Nutcracker Mechanism | Compression Injury | ORIF Required
- Cuboid fractures = nutcracker mechanism - compression between calcaneus and 4th/5th metatarsals during forced plantarflexion and abduction
- Often associated with Lisfranc injuries - Cuboid fracture suggests midfoot instability, check for Lisfranc injury
- ORIF required if displaced - Prevents lateral column shortening and midfoot collapse
- Lateral column key - Cuboid is keystone of lateral column, loss of length causes lateral foot pain and midfoot instability
- Bone graft often needed - Compression mechanism causes impaction, bone loss requires grafting
- “Nutcracker mechanism = compression between calcaneus and metatarsals
- “Often associated with Lisfranc injuries
- “ORIF required if displaced - prevents lateral column shortening
- “Bone graft often needed for impaction
Cuboid fractures = nutcracker mechanism - Compression between calcaneus and 4th/5th metatarsals during forced plantarflexion and abduction. Causes impaction and bone loss. Often associated with Lisfranc injuries.
Cuboid fracture suggests midfoot instability - Often associated with Lisfranc injuries. Check for Lisfranc injury if cuboid fracture present. Midfoot instability requires ORIF of both injuries.
Cuboid is keystone of lateral column - Loss of length causes lateral column shortening and midfoot collapse. ORIF required if displaced to restore lateral column length and prevent midfoot instability.
Compression mechanism causes impaction - Bone loss requires bone graft to restore lateral column length. Autograft from calcaneus or iliac crest. Allograft acceptable. Prevents lateral column shortening.
- Pattern
- CCJ capsular avulsion
- Treatment
- Conservative
- Key Point
- Most common; benign
- Pattern
- Extra-articular body
- Treatment
- Conservative if undisplaced
- Key Point
- Watch lateral column length
- Pattern
- Intra-articular body
- Treatment
- ORIF if step-off or displaced
- Key Point
- Restore articular congruity
- Pattern
- With TMT (Lisfranc) injury
- Treatment
- ORIF midfoot + cuboid
- Key Point
- Always check Lisfranc
- Pattern
- Nutcracker / midtarsal crush
- Treatment
- ORIF +/- graft, bridge plate/ex-fix
- Key Point
- Restore lateral column length
CHECKLisfranc Association
Hook:CHECK: Cuboid fracture, High association with Lisfranc, Examine for Lisfranc, CT to assess, Key to check!
Overview and Epidemiology
Cuboid fractures are rare but important injuries involving the cuboid bone, which serves as the keystone of the lateral column. These fractures result from a nutcracker mechanism and are often associated with Lisfranc injuries.
Definition
Cuboid fracture: Fracture of the cuboid bone, which:
- Location: Lateral midfoot
- Function: Keystone of lateral column
- Mechanism: Nutcracker (compression)
- Association: Often with Lisfranc injuries
Nutcracker mechanism:
- Compression: Between calcaneus and 4th/5th metatarsals
- Forced plantarflexion and abduction: Classic mechanism
- Impaction: Causes bone loss and shortening
- Lisfranc: Often associated with midfoot instability
Epidemiology
- Incidence: Less than 1% of foot fractures
- Age: Peak 20-40 years (trauma population)
- Gender: No clear predominance
- Mechanism: High-energy trauma, forced plantarflexion and abduction
- Associated injuries: Lisfranc injuries, other midfoot trauma
Cuboid fractures = nutcracker mechanism - Compression between calcaneus and 4th/5th metatarsals during forced plantarflexion and abduction. Causes impaction and bone loss. Often associated with Lisfranc injuries - check for midfoot instability.
Anatomy and Pathophysiology
Cuboid Anatomy
Cuboid bone:
- Location: Lateral midfoot
- Function: Keystone of lateral column
- Articulations: Calcaneus (proximal), 4th/5th metatarsals (distal), navicular (medial), lateral cuneiform (medial)
- Blood supply: Branches from dorsalis pedis and lateral plantar arteries
Lateral column:
- Components: Calcaneus, cuboid, 4th/5th metatarsals
- Function: Lateral foot stability and weight bearing
- Cuboid role: Keystone, maintains lateral column length
Nutcracker mechanism:
- Compression: Between calcaneus and 4th/5th metatarsals
- Forced plantarflexion and abduction: Classic mechanism
- Impaction: Causes bone loss and shortening
Pathophysiology
Injury mechanism:
- Forced plantarflexion and abduction: Classic mechanism
- Compression: Cuboid compressed between calcaneus and metatarsals
- Impaction: Causes bone loss and lateral column shortening
- Lisfranc association: Often associated with midfoot instability
Why displacement matters:
- Lateral column shortening: Displacement causes loss of length
- Midfoot collapse: Shortening causes midfoot instability
- Arthritis risk: Malunion leads to lateral column arthritis
Why ORIF required:
- Restore length: Anatomic reduction restores lateral column length
- Prevent collapse: Prevents midfoot collapse
- Bone graft: Often needed for impaction defects
Classification Systems
Fenton Classification (Bone Joint J 2016, n=192)
The Fenton classification is the most widely cited descriptive system, derived from 192 fractures in 188 patients and based on mechanism of injury:
Type 1 (48.4%) — Avulsion:
- Capsular avulsion of the calcaneocuboid joint
- Most common; usually benign
- Treatment: conservative
Type 2 (13%) — Extra-articular body:
- Isolated extra-articular body fracture
- Treatment: conservative if undisplaced; watch lateral column length
Type 3 (6.8%) — Intra-articular body:
- Intra-articular fracture confined to the cuboid body
- Treatment: ORIF if articular step-off or displacement
Type 4 (18.2%) — Midfoot / tarsometatarsal:
- Associated with midfoot and tarsometatarsal (Lisfranc) disruption
- Treatment: ORIF of the midfoot complex and cuboid
Type 5 (13.5%) — Nutcracker / midtarsal crush:
- Mid-tarsal (Chopart) disruption with crushing of the lateral column (5a) or both columns (5b); the classic "nutcracker"
- Treatment: ORIF +/- bone graft, bridging plate or external fixation to restore length
The original Fenton paper recommended fixation for fractures with significant articular disruption or loss of lateral column length.
Clinical Assessment
History
Symptoms:
- Lateral foot pain: Pain on lateral side of foot
- Swelling: Localised to lateral midfoot
- Difficulty weight bearing: Pain with weight bearing
- Mechanism: Forced plantarflexion and abduction
Risk factors:
- High-energy trauma
- Lisfranc injury mechanism
- Midfoot instability
Physical Examination
Inspection:
- Swelling on lateral midfoot
- Ecchymosis (may be delayed)
- Deformity (lateral column shortening if displaced)
Palpation:
- Tenderness over cuboid
- Lisfranc joint tenderness (if associated)
- Lateral column instability
Range of Motion:
- Midfoot ROM limited and painful
- Inversion/eversion painful
- Plantarflexion/dorsiflexion painful
Special tests:
- Lisfranc stress test: Check for midfoot instability
- Lateral column stress: Pain with stress
- Midfoot alignment: Check for collapse
Check for Lisfranc injury - Cuboid fractures are often associated with Lisfranc injuries. Perform Lisfranc stress test and check for midfoot instability. CT is often needed to assess both injuries.
Differential Diagnosis of Lateral Midfoot Pain
- Typical Mechanism
- Forced abduction / axial crush
- Key Clinical/Imaging Feature
- Cuboid tenderness; lateral column shortening on CT
- Discriminator
- Direct cuboid tenderness + CT fracture
- Typical Mechanism
- Axial load on plantarflexed foot
- Key Clinical/Imaging Feature
- Plantar ecchymosis; TMT diastasis on weight-bearing/CT
- Discriminator
- Instability at tarsometatarsal joints
- Typical Mechanism
- Inversion + plantarflexion
- Key Clinical/Imaging Feature
- Tenderness anterior process, dorsolateral foot
- Discriminator
- Fracture seen on oblique X-ray/CT of calcaneus
- Typical Mechanism
- Inversion injury
- Key Clinical/Imaging Feature
- Tenderness at MT base; peroneus brevis avulsion
- Discriminator
- Fracture at metatarsal base, not cuboid
- Typical Mechanism
- Inversion / eversion strain
- Key Clinical/Imaging Feature
- Retromalleolar/lateral pain, subluxation
- Discriminator
- Tenderness along tendon, no bony injury
- Typical Mechanism
- Inversion
- Key Clinical/Imaging Feature
- ATFL tenderness, normal bony exam
- Discriminator
- No midfoot bony tenderness; normal CT
Investigations
Standard X-ray Protocol
AP view:
- May show cuboid fracture
- Check for Lisfranc injury
Lateral view:
- May show fracture
- Assess lateral column alignment
Oblique view:
- May show fracture better
- Lisfranc joint view
Key point: CT is often needed for diagnosis and planning.

Management Algorithm

Management Pathway
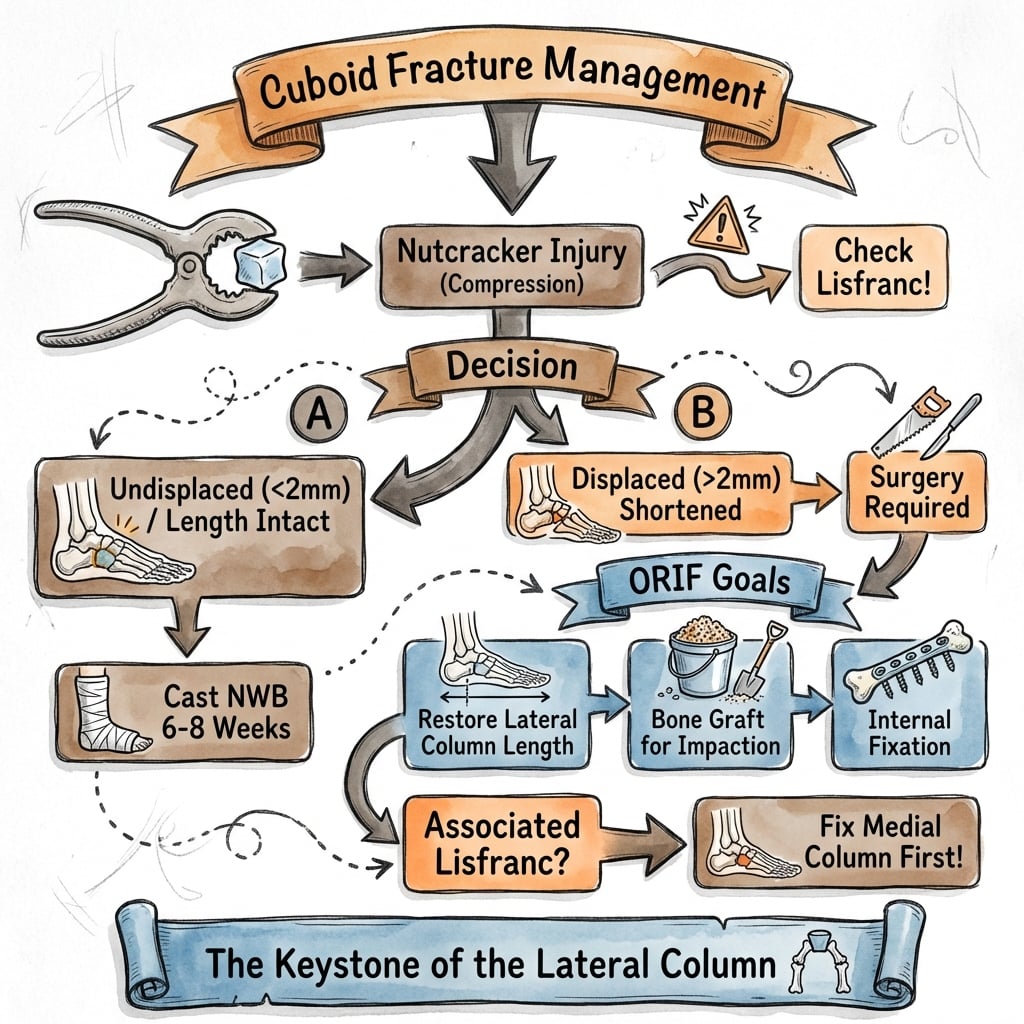
Cuboid Fracture Management
CT is usually required for diagnosis - cuboid fractures are difficult to see on X-ray alone. Assess displacement, impaction, and associated Lisfranc injury. Check for lateral column shortening.
If non-displaced (less than 2mm step-off) and isolated, conservative treatment with cast and non-weight bearing for 6-8 weeks. Success rate 85-90%.
If displaced (greater than 2mm) or part of Lisfranc injury, ORIF required. Restore lateral column length. Bone graft if impaction. Success rate 80-85%.
If part of Lisfranc injury, address both injuries. Cuboid ORIF as part of Lisfranc fixation. Restore lateral column length and midfoot stability. Success rate 75-85%.
ORIFTreatment Decision
Hook:ORIF: ORIF Required if displaced, Restore lateral column length, Impaction requires bone graft, Fixation with screws or plate!
Surgical Technique
ORIF Technique
Indications:
- Displaced cuboid fractures
- Part of Lisfranc injury
- Lateral column shortening
Approach:
- Lateral approach to cuboid
- Expose cuboid
- Protect peroneal tendons
Technique:
- Exposure: Lateral approach to cuboid, expose fracture, protect peroneal tendons
- Debridement: Remove impacted bone fragments, assess bone loss
- Bone graft: Fill impaction defect with bone graft (autograft from calcaneus or iliac crest, allograft acceptable)
- Reduction: Restore lateral column length, reduce fracture anatomically
- Fixation: Screws (2.7-3.5mm) or mini-fragment plate (2.0-2.7mm)
- Verification: Confirm reduction and hardware position fluoroscopically, verify lateral column length restored
Advantages:
- Restores lateral column length
- Prevents midfoot collapse
- Allows early motion
ORIF restores lateral column length.
Complications
- Incidence
- 10-15%
- Risk Factors
- Impaction, inadequate reduction
- Prevention/Management
- Bone graft, restore length
- Incidence
- 10-15%
- Risk Factors
- Lateral column shortening
- Prevention/Management
- Restore length, adequate fixation
- Incidence
- Underreported
- Risk Factors
- Normal-looking plain films, focus on cuboid only
- Prevention/Management
- Routine CT; examine whole midfoot
- Incidence
- 5-10%
- Risk Factors
- Displacement, inadequate fixation
- Prevention/Management
- Rigid fixation, bone graft
Lateral Column Shortening
10-15% incidence (if untreated):
- Cause: Impaction, inadequate reduction, bone loss
- Prevention: Bone graft, restore length, adequate fixation
- Management: Revision ORIF with bone graft if symptomatic
Midfoot Collapse
10-15% incidence (if untreated):
- Cause: Lateral column shortening, inadequate fixation
- Prevention: Restore length, adequate fixation
- Management: Revision ORIF or midfoot fusion if severe
Peroneus Longus and the Peroneal Groove of the Cuboid
The surgical technique repeatedly instructs the surgeon to "protect the peroneal tendons," but the topic never explains why the peroneus longus is uniquely at risk in cuboid injuries — an anatomical relationship examiners like to probe.
The peroneal sulcus
- The cuboid carries a distinct oblique groove — the peroneal sulcus (groove) — on its plantar-lateral surface, running infero-medially from the lateral margin toward the plantar tuberosity.
- The peroneus longus (fibularis longus) tendon turns around the lateral cuboid and enters this sulcus to cross the sole obliquely and insert on the plantar base of the first metatarsal and medial cuneiform, where it is a key stabiliser of the medial (first-ray) column and the transverse arch.
- The long plantar ligament roofs the sulcus, converting it into a fibro-osseous tunnel; the peroneus brevis lies more superficially and inserts on the fifth metatarsal base.
Os peroneum and clinical relevance
- An os peroneum — a sesamoid within the peroneus longus tendon — lies at the level of the calcaneocuboid joint in a variable minority of feet and may be bipartite; on radiographs it must not be mistaken for an avulsion fracture, and conversely a genuine os peroneum fracture (painful os peroneum syndrome) is a differential for lateral midfoot pain.
- Because the tendon is intimate with the plantar-lateral cuboid, plantar/lateral cuboid avulsion and crush fractures can lacerate, entrap or dislocate the peroneus longus, or fracture the os peroneum — an overlooked cause of persistent lateral-column pain and weak eversion after apparent bony union.
- During the lateral (Ollier-type or longitudinal) approach for cuboid ORIF, the peroneus longus and brevis tendons and the sural nerve overlie the operative field and must be identified and retracted; hardware placed on the plantar-lateral surface can irritate the tendon.
The peroneus longus rides in a groove on the plantar-lateral cuboid on its way to the first-ray base, so cuboid fractures can injure the tendon or fracture an os peroneum (do not confuse a normal-variant os peroneum with an avulsion). At lateral ORIF, protect the peroneus longus/brevis and the sural nerve, and beware plantar-lateral hardware causing tendon irritation.
NUTCRACKERCuboid Fracture Features
Hook:NUTCRACKER: Nutcracker mechanism, Usually associated with Lisfranc, Tarsal bone, Compression injury, Restore lateral column, Abduction mechanism, Calcaneus compression, Keystone of lateral column, Examine for Lisfranc, Restore with ORIF!
Foot Compartment Syndrome in Crush (Nutcracker) Patterns
The viva traps warn about "missing foot compartment syndrome in high-energy crush patterns" and the Metcalfe systematic review recommends "formal assessment for compartment syndrome," yet the topic never develops this limb-threatening companion of the crush cuboid.
Why it happens
- High-energy nutcracker/Chopart crush patterns (Fenton Type 5, and Type 4 with Lisfranc disruption) transmit large compressive and shearing loads across the midfoot, producing marked oedema and bleeding within the osseofascial compartments of the foot (classically described as nine to ten, including the deep calcaneal compartment that communicates with the deep posterior compartment of the leg).
- The risk is greatest with delayed presentation, associated Lisfranc/tarsometatarsal disruption, and polytrauma.
Diagnosis and management
- Clinical: pain out of proportion, a tensely swollen foot, and pain on passive extension of the toes are the key signs; pulses and capillary refill are unreliable and are typically preserved.
- Measurement: compartment pressures support the diagnosis when the difference between diastolic blood pressure and compartment pressure (delta-p) falls to fewer than 30 mmHg (equivalently, absolute pressure within roughly 30 mmHg of diastolic).
- Treatment: emergent foot fasciotomy — commonly two dorsal (second and fourth intermetatarsal) incisions, with a medial incision added to release the calcaneal and deep compartments if pressures remain elevated.
- Consequence of a missed diagnosis: ischaemic contracture with claw-toe deformity, intrinsic muscle fibrosis, chronic pain and sensory loss — a far worse outcome than the fracture itself.
A crush/nutcracker cuboid rarely occurs alone — screen every high-energy midfoot injury for foot compartment syndrome. Diagnosis is clinical (disproportionate pain, tense swelling, pain on passive toe extension) supported by a delta-p of fewer than 30 mmHg; treat with emergent fasciotomy. A missed compartment syndrome causes claw-toe contracture and outweighs any benefit from a perfect cuboid reduction.
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Midfoot ROM and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- CT to confirm healing
- Cast removal if healing
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
ORIF (isolated):
- Success rate: 80-85% (union, pain relief)
- Functional outcomes: 75-80% return to pre-injury level
- Lateral column: 80-85% maintain length
ORIF (part of Lisfranc):
- Success rate: 75-85% (union, pain relief)
- Functional outcomes: 70-75% return to pre-injury level
- Lateral column: 75-80% maintain length
Conservative (non-displaced):
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- Lateral column: 85-90% maintain length
Long-Term Prognosis
Lateral column shortening progression:
- With proper treatment: 10-15% develop shortening
- Without treatment: 20-30% develop shortening
- Risk factors: Impaction, displacement, delayed treatment
Guidelines, Registries & Global Practice
Global Epidemiology
- Cuboid fractures account for under 1% of all foot fractures; isolated cuboid fractures are rarer still, as most occur within a midtarsal (Chopart) or tarsometatarsal injury.
- In the largest series (Fenton 2016, n=192), capsular avulsion (Type 1) made up nearly half of all cuboid fractures, while true crush "nutcracker" patterns were a minority (~14%).
- Paediatric distribution differs - extra-articular body fractures predominate and grafting is rarely required (Ruffing 2018).
Guideline and Society Positions (side by side)
- Emphasis
- Lateral column integrity
- Practical Recommendation
- Restore and maintain lateral column length; bridge/span comminution if needed
- Emphasis
- Soft-tissue first, CT for midfoot
- Practical Recommendation
- Low threshold for CT in suspected midfoot injury; senior decision-making for operative cases
- Emphasis
- Articular congruity and function
- Practical Recommendation
- Fix displaced intra-articular fractures; AOFAS Midfoot score used for outcome reporting
- Emphasis
- Treat within Chopart spectrum
- Practical Recommendation
- Early anatomical reduction, exclude compartment syndrome, ORIF for displaced patterns
Note: there is no dedicated high-level guideline specific to cuboid fractures. Practice is extrapolated from midfoot/Chopart injury principles. No national joint registry captures cuboid fracture fixation (registries track arthroplasty, not midfoot trauma).
High- vs Limited-Resource Practice
- Routine CT for suspected midfoot injury and pre-operative planning
- Locking plates, mini-fragment systems and bone substitutes readily available
- Early ORIF for displaced/crush patterns
- Reliance on plain radiographs (oblique views) and clinical examination; risk of missed injuries
- Greater use of K-wires, external fixation and autograft (e.g. local calcaneal/iliac crest) where implants are scarce
- Threshold for transfer/referral when crush patterns or compartment syndrome are suspected
Cuboid fractures are a common viva topic. Anchor your answer to the Fenton classification (avulsion most common; nutcracker/Type 5 is the crush pattern), the nutcracker mechanism (forced abduction compressing the cuboid between calcaneus and 4th/5th metatarsals), the imperative to restore lateral column length and exclude an associated Lisfranc/midtarsal injury, and the role of CT in diagnosis and planning.
Controversies and Areas of Uncertainty
The evidence base is limited to small retrospective series and case reports, so several questions remain genuinely unresolved:
No agreed numeric threshold exists. Reported indications range from articular displacement over 1 mm (Yu, Acta Orthop Belg 2012) to any loss of lateral column length (Fenton 2016). The pragmatic consensus is that lateral column shortening or intra-articular incongruity - not an arbitrary millimetre cut-off - drives the decision to operate.
Screws, mini-fragment plates, locking plates, bridging plates and external fixation have all been described. Comminuted crush patterns may need a bridging/spanning construct to hold length; simpler patterns suit direct fixation. No comparative data favour one construct.
Impaction voids have been filled with autograft, allograft and synthetic substitutes. Children frequently need no graft (Ruffing 2018). There is no evidence that one void filler is superior.
Arthroscopic-assisted elevation with percutaneous void filling has been reported successfully (Ohmori 2016), but remains anecdotal. Its role versus open reduction is undefined.
MCQ Practice Points
Q: What is the nutcracker mechanism for cuboid fractures? A: Compression between calcaneus and 4th/5th metatarsals - During forced plantarflexion and abduction. Causes impaction and bone loss. Often associated with Lisfranc injuries.
Q: Why are cuboid fractures often associated with Lisfranc injuries? A: Cuboid fracture suggests midfoot instability - in the Fenton series roughly one in five cuboid fractures (Type 4, ~18%) involved a tarsometatarsal (Lisfranc) injury, and Type 5 added midtarsal disruption. Always check for an associated Lisfranc/midtarsal injury; both require ORIF.
Q: Why is the cuboid important for lateral column stability? A: Cuboid is keystone of lateral column - Loss of length causes lateral column shortening and midfoot collapse. ORIF required if displaced to restore length. Bone graft often needed for impaction.
Q: When is ORIF required for cuboid fractures? A: Displacement greater than 2mm or part of Lisfranc injury - Prevents lateral column shortening and midfoot collapse. Bone graft needed for impaction. Success rate 80-85%.
Q: Why is bone graft often needed for cuboid fractures? A: Compression mechanism causes impaction and bone loss - Bone graft required to restore lateral column length. Autograft from calcaneus or iliac crest. Prevents lateral column shortening.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old patient presents with lateral foot pain after forced plantarflexion and abduction injury. CT shows displaced cuboid fracture with 3mm displacement and impaction. No associated Lisfranc injury.”
“A 35-year-old patient has a cuboid fracture as part of a Lisfranc injury. The examiner asks you to explain how you manage both injuries.”
“A 28-year-old is reviewed in fracture clinic two weeks after an inversion ankle injury. Foot radiographs were reported as normal in the emergency department, but he has persistent, well-localised lateral midfoot pain and tenderness over the cuboid. How do you proceed?”
Key Concepts
- Nutcracker mechanism = compression between calcaneus and 4th/5th metatarsals
- Associated tarsometatarsal/midtarsal injury in a substantial minority (Fenton Type 4 ~18%, Type 5 ~14%)
- Cuboid is keystone of lateral column
- ORIF required if displaced (restores lateral column length)
Classification
- Fenton Type 1 (~48%): CCJ capsular avulsion - conservative
- Fenton Type 2 (~13%): extra-articular body - conservative if undisplaced
- Fenton Type 3 (~7%): intra-articular body - ORIF if displaced
- Fenton Type 4 (~18%): with tarsometatarsal (Lisfranc) injury - ORIF midfoot + cuboid
- Fenton Type 5 (~14%): nutcracker / midtarsal crush - ORIF +/- graft, restore length
Treatment
- Non-displaced, isolated: Conservative (cast, NWB 6-8 weeks)
- Displaced, isolated: ORIF with bone graft if impaction (80-85% good results)
- Part of Lisfranc: ORIF as part of Lisfranc fixation (75-85% good results)
- Displacement greater than 2mm: ORIF required
Surgical Technique
- Lateral approach: Protect peroneal tendons
- Debride impacted bone, assess bone loss
- Bone graft: Fill impaction defect (autograft from calcaneus or iliac crest)
- Fixation: Screws (2.7-3.5mm) or mini-fragment plate (2.0-2.7mm)
- Restore lateral column length
- Verify reduction fluoroscopically
Complications
- Lateral column shortening: 10-15% if untreated (prevent with bone graft, restore length)
- Midfoot collapse: 10-15% if untreated (prevent with adequate fixation)
- Missed associated injury: Lisfranc/midtarsal/navicular often overlooked (prevent with routine CT)
- Nonunion: 5-10% (prevent with rigid fixation, bone graft)
Evidence Base
The literature on cuboid fractures is dominated by small retrospective series and case reports - there are no randomised trials. The strongest single dataset is the Fenton classification series of 192 fractures. Treatment principles (restore lateral column length, fix displaced intra-articular fractures, always exclude associated Lisfranc/midtarsal injury) are consistent across all reports.
Fenton Classification of Cuboid Fractures (landmark series)
- Largest cuboid fracture series (n=192) - basis of the standard classification
- Avulsion (Type 1) is by far the most common pattern (~48%)
- Only a minority are true crush/nutcracker (Type 5, ~14%)
- Indications for fixation: articular disruption or lateral column shortening
Nutcracker Fracture: ORIF + Graft Restores Lateral Column
- All nutcracker fractures had lateral column shortening
- Surgical threshold proposed: articular displacement over 1 mm or any column shortening
- Allograft used to fill impaction defects
- Outcomes good-to-fair - reflects difficulty of these injuries