Fixed Lateral Dislocation | Flexion Contracture | Extensor Realignment
- Patella dislocated laterally at birth with fixed flexion contracture and valgus
- Associated with external tibial torsion and quadriceps contracture
- Differs from habitual dislocation which reduces in extension
- Requires extensive lateral release, medial reefing and tubercle medialisation
- Untreated leads to permanent deformity and early arthritis
- “Fixed lateral patella with absent medial retinaculum
- “Genu valgum and external tibial rotation are hallmarks
- “Differentiate fixed congenital from reducible habitual type
- “Early surgery before age 2 improves extensor mechanism balance
Fixed lateral dislocation. Patella cannot be reduced even under anaesthesia. Knee flexion contracture of 20-60 degrees with valgus deformity.
Quadriceps contracture. Vastus lateralis and iliotibial band tight. External tibial torsion greater than 30 degrees common. Hypoplastic lateral femoral condyle.
Vs habitual dislocation. Habitual reduces in extension and dislocates only in flexion. Congenital remains dislocated in all positions.
Operate before age 2. Allows remodelling of trochlea and prevents fixed contractures. Delay increases risk of permanent valgus and torsion.
- Diagnosis
- Clinical + X-ray skyline view
- Treatment
- Serial casting then surgery by 12-18 months
- Key Pearl
- Early realignment prevents permanent valgus
- Diagnosis
- Habitual dislocation pattern
- Treatment
- Isolated vastus lateralis release
- Key Pearl
- Avoid over-release causing medial instability
- Diagnosis
- Missed congenital or syndromic
- Treatment
- Extensive release + tubercle transfer
- Key Pearl
- May require femoral osteotomy for valgus
FIXEDCongenital vs Habitual Dislocation
Hook:Congenital dislocation stays FIXED from birth - do not confuse with reducible habitual type!
VALGUSAssociated Findings
Hook:VALGUS deformity with lateral contracture defines the congenital pattern!
Overview and Epidemiology
Congenital dislocation of the patella is a rare but important paediatric condition that presents at birth with a fixed lateral position of the patella. Unlike habitual dislocation, which is reducible in extension, the congenital form remains dislocated in all positions and is associated with significant flexion contracture, valgus deformity and external tibial torsion. Early recognition and surgical realignment before age two allows trochlear remodelling and prevents lifelong extensor mechanism dysfunction and early osteoarthritis.
- Incidence: Less than 1 in 100000 live births
- Bilateral: Up to 40 percent of cases
- Sex: Slight female predominance
- Associations: Nail-patella syndrome, trisomy 21, Rubinstein-Taybi syndrome
- Gait abnormality: External rotation and valgus thrust
- Knee function: Limited extension and instability
- Growth disturbance: Progressive valgus and torsion
- Long-term: Early patellofemoral arthritis if untreated
Pathophysiology
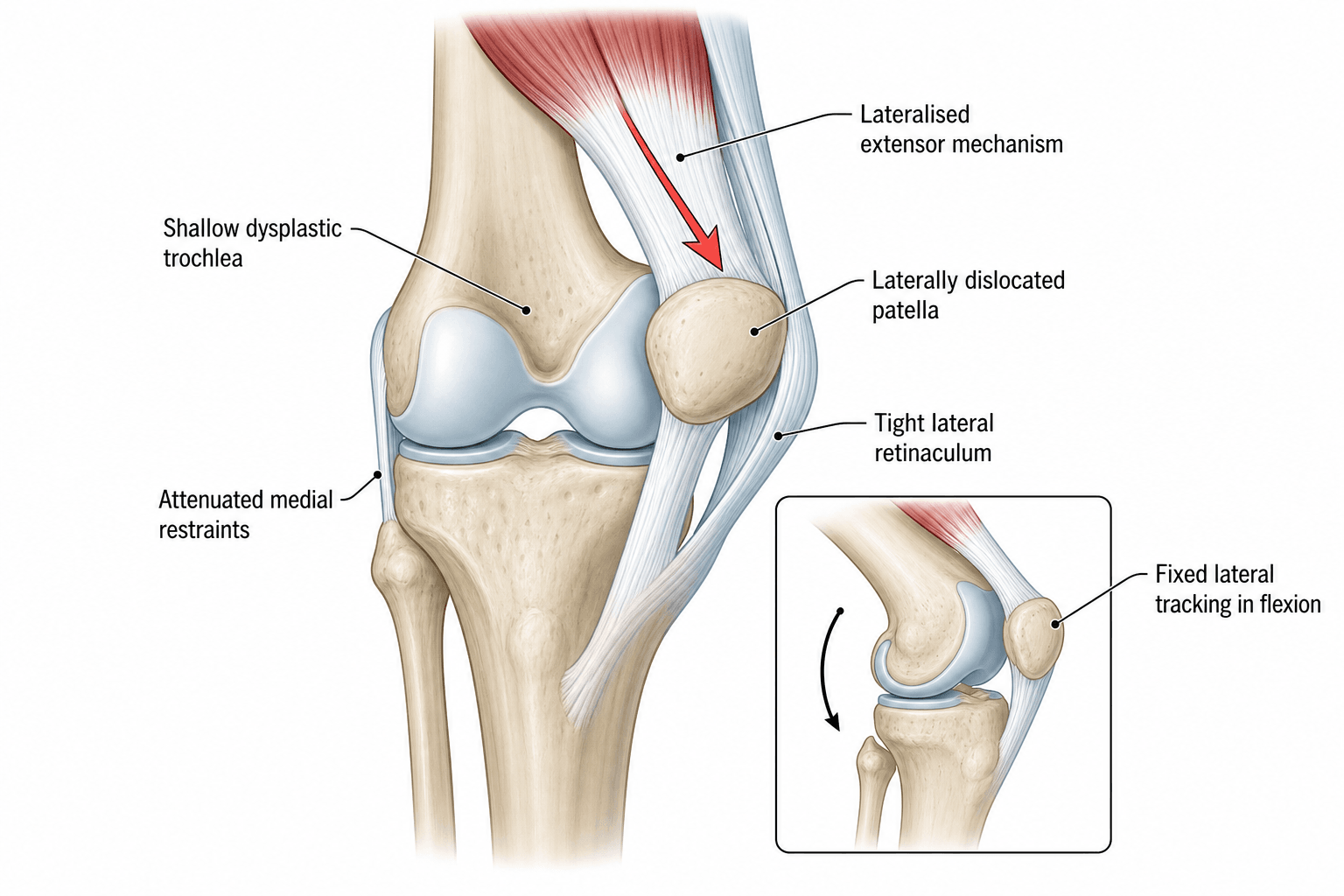
The patella normally develops within the quadriceps tendon and engages the trochlear groove by 12-16 weeks gestation. In congenital dislocation, failure of internal rotation of the quadriceps muscle mass during limb bud development leaves the patella permanently lateral. The vastus lateralis and iliotibial band become contracted, the medial retinaculum fails to develop, and the lateral femoral condyle remains hypoplastic. The tibia develops external torsion as a secondary adaptation to the laterally displaced extensor pull.
Failure of quadriceps internal rotation. The entire extensor apparatus rotates externally during embryogenesis. Patella never enters trochlear groove. Medial capsular structures remain rudimentary.
Lateral contracture and bony remodelling. Vastus lateralis and ITB shorten. Lateral condyle hypoplasia deepens the lateral gutter. External tibial torsion develops from unbalanced forces.
- Change
- Failed internal rotation of quadriceps
- Result
- Patella remains lateral
- Clinical Consequence
- Fixed dislocation at birth
- Change
- Lateral structures contract
- Result
- Flexion contracture develops
- Clinical Consequence
- Knee cannot extend fully
- Change
- Weight-bearing on valgus knee
- Result
- Progressive genu valgum
- Clinical Consequence
- Worsening mechanical axis
Classification and Types

Congenital Fixed Lateral Dislocation
Present at birth, irreducible in any position. Associated with flexion contracture 20-60 degrees, genu valgum and external tibial torsion. Quadriceps mechanism is contracted and laterally displaced. Medial retinaculum absent or severely attenuated. Trochlea is flat or convex.
- Congenital Fixed
- Birth, fixed
- Habitual
- Childhood, reducible
- Recurrent Traumatic
- After trauma
- Congenital Fixed
- Never reduces
- Habitual
- Reduces in extension
- Recurrent Traumatic
- Reduces with manipulation
- Congenital Fixed
- Flexion + valgus fixed
- Habitual
- Minimal contracture
- Recurrent Traumatic
- None or mild
- Congenital Fixed
- Extensive lateral release
- Habitual
- Isolated release
- Recurrent Traumatic
- MPFL reconstruction
Fixed congenital type requires comprehensive realignment addressing all deforming forces.
Clinical Assessment
- Birth history: Noted at delivery or neonatal check
- Family history: Syndromic associations or other congenital anomalies
- Function: Delayed walking, external rotation gait, falls
- Pain: Usually minimal in infancy, appears with activity later
- Inspection: Patella lateral, knee flexed, valgus, external foot progression
- Palpation: Patella fixed lateral, absent medial retinaculum, prominent lateral condyle
- ROM: Fixed flexion contracture 20-60 degrees, limited active extension
- Special tests: Apprehension negative (already dislocated), Q-angle increased
Technique: Attempt reduction with knee in full extension under anaesthesia if possible. In congenital fixed type the patella remains lateral even in extension. In habitual type the patella reduces fully in extension and only dislocates with flexion. This distinction determines the extent of surgery required.
- Onset
- Birth
- Reducibility
- Never reduces
- Associated Features
- Flexion contracture, valgus, ER torsion
- Key Test
- Fixed lateral on all views
- Onset
- Early childhood
- Reducibility
- Reduces in extension
- Associated Features
- Mild valgus, tight vastus lateralis
- Key Test
- Dislocates only in flexion
- Onset
- Variable
- Reducibility
- Variable
- Associated Features
- Nail-patella, trisomy 21, ligamentous laxity
- Key Test
- Systemic features
- Onset
- After injury
- Reducibility
- Reducible
- Associated Features
- Normal trochlea, MPFL tear
- Key Test
- Positive apprehension
Nail-patella syndrome features absent or hypoplastic patellae, nail dysplasia and iliac horns. Trisomy 21 has ligamentous laxity and increased risk of fixed dislocation. Always examine hands, nails and perform karyotype if dysmorphic features present. Syndromic cases may require modified surgical goals.
Investigations

Imaging Protocol
Views: AP, lateral, skyline (Merchant or Laurin) of both knees
Look for: Patella position lateral to trochlea, hypoplastic lateral condyle, shallow trochlea, patella alta
Clinical correlation: In infants the patella is cartilaginous and may not be visible on X-ray until 3-5 years
Indication: Assess trochlear morphology, tibial tubercle-trochlear groove (TT-TG) distance, femoral and tibial version
Threshold: TT-TG greater than 20 mm indicates need for tubercle medialisation
Pre-op planning: Quantify external tibial torsion and femoral anteversion for derotation planning
Indication: Evaluate cartilage status, MPFL remnant, quadriceps muscle quality, associated ligamentous anomalies
Findings: Absent medial retinaculum, contracted vastus lateralis, chondral damage if delayed presentation
Reconstruction planning: Determines need for MPFL reconstruction versus soft-tissue realignment only
X-rays in infants are limited because the patella is unossified until age 3-5 years. Ultrasound can confirm the cartilaginous patella position lateral to the femur. Do not delay diagnosis waiting for ossification. Clinical examination and attempted reduction are diagnostic.
Management Algorithm
Timing of Intervention
Goal: Achieve reduction and realignment before age two to allow trochlear remodelling and prevent progressive valgus and torsion.
Treatment Timeline
Serial casting: Weekly long-leg casts to gradually correct flexion contracture Monitor: Skin integrity and neurovascular status Decision point: If not reduced by 6 months proceed to surgery
Extensive lateral release: ITB, vastus lateralis, lateral capsule Medial reefing: Plication of medial retinaculum Tubercle transfer: If TT-TG elevated and age permits Post-op: Long-leg cast in extension 6 weeks
Combined procedures: Lateral release, medial reefing, tubercle medialisation, possible femoral derotation Consider: Distal femoral osteotomy for severe valgus Goal: Mechanical axis correction and stable tracking
The trochlea remodels only when the patella is reduced early. After age 5-6 years the trochlear shape is largely established and outcomes of realignment are poorer. Operate before the child starts school if possible.
Distal Realignment in the Skeletally Immature Knee
A true tibial tubercle osteotomy cannot be performed in the young child: the tubercle is an apophysis continuous with the proximal tibial physis, and disturbing it risks growth arrest and progressive genu recurvatum from an anterior tether. In the immature knee, distal realignment of the extensor mechanism therefore relies on soft-tissue transfers rather than moving bone.
- Roux-Goldthwait procedure: the patellar tendon is split longitudinally and the lateral half is detached distally and transferred medially (passed beneath the medial half and sutured to periosteum/pes), shifting the line of pull medially without touching the apophysis.
- Galeazzi semitendinosus tenodesis: the semitendinosus, left attached distally, is rerouted and fixed to the patella as a medial check-rein - a physeal-sparing restraint against lateral dislocation.
- Medial soft-tissue realignment (medial reefing, VMO advancement) plus extensive lateral release are combined with one of the above.
- A formal tibial tubercle (Elmslie-Trillat-type) osteotomy is reserved until the apophysis is closing or closed (adolescence), when the TT-TG distance can be corrected directly.
Q: Why is a tibial tubercle transfer avoided in the skeletally immature knee, and what is used instead? A: The tibial tubercle apophysis is contiguous with the proximal tibial physis; an osteotomy through it risks anterior physeal arrest and genu recurvatum with growth disturbance. Distal realignment in children is therefore performed with soft-tissue transfers - the Roux-Goldthwait hemi-patellar-tendon transfer or a Galeazzi semitendinosus tenodesis - reserving a formal tubercle osteotomy for the adolescent with a closing apophysis.
LATERALSurgical Steps for Realignment
Hook:LATERAL release is the cornerstone - extensive lateral structures must be addressed!
Complications
- Incidence
- 10-20 percent after surgery
- Risk Factors
- Inadequate lateral release, persistent valgus
- Management
- Revision realignment or trochleoplasty
- Incidence
- 5-10 percent
- Risk Factors
- Excessive tubercle transfer
- Management
- Lateral release revision
- Incidence
- 5-15 percent
- Risk Factors
- Over-release of lateral structures
- Management
- Anterior closing wedge osteotomy
- Incidence
- 15-25 percent
- Risk Factors
- Prolonged casting, scarring
- Management
- Manipulation under anaesthesia
- Incidence
- Rare
- Risk Factors
- Excessive medial reefing
- Management
- Patellar tendon lengthening
The most common cause of failure is inadequate release of the vastus lateralis and iliotibial band. The release must be extensive proximally to the mid-thigh. Incomplete release leaves a lateral tether that pulls the patella out again. Always confirm free medial translation of the patella to the midline after release before closing.
The Contracted Quadriceps: When Release Is Not Enough
In long-standing or severe congenital dislocation the quadriceps - especially rectus femoris and vastus lateralis - is itself short and fibrotic, not merely laterally tethered. Lateral release and medial reefing alone then cannot bring the patella distally into the trochlea without excessive tension; forcing the reduction risks patella baja, skin necrosis or early recurrence.
- V-Y quadricepsplasty (quadriceps lengthening / Z-plasty): an inverted-V incision in the contracted quadriceps tendon and rectus, closed in a Y, that lengthens the extensor mechanism so the reduced patella seats in the groove while still allowing knee flexion. It is the key adjunct once a fixed flexion-extension mismatch persists after release.
- Extensor-mechanism mobilisation (Stanisavljevic principle): subperiosteal release of the whole laterally displaced extensor apparatus off the lateral femur and proximal tibia so it can be rotated medially as a unit.
- Intra-operative rule: if, after a complete lateral release, the patella still will not reach the midline trochlea with the knee extended, the quadriceps is the remaining tether and must be lengthened rather than forced.
Q: After a complete lateral release the patella still will not sit in the trochlea without tension - what is the problem and the solution? A: The quadriceps myotendinous unit is intrinsically contracted and short, not just laterally tethered. The solution is to lengthen the extensor mechanism with a V-Y quadricepsplasty (combined with proximal mobilisation of the displaced extensor apparatus), permitting tension-free patellar reduction and knee flexion rather than forcing reduction and producing patella baja or recurrence.
Outcomes and Prognosis
- Expected Outcome
- Stable tracking, trochlear remodelling
- Reoperation Rate
- Less than 10 percent
- Long-term Function
- Near-normal gait and function
- Expected Outcome
- Good stability, mild residual valgus
- Reoperation Rate
- 15-20 percent
- Long-term Function
- Good for daily activities
- Expected Outcome
- Variable stability, persistent valgus
- Reoperation Rate
- 25-40 percent
- Long-term Function
- Functional limitation common
Best prognosis: Surgery before age two, complete lateral release, correction of torsion and valgus, compliant post-operative rehabilitation. Poor prognosis: Delayed presentation after age five, syndromic laxity, incomplete release, persistent external torsion. Key threshold: Age two years - outcomes decline sharply after this window because trochlear remodelling potential is lost.
Guidelines, Registries & Global Practice
- Rare condition with incidence under 1 per 100000 births worldwide
- Bilateral cases reported consistently across all populations
- Syndromic associations (nail-patella, trisomy 21) recognised universally
- Missed diagnosis common in resource-limited settings without neonatal screening
- High-resource: Early ultrasound screening, CT planning, custom bracing post-op
- Limited-resource: Clinical diagnosis, serial casting with plaster, delayed surgery common
- Universal principle: Outcome depends on age at reduction more than technology
- Surgery: Extensive lateral release principles are the same globally
- Diagnosis emphasis
- Clinical differentiation of fixed vs habitual
- Surgical timing
- Surgery by 12-18 months for best remodelling
- Key technical points
- Extensive proximal lateral release mandatory
- Diagnosis emphasis
- Ultrasound confirmation in infants
- Surgical timing
- Serial casting first, surgery under age 2
- Key technical points
- Combined soft-tissue and tubercle transfer
- Diagnosis emphasis
- CT for TT-TG and version planning
- Surgical timing
- Individualised timing based on deformity
- Key technical points
- Address valgus and torsion in older children
No dedicated international registry exists for congenital patellar dislocation due to extreme rarity. Evidence is limited to small case series from tertiary paediatric centres. Principles are consistent across guidelines: differentiate fixed from habitual type, release lateral structures extensively, correct alignment early, and monitor for recurrence and arthritis long-term.
Controversies & Areas of Uncertainty
Some surgeons perform tibial tubercle osteotomy as early as age 4-5 years while others wait until physeal closure to avoid growth disturbance. Evidence is insufficient to define a safe lower age limit.
Trochleoplasty is rarely performed in young children because the trochlea remodels after reduction. In older children with established dysplasia the procedure remains controversial with limited paediatric data.
Over-plication risks patella baja and limited flexion. Under-plication risks recurrence. No validated intraoperative tensioning protocol exists.
Staged versus simultaneous surgery and the interval between sides are decided case-by-case. No comparative studies guide practice.
MCQ Practice Points
Q: What is the primary embryological cause of congenital patellar dislocation? A: Failure of internal rotation of the quadriceps muscle mass during limb bud development. This leaves the entire extensor mechanism laterally displaced, the patella never engages the trochlea, and the medial retinaculum fails to form.
Q: How do you differentiate congenital fixed dislocation from habitual dislocation on examination? A: Attempt reduction in full extension. In congenital fixed type the patella remains lateral in all positions including extension. In habitual type the patella reduces fully in extension and only dislocates with flexion beyond 30-40 degrees.
Q: What is the key surgical principle in congenital fixed dislocation? A: Extensive lateral release of the iliotibial band and vastus lateralis from mid-thigh to tubercle. Incomplete proximal release is the most common cause of recurrence. Medial reefing and tubercle transfer are adjuncts performed after adequate release.
Q: What is the ideal age for surgical realignment and why? A: 12-18 months. This window allows trochlear remodelling once the patella is reduced and prevents progressive valgus and external torsion. Surgery after age five has poorer outcomes because the trochlear shape is established and bony deformity is fixed.
Q: What torsional abnormality is commonly associated and how is it addressed? A: External tibial torsion greater than 30 degrees. It develops secondary to the laterally displaced extensor pull. If severe it is corrected with a tibial derotation osteotomy at the time of realignment surgery.
Clinical Imaging
Radiographic Features of Congenital Patellar Dislocation
Congenital dislocation presents with the patella permanently displaced lateral to the trochlear groove on all views. Skyline views are essential but difficult in young children. The femoral condyles appear hypoplastic and the trochlea is shallow or absent. Standing alignment films demonstrate genu valgum and external tibial torsion.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-week-old infant is referred with a fixed lateral patellar dislocation noted at birth. The knee has a 40-degree flexion contracture and 15-degree valgus. Attempted reduction under anaesthesia fails. How do you manage this child?”
“A 7-year-old presents with longstanding external rotation gait and inability to fully extend the knee. Examination shows the patella fixed laterally with 30-degree valgus and 25-degree external tibial torsion. This was not treated in infancy. What is your surgical plan?”
Key Anatomy and Development
- Failure of quadriceps internal rotation leaves patella lateral from birth
- Medial retinaculum absent, lateral structures contracted
- Lateral femoral condyle hypoplastic, trochlea shallow
- External tibial torsion and genu valgum develop secondarily
Diagnosis
- Fixed lateral patella in all positions including extension
- Flexion contracture 20-60 degrees with valgus
- Differentiate from habitual (reduces in extension)
- Ultrasound in infants, skyline X-ray once ossified, CT for TT-TG
Treatment Algorithm
- Serial casting 0-6 months to correct contracture
- Surgery 12-18 months: extensive lateral release + medial reefing
- Add tubercle transfer if TT-TG greater than 20 mm
- Derotation or valgus osteotomy in older or missed cases
Surgical Pearls
- Release ITB and vastus lateralis proximally to mid-thigh
- Confirm free medial translation of patella before closing
- Avoid over-medialisation causing patella baja
- Long-leg cast in extension 6 weeks post-op
Complications and Prognosis
- Recurrence 10-20 percent if release incomplete
- Best outcomes with surgery before age 2
- Delayed surgery increases arthritis risk
- Monitor for over-medialisation and recurvatum
Evidence Base and Key Trials
Fixed (Congenital) Patellar Dislocation
- Review of fixed congenital patellar dislocation emphasizing clinical presentation and surgical realignment strategies
Congenital Dislocation of the Patella - Surgical Treatment Rationale and Literature Review
- Literature review and case-based rationale for staged surgical reconstruction in congenital patellar dislocation
Femoral Shortening Osteotomy in Managing Congenital Patellar Dislocation
- Case report demonstrating femoral shortening osteotomy as adjunct for managing congenital patellar dislocation with associated deformities
Surgical Treatment for Congenital Dislocation of the Patella in a Young Adult
- Case report of successful surgical reconstruction for congenital patellar dislocation presenting in young adulthood
Postaxial Hypoplasia of the Lower Extremity Associated with Congenital Dislocation of the Patella
- Case report highlighting syndromic associations and surgical considerations in congenital patellar dislocation with limb hypoplasia