Rhabdomyolysis | Hyperkalemia | Myoglobinuria | Acute Kidney Injury
- Crush syndrome = systemic manifestation after release; crush injury = localized damage
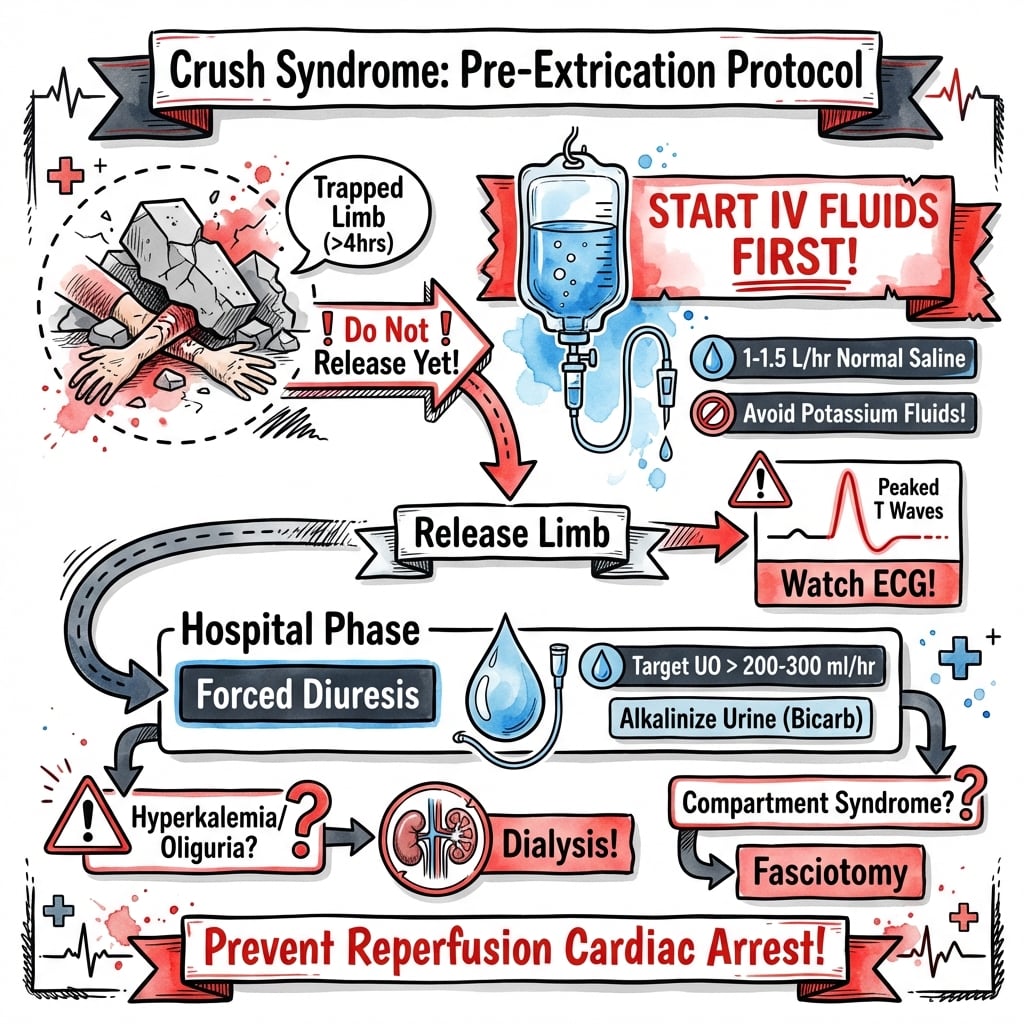
- IV fluids MUST start BEFORE extrication - prevents reperfusion cardiac arrest
- Lethal triad: Hyperkalemia (cardiac arrest), metabolic acidosis, hypocalcemia
- Target urine output 200-300mL/hour to flush myoglobin and prevent AKI
- Fasciotomy threshold: Compartment pressure greater than 30mmHg or delta pressure less than 30mmHg
- “Pre-hospital IV fluids before release distinguishes survivors from non-survivors
- “Hyperkalemia kills in minutes - treat before other priorities if K+ greater than 6.5
- “Dark tea-colored urine = myoglobinuria until proven otherwise
- “Hypocalcemia from calcium sequestration in damaged muscle - do NOT aggressively replace
Crush syndrome kills at the moment of release, not while the patient is trapped. Never extricate a long-entrapped limb without intravenous (or intraosseous) fluids running and a plan for hyperkalaemia. Treat hyperkalaemia and hypovolaemia before any orthopaedic intervention.
Overview & Epidemiology
Definitions
Crush injury is the direct local tissue damage caused by sustained mechanical compression of a body part. Crush syndrome (traumatic rhabdomyolysis) is the systemic sequelae - rhabdomyolysis, electrolyte disturbance and acute kidney injury (AKI) - that follow compression and, critically, the moment of reperfusion when the limb is released. The condition was first characterised by Bywaters and Beall during the London Blitz of 1941, who linked limb crush to dark urine and fatal renal failure.
Who Gets It
Crush syndrome occurs after earthquakes and building collapse (the leading cause of mass-casualty crush), industrial and motor-vehicle entrapment, and prolonged immobilisation ("long-lie" after collapse, overdose, or being found-down). Risk rises sharply with entrapment beyond roughly 4-6 hours, large muscle-mass involvement (thigh, trunk, bilateral limbs), and delayed or absent pre-extrication resuscitation. After major earthquakes a significant minority of rescued survivors develop crush-related AKI, and the proportion requiring dialysis depends heavily on rescue speed and access to renal services.
Pathophysiology
The Compression-Reperfusion Mechanism
Pathophysiological Cascade
Direct pressure plus arterial occlusion produces myocyte ischaemia. ATP depletion disables the Na+/K+ and Ca2+ pumps, so sodium, water and calcium flood into cells while potassium and myoglobin leak out. Muscle is relatively protected from acute systemic toxicity while still compressed because the venous outflow is occluded.
On extrication, restored blood flow flushes accumulated potassium, myoglobin, phosphate, urate, lactate and creatine kinase into the systemic circulation. This sudden potassium and acid load can precipitate ventricular fibrillation within minutes - the classic "smiling death" or extrication death.
Reperfused muscle sequesters massive volumes of fluid (litres per limb), causing profound hypovolaemia, hypotension and worsening renal hypoperfusion. Compartment pressures rise, perpetuating ischaemia.
AKI results from three converging mechanisms - renal vasoconstriction (hypovolaemia plus scavenging of nitric oxide by myoglobin), intratubular cast formation (myoglobin precipitating with Tamm-Horsfall protein in acidic urine), and direct myoglobin/ferrihaemate tubular toxicity with oxidative injury.
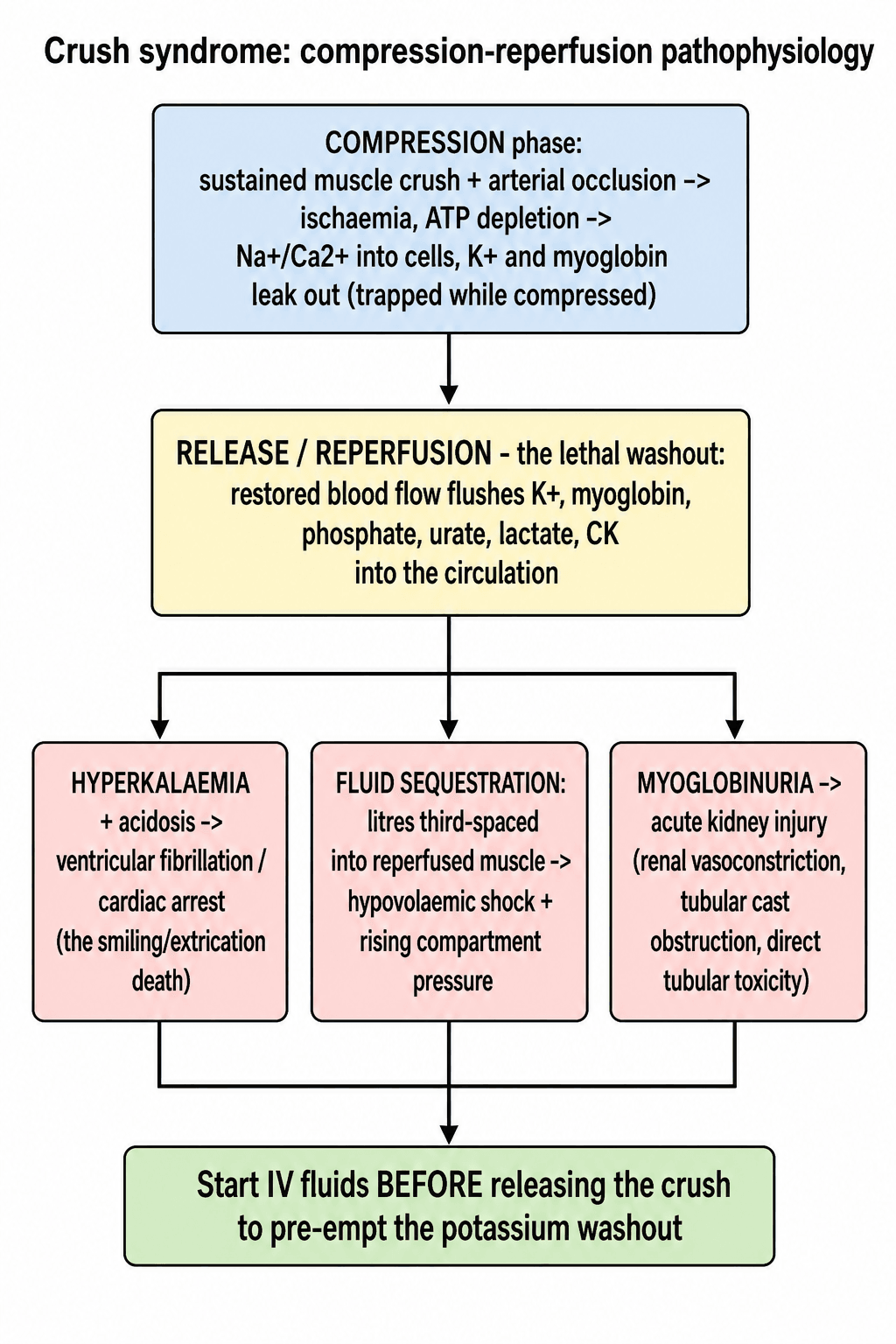
The single most examined concept: the patient is often haemodynamically deceptive while trapped, then deteriorates or arrests on release. This is why intravenous fluids must be running before the crushing force is removed - to dilute the potassium load and pre-empt the reperfusion washout.
Clinical Presentation
Recognising Crush Syndrome
- Swollen, tense, often pulseless limb
- Pain out of proportion; pain on passive stretch
- Sensory loss, paraesthesia, motor weakness
- Skin necrosis, blistering, fixed compression marks
- Hypovolaemic shock after release (third-spacing)
- Dark tea/cola-coloured urine (myoglobinuria)
- Cardiac arrhythmia from hyperkalaemia
- Oliguria progressing to anuria
- Nausea, confusion, features of metabolic acidosis
A trapped patient may look stable with a normal blood pressure because the compressed limb is not yet reperfused. Do not be reassured - the metabolic load is building and will be released the moment compression ends.
Differential Diagnosis
- Distinguishing Features
- Prolonged compression, rising CK, hyperkalaemia, myoglobinuria, AKI after release
- Key Discriminator
- History of entrapment plus systemic rhabdomyolysis
- Distinguishing Features
- Tense compartment, pain on passive stretch, usually after fracture/reperfusion
- Key Discriminator
- Local limb-threat without the systemic metabolic load (they overlap)
- Distinguishing Features
- Pulseless, cold, pale limb; hard signs of vascular injury
- Key Discriminator
- Vascular imaging and absent distal flow rather than diffuse muscle necrosis
- Distinguishing Features
- Statins, exertion, seizures, NMS, toxins; high CK without crush history
- Key Discriminator
- No mechanical entrapment
- Distinguishing Features
- Dipstick blood positive, plasma pink, low haptoglobin
- Key Discriminator
- Plasma colour and haemolysis markers, not muscle injury
- Distinguishing Features
- Fever, vasodilatation, infection source
- Key Discriminator
- Sepsis markers and absence of massive CK rise
Crush Care Algorithm
Management
1. Pre-extrication fluids (prevents cardiac arrest at release) 2. Treat hyperkalemia (immediate life threat) 3. Massive IV fluid resuscitation (prevents AKI) 4. Cardiac monitoring (continuous) 5. Consider dialysis early (if oliguria persists)
Volume Resuscitation Protocol
Fluid Management
1-1.5L/hour of 0.9% saline starting before release. Continue through extrication. If delayed extrication, may need 1L every 30 minutes.
1-1.5L/hour continuing in hospital. Target urine output 200-300mL/hour. May require 10-12L in first 24 hours. Central line and arterial line recommended.
Add 50-100mEq sodium bicarbonate to each liter of half-normal saline. Target urine pH greater than 6.5. Monitor serum pH (avoid greater than 7.50).
Adjust based on urine output, electrolytes, and clinical status. May continue high-volume fluids for 48-72 hours. Monitor for fluid overload.
Normal saline is preferred because it does not contain potassium (unlike Hartmann's/Ringer's lactate). Lactated solutions should be avoided in crush syndrome due to the potassium content.
Surgical Management
Compartment Syndrome in Crush Injury
Crush injuries carry high risk of compartment syndrome. Fasciotomy is indicated if: compartment pressure greater than 30mmHg, delta pressure (DBP - compartment pressure) less than 30mmHg, or clinical signs present. Do not delay for pressure measurements if clinical picture is clear.
- Threshold
- Greater than 30mmHg
- Urgency
- Emergency fasciotomy
- Threshold
- Less than 30mmHg (DBP - CP)
- Urgency
- Emergency fasciotomy
- Threshold
- Pain on passive stretch, tense compartment
- Urgency
- Emergency fasciotomy
- Threshold
- Before reperfusion
- Urgency
- Prophylactic fasciotomy
- Threshold
- High clinical suspicion
- Urgency
- Low threshold for fasciotomy
For prolonged entrapment (greater than 6 hours) or severe crush injury with anticipated massive swelling, consider prophylactic fasciotomy at time of extrication or early in hospital course. This prevents the devastating consequences of delayed compartment syndrome.
Complications
- Incidence
- 50% (30-50% need dialysis)
- Timing
- 24-72 hours
- Management
- Fluids, dialysis if refractory
- Incidence
- 30-40%
- Timing
- Minutes to hours (at extrication)
- Management
- Calcium, insulin, dialysis
- Incidence
- 20-30%
- Timing
- Hours to days
- Management
- Emergency fasciotomy
- Incidence
- 15-20%
- Timing
- 24-48 hours
- Management
- Treat underlying cause, FFP, platelets
- Incidence
- 10-20%
- Timing
- Days to weeks
- Management
- Debridement, antibiotics
- Incidence
- 10-15%
- Timing
- 24-72 hours
- Management
- Ventilatory support, lung protective strategy
- Incidence
- 10-20%
- Timing
- Days
- Management
- ICU support, treat underlying cause
- Incidence
- 10-15%
- Timing
- Days to weeks
- Management
- For non-viable limb, uncontrolled infection
- Incidence
- 10-20%
- Timing
- Variable
- Management
- Prevention through early aggressive treatment
Poor prognostic factors include: greater than 6 hours entrapment, trunk or bilateral limb involvement, CK greater than 75,000 U/L, delayed fluid resuscitation, DIC, and multi-organ failure. Early aggressive management significantly improves survival.
Guidelines, Registries & Global Practice
Global Epidemiology
Crush syndrome arises in three broad contexts worldwide: natural disasters (earthquakes are the dominant cause of mass-casualty crush, e.g. Marmara 1999, Kashmir 2005, Haiti 2010, Turkey-Syria 2023), industrial and motor-vehicle entrapment (mining, construction, building collapse, prolonged extrication after road traffic collisions), and prolonged immobilisation (collapse with "long-lie", drug overdose, the elderly found-down). After a major earthquake, crush-related AKI develops in a substantial minority of rescued survivors; the proportion needing dialysis varies enormously with rescue speed and access to renal services - illustrated by the Marmara series (74.6% of renal victims dialysed) versus the rural Kashmir earthquake, where far fewer reached dialysis at all.
Side-by-Side Guidance
- Emphasis
- Disaster nephrology
- Key Position
- Pre-extrication and early high-volume isotonic fluids; early dialysis mobilisation; avoid potassium-containing fluids
- Emphasis
- Renal protection
- Key Position
- Volume expansion as primary renoprotection; routine bicarbonate/mannitol not supported by strong evidence
- Emphasis
- Limb & compartment
- Key Position
- Low threshold for fasciotomy; serial compartment assessment; damage-control surgery
- Emphasis
- Pre-hospital & field
- Key Position
- IV/IO access and fluids before release; cardiac monitoring; treat hyperkalaemia empirically in the field
- Emphasis
- Cardiac arrest
- Key Position
- Hyperkalaemia is a reversible cause of arrest; give calcium early, consider dialysis
High- vs Limited-Resource Practice Variation
In well-resourced settings, rapid extrication, point-of-care potassium, continuous renal replacement therapy and intensive care allow aggressive support and comparatively low renal-cause mortality. In limited-resource or austere disaster settings, delayed rescue, scarce dialysis and limited transport drive higher rates of hyperkalaemic death and amputation; field priorities shift toward early fluids, empirical hyperkalaemia treatment, and triage of who can be transferred for renal replacement. International coordination (e.g. deploying mobile dialysis capacity after earthquakes) materially changes outcomes.
Controversies and Areas of Uncertainty
Standard orthopaedic teaching is to fasciotomy a genuine acute compartment syndrome. In crush syndrome this is genuinely contested: disaster-nephrology guidance (Renal Disaster Relief Task Force / Sever) cautions against routine or prophylactic fasciotomy, because cutting down on devitalised muscle converts a closed injury into an open one and creates a portal for infection and sepsis — a leading cause of late death after crush (note the Marmara data: deaths were driven by sepsis/DIC, not renal failure alone). The reconciled position: reserve fasciotomy for a tense compartment in a still-VIABLE limb with measured raised pressures (or unequivocal clinical signs); do NOT reflexively decompress a limb whose muscle is already dead — that limb may be better served by resuscitation, demarcation, or amputation. This is why measured pressures (delta <30 mmHg) matter more here than elsewhere.
A proximal tourniquet applied BEFORE releasing a long-entrapped, clearly non-salvageable (mangled) limb can blunt the lethal reperfusion washout of potassium and myoglobin, and is part of field-amputation decision-making in mass-casualty settings. It is selective and debated — not routine — and must not delay fluid resuscitation; for a salvageable limb the priority remains pre-extrication fluids rather than ischaemic tourniquet time.
Aggressive volume expansion is the proven renoprotective measure. Bicarbonate alkalinisation (urine pH >6.5) and mannitol are widely taught but the supporting evidence is weak/observational; mannitol may harm if the patient is hypovolaemic and is not given routinely. Fluids first; alkalinisation/mannitol are adjuncts, not substitutes.
For a non-viable, heavily contaminated or overwhelmingly toxic limb, early amputation can be life-saving by removing the source of ongoing potassium/myoglobin load and infection, and is sometimes the correct disaster decision over repeated debridement of dead muscle. The threshold is a clinical judgement balancing systemic toxicity against limb salvage.
Controversies & Areas of Uncertainty
Isotonic saline is favoured to avoid potassium, but large-volume saline risks hyperchloraemic acidosis; some advocate balanced (low-potassium) crystalloid once hyperkalaemia is controlled. Optimal rate (commonly cited 1-1.5 L/h, titrated to urine output) is consensus-based, not trial-proven.
Bicarbonate to raise urine pH above 6.5 is widely taught, but Brown et al. and others show no clear added benefit over volume alone; alkalinisation risks worsening hypocalcaemia and metabolic alkalosis.
Once routine, now largely abandoned - no proven benefit and potential harm (osmotic nephrosis, volume shifts) in hypovolaemic patients. Reserve, if ever, for well-hydrated patients with persistent oliguria.
Routine prophylactic fasciotomy in crush limbs is debated: it can prevent ischaemic necrosis but converts a closed injury into an open wound with infection and bleeding risk, especially in disaster settings with limited sterility. Decompress on clear indication; individualise the prophylactic decision.
Memory Aids
CBIGKDC-BIG-K-DROP (Hyperkalaemia)
Hook:Stabilise the heart first, then shift, then remove the potassium.
FLUSHFLUSH (Crush Priorities)
Hook:FLUSH the myoglobin and FLUSH the potassium before it stops the heart.
CCCC4 Cs of Muscle Viability
Hook:Assessed at fasciotomy; extensive non-viable muscle driving toxicity may mandate amputation.
AEIOUDialysis Triggers (AEIOU)
Hook:The classic dialysis vowels, applied to the crush patient.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are called to a building collapse where a 35-year-old construction worker has been trapped under concrete debris for 5 hours. His right leg is crushed. Rescue teams are preparing to extricate him. What is your management?”
“A 28-year-old woman was trapped in a car accident for 3 hours with her legs crushed. She was extricated by paramedics and appeared stable initially. Ten minutes after extrication, she develops VF arrest. What is the likely cause and how would you manage this?”
“A 40-year-old man is admitted following a mining accident. His right thigh was crushed for 4 hours. He is hypotensive, has dark urine, and his thigh is massively swollen and tense. Potassium is 6.8, CK is 85,000, creatinine is rising. His leg is pulseless. How would you manage him?”
Definitions
- Crush injury = localized tissue damage from compression
- Crush syndrome = SYSTEMIC manifestation after release (rhabdomyolysis, AKI, hyperkalemia)
- Develops after greater than 4-6 hours of compression
- Reperfusion injury = metabolic derangement at moment of release
Lethal Triad
- Hyperkalemia - causes cardiac arrest (K+ greater than 6.5 is dangerous)
- Metabolic acidosis - lactic + phosphoric acid
- Hypocalcemia - sequestered in muscle (do NOT aggressively replace)
Pre-Extrication Protocol
- IV access BEFORE release - never extricate without IV
- Normal saline 1-1.5L/hour (NOT Hartmann's - contains K+)
- Cardiac monitoring if available
- Intraosseous access if IV impossible
Fluid Targets
- Urine output 200-300mL/hour (3mL/kg/hr)
- May need 10-12L in first 24 hours
- Alkalinize urine to pH greater than 6.5 with bicarbonate
- Avoid nephrotoxins (NSAIDs, aminoglycosides, contrast)
Hyperkalemia Treatment (C-BIG-K-DROP)
- Calcium gluconate 10% 10-20mL IV (membrane stabilization)
- Bicarbonate 50-100mEq IV (K+ shift)
- Insulin 10U + Dextrose 50mL 50% (K+ shift)
- Salbutamol 10-20mg nebulized (K+ shift)
- Kayexalate/Dialysis (K+ removal)
Fasciotomy Indications
- Compartment pressure greater than 30mmHg
- Delta pressure (DBP - CP) less than 30mmHg
- Clinical: pain on passive stretch + tense compartment
- Prophylactic for prolonged ischemia greater than 6 hours
Dialysis Indications
- Refractory hyperkalemia (K+ greater than 6.5 despite treatment)
- Severe acidosis (pH less than 7.1)
- Fluid overload/pulmonary edema
- Oliguria (less than 0.5mL/kg/hr despite fluids)
Key Numbers
- CK greater than 5,000 U/L = high risk AKI
- CK greater than 15,000-20,000 U/L = almost certain dialysis
- Entrapment greater than 4-6 hours = high risk crush syndrome
- 20% overall mortality; 50% of AKI need dialysis
Evidence Base
Management of Crush-Related Injuries After Disasters (Landmark Review)
- Definitive review of disaster-related crush injury drawing on the Renal Disaster Relief Task Force experience
- Establishes pre-extrication and early intravenous fluid loading as the central preventive intervention against crush-induced AKI
- Frames hyperkalaemia, hypovolaemia and myoglobinuric AKI as the principal early killers
- Calls for early mobilisation of dialysis and intensive-care resources in mass-casualty settings
Marmara Earthquake - Largest Crush Syndrome Renal Series
- 639 patients with crush-related acute renal failure across 35 hospitals after the 1999 Marmara earthquake
- 477 patients (74.6%) received one or more dialysis treatments
- Overall mortality 15.2% (17.2% in dialysed vs 9.3% in non-dialysed patients)
- Death was driven by sepsis, thrombocytopenia, DIC, ARDS and thoraco-abdominal trauma rather than renal failure alone