Polytrauma | Temporary Stabilization | Second Hit Prevention
- DCO = temporary external fixation, delay definitive surgery until physiology normalizes
- Second hit phenomenon - surgery adds insult to already inflamed patient
- Borderline patients benefit most from DCO approach
- Start definitive surgery day 5-10 when inflammation subsides
- Lactate, pH, base deficit are key monitoring parameters
- “DCO prevents the 'second hit' of major surgery to inflammatory system
- “External fixation of femur reduces pulmonary complications in polytrauma
- “ISS greater than 20 + chest/head injury = consider DCO
- “Only borderline patients need decision-making - stable gets ETC, unstable gets DCO
Polytrauma patients with physiological derangement from multiple injuries. Key is recognizing the borderline patient who may decompensate with definitive surgery. ISS greater than 20, bilateral femur fractures, or chest/head injury are triggers.
Major surgery is an inflammatory insult. In polytrauma, the patient is already in systemic inflammatory response. Adding surgery creates a second hit that can precipitate ARDS, MOF, and death. DCO delays this until inflammation subsides.
Monitor lactate, pH, base deficit to assess resuscitation status. Do NOT proceed to definitive surgery until: pH greater than 7.25, lactate less than 4, base deficit less than 6, temperature greater than 35C, platelets greater than 50.
Day 1-4: Window of opportunity (if patient very stable) or Day 5-10: Safe window after inflammatory response subsides. Avoid days 2-4 in borderline patients (peak inflammation).
- Physiology
- Normal lactate, pH, hemodynamics
- Fracture Management
- Early Total Care (ETC) - definitive fixation
- Key Pearl
- This is the majority of trauma patients
- Physiology
- Moderate derangement, responding to resuscitation
- Fracture Management
- DCO - external fixation, reassess daily
- Key Pearl
- This group benefits most from DCO
- Physiology
- Ongoing hemorrhage, acidosis despite resuscitation
- Fracture Management
- DCO mandatory - minimal intervention
- Key Pearl
- Definitive surgery would be fatal
- Physiology
- Moribund, cardiac arrest, perimortem
- Fracture Management
- Hemorrhage control only, no fracture fixation
- Key Pearl
- Focus on survival, not fractures
SAFEPhysiological Thresholds for Surgery
Hook:Is the patient SAFE for definitive surgery? Check these parameters!
STOPSecond Hit Prevention
Hook:STOP the second hit - stabilize temporarily and optimize before definitive surgery!
Overview and Epidemiology
Definition
Damage Control Orthopaedics (DCO) is a staged approach to managing fractures in polytrauma patients. The concept involves temporary stabilization (usually external fixation) followed by delayed definitive surgery once the patient's physiology has normalized.
Historical Context
Evolution from ETC to DCO:
- 1980s-1990s: Early Total Care (ETC) paradigm - early definitive fixation of all fractures
- Femoral nailing within 24 hours became standard
- Recognition that some patients deteriorated after early surgery
- Second hit phenomenon described - surgery adds inflammatory insult
- DCO concept developed for high-risk polytrauma patients
Rationale
The Second Hit Phenomenon:
- Major trauma causes systemic inflammatory response (SIRS)
- Additional surgical insult amplifies the inflammatory cascade
- Can precipitate ARDS, MOF, and death
- DCO minimizes surgical trauma until inflammation subsides
DCO is only for unstable or borderline patients. The majority of trauma patients (stable physiology) should receive Early Total Care (ETC) with definitive fixation. DCO in stable patients delays mobilization and increases infection risk.
Major trauma is a leading global cause of death in those under 45, with variable access to definitive care worldwide. DCO allows district and regional hospitals to stabilize fractures for safe transfer to tertiary trauma centres - a principle as relevant to remote high-income regions as to limited-resource settings. External fixation is a core skill for every orthopaedic surgeon.
Pathophysiology
The Inflammatory Response to Trauma
- Tissue damage releases damage-associated molecular patterns (DAMPs)
- Activation of innate immune system
- Cytokine release: IL-1, IL-6, TNF-alpha
- Systemic inflammatory response syndrome (SIRS)
- Compensatory anti-inflammatory response (CARS)
- Additional tissue damage from surgery
- Further cytokine release
- Tips the balance toward hyperinflammation
- End-organ damage: lungs (ARDS), kidneys, liver
- Multi-organ failure (MOF)
Patient Classification
- Definition
- Isolated injuries, responding to resuscitation
- Physiology
- Normal lactate, pH, hemodynamics
- Management
- ETC - definitive surgery
- Definition
- Multiple injuries, moderate derangement
- Physiology
- Lactate 2-4, mild acidosis, soft tissue injury
- Management
- DCO vs ETC - individualized decision
- Definition
- Ongoing hemorrhage, not responding
- Physiology
- Lactate greater than 4, pH less than 7.25, coagulopathy
- Management
- DCO mandatory
- Definition
- Moribund, cardiac arrest, perimortem
- Physiology
- Unresponsive to resuscitation
- Management
- Hemorrhage control only
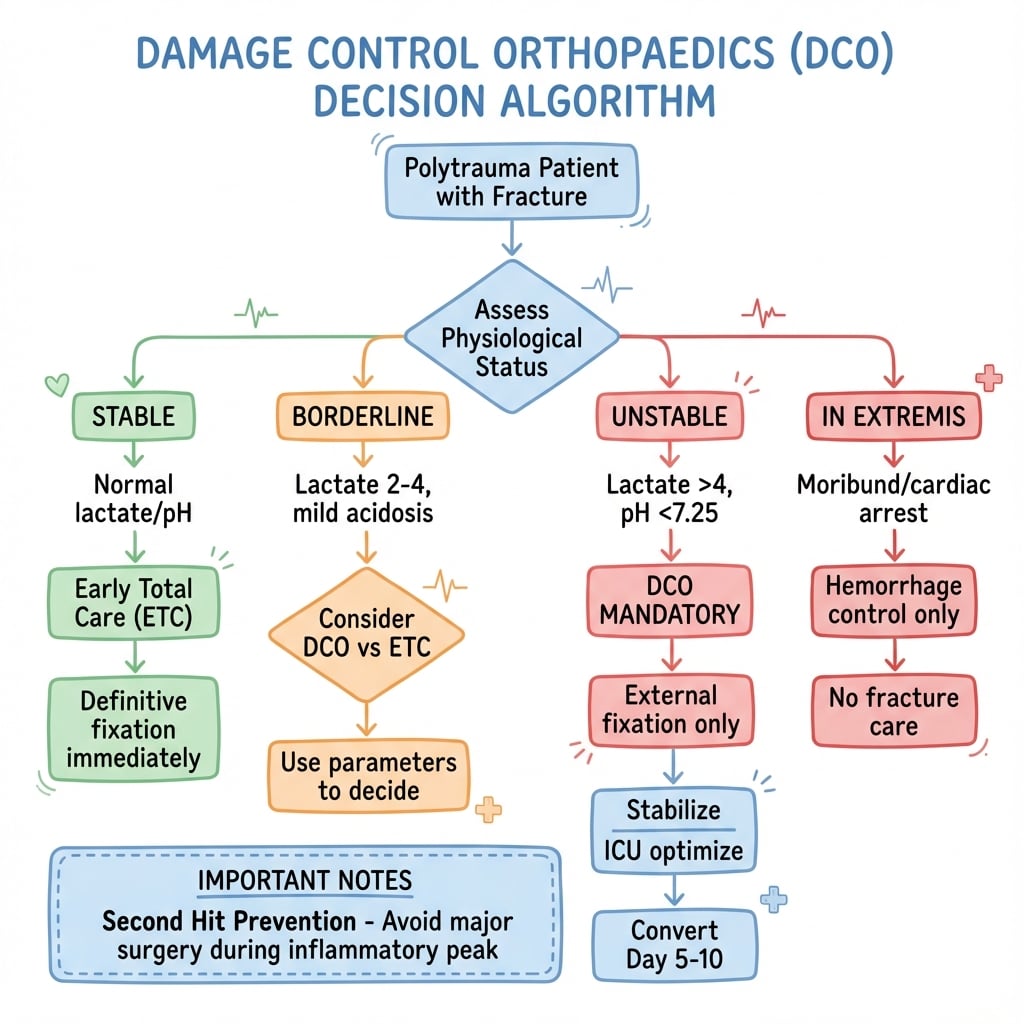
Stable patients get ETC. Unstable patients get DCO. The decision-making challenge is the BORDERLINE patient. Use physiological parameters, injury pattern (ISS, chest injury), and clinical trajectory to decide. When in doubt, choose DCO.
Damage Control Resuscitation and the Lethal Triad
Damage control orthopaedics cannot be separated from damage control resuscitation (DCR) — the two run in parallel. DCO controls the skeletal "second hit"; DCR reverses the physiology that makes the patient unsafe to operate on.
The Lethal Triad (Trauma Triad of Death)
The scattered thresholds above are unified by the lethal triad: hypothermia, acidosis, and coagulopathy. Each worsens the others in a self-perpetuating vicious cycle — hypothermia and acidosis impair the clotting cascade and platelet function, bleeding worsens acidosis, and transfusion/exposure worsen hypothermia. Breaking this cycle is the whole point of "damage control": do the minimum to stop bleeding and stabilise, then correct physiology before any definitive reconstruction.
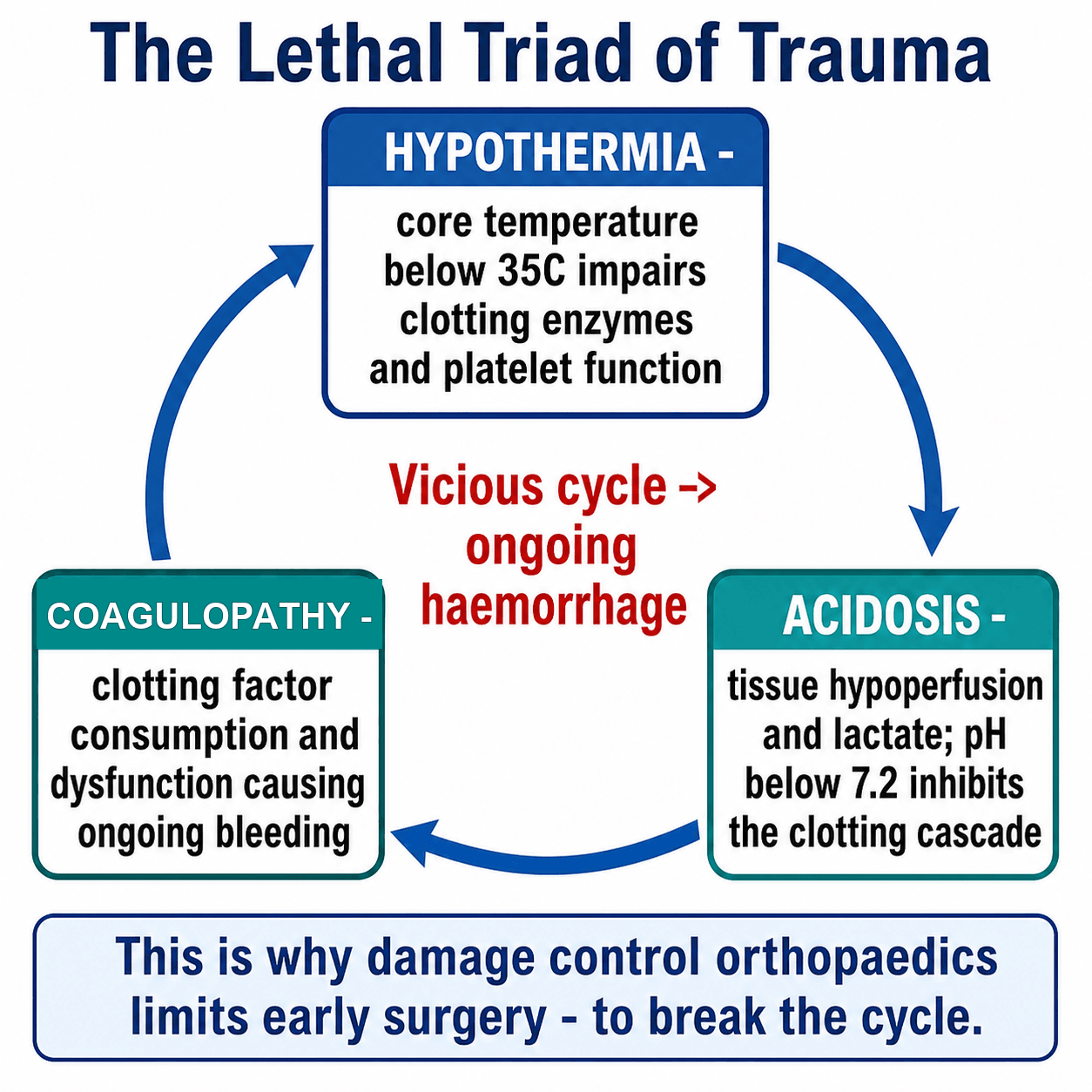
Coagulopathy in major trauma is not just dilutional — an acute traumatic coagulopathy driven by tissue hypoperfusion and inflammation is present on arrival in severely injured patients, then amplified by hypothermia, acidosis and crystalloid dilution. This is why early haemostatic resuscitation, not late correction, is key.
Principles of Damage Control Resuscitation
- Permissive (hypotensive) resuscitation: tolerate a lower blood pressure (e.g. a palpable radial pulse / SBP ~80-90 mmHg) until surgical haemorrhage control is achieved, to avoid "popping the clot" and dilutional coagulopathy. Exception: traumatic brain injury, where cerebral perfusion must be maintained (avoid hypotension).
- Haemostatic (balanced) resuscitation: give blood products early in balanced ratios approximating whole blood (around 1:1:1 red cells : plasma : platelets) via a massive transfusion protocol, and minimise crystalloid (which dilutes clotting factors and worsens the triad).
- Tranexamic acid: give early — CRASH-2 showed TXA given within 3 hours of injury reduces death due to bleeding in trauma haemorrhage (and is harmful if given late).
- Goal-directed correction: rewarm aggressively, correct ionised calcium, and guide product use with point-of-care viscoelastic testing (ROTEM/TEG) where available.
- Resuscitation endpoints: clearance of lactate and base deficit (not blood pressure alone) signal adequate resuscitation and readiness to escalate fracture care.
DAMAGEDamage Control Orthopaedics Indications
Hook:If DAMAGE is present, do DCO to prevent the second hit!
Classification
Parameters to Guide Decision-Making
Pro-DCO Indicators (favor temporary fixation):
- Threshold
- Less than 7.25
- Reasoning
- Significant acidosis indicates poor perfusion
- Threshold
- Greater than 4 mmol/L
- Reasoning
- Marker of tissue hypoxia
- Threshold
- Greater than 6
- Reasoning
- Reflects degree of metabolic derangement
- Threshold
- Less than 35°C
- Reasoning
- Hypothermia impairs coagulation
- Threshold
- Less than 50
- Reasoning
- Coagulopathy, ongoing hemorrhage
- Threshold
- Greater than 10 units in 24h
- Reasoning
- Massive transfusion = unstable
- Threshold
- Greater than 1.5
- Reasoning
- Coagulopathy
Note: These are guidelines, not absolute cutoffs. Clinical judgment remains essential.

Clinical Assessment
- ATLS principles first and foremost
- Control hemorrhage - pelvic binder, tourniquet
- Resuscitation with blood products
- Identify all injuries - tertiary survey essential
- Classify patient - stable, borderline, unstable, in extremis
- Trend physiological parameters - improving or deteriorating?
- Response to resuscitation - key decision point
- Serial lactate - most useful single parameter
- Reassess regularly - status can change rapidly
- Team communication - trauma team, anesthesia, ICU
Key Clinical Findings
- Persistent tachycardia despite fluid
- Ongoing blood product requirements
- Rising or static lactate
- Worsening acidosis
- Cold peripheries, delayed capillary refill
- Normalizing heart rate
- Decreasing blood product requirement
- Falling lactate
- Improving acidosis
- Warm peripheries, urine output greater than 0.5ml/kg/hr
Young patients compensate well. Blood pressure may be normal despite significant blood loss. Use lactate, base deficit, and clinical signs to assess perfusion. Hypotension is a LATE sign of decompensation.
Investigations
- Pro-ETC
- Greater than 7.35
- Borderline
- 7.25-7.35
- Pro-DCO
- Less than 7.25
- Pro-ETC
- Less than 2
- Borderline
- 2-4
- Pro-DCO
- Greater than 4
- Pro-ETC
- Less than 4
- Borderline
- 4-6
- Pro-DCO
- Greater than 6
- Pro-ETC
- Greater than 36°C
- Borderline
- 35-36°C
- Pro-DCO
- Less than 35°C
- Pro-ETC
- Greater than 100
- Borderline
- 50-100
- Pro-DCO
- Less than 50
Serial lactate is the single most useful parameter. A falling lactate indicates adequate resuscitation. A rising lactate despite resuscitation indicates ongoing hemorrhage or inadequate perfusion - this patient needs DCO, not definitive surgery.
Decision Differential: ETC vs DCO vs EAC
The viva trap is treating DCO and ETC as a binary. They sit on a spectrum, with Early Appropriate Care (EAC) as the modern, resuscitation-led bridge. Distinguish them clearly.
- Early Total Care (ETC)
- Definitive fixation of all fractures early
- Early Appropriate Care (EAC)
- Resuscitate to targets, then fix definitively early
- Damage Control (DCO)
- Temporary stabilization, delay definitive surgery
- Early Total Care (ETC)
- Stable physiology
- Early Appropriate Care (EAC)
- Achieves lactate less than 4, pH at least 7.25, BE at least -5.5
- Damage Control (DCO)
- Persistent derangement / high-risk pattern
- Early Total Care (ETC)
- Definitive (nail/ORIF)
- Early Appropriate Care (EAC)
- Definitive once resuscitated (often within 36h)
- Damage Control (DCO)
- External fixation / splint
- Early Total Care (ETC)
- Bone 1989 (RCT)
- Early Appropriate Care (EAC)
- Vallier 2013/2015
- Damage Control (DCO)
- Pape 1993, EPOFF 2003
- Early Total Care (ETC)
- Second hit in the unstable patient
- Early Appropriate Care (EAC)
- Delay if resuscitation targets ignored
- Damage Control (DCO)
- Prolonged ex-fix, pin infection, delayed union
Controversies and Areas of Uncertainty
- Fixed timing vs physiology-led timing. The traditional "avoid days 2-4, convert day 5-10" teaching is being displaced by EAC, which fixes definitively as soon as resuscitation endpoints are met - sometimes within 36 hours. The day-count is a guide, not a rule.
- Who is truly 'borderline'? There is no universally validated cut-off. Lactate trajectory, base deficit, chest injury severity and response to resuscitation matter more than any single number.
- Reamed vs unreamed nailing in chest injury. The fat-embolism/second-hit concern around reaming is debated; modern data suggest adequate resuscitation matters more than reaming per se.
- Head injury and timing. Avoiding hypotension and hypoxia for the injured brain can argue for prompt fixation, complicating a simple "delay everything" approach.
- Selection bias. Because sicker patients receive DCO, observational DCO-vs-ETC comparisons cannot be taken at face value; the physiological rationale (EPOFF) remains the strongest support.
Management
Damage Control Orthopaedics Strategy
- Temporary fracture stabilization
- Minimize surgical insult ("second hit")
- Control hemorrhage from fractures
- Allow patient resuscitation and optimization
- Enable safe transfer to ICU
- External fixation - pelvis, femur, tibia, humerus
- Splinting - forearm, ankle, foot
- Spanning plates - alternative for some sites
- Wound VAC - open fractures
Definitive ORIF, intramedullary nailing with extensive reaming, prolonged surgical time, or non-essential procedures.

Surgical Technique
Anterior Pelvic External Fixation
- Unstable pelvic ring injury
- Ongoing hemorrhage
- Temporary stabilization
Position supine. Identify ASIS and iliac crest. Make 2cm incision over iliac crest, 3cm posterior to ASIS. Insert 5mm Schanz pins under image guidance, aiming toward AIIS. Two pins per side. Apply connecting bar across anterior pelvis. Tighten frame to reduce and stabilize.
Pelvic C-clamp for posterior injuries (higher risk, requires experience).
Haemorrhage Control in the Bleeding Pelvis (Escalation Ladder)
The exsanguinating pelvic ring injury is a prototypical DCO/DCR emergency. Stabilisation and haemorrhage control escalate stepwise:
- Pelvic binder — applied first, centred over the greater trochanters (not the iliac crests); reduces pelvic volume and tamponades venous/bony bleeding. A simple, immediate, life-saving step.
- Mechanical stabilisation — anterior external fixation (for anteroposterior-compression / "open-book" patterns) or a posterior C-clamp (for vertically/rotationally unstable posterior injuries) when the binder is insufficient.
- Divergent haemorrhage control by bleeding source:
- Angioembolization for arterial bleeding — suggested by a contrast blush on CT and ongoing instability despite mechanical control.
- Preperitoneal pelvic packing for venous and bony surface bleeding (the majority) — rapid, especially where angiography is unavailable or the patient is too unstable to transfer.
- REBOA (resuscitative endovascular balloon occlusion of the aorta, Zone III) — a temporising adjunct in the in extremis patient to control inflow while definitive haemorrhage control is arranged.
The binder/ex-fix controls the fracture; it does not by itself control arterial bleeding — escalate to angio/packing if the patient remains unstable.

Complications
- DCO Risk
- Lower in unstable patients
- ETC Risk
- Higher if done in unstable patient
- DCO Risk
- 5-10%
- ETC Risk
- N/A
- DCO Risk
- Possible if prolonged external fixation
- ETC Risk
- Lower
- DCO Risk
- Reduced by avoiding second hit
- ETC Risk
- Higher in unstable patient
- DCO Risk
- Similar
- ETC Risk
- Similar
Complications of External Fixation:
- Pin site infection (5-10%)
- Pin loosening
- Malunion if pins placed incorrectly
- Nerve injury from pin placement
- Conversion complexity if pins in nail path
Pin site infection increases risk of deep infection after conversion to internal fixation. If significant pin site infection develops, consider a staged approach: remove external fixator, treat infection, then definitive fixation after pin sites healed.
Postoperative Care
After DCO Stabilization
Review physiological parameters daily. The goal is to convert to definitive fixation as soon as safely possible. Prolonged external fixation increases infection risk and complicates conversion surgery.
Outcomes and Prognosis
Evidence for DCO
- Reduced ARDS in patients with femur + chest injury
- Lower mortality in borderline/unstable patients
- Comparable long-term outcomes when DCO used appropriately
- DCO in stable patients = worse outcomes (delayed care)
- DCO in unstable patients = improved survival
- Key is identifying the borderline patient
DCO vs ETC studies suffer from selection bias. Sicker patients get DCO, so direct comparisons are challenging. The principle of minimizing surgical insult in the already-stressed patient remains sound.
Guidelines, Registries & Global Practice
Global Epidemiology
- Trauma is among the leading causes of death worldwide in people aged under 45, and the leading cause of years of life lost.
- Long-bone and pelvic fractures are common in major polytrauma; the femur-plus-chest pattern is the prototypical high-risk DCO group (Pape 1993).
- Most major-trauma deaths follow a trimodal distribution; the late peak (days to weeks) from sepsis and multi-organ failure is the window DCO seeks to influence by limiting the surgical "second hit".
Side-by-Side Guidance
- Core Position
- Stable / borderline / unstable / in-extremis grading drives ETC vs DCO
- Practical Emphasis
- Physiology-led; reassess the borderline patient repeatedly
- Core Position
- Resuscitate to lactate/pH/base-excess targets, then fix definitively early (within 36h)
- Practical Emphasis
- Avoid both under-resuscitation AND unnecessary delay
- Core Position
- Major-trauma networks; definitive care at the right centre by the right team
- Practical Emphasis
- Damage control and timely transfer within a regional network
- Core Position
- Haemorrhage control and physiological correction precede skeletal reconstruction
- Practical Emphasis
- Lactate/base deficit clearance as resuscitation endpoints
- National major-trauma networks (e.g. UK TARN, German TraumaRegister DGU) link early appropriate care to lower mortality
- Registry data underpin the move from rigid "day 5-10" rules toward resuscitation-guided timing
- Damage control enables safe inter-hospital transfer to the definitive-care centre
- Well-resourced centres: ICU optimization, point-of-care coagulation (ROTEM/TEG), early conversion to definitive fixation
- Limited-resource settings: external fixation may remain the definitive construct where ICU/implant access is constrained
- External fixation is a universal core skill - low cost, rapid, life-saving for haemorrhage control
DCO is the bridge across geography and resource gaps. A patient stabilized with external fixation at a district hospital can be safely transported over long distances - relevant to remote regions of any country and to limited-resource health systems alike.
MCQ Practice Points
Q: What is the 'second hit' phenomenon in polytrauma management? A: Major surgery causes an additional inflammatory insult to an already compromised patient. This can precipitate ARDS and multi-organ failure. DCO minimizes this by delaying definitive surgery until the initial inflammatory response subsides.
Q: What are the physiological thresholds that indicate a patient needs DCO rather than ETC? A: pH less than 7.25, lactate greater than 4 mmol/L, base deficit greater than 6, temperature less than 35°C, platelets less than 50,000. Also consider DCO for ISS greater than 20, bilateral femur fractures, or femur + chest/head injury.
Q: When is the optimal time to convert external fixation to definitive fixation in DCO patients? A: Day 5-10 after injury. This is the immunological window after the initial inflammatory peak (days 2-4) has subsided. Convert when physiological parameters normalize (lactate less than 2, pH greater than 7.35).
Q: What are the four patient categories in DCO decision-making? A: Stable (ETC appropriate), Borderline (individualized decision based on parameters), Unstable (DCO mandatory), In Extremis (hemorrhage control only, no fracture fixation).
Q: Why is femoral fracture + chest injury a classic DCO indication? A: Early femoral nailing increases pulmonary complications in patients with chest injury. Pape (1993) showed early nailing with severe chest injury raised ARDS (33% vs 7.7%) and mortality (21% vs 4%). External fixation allows fracture stabilization without the second hit of intramedullary reaming.
Q: What is the single most useful parameter for monitoring resuscitation adequacy in polytrauma? A: Serial lactate. Falling lactate indicates adequate tissue perfusion. Rising or static lactate despite resuscitation suggests ongoing hemorrhage or inadequate perfusion - this patient needs DCO approach.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old male is brought to ED following a high-speed motor vehicle accident. He has bilateral femoral shaft fractures and a pulmonary contusion. His lactate is 4.5, pH 7.28, and he has required 6 units of blood in the ED. How would you manage his femoral fractures?”
“Explain the concept of damage control orthopaedics and when you would apply it.”
“A polytrauma patient had a femoral external fixator applied 3 days ago for DCO. Today their lactate is 1.5, pH 7.38, and they are hemodynamically stable off vasopressors. When would you convert to definitive fixation?”
Patient Categories
- Stable: ETC - definitive fixation
- Borderline: Decision point - use parameters
- Unstable: DCO mandatory
- In Extremis: Hemorrhage control only
DCO Indications
- pH less than 7.25
- Lactate greater than 4
- ISS greater than 20
- Bilateral femur or femur + chest injury
- Ongoing hemorrhage despite resuscitation
Second Hit Phenomenon
- Surgery is inflammatory insult
- Can precipitate ARDS, MOF
- DCO minimizes surgical trauma
- Allow inflammation to subside
Timing
- Day 0-1: Window of opportunity if stable
- Day 2-4: Avoid surgery (peak inflammation)
- Day 5-10: Safe window for conversion
- Monitor lactate, pH, base deficit
Evidence Base and Key Trials
Bone (1989) - Early vs Delayed Femoral Stabilization (RCT)
- Prospective RCT of 178 adults comparing early (less than 24h) vs delayed femoral fracture stabilization
- In multiply injured patients, DELAYED fixation increased pulmonary complications (ARDS, fat embolism, pneumonia), ICU stay and hospital stay
- Hospital costs were significantly higher in the delayed-treatment group across all patients
- Established the original 'early total care' (ETC) paradigm of urgent definitive femoral fixation
Pape (1993) - Early Femoral Nailing + Chest Injury and ARDS
- Retrospective study of 106 multiply-injured patients with femoral midshaft fracture treated by intramedullary nailing
- With severe chest injury, early (less than 24h) nailing carried higher post-traumatic ARDS (33% vs 7.7%) and mortality (21% vs 4%)
- Without chest injury, early nailing REDUCED ICU and intubation time - benefit depends on the chest
- Provided the physiological rationale that femur-plus-chest is the high-risk group
Pape - EPOFF Study (Randomized, Inflammatory Burden)
- Prospective randomized multicentre trial (n=35) in clinically stable multiply-injured patients: primary IM nailing vs DCO (external fixation then secondary nailing)
- Primary IM nailing produced a sustained perioperative rise in IL-6 and IL-8; external fixation did NOT
- Secondary conversion to a nail (day 5-10 window) caused no inflammatory surge - the 'second hit' is avoided
- No difference in ARDS/sepsis/MOF rates in this small stable cohort