, adoption, adherence).
- “Strong recommendation does NOT always require high-quality evidence (can have low quality if large effect)
- “Guideline development panels should be multidisciplinary and free from conflicts of interest
- “AGREE II tool assesses guideline quality across 6 domains (scope, stakeholder involvement, rigor, clarity, applicability, independence)
- “Guidelines are population-level tools - they inform, but never override, individualised clinical judgement and shared decision-making
- “International guidelines require local adaptation using regional registry data (AOANJRR, NJR, AJRR) and resource setting
Do not state that a strong recommendation requires high-quality evidence. GRADE explicitly decouples the two - a strong recommendation can rest on low-quality evidence when the effect is large, harm is minimal, or there is an ethical imperative. Reciting this decoupling correctly is a high-yield mark.
Overview
Introduction
Clinical practice guidelines (CPGs) are systematically developed statements that link the best available evidence to explicit, actionable recommendations for specific clinical circumstances. They sit at the junction of evidence-based medicine, implementation science and medicolegal practice, and are a recurring theme in basic-science and clinical vivas because they test whether a candidate can appraise evidence, not merely recall it.
The modern exam-relevant understanding rests on three pillars: how a guideline grades its evidence and recommendations (GRADE), how its methodological quality is appraised (AGREE II), and why good guidelines still fail at the bedside (implementation science). A consultant-level answer treats a guideline as a population-level tool that informs but never dictates the care of the individual in front of you.
Principles and Core Concepts
The Three Pillars
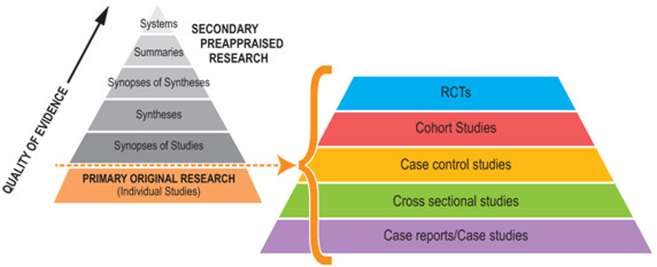
Grades evidence quality (High/Moderate/Low/Very Low) separately from recommendation strength (Strong/Weak). RCTs start High, observational studies start Low, then are up- or downgraded by explicit factors.
Appraises a guideline's methodological quality across 6 domains and 23 items. The rigor of development domain best reflects whether the guideline is truly evidence-based.
A high-quality guideline changes nothing unless it changes practice. Passive dissemination is weak; active, barrier-matched strategies (audit and feedback, reminders, decision support) drive uptake.
Key Definitions
- Strong recommendation - most informed patients would choose this option; clinicians can apply it to most patients and use it as a quality indicator. Worded "we recommend".
- Weak (conditional) recommendation - choices vary with patient values; requires shared decision-making and should not be used as a rigid quality measure. Worded "we suggest".
- Living guideline - continuously surveilled and updated as new evidence emerges, rather than on a fixed 3-5 year cycle.
GRADE System in Depth
Quality of Evidence
Four Levels: High, Moderate, Low, Very Low
Determining Starting Quality
RCT: Start at HIGH quality
Observational Study: Start at LOW quality
Then Apply Modifiers: Downgrade or upgrade based on factors.
This establishes baseline before applying judgment.
Recommendation Strength
Two Levels: Strong or Weak (for or against)
- Strong Recommendation
- We recommend... / Clinicians should...
- Weak Recommendation
- We suggest... / Clinicians might consider...
- Strong Recommendation
- Most patients would want this intervention
- Weak Recommendation
- Different choices for different patients based on values
- Strong Recommendation
- Most patients should receive this intervention
- Weak Recommendation
- Engage in shared decision-making, individualize
- Strong Recommendation
- Can be used as performance measure or quality indicator
- Weak Recommendation
- Should NOT be used as performance measure (patient choice matters)
Wording signals strength - surgeons must recognize difference.
RIIIPGRADE Downgrade Factors - RIIIP
Hook:Each factor can drop quality by 1 or 2 levels. The mirror-image upgrade factors (large effect, dose-response, opposing residual confounding) apply mainly to observational data.
Appraising Guideline Quality
AGREE II Tool
Purpose: Assess methodological rigor and transparency of guidelines.
Six Domains (23 items total):
Domain 1: Scope and Purpose
Questions:
- Are objectives clearly described?
- Are health questions covered by guideline specified?
- Is target population clearly described?
Why Important: Clarity on who guideline applies to prevents misapplication.
Well-defined scope prevents guideline creep.
Scoring: Each item rated 1-7. Domain scores calculated as percentage of maximum possible.
Overall Assessment: Would you recommend this guideline for use? Yes / Yes with modifications / No
AGREE II is the gold standard for guideline appraisal.
Implementation and Barriers
Why Guidelines Fail
- Example
- Clinicians unaware guideline exists
- Solution
- Active dissemination: conferences, emails, clinical reminders
- Example
- Clinicians disagree with recommendations
- Solution
- Local adaptation, opinion leader endorsement, involve skeptics in process
- Example
- Requires resources or system changes not available
- Solution
- Simplify, provide tools, address local barriers
- Example
- Intention-behavior gap, revert to old habits
- Solution
- Clinical decision support, reminders, audit and feedback
Implementation Strategies
Passive Dissemination: Publication, mailing - LOW effectiveness.
Active Strategies:
- Clinical Decision Support: Electronic alerts, order sets
- Audit and Feedback: Compare performance to guideline, provide feedback
- Academic Detailing: One-on-one education with opinion leaders
- Multifaceted Interventions: Combine strategies - MOST effective
Understanding barriers and targeting interventions improves uptake.
The topic lists "audit and feedback" as an implementation strategy but never defines the clinical audit cycle, which is the quality-improvement engine that turns a guideline into measured practice - a classic basic-science/QI viva:
- The clinical audit cycle (a closed loop): (1) set a standard/criterion - usually taken directly from a guideline (e.g. "antibiotics within 60 minutes of incision in 100 percent of cases"); (2) measure current practice against it; (3) compare performance to the standard and identify the gap; (4) implement change (the barrier-matched intervention); and crucially (5) RE-AUDIT to close the loop. An audit that never re-measures is not a true audit - closing the loop is the examiner's favourite point.
- PDSA (Plan-Do-Study-Act) is the rapid, small-scale iterative cousin: plan a change, do it on a small scale, study the effect, act (adopt/adapt/abandon), then repeat - multiple fast cycles rather than one big annual audit.
- Audit vs research: audit measures practice against an existing standard (no new knowledge, usually no ethics approval); research generates new knowledge and needs ethical review. Confusing the two is a common error.
Exam point: implement a guideline through the closed-loop clinical audit cycle (set standard → measure → compare → change → re-audit) or iterative PDSA cycles - the defining feature is re-auditing to close the loop, and audit (against a standard) is distinct from research (new knowledge).
AAAAImplementation Barriers - The 4 As
Hook:Diagnose which barrier dominates locally, then match the intervention - Grimshaw showed simply stacking more components does not reliably help.
Anatomy
- Clinical question (PICO): Population, Intervention, Comparison, Outcome
- Evidence summary: Systematic review of available evidence
- Evidence quality assessment: GRADE or similar system
- Recommendation statements: Clear, actionable guidance
- Rationale: Explanation linking evidence to recommendation
- Strong: Benefits clearly outweigh harms
- Weak/Conditional: Balance of benefits and harms is close
RCTs without serious limitations
- Further research unlikely to change confidence in effect
RCTs with limitations or strong observational
- Further research likely to change confidence
Observational studies
- Further research very likely to change effect estimate
Case series, expert opinion
- Estimate of effect is very uncertain
Strong recommendation CAN come from low-quality evidence when: (1) benefits clearly outweigh harms even with uncertainty, (2) ethical considerations mandate action, or (3) resource implications favor intervention. Example: Prophylactic antibiotics for open fractures (strong recommendation) despite limited RCT evidence.
Classification
- Condition-specific: Single disease or injury (e.g., ACL rupture)
- Procedure-specific: Single intervention (e.g., TKA)
- Cross-cutting: Apply across conditions (e.g., VTE prophylaxis)
- Professional societies (AAOS, AOA)
- Government agencies (NHMRC, NICE)
- Health systems (hospital-specific)
- Cochrane groups
Guideline Quality Assessment:
- Scope and Purpose (23%): Objectives, questions, population
- Stakeholder Involvement (18%): Relevant expertise, patient input
- Rigor of Development (27%): Evidence search, grading, updating
- Clarity of Presentation (13%): Specific, unambiguous recommendations
- Applicability (12%): Implementation advice, barriers, costs
- Editorial Independence (7%): Conflicts of interest, funding
AGREE II scores above 60% in Rigor of Development indicate a methodologically sound guideline. Many orthopaedic guidelines score poorly on this domain. Always check evidence grading and systematic review methodology before applying recommendations.
Investigations
- TRIP Database: Searches multiple guideline databases
- NHMRC Clinical Guidelines Portal: national guidelines
- NICE Evidence: UK guidelines, highly rigorous
- AAOS Clinical Practice Guidelines: Orthopaedic-specific
- Start with specialty society guidelines
- Check government/national guideline databases
- Search PubMed for "clinical practice guideline" + topic
- Who developed it? (reputation, expertise)
- When updated? (currency, within 5 years ideal)
- Evidence grading used? (GRADE preferred)
- Conflicts declared? (funding source, disclosures)
- AGREE II instrument (6 domains, 23 items)
- Score above 60% in Rigor indicates quality
Guidelines more than 5 years old may be outdated. Always check the publication date and whether there have been subsequent updates or superseding guidelines. Key orthopaedic guidelines (AAOS, NICE) are typically reviewed every 3-5 years.
Management
Key Strategies:
- Education and dissemination
- Clinical decision support and reminders
- Audit and feedback
- Local champions and opinion leaders
- Multifaceted interventions (most effective)
- Patient contraindications
- Patient values differ
- Resources unavailable
- New evidence since publication
Record rationale for deviation
Strong recommendations don't mean every patient must receive the intervention. Individualize based on patient factors and preferences, documenting rationale when deviating.
Surgical Technique
- Indications for surgery
- VTE and antibiotic prophylaxis
- Perioperative care protocols
- Enhanced recovery pathways
- Specific surgical techniques
- Implant selection
- Approach comparisons
- Sign in: Identity, consent, site marking
- Time out: Team briefing, antibiotic timing
- Sign out: Counts, recovery plan
death 1.5% to 0.8%, complications 11.0% to 7.0%
Most surgical technique recommendations are consensus-based. Guidelines typically address indications and perioperative care rather than operative technique. Surgical technique relies on training and observational evidence.
Complications
- Applying to wrong population
- Using outdated guidelines
- Ignoring individual factors
- "Cookbook medicine"
- Defensive practice
- Ignoring clinical judgment
- Evidence gaps
- Lag time in development
- Population vs individual focus
- Conflicts of interest
- Industry influence
- Variable methodology
Always check conflict of interest disclosures. Industry-funded guidelines may overestimate treatment benefits.
Postoperative Care
Key areas:
- VTE prophylaxis (duration, agent)
- Antibiotic prophylaxis
- Pain management protocols
- ERAS pathways
Quality indicators:
- VTE prophylaxis timing
- Antibiotic compliance
- SSI rates
- Readmission rates
Enhanced Recovery After Surgery bundles combine multiple guideline recommendations. Shown to reduce complications, length of stay, and costs in arthroplasty.
Outcomes
- Reduced variation in care
- Improved best practice adherence
- Measurable outcome improvements
- WHO surgical checklist (Haynes 2009): death 1.5% to 0.8%, complications 11.0% to 7.0%
- VTE guidelines: reduced symptomatic PE rates
- Guideline awareness
- Compliance rates
- Complication rates
- Patient-reported outcomes
- Cost-effectiveness
Most guideline-impact studies report process measures (e.g. proportion receiving prophylaxis on time), not patient outcomes. A high compliance rate is necessary but not sufficient - it does not prove patient benefit unless linked to a hard outcome. When appraising an implementation study, ask whether it measured what patients actually care about.
The topic contrasts process and outcome measures but never names the framework that organises quality measurement: the Donabedian model, the standard way to measure whether guideline-concordant care actually improves quality.
- Structure - the fixed attributes of the setting: staffing, equipment, theatre/ICU availability, whether a guideline/protocol exists at all. Easy to measure but the weakest link to patient benefit.
- Process - what is actually done to the patient: proportion receiving timely antibiotics, VTE prophylaxis prescribed, guideline-concordant care delivered. The most sensitive and actionable measure of guideline uptake, and what most implementation studies report.
- Outcome - what happens to the patient: mortality, surgical-site infection, symptomatic VTE, patient-reported outcome measures (PROMs). What patients ultimately care about, but confounded by case-mix and often needs risk-adjustment and large numbers.
The key insight (linking to the "process vs outcome" pearl above): good structure and process are necessary but not sufficient - high compliance (process) only proves benefit when it is shown to move a hard outcome. Use a balanced set across all three, and risk-adjust outcomes before comparing units.
Exam point: frame quality measurement with the Donabedian triad - structure, process and outcome - process measures best capture guideline uptake, outcome measures (risk-adjusted) capture patient benefit, and you need both because high process compliance does not by itself prove improved outcomes.
Exam Focus
Differential: Guideline vs Related Evidence Documents
A frequent viva trap is conflating a clinical practice guideline with other documents that look similar but carry different authority. Know the distinctions.
- Basis
- Systematic review of evidence + explicit benefit-harm appraisal
- How Recommendations Are Made
- GRADE or similar; strength separated from evidence quality
- Authority
- Highest - evidence-based, transparent, updatable
- Basis
- Expert opinion, often without systematic review
- How Recommendations Are Made
- Voting / Delphi process; evidence link often implicit
- Authority
- Lower - reflects opinion, useful where evidence is sparse
- Basis
- Systematic synthesis of primary studies
- How Recommendations Are Made
- Summarises evidence but makes NO clinical recommendation
- Authority
- Evidence source - feeds guidelines, not a recommendation itself
- Basis
- Local operationalisation of guidance
- How Recommendations Are Made
- Translates recommendations into step-by-step local actions
- Authority
- Local - implementation tool, not de novo evidence
- Basis
- Auditable minimum requirements derived from guidelines
- How Recommendations Are Made
- Short, mandatory-style statements for audit
- Authority
- Sets a measurable floor for quality
Controversies and Areas of Uncertainty
Critics argue rigid guideline adherence promotes "cookbook medicine" and erodes clinical judgement; proponents counter that they reduce unwarranted variation. The resolution is that strong recommendations apply to populations, while individuals are still managed by shared decision-making.
Many guideline panels historically included members with financial conflicts. Whether full recusal, a conflict-free chair, or transparent declaration is sufficient remains debated - AGREE II's editorial-independence domain captures this concern.
Traditional 3-5 year update cycles leave guidelines outdated between revisions. Living guidelines with continuous surveillance address this but are resource-intensive and not yet standard in orthopaedics.
Guidelines built largely on trial populations may not apply to the comorbid, elderly, or under-represented patients seen in practice - a key reason a guideline informs but never replaces individualised judgement.
Clinical Relevance and Applications
Applying Guidelines in Orthopaedic Practice
- Apply to most patients unless contraindicated
- Example: "We recommend VTE prophylaxis for major orthopaedic surgery" - give prophylaxis to essentially all patients
- Shared decision-making required
- Example: "We suggest arthroscopic debridement may be considered for mechanical symptoms in early OA" - discuss alternatives, patient values matter
- Evidence insufficient to guide practice
- Use clinical judgment, inform patient of uncertainty
Guideline Limitations
- Guidelines inform, not dictate decisions
- Individual patient factors may override recommendations
- Rare complications or comorbidities may not be addressed
- Atypical patient characteristics (age, comorbidities)
- Patient preferences differ from guideline assumptions
- Local resources unavailable
- New evidence published since guideline development
Wise clinicians use guidelines as a starting point, then individualize based on patient-specific factors.
Guidelines, Registries & Global Practice
Major Guideline Developers Worldwide
American Academy of Orthopaedic Surgeons. GRADE-based orthopaedic CPGs (hip fracture, knee/hip OA, VTE, rotator cuff, distal radius). Strength downgraded transparently when evidence is limited.
National Institute for Health and Care Excellence plus British Orthopaedic Association standards. Highly rigorous methodology, economic modelling (cost-per-QALY), and short, auditable BOAST standards for trauma.
AO Foundation fracture-management principles and EFORT European consensus statements. Strong on operative technique consensus where RCT evidence is sparse.
NHMRC (Australia), AOA (Australia), SIGN (Scotland), WHO (global surgical safety), and society guidelines elsewhere. Therapeutic Guidelines-type formularies localise antibiotic and VTE prophylaxis.
Side-by-Side: Where Guidelines Genuinely Differ
- Position
- AAOS and many US/Australian protocols accept aspirin; NICE/ACCP historically favoured LMWH or DOACs
- Reason for Divergence
- Weighting of bleeding vs thrombosis, cost, and registry/RCT evidence (e.g. CRISTAL)
- Position
- AAOS strong recommendation AGAINST; broadly concordant across NICE/EFORT
- Reason for Divergence
- Consistent high-quality RCT evidence (Moseley, Kirkley) - rare global agreement
- Position
- NICE favours cemented for fragility hip fracture; registries inform nuance
- Reason for Divergence
- Registry signals (cement implantation syndrome vs periprosthetic fracture) weighted differently
Registry Evidence Feeding Guidelines
Arthroplasty and fixation guidance increasingly draws on national joint registries rather than RCTs alone:
- NJR (England, Wales, NI, IoM, Guernsey), AJRR (US), AOANJRR (Australia), SHAR (Sweden), Norwegian and NZJR registries supply implant survival and revision-rate data on millions of procedures.
- Registries provide external validity and rare-event detection (e.g. metal-on-metal failure) that trials cannot, but are observational - they inform but cannot prove causation.
- Guideline panels combine registry survival data with RCT functional outcomes and GRADE the resulting body of evidence.
High- vs Limited-Resource Practice Variation
International guidelines require local adaptation; the ADAPTE and GRADE-ADOLOPMENT frameworks formalise this.
Key drivers of variation:
- Resource setting: availability of DOACs, intra-operative imaging, implant range, and theatre capacity changes what is feasible (a strong recommendation is meaningless if the drug or implant is unavailable).
- Local epidemiology: injury patterns, comorbidity burden, and antimicrobial resistance differ by region and alter the benefit-harm balance.
- Local registry data: revision rates for a given implant in the local population may justify departing from an international default.
Example: an international guideline may default to a DOAC for thromboprophylaxis, but a limited-resource setting may justifiably adopt aspirin plus mechanical prophylaxis based on cost, monitoring capacity, and acceptable local outcome data - a defensible local adaptation, not a deviation in error.
MCQ Practice Points
Q: Can a guideline make a strong recommendation based on low-quality evidence? A: Yes - GRADE separates evidence quality (confidence in effect) from recommendation strength (should we do it). Strong recommendation possible with low-quality evidence if there is a large magnitude of effect, ethical imperative, or clear benefit-harm balance favoring intervention. Example: Strong recommendation for surgery in displaced fractures despite lack of RCTs.
Q: What is the most important AGREE II domain for assessing guideline quality? A: Rigor of Development - assesses whether systematic methods were used to search for evidence, appraise quality, link evidence to recommendations, and formulate recommendations using explicit criteria. This distinguishes evidence-based guidelines from expert consensus documents.
Q: What are the main barriers to guideline implementation? A: The 4 As: Awareness (clinicians do not know guideline exists), Agreement (disagree with recommendations), Adoption (too difficult to implement due to resources or system barriers), Adherence (forget to apply or revert to old habits). Multifaceted active implementation strategies needed.
Q: How often should clinical practice guidelines be updated? A: Guidelines should be reassessed every 2-3 years and formally updated every 3-5 years. Living guidelines use continuous surveillance to update recommendations as new evidence emerges. A guideline is considered outdated if it has not been updated within 5 years or if substantial new evidence contradicts current recommendations.
Q: How should conflicts of interest be managed in guideline development? A: Panel members should declare all financial and intellectual COI at the outset. Those with significant COI should recuse from voting on related recommendations. The chair of the guideline panel should ideally be free from relevant COI. All declarations should be publicly available in guideline documentation. COI management is a key domain assessed by AGREE II.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“How do you critically appraise a clinical practice guideline?”
“A patient asks about a new treatment they read about online. How do you use clinical practice guidelines to inform your discussion?”
“How do you approach shared decision-making when guidelines make a weak recommendation?”
“You deviate from a guideline and the patient has a complication. How do you defend your decision?”
“How would you implement a new guideline in your department?”
Guideline Definition and Purpose
- CPG = Systematically developed statements to guide clinical decisions
- Based on systematic review of evidence and explicit consideration of benefits/harms
- Purpose: Reduce unwarranted variation, improve quality, inform policy
- Should be updated every 3-5 years as new evidence emerges
- Distinguish from consensus statements (opinion-based, not systematic)
GRADE System
- Evidence Quality: High/Moderate/Low/Very Low (confidence in effect estimate)
- Recommendation Strength: Strong/Weak (should we do it?)
- RCT starts at High, Observational starts at Low, then apply modifiers
- Downgrade for: RIIIP (Risk of bias, Inconsistency, Indirectness, Imprecision, Publication bias)
- Strong recommendation possible with low evidence if large effect or ethical imperative
Strong vs Weak Recommendations
- Strong: We recommend / Most patients should receive / Can use as quality measure
- Weak: We suggest / Different choices for different patients / Shared decision-making
- Strong requires: Large benefit, minimal harm, aligned values, feasible, OR ethical imperative
- Weak: Close benefit-harm balance, varied patient values, high cost, or uncertain evidence
- Wording signals strength - clinicians must recognize difference
AGREE II Quality Appraisal
- 6 domains: Scope, Stakeholder involvement, Rigor (most important), Clarity, Applicability, Independence
- Rigor domain: Systematic search, explicit methods, evidence-to-recommendation link, external review, update plan
- Editorial independence: Funding declared, conflicts managed, majority non-conflicted
- Patient involvement essential for patient-centered guidelines
- Overall assessment: Recommend for use / With modifications / Do not recommend
Implementation Barriers and Solutions
- 4 As: Awareness, Agreement, Adoption, Adherence
- Passive dissemination (publication, mailing) = ineffective
- Active strategies: Clinical decision support, audit-feedback, academic detailing, reminders
- Multifaceted interventions (combine strategies) most effective
- Local adaptation needed to address barriers and context
Guidelines, Registries & Global Practice
- Major developers: AAOS (US), NICE/BOA-BOAST (UK), AO Foundation/EFORT (Europe), NHMRC/AOA, SIGN, WHO
- Registries (NJR, AJRR, AOANJRR, SHAR, NZJR) supply implant survival and revision data feeding guidelines
- Genuine divergence: aspirin vs LMWH/DOAC for VTE; consensus AGAINST knee arthroscopic debridement
- Adaptation frameworks: ADAPTE and GRADE-ADOLOPMENT formalise local tailoring
- Adapt to local epidemiology, registry data, and resource setting - a strong rec is meaningless if the drug/implant is unavailable
Evidence Base
GRADE: an emerging consensus on rating quality of evidence and strength of recommendations
- Landmark statement introducing the GRADE system to a broad clinical audience
- Separates evidence quality (confidence in the effect estimate) from recommendation strength (should we do it)
- Evidence rated High/Moderate/Low/Very Low; recommendations Strong or Weak
- RCTs start High and observational studies start Low, then are up- or downgraded by explicit factors
- Now adopted by WHO, Cochrane and over 100 organisations worldwide
GRADE guidelines: 15. Going from evidence to recommendation - determinants of a recommendation's direction and strength
- Defines how panels move from a body of evidence to a graded recommendation
- Four determinants: balance of desirable vs undesirable effects, confidence in estimates, values and preferences, and resource use
- Strength reflects confidence that net desirable effects outweigh undesirable effects
- Explicitly allows a strong recommendation despite low-confidence evidence in defined situations
- Requires explicit panel judgement integrating all four domains