Budapest Criteria | Vitamin C Prevention | Multidisciplinary Management | Early Treatment Critical
- Budapest criteria: continuing disproportionate pain plus symptoms in ≥3 of 4 categories (sensory, vasomotor, sudomotor/edema, motor/trophic) AND signs in ≥2, with no better diagnosis
- Vitamin C prophylaxis: 500mg daily for 50 days cut CRPS after wrist fracture from ~10% to ~2.4% in the Zollinger RCT (later evidence mixed)
- Function-focused rehabilitation is the foundation - graded motor imagery, mirror therapy, desensitisation; escalate by response
- Multidisciplinary care: rehabilitation, neuropathic agents, psychology, sympathetic blocks; SCS for refractory pain
- Diagnosis of exclusion: actively rule out infection, DVT, compartment syndrome and nerve injury before diagnosing CRPS
- “Budapest criteria: disproportionate pain plus symptoms in ≥3 of 4 categories and signs in ≥2, with no better explanation
- “Vitamin C 500mg daily for 50 days reduced CRPS after wrist fracture (~10% to ~2.4%); the RCT was in wrist, not foot/ankle, and later data are mixed
- “Rehabilitation (graded motor imagery, desensitisation, mirror therapy) is the foundation of treatment
- “The classic 3-stage model is traditional but not validated - do not quote it as prognosis
Need symptoms in ≥3 of 4 categories: Sensory (allodynia, hyperalgesia), Vasomotor (temperature/color asymmetry), Sudomotor/Edema (swelling, sweating), Motor/Trophic (decreased ROM, trophic changes). Plus continuing pain disproportionate to injury. This is the diagnostic standard.
Vitamin C 500mg daily for 50 days cut CRPS after wrist (distal radius) fracture from ~10% to ~2.4% in the Zollinger dose-response RCT. Cheap and safe; the trial was in wrist fractures, and later/foot-ankle evidence is mixed. Many guidelines still recommend it for high-risk fractures.
CRPS requires ruling out mimics - infection, DVT, compartment syndrome, occult fracture/hardware problems and nerve injury. Budapest criterion 4 ("no other diagnosis better explains the findings") is mandatory. Around 74% of CRPS-I cases resolve, often spontaneously.
Physiotherapy is cornerstone - graded motor imagery, desensitization, mirror therapy. Medications: gabapentin/pregabalin first-line. Sympathetic blocks for diagnostic/therapeutic. Psychological support essential. Pain clinic referral for complex cases.
- Timeline
- 0-3 months
- Features
- Pain, swelling, warmth, erythema, limited ROM
- Note
- Warm inflammatory picture
- Timeline
- 3-6 months
- Features
- Trophic changes, cool skin, hair loss, nail changes
- Note
- Transitional features
- Timeline
- Over 6 months
- Features
- Atrophy, contractures, fixed deformity
- Note
- Cold/established picture
The three-stage sequence is a useful descriptive vocabulary but is not a validated prognostic model - many patients do not progress sequentially. Cluster analysis supports CRPS sub-types (warm vs cold) rather than fixed stages.
SVSMBudapest Criteria
Hook:SVSM: Need symptoms in ≥3 of 4 categories (Sensory, Vasomotor, Sudomotor/Edema, Motor/Trophic) plus continuing pain!
Overview and Epidemiology
Complex Regional Pain Syndrome (CRPS) is a chronic pain condition that typically develops after trauma or surgery, characterized by disproportionate pain, vasomotor changes, and trophic changes. Formerly known as Reflex Sympathetic Dystrophy (RSD) or Sudeck's atrophy.
- First described by Silas Weir Mitchell in 1864 (causalgia)
- Sudeck described atrophy in 1900
- Reflex Sympathetic Dystrophy term used until 1994
- CRPS term adopted in 1994 (IASP)
- Budapest criteria established in 2003 (current diagnostic standard)
- Population incidence: 5-26 per 100,000 person-years (Olmsted County vs Dutch primary-care data — estimates vary several-fold with case-finding method)
- Female:Male ratio: 3-4:1; highest incidence in postmenopausal women (61-70 years)
- Median onset age ~46 years; upper limb affected more often than lower limb
- Commonest trigger: fracture (44-46%), especially distal radius; also surgery, sprains, spontaneous onset
- After distal radius fracture, untreated CRPS occurred in ~10% of placebo patients in the Zollinger RCT
- Risk factors: female sex, fracture/immobilisation, cast-related complaints, possibly anxiety/depression
- Around 74% of CRPS-I cases resolve, often spontaneously (Olmsted County data)
Vitamin C 500mg daily for 50 days reduced CRPS after distal radius fracture from ~10% (placebo) to ~2.4% in the Zollinger dose-response RCT, with no added benefit from higher doses. The evidence is strongest for wrist fractures; later trials and foot/ankle data are mixed, but the low cost and safety mean it is still widely recommended for high-risk fractures.
Anatomy and Pathophysiology
Pathophysiology: The exact mechanism is unclear, but multiple theories exist:
- Mechanism
- Release of neuropeptides (substance P, CGRP)
- Evidence
- Elevated levels in CRPS
- Mechanism
- Altered pain processing in CNS
- Evidence
- Functional MRI changes
- Mechanism
- Abnormal sympathetic activity
- Evidence
- Response to sympathetic blocks
- Mechanism
- Autoantibodies against nervous system
- Evidence
- Some evidence
- Allodynia: Pain from non-painful stimuli (light touch) - indicates central sensitization
- Hyperalgesia: Exaggerated pain from painful stimuli - indicates peripheral and central sensitization
- Vasomotor changes: Temperature/color asymmetry - indicates autonomic dysfunction
- Trophic changes: Hair loss, nail changes, skin atrophy - indicates chronic changes
Stages of CRPS
- Pain, swelling, warmth, erythema
- Limited ROM
- Hyperalgesia, allodynia
- Best prognosis with treatment
- Progression of trophic changes
- Skin becomes cool and clammy
- Hair loss, nail brittleness
- Muscle atrophy begins
- Treatment still helps but prognosis moderate
- Irreversible changes
- Severe atrophy, contractures
- Severe pain, functional disability
- Poor prognosis - permanent disability
Early recognition matters, but the classic acute/dystrophic/atrophic three-stage model is traditional and not validated by prospective data. Cluster analysis points to CRPS sub-types (warm-inflammatory vs cold-central) rather than an inevitable progression. Diagnose early with the Budapest criteria, start function-focused rehabilitation, and avoid quoting fixed stage-based recovery percentages as established fact.

Classification Systems
Budapest Diagnostic Criteria (Current Standard)
- Continuing pain disproportionate to inciting event
- Symptoms in ≥3 of 4 categories:
- Sensory: Allodynia (pain from light touch), hyperalgesia (exaggerated pain)
- Vasomotor: Temperature asymmetry (greater than 1°C), skin color changes (blotchy, purple, red, pale)
- Sudomotor/Edema: Swelling, sweating changes (hyperhydrosis or anhydrosis)
- Motor/Trophic: Decreased ROM, motor dysfunction (weakness, tremor), trophic changes (hair loss, nail changes, skin atrophy)
- Signs in ≥2 of 4 categories (same as above)
- No other diagnosis that better explains the symptoms
- Budapest criteria are the current diagnostic standard
- No definitive test confirms CRPS
- Diagnosis is clinical based on criteria
- Early diagnosis improves outcomes
Budapest criteria are the current diagnostic standard for CRPS.
Clinical Assessment
History:
- Recent trauma or surgery (weeks to months)
- Pain out of proportion to injury
- Progressive symptoms
- Previous CRPS (10-30% recurrence risk)
- Female, smoking, anxiety/depression (risk factors)
Physical Examination:
- Allodynia: Pain from light touch
- Hyperalgesia: Exaggerated pain from pinprick
- Temperature asymmetry: Greater than 1°C difference
- Color changes: Blotchy, purple, red, pale
- Decreased ROM: Out of proportion to injury
- Weakness: Motor dysfunction
- Trophic changes: Hair loss, nail changes, skin atrophy
- Swelling: Persistent edema
Key Clinical Signs:
- Allodynia: Light touch causes pain - pathognomonic
- Temperature asymmetry: Measure with thermometer - greater than 1°C difference
- Color changes: Blotchy, purple, red, or pale appearance
- Trophic changes: Hair loss, nail brittleness, skin atrophy (late finding)
Allodynia (pain from light touch) is pathognomonic for CRPS and indicates central sensitization. This is a key diagnostic feature. If a patient has pain from light touch after trauma/surgery, strongly consider CRPS.
Investigations
Clinical Diagnosis:
- CRPS is primarily a clinical diagnosis
- Budapest criteria are diagnostic
- No definitive test confirms CRPS
- Tests are supportive, not diagnostic
Supportive Investigations:
- Finding
- Increased uptake in affected limb
- Significance
- Supportive but not diagnostic
- Finding
- Patchy bone marrow edema, soft tissue edema
- Significance
- Supportive but not diagnostic
- Finding
- Patchy osteopenia (late)
- Significance
- Late finding, not early
- Finding
- Temperature asymmetry
- Significance
- Supportive but not diagnostic
- Phase 1 (blood flow): Increased perfusion
- Phase 2 (blood pool): Increased pooling
- Phase 3 (delayed): Increased uptake in affected limb
- Sensitivity: 50-80% (normal scan doesn't exclude CRPS)
- Specificity: Moderate
- Patchy bone marrow edema
- Soft tissue edema
- Not diagnostic but supportive
- May help exclude other diagnoses
CRPS is a clinical diagnosis based on Budapest criteria. No test is diagnostic. Three-phase bone scan and MRI are supportive but not required. Normal scans don't exclude CRPS. Early diagnosis based on clinical criteria is essential for good outcomes.
Sympathetically Maintained vs Sympathetically Independent Pain
CRPS pain is classically divided by its response to sympathetic blockade - not into a separate diagnosis, but into two mechanistic categories. This distinction is what explains why the sympathetic blocks used throughout this topic help some patients and not others.
- Sympathetically maintained pain (SMP): the component of pain relieved by interrupting sympathetic outflow - a local-anaesthetic sympathetic block, or an intravenous phentolamine (alpha-adrenergic blocker) infusion test. Here catecholamines drive nociceptor firing through up-regulated adrenoceptors on sensitised primary afferents.
- Sympathetically independent pain (SIP): pain that persists despite an adequate sympathetic block. A large share of CRPS pain is sympathetically independent, which is exactly why sympatholysis is not a universal cure.
Key exam points:
- A diagnostic sympathetic block (stellate ganglion for the upper limb, lumbar sympathetic chain for the lower limb) is used to unmask an SMP component; genuine relief that outlasts the local-anaesthetic duration and reproduces on repeat blockade supports SMP.
- SMP and SIP can coexist in the same limb and shift over time - a patient is not permanently "sympathetic" or not.
- The therapeutic value of sympathetic blocks lies mainly in the SMP subgroup, and chiefly to provide a window of analgesia that enables active rehabilitation; high-quality evidence for durable benefit is limited, so blocks are an adjunct, never a stand-alone treatment.
- The old assumption that all CRPS (the historical "reflex sympathetic dystrophy") is sympathetically driven is outdated - the SMP/SIP framework replaced it.
A sympathetic block is both a diagnostic probe and a therapeutic adjunct. Relief identifies sympathetically maintained pain (SMP) and predicts who may benefit from repeated blocks to unlock rehabilitation; failure to respond indicates sympathetically independent pain (SIP), in which sympatholysis - including surgical sympathectomy - is futile. Never offer sympathectomy to a patient whose pain is sympathetically independent.
Differential Diagnosis
CRPS is a clinical diagnosis of exclusion (Budapest criterion 4: no other diagnosis better explains the findings). The key mimics after limb trauma or surgery must be actively excluded before labelling a patient with CRPS.
- Discriminating features
- Disproportionate pain plus vasomotor, sudomotor/oedema and motor/trophic signs in one region
- Excluded by
- Meets Budapest criteria; no better explanation
- Discriminating features
- Fever, raised CRP/WCC, localised collection, systemic upset
- Excluded by
- Bloods, aspiration, MRI/imaging
- Discriminating features
- Unilateral swelling, calf tenderness, risk factors
- Excluded by
- Doppler ultrasound, D-dimer
- Discriminating features
- Pain on passive stretch, tense compartment, early post-injury
- Excluded by
- Clinical exam, compartment pressures
- Discriminating features
- Pain in defined nerve territory, sensory/motor map fits a nerve
- Excluded by
- Examination, nerve conduction studies
- Discriminating features
- Focal bony tenderness, mechanical pain, implant prominence
- Excluded by
- Radiographs, CT
- Discriminating features
- Joint-centred swelling, polyarticular pattern, raised inflammatory markers
- Excluded by
- Bloods, joint aspiration, serology
Never diagnose CRPS until infection, DVT and compartment syndrome have been considered and excluded. Vasomotor change plus disproportionate pain can be the presentation of all four. Budapest criterion 4 ("no other diagnosis") is not optional.
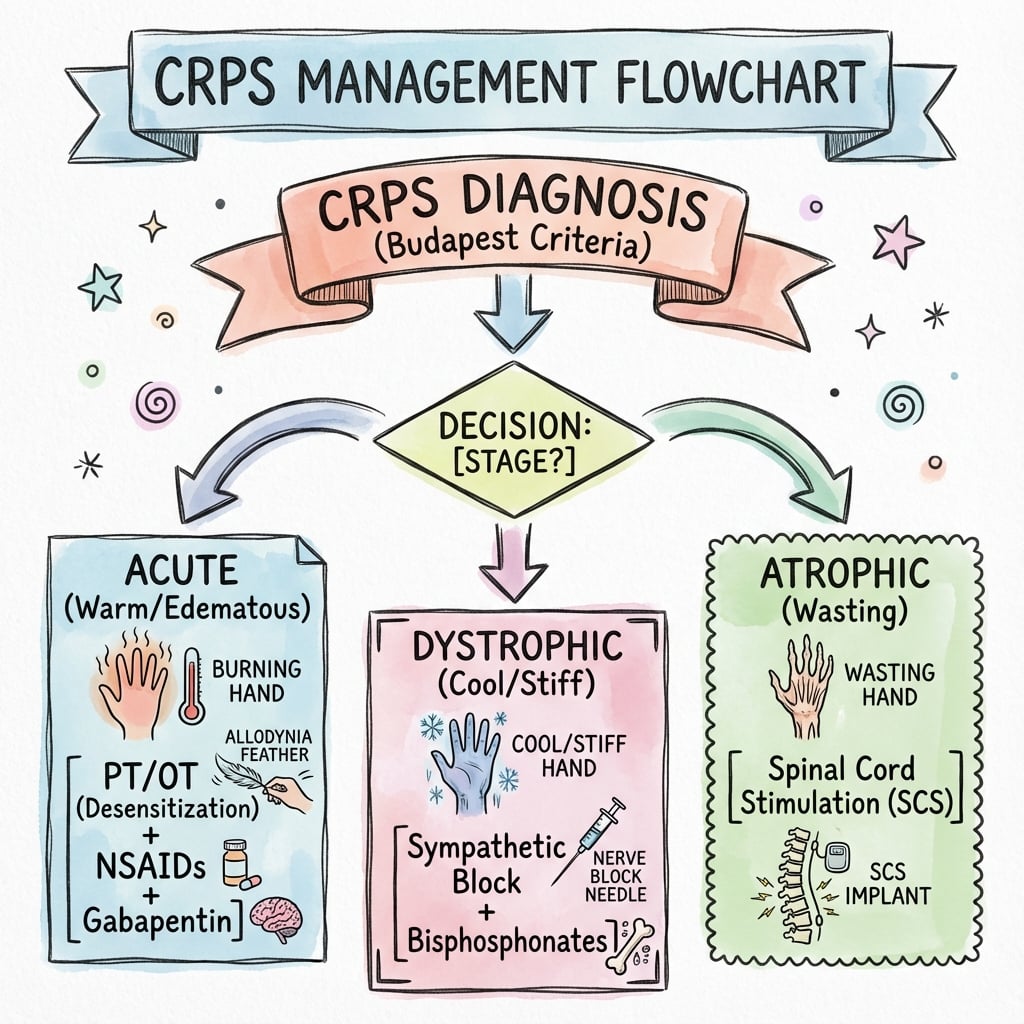
Management Algorithm
Prevention Strategies
- 500mg daily for 50 days starting peri-operatively
- Reduced CRPS after distal radius fracture from ~10% to ~2.4% (Zollinger RCT)
- Strongest evidence in wrist fractures; later/foot-ankle data mixed
- Inexpensive and safe
- Reasonable to use in high-risk fractures
- Early mobilization (avoid prolonged immobilization)
- Adequate pain control (multimodal analgesia)
- Gentle tissue handling
- Patient education about expectations
Prevention is far superior to treatment.
PMPSCRPS Treatment
Hook:PMPS: Physiotherapy is cornerstone, Medications (gabapentin), Psychological support, Sympathetic blocks!
Treatment Details
Physiotherapy - Cornerstone of Treatment
- Laterality training (identify left vs right)
- Motor imagery (mental practice)
- Mirror therapy (visual feedback)
- Progressive sequence
- Progressive tactile stimulation
- Start with soft textures
- Progress to rough textures
- Patient-controlled pace
- Active ROM (patient-controlled)
- Avoid passive aggressive therapy (worsens symptoms)
- Functional restoration
- Weight-bearing as tolerated
- Stress loading (weight-bearing activities)
- Normal gait pattern training
- Functional restoration
Physiotherapy is the cornerstone and must be started early.
Bisphosphonates in CRPS
Bisphosphonates are the best-evidenced pharmacological disease-modifier in early CRPS, yet the topic elsewhere lists them only in passing. The exam rewards the mechanistic rationale, so it is worth developing.
- Early CRPS shows accelerated regional bone turnover - the patchy periarticular osteopenia on late radiographs, the increased delayed-phase uptake on three-phase bone scan, and the bone-marrow oedema on MRI all reflect osteoclast-driven bone resorption.
- Bisphosphonates inhibit osteoclastic resorption, damp this heightened turnover, and may additionally reduce the local acidic and inflammatory microenvironment and associated nociceptor sensitisation.
- Benefit is greatest in the early, "warm", high-turnover phase with increased bone-scan uptake - the subgroup most likely to respond - and little in long-standing "cold" disease.
- Randomised trials support several agents (oral alendronate, intravenous pamidronate, intravenous neridronate); the neridronate multicentre RCT is the most cited and most positive.
- They are a reasonable adjunct to function-focused rehabilitation in early CRPS, especially with imaging evidence of increased bone turnover - not a substitute for rehabilitation.
Neridronate for Early CRPS-I (Randomised Controlled Trial)
- Multicentre double-blind RCT, 82 patients with acute CRPS-I of the hand or foot: IV neridronate 100mg four times over 10 days vs placebo
- VAS pain fell significantly more with neridronate (further reduction 46.5mm vs 22.6mm over days 20-40; p less than 0.0001)
- Significant gains across other pain and quality-of-life indices; formerly-placebo patients matched the active group after open-label crossover
- At one year no patient reported CRPS-related symptoms
Consider a bisphosphonate in early, warm CRPS with increased three-phase bone-scan uptake: the mechanism is inhibition of the accelerated osteoclastic bone resorption that also produces the patchy osteopenia and bone-marrow oedema. It is an adjunct to rehabilitation, best-evidenced early, and of little value in established "cold" disease.
VITAMIN CCRPS Prevention
Hook:VITAMIN C: Vitamin C prophylaxis, Immobilization minimal, Trauma minimize, Analgesia adequate, Mobilization early, Immobilization avoid, NSAIDs, Control pain!
Surgical Technique
Note: CRPS itself is not a surgical condition, but surgical procedures may be needed for the underlying injury. This section addresses surgical considerations when CRPS is present or at risk.
Surgical Considerations
- Vitamin C 500mg daily for 50 days starting peri-operatively
- Minimize surgical trauma
- Adequate analgesia
- Early mobilization post-operatively
- Gentle tissue handling
- Meticulous hemostasis
- Avoid excessive retraction
- Minimize tourniquet time if possible
- Multimodal analgesia
- Early mobilization
- Monitor for CRPS signs
- Early recognition and treatment if CRPS develops
Prevention through careful surgical technique is key.
Complications
- Timing
- Persistent
- Management
- Multidisciplinary pain management
- Timing
- Persistent
- Management
- Physiotherapy, occupational therapy
- Timing
- Late (Stage 3)
- Management
- Surgical release if severe
- Timing
- Common
- Management
- Psychological support, CBT
- Timing
- Ongoing
- Management
- Monitor and adjust
- 10-20% develop chronic CRPS with permanent disability
- Poor prognosis if treatment delayed
- May require long-term pain management
- Functional impairment may be permanent
- Late complication (Stage 3)
- May require surgical release
- Prevention through early treatment is key
- Physiotherapy essential
Early recognition plus active, function-focused rehabilitation reduces the risk of fixed contractures and chronic disability. Most CRPS-I cases improve (often spontaneously), but a minority progress to chronic, disabling disease; established contractures and the cold phenotype carry the worst outlook.
Postoperative Care
After Surgery (CRPS Prevention):
CRPS Prevention Protocol
- Start vitamin C 500mg daily (continue for 50 days)
- Multimodal analgesia
- Gentle tissue handling
- Minimize immobilization
- Continue vitamin C
- Adequate pain control
- Early mobilization if fracture stable
- Monitor for CRPS signs
- Continue vitamin C (total 50 days)
- Physiotherapy (ROM exercises)
- Functional restoration
- Monitor for CRPS
- Continue monitoring
- Early recognition if CRPS develops
- Multidisciplinary treatment if needed
If CRPS Develops:
- Immediate multidisciplinary referral
- Physiotherapy (cornerstone)
- Medications (gabapentin first-line)
- Sympathetic blocks if needed
- Psychological support
- Pain clinic referral
Outcomes and Prognosis
- In the Olmsted County population study, ~74% of CRPS-I cases resolved, often spontaneously (Sandroni 2003)
- A minority develop persistent, disabling chronic CRPS; outcomes are heterogeneous and hard to predict
- Beware quoting precise stage-based recovery percentages: the three-stage model is not validated
- Longer symptom duration and delayed recognition
- The "cold"/central CRPS phenotype
- Marked motor/trophic changes and established contractures
- Psychological distress (anxiety/depression) as a comorbidity
- Previous CRPS (recurrence risk)
Counsel patients that the majority of CRPS-I cases resolve, frequently spontaneously (~74% in population data), while a minority become chronic. This realistic framing is more defensible than the older claim of fixed stage-linked recovery rates.
Guidelines, Registries & Global Practice
Global epidemiology:
- Population incidence varies several-fold by case-finding: 5.5 per 100,000 person-years (Olmsted County, USA) to 26.2 per 100,000 (Dutch primary care)
- Consistently female-predominant (3-4:1), peaking in postmenopausal women; fracture is the commonest trigger worldwide (44-46%)
- The diagnosis is clinical and standardised internationally by the Budapest criteria, so cross-country comparison is more consistent than for many pain conditions
Side-by-side guideline comparison:
- Diagnostic standard
- Budapest criteria
- Emphasis / notable position
- Function-focused interdisciplinary rehabilitation as the foundation; pragmatic recommendations given limited high-grade evidence
- Diagnostic standard
- Budapest criteria
- Emphasis / notable position
- Early diagnosis and the '4 pillars' (education, pain relief, physical/vocational rehab, psychology); GP-level recognition
- Diagnostic standard
- Clinical signs/symptoms
- Emphasis / notable position
- Free-radical scavengers (DMSO/N-acetylcysteine) for inflammatory CRPS; vitamin C to prevent CRPS after wrist fracture
- Diagnostic standard
- Budapest criteria
- Emphasis / notable position
- Stepwise, multidisciplinary care; SCS reserved for refractory disease in specialist centres
- CRPS is not tracked in joint registries, but registry-level evidence informs prevention: minimising re-operation, immobilisation and repeated cast complaints reduces risk
- Spinal cord stimulation outcomes are followed in device/pain registries; real-world data echo the trial finding of pain (not function) benefit with a meaningful revision rate
- High-resource settings: ready access to multidisciplinary pain services, graded motor imagery programmes, interventional blocks and SCS
- Limited-resource settings: emphasis shifts to early recognition, low-cost interventions (active rehabilitation, simple analgesics, amitriptyline, vitamin C prophylaxis after wrist fracture) and avoidance of prolonged immobilisation, since advanced interventional and neuromodulation options may be unavailable
Across all major guidance the message is the same: diagnose with the Budapest criteria, exclude mimics, and make function-focused rehabilitation the foundation, escalating to pharmacology, psychology and interventional procedures by response. Differences are mainly in adjuncts (e.g. Dutch free-radical scavengers) and in access to neuromodulation.
Controversies and Areas of Uncertainty
CRPS is one of the most contested diagnoses in orthopaedics. High-yield areas of genuine uncertainty:
The acute / dystrophic / atrophic staging (used historically and in many revision aids) is traditional but not supported by prospective data. Cluster analysis suggests CRPS sub-types (e.g. a warm inflammatory form and a cold central form) rather than an inevitable sequential progression. Use staging as a descriptive aid, not a validated prognostic tool.
No single mechanism explains CRPS. Peripheral and central sensitisation, neurogenic inflammation, altered sympathetic function, cortical reorganisation and possible autoimmune contributions all have supporting evidence but none is fully proven. The condition is best viewed as multi-mechanistic.
The Zollinger wrist-fracture RCTs are positive, but later trials and meta-analyses have produced mixed results, and the effect was not reproduced in some surgical/foot-ankle cohorts. Many guidelines still recommend it given low cost and safety, but the certainty of benefit is lower than once thought.
The 4th-edition guidelines explicitly note a paucity of level 1-2 evidence. Spinal cord stimulation reduces pain but not function and its benefit attenuates over years; bisphosphonates and ketamine have limited supporting data; sympathectomy is largely abandoned. Function-focused rehabilitation has the most consistent support.
MCQ Practice Points
Q: What are the Budapest diagnostic criteria for CRPS? A: Need symptoms in ≥3 of 4 categories (Sensory, Vasomotor, Sudomotor/Edema, Motor/Trophic) plus continuing pain disproportionate to injury. This is the current diagnostic standard. No definitive test confirms CRPS.
Q: What is the best-evidenced prophylaxis for CRPS after fracture? A: Vitamin C 500mg daily for 50 days starting peri-operatively - in the Zollinger dose-response RCT this cut CRPS after distal radius fracture from ~10% to ~2.4%, with no extra benefit from higher doses. The strongest evidence is in wrist fractures; later/foot-ankle data are mixed, but it is cheap and safe.
Q: What is the natural history and prognosis of CRPS-I? A: Most cases (~74% in population data) resolve, often spontaneously, while a minority become chronic and disabling. The classic three-stage model is not validated and should not be quoted as fixed prognosis. Early recognition and function-focused rehabilitation remain the priority.
Q: What is the cornerstone of CRPS treatment? A: Physiotherapy - graded motor imagery, desensitization, mirror therapy, active ROM exercises. This is the cornerstone and must be started early. Medications, sympathetic blocks, and psychological support are also essential.
Q: What is allodynia in CRPS? A: Pain from non-painful stimuli (light touch) - this is pathognomonic for CRPS and indicates central sensitization. It's a key diagnostic feature in the Budapest criteria (sensory category).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman presents 6 weeks after ankle fracture fixation. She has severe pain out of proportion, allodynia (pain from light touch), temperature asymmetry (2°C difference), and persistent swelling. How do you diagnose and manage this?”
“You are planning ankle fracture fixation in a 50-year-old woman with a history of anxiety. How do you prevent CRPS?”
“A 55-year-old man is referred 9 months after distal radius fixation with persistent burning pain, a cold mottled hand, fixed wrist stiffness and patchy osteopenia on radiographs. He has failed gabapentin and physiotherapy. How do you approach this, and how confident are you in the diagnosis?”
Key Facts
- Population incidence: 5-26 per 100,000 person-years
- Female:Male ratio: 3-4:1; fracture is commonest trigger
- Budapest criteria: symptoms in ≥3 of 4 categories plus signs in ≥2
- Vitamin C 500mg/50 days reduces post-wrist-fracture CRPS
Budapest Criteria (SVSM)
- Sensory: Allodynia, hyperalgesia
- Vasomotor: Temperature/color asymmetry
- Sudomotor/Edema: Swelling, sweating changes
- Motor/Trophic: Decreased ROM, trophic changes
- Need ≥3 of 4 categories plus continuing pain
Prevention
- Vitamin C 500mg daily for 50 days (CRPS ~10% to ~2.4% after wrist #)
- Early mobilization (avoid prolonged immobilization)
- Adequate multimodal analgesia
- Gentle tissue handling
- Start vitamin C peri-operatively
Treatment (PMPS)
- Physiotherapy: Cornerstone - graded motor imagery, desensitization, mirror therapy
- Medications: Gabapentin/pregabalin first-line, amitriptyline, bisphosphonates
- Psychological: CBT, pain psychology, biofeedback
- Sympathetic blocks: Diagnostic and therapeutic, may facilitate PT
Prognosis & Staging
- Most CRPS-I cases improve, often spontaneously (~74% in population data)
- Classic acute/dystrophic/atrophic staging is descriptive, NOT validated prognosis
- Cluster analysis supports warm vs cold sub-types, not fixed sequential stages
- Worse outlook: long duration, cold phenotype, established contractures, psychological distress
- Refractory disease - manage in a multidisciplinary pain service; consider SCS trial
Evidence Base
Incidence of CRPS: Dutch Population-Based Study
- Population-based cohort, 600,000 patients in Dutch primary care
- Overall CRPS incidence 26.2 per 100,000 person-years (95% CI 23.0-29.7)
- Females affected at least 3.4 times more often; highest incidence in women aged 61-70
- Upper limb more affected than lower limb; fracture the commonest trigger (44%)
Incidence, Prevalence and Outcome of CRPS-I: Olmsted County
- US population-based study, 74 CRPS-I cases over 1989-1999
- Incidence 5.46 per 100,000 person-years; period prevalence 20.57 per 100,000
- Female:male 4:1, median onset age 46; fracture the commonest trigger (46%)
- 74% of patients underwent resolution, often spontaneously
Vitamin C Prevention of CRPS after Wrist Fracture (Dose-Response RCT)
- Double-blind multicentre RCT, 416 patients with 427 wrist fractures (placebo vs 200, 500 or 1500mg vitamin C daily for 50 days)
- CRPS prevalence 2.4% with vitamin C vs 10.1% with placebo (p=0.002)
- 500mg dose: relative risk 0.17 (95% CI 0.04-0.77); no added benefit from 1500mg
- A daily dose of 500mg for 50 days is recommended
Validation of the Budapest Diagnostic Criteria
- Validation study in 113 CRPS-I and 47 non-CRPS neuropathic pain patients
- Budapest clinical criteria: sensitivity 0.99, specificity 0.68 (vs IASP specificity 0.41)
- Budapest research criteria: highest specificity 0.79
- Four-component structure (sensory, vasomotor, sudomotor/oedema, motor/trophic) drives improved specificity
CRPS: Practical Diagnostic and Treatment Guidelines, 4th Edition
- Interdisciplinary consensus guideline endorsing function-focused rehabilitation as the foundation of care
- Recommends a coordinated rehabilitation-pharmacology-psychology-interventional pathway, escalated by response
- Notes paucity of level 1-2 evidence; most modalities rest on lower-grade evidence and clinical experience
- Emphasises early, function-directed therapy rather than rest/immobilisation
Does Evidence Support Physiotherapy for Adult CRPS-I? Systematic Review
- Systematic review of 11 studies (5 RCTs) on physiotherapy for adult CRPS-I
- Good-to-very-good quality level II evidence that graded motor imagery reduces pain
- No evidence found to support commonly recommended treatments such as stress loading
- Heterogeneity prevented meta-analysis; physiotherapy often combined with medical management
Spinal Cord Stimulation for Chronic Refractory CRPS (RCT)
- RCT: 36 patients SCS plus physiotherapy vs 18 physiotherapy alone (CRPS over 6 months)
- Mean pain fell 2.4cm on a 10cm VAS at 6 months vs +0.2cm in controls (p less than 0.001)
- 39% of SCS patients much improved vs 6% of controls; no significant functional gain
- Complications requiring further procedures in 6 of 24 implanted patients