Denosumab
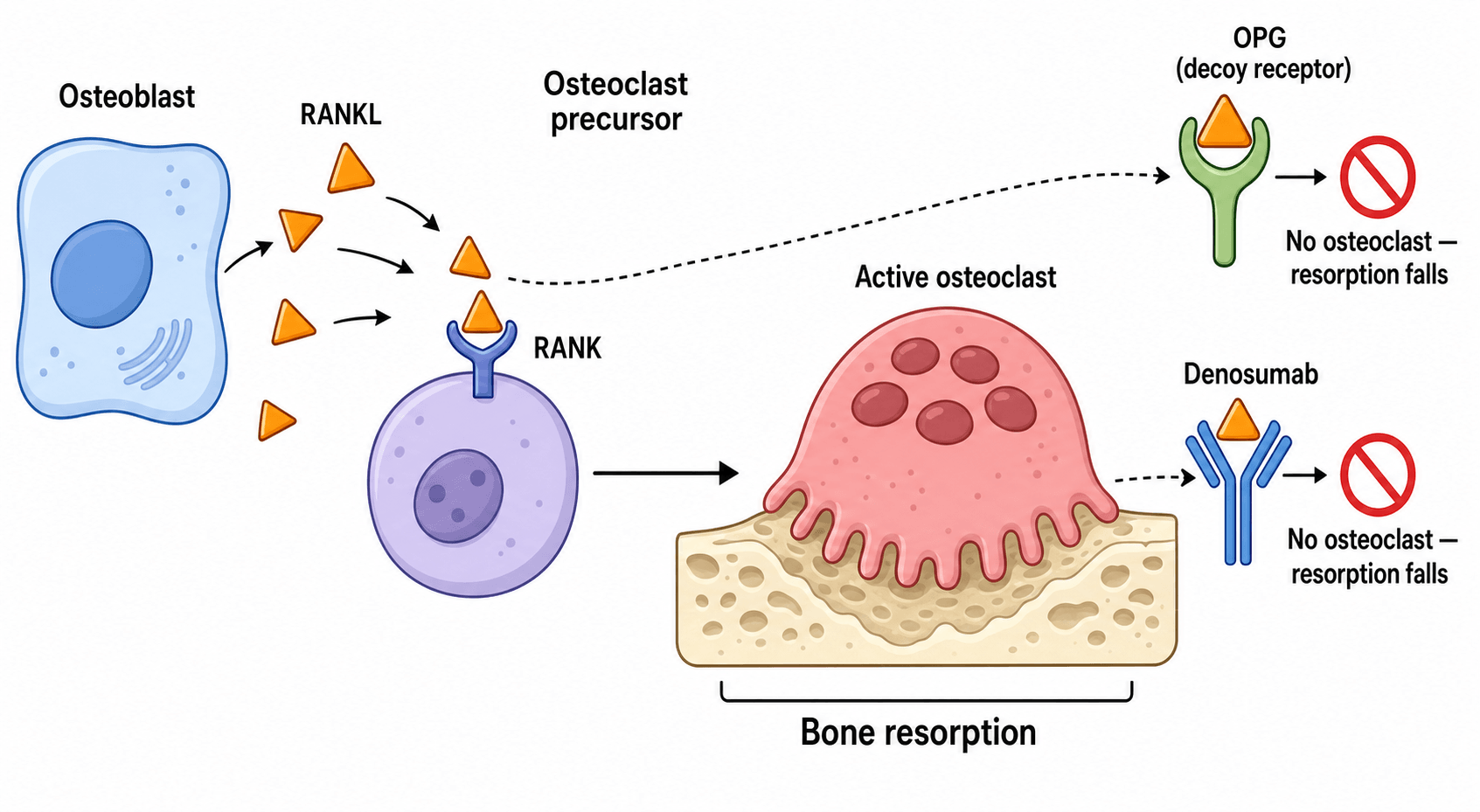
Denosumab is a monoclonal antibody to RANKL. RANKL is made by osteoblasts and binds RANK on osteoclast precursors to drive them to mature osteoclasts. By neutralising RANKL, denosumab stops osteoclast formation, function, and survival, so resorption falls and bone density rises. This is the classic basic-science answer - and the contrast with the bisphosphonate mechanism.
Because denosumab is not bound to bone, its effect is fully reversible. Stopping it causes a sharp rebound in bone turnover and rapid bone loss, and some patients suffer multiple vertebral fractures within months. Never stop denosumab without a follow-on antiresorptive (usually a bisphosphonate), and never let a dose lapse.
Denosumab can cause severe hypocalcaemia, particularly in renal impairment or vitamin D deficiency. Correct calcium and vitamin D before every dose and check renal function. This is a more prominent and earlier risk than with oral bisphosphonates.
Like all potent antiresorptives, denosumab carries the rare risks of osteonecrosis of the jaw and atypical femoral fracture - arrange dental review and counsel on thigh pain. It does not cause pill oesophagitis (it is an injection) and is not renally cleared.
Overview
Denosumab is a fully human monoclonal antibody that has become one of the most important anti-resorptive drugs in metabolic bone disease and orthopaedic oncology. Like bisphosphonates, it inhibits osteoclasts and so reduces bone resorption, raises bone mineral density, and lowers fracture risk. But it does this in a completely different way - by neutralising a single signalling protein, RANKL - and, crucially, it is not stored in the skeleton, so everything it does is reversible.
That reversibility is the heart of the topic. It gives denosumab some advantages (it works in renal impairment, and the effect can be measured cleanly) but also its single most dangerous property: when the drug is stopped or even just delayed, bone turnover rebounds and a cluster of vertebral fractures can follow. For the exam, three threads recur throughout: how it works (the RANK / RANKL / OPG system), what it treats (osteoporosis and giant cell tumour of bone, with strong evidence), and why you must never simply stop it (the rebound phenomenon).
Principles: The RANK / RANKL / OPG System
To understand denosumab you need the RANK / RANKL / OPG system - the master switch for osteoclast activity and a favourite basic-science viva.
- RANKL (receptor activator of nuclear factor-kappa-B ligand) is produced by osteoblasts and bone marrow stromal cells.
- RANK is the receptor on osteoclast precursors (and mature osteoclasts).
- When RANKL binds RANK, the precursors mature into active osteoclasts, survive longer, and resorb bone.
- Osteoprotegerin (OPG), also made by osteoblasts, is a natural decoy receptor: it binds RANKL and stops it reaching RANK, putting the brakes on resorption.
The balance of RANKL versus OPG therefore sets the rate of bone resorption. Denosumab works exactly like OPG - it is an antibody that binds RANKL and prevents it activating RANK. With RANKL neutralised, osteoclasts do not form, do not function, and do not survive, so resorption falls quickly and bone mineral density rises.
- Denosumab
- Fully human monoclonal antibody (IgG2)
- Bisphosphonates
- Synthetic pyrophosphate analogues
- Denosumab
- Binds and neutralises RANKL (acts like OPG)
- Bisphosphonates
- Bind hydroxyapatite, taken up by osteoclasts; nitrogen agents inhibit farnesyl pyrophosphate synthase
- Denosumab
- No - circulates, not stored in the skeleton
- Bisphosphonates
- Yes - bind avidly to bone mineral and persist for years
- Denosumab
- Fully reversible - effect wears off in months
- Bisphosphonates
- Long-lasting after stopping (basis of the drug holiday)
- Denosumab
- Rebound bone turnover and risk of multiple vertebral fractures
- Bisphosphonates
- Gradual offset; a drug holiday is acceptable in lower-risk patients
- Denosumab
- Not renally cleared - usable in renal impairment (watch hypocalcaemia)
- Bisphosphonates
- Renally cleared - avoid IV zoledronate if eGFR less than 35
The line examiners want to hear: denosumab and bisphosphonates reach the same end (less osteoclast resorption) by different means, and they behave very differently when stopped - which is why denosumab must never simply be discontinued.
Indications, Dosing and Routes
Denosumab is given by subcutaneous injection, with the dose and frequency depending on the indication.
- Typical regimen
- 60mg subcutaneously every 6 months
- Notes
- Marketed as Prolia; second-line or first-line where bisphosphonates are unsuitable
- Typical regimen
- 60mg subcutaneously every 6 months
- Notes
- Effective option in patients on long-term steroids
- Typical regimen
- 120mg subcutaneously monthly (with loading doses)
- Notes
- Marketed as Xgeva; for unresectable or morbid surgery, or to downstage before surgery
- Typical regimen
- 120mg subcutaneously every 4 weeks
- Notes
- Reduces skeletal-related events; higher hypocalcaemia and jaw osteonecrosis risk at this dose
- Typical regimen
- 120mg subcutaneously (refractory cases)
- Notes
- Used when bisphosphonates fail or are contraindicated by renal function
Two practical points the exam loves:
- The higher, more frequent oncology dose (120mg monthly) carries a much greater risk of osteonecrosis of the jaw and hypocalcaemia than the osteoporosis dose (60mg every 6 months).
- Because denosumab is not renally cleared, it is an option in patients with poor renal function where intravenous zoledronate would be avoided - but you must watch even more carefully for hypocalcaemia.
Denosumab's role in giant cell tumour of bone (GCTB) carries nuances examiners probe beyond the ossification response:
- It controls rather than cures. It is reserved for unresectable or axial/sacral/spinal disease, or to downstage a tumour so a less morbid operation becomes possible — not as a routine substitute for surgery in a resectable limb lesion.
- The curettage caveat. Neoadjuvant denosumab lays down a peripheral sclerotic neocortex/bony shell that can mask viable tumour at the margin, and several series report a higher local recurrence after intralesional curettage in patients pre-treated with denosumab — so its peri-operative use is debated.
- A histological pitfall. Denosumab depletes the osteoclast-like giant cells and induces new woven bone and spindle (stromal) cell proliferation, so a biopsy taken after treatment may lack the characteristic giant cells and mimic another lesion — the pathologist must be told the treatment history.
- Malignancy and metastasis. GCTB can produce benign pulmonary "metastases" in a small minority, and rare malignant transformation (secondary sarcoma) is reported — both reasons for specialist follow-up and caution with very long denosumab courses.
Complications and Safe Stopping
- Who and when
- Renal impairment, vitamin D deficiency, oncology dosing
- Key point
- Correct calcium and vitamin D before every dose; can be severe
- Who and when
- After stopping or delaying a dose
- Key point
- Sharp turnover rebound; cover with a bisphosphonate when stopping
- Who and when
- Oncology (120mg) dosing, dental work
- Key point
- Dental review before starting; far higher risk at oncology doses
- Who and when
- Long-duration potent antiresorptive use
- Key point
- Subtrochanteric or diaphyseal, transverse, thigh-pain prodrome
- Who and when
- Reported in trials
- Key point
- RANKL has immune roles; cellulitis and eczema reported
The Rebound Phenomenon - the must-know safety point
Because denosumab is not stored in bone, stopping it removes the brake on osteoclasts all at once. Bone turnover then rebounds above the pre-treatment level, bone density is lost rapidly over months, and a subset of patients sustain multiple spontaneous vertebral fractures. The risk is greatest in patients who already have vertebral fractures, who have been off therapy longer, and who gained a lot of hip bone density on treatment.
Denosumab should not be discontinued without a plan. If it must be stopped, give a follow-on antiresorptive - usually a bisphosphonate - starting about 6 months after the last injection to blunt the rebound. A missed or delayed dose carries the same danger, so injections must be given on schedule. New back pain after stopping denosumab is a rebound vertebral fracture until proven otherwise.
The cleanest viva line: "Unlike a bisphosphonate, denosumab is not bound to bone, so its effect is reversible. That is why there is no safe drug holiday - stopping it causes a rebound in bone turnover and can trigger multiple vertebral fractures, so I would either continue it long term or bridge with a bisphosphonate when stopping."
Osteonecrosis of the Jaw and Atypical Femoral Fracture
These rare class effects of potent antiresorptives also apply to denosumab. Arrange dental assessment before starting where feasible (the risk is much higher at the oncology dose), and counsel patients to report new thigh pain, which warrants radiographs of both femurs to look for an atypical femoral fracture.
The rebound after stopping denosumab does not only cause fractures — the same surge in osteoclast activity can release skeletal calcium and produce rebound hypercalcaemia. It is reported weeks to months after a missed or final dose and is most characteristic in children and young adults, particularly those treated for giant cell tumour of bone at the high oncology dose with a growing skeleton. It can be severe and symptomatic (the usual hypercalcaemia picture — confusion, dehydration, renal impairment). Anticipate it: monitor calcium after stopping in at-risk (especially young or oncology) patients, and treat with rehydration and a bisphosphonate, which also blunts the underlying turnover rebound. So denosumab can cause hypocalcaemia during treatment and hypercalcaemia after it is stopped in the at-risk group.
Clinical Relevance
Denosumab turns up across the whole exam and in daily orthopaedic practice. In fracture liaison and bone-health clinics it is a key agent for secondary fracture prevention, especially when bisphosphonates are not tolerated or renal function is poor. In basic-science vivas the RANK / RANKL / OPG axis and the contrast with bisphosphonates are classic asks. In orthopaedic oncology denosumab is central to the modern management of giant cell tumour of bone, both to downstage tumours before surgery and to treat unresectable disease. And the rebound fracture problem - recognising it, preventing it, and never stopping the drug without cover - is a safety-critical theme examiners reward. Knowing when to start, how to dose, what to check before each injection, and how to stop safely is the practical core.
Guidelines, Registries and Global Practice
- Osteoporosis guidelines (for example AAOS/AOA bone-health initiatives, NICE/NOGG in the UK, and endocrine society guidance) position denosumab as an effective antiresorptive, often second-line or for patients in whom bisphosphonates are unsuitable (for example renal impairment or intolerance), given its efficacy and non-renal clearance.
- The rebound phenomenon is now formally recognised across major bodies: the European Calcified Tissue Society and others advise never stopping denosumab without follow-on antiresorptive cover, usually a bisphosphonate started about 6 months after the last dose.
- In orthopaedic oncology, denosumab is established for giant cell tumour of bone - to downstage unresectable or morbid lesions and to control disease - with specialist guidance emphasising close imaging follow-up because the tumour can recur after cessation.
- Global practice variation largely reflects cost, access, and whether a bisphosphonate or denosumab is preferred first-line, rather than disagreement on the underlying biology - but the safety message about not stopping denosumab is universal.
Memory aids
RANKDenosumab Mechanism and Identity
Hook:Think RANK - it blocks RANKL, is an Antibody not stored in bone, leaves No osteoclasts, and is Kidney-safe to clear.
CRABDenosumab Complications
Hook:Watch the CRAB - Calcium low, Rebound fractures, Atypical femoral fracture, Bone necrosis of the jaw.
BRAVEDenosumab vs Bisphosphonates
Hook:Be BRAVE comparing the two - Bone binding, Reversible, Antibody, Very different on stopping, Excretion route.

Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman with osteoporosis and chronic kidney disease is started on denosumab because a bisphosphonate was unsuitable. The examiner asks how denosumab works, how it differs from bisphosphonates, and what you would check before each dose.”
“A 68-year-old woman stopped denosumab a year ago after several years of treatment because she moved and lost follow-up. She now presents with sudden severe back pain after bending. How do you proceed and what has gone wrong?”
Mechanism
- Fully human monoclonal antibody to RANKL
- Neutralises RANKL, acting like natural osteoprotegerin (OPG)
- Osteoclasts do not form, function, or survive - resorption falls
- Not bound to bone, so the effect is fully reversible
Indications and Dose
- Osteoporosis: 60mg subcutaneously every 6 months (Prolia)
- Giant cell tumour of bone: 120mg monthly (Xgeva)
- Bone metastases / myeloma: 120mg every 4 weeks
- Usable in renal impairment - not renally cleared
Before Each Dose
- Correct calcium and vitamin D - can cause severe hypocalcaemia
- Check renal function (hypocalcaemia risk higher if impaired)
- Arrange dental review (especially at oncology doses)
- Confirm the patient will continue - never let a dose lapse
Red Flags
- Stopping or delaying - rebound multiple vertebral fractures
- If stopping, bridge with a bisphosphonate about 6 months after last dose
- Thigh pain on long-term use - image both femurs for atypical fracture
- Exposed jaw bone for more than 8 weeks - osteonecrosis of the jaw
Evidence
Every citation below has been checked against its source record in PubMed. FREEDOM is the pivotal fracture-prevention RCT; the ECTS position statement formalises the rebound-on-discontinuation problem and the bridging strategy; and the van Langevelde review describes the characteristic ossification response of giant cell tumour of bone to denosumab.
Denosumab for prevention of fractures in postmenopausal women with osteoporosis (FREEDOM)
- Double-blind RCT, 7868 postmenopausal women, denosumab 60mg subcutaneously every 6 months vs placebo over 3 years
- New radiographic vertebral fracture cut by about 68 percent (2.3 vs 7.2 percent)
- Hip fracture reduced by about 40 percent (0.7 vs 1.2 percent) and nonvertebral fracture by about 20 percent
- No increase in cancer, infection, delayed fracture healing, or hypocalcaemia, and no jaw osteonecrosis in this 3-year study
Stopping Denosumab Causes Rebound Bone Loss and Vertebral Fractures (ECTS Position Statement)
- Systematic review and European Calcified Tissue Society position statement on stopping denosumab
- Discontinuation drives bone turnover above pre-treatment levels, with rapid bone loss and multiple vertebral fractures in some patients
- Higher risk with prevalent vertebral fractures, longer time off therapy, and larger gains then losses in hip bone density
- If denosumab is stopped, start an antiresorptive (usually a bisphosphonate) about 6 months after the last dose
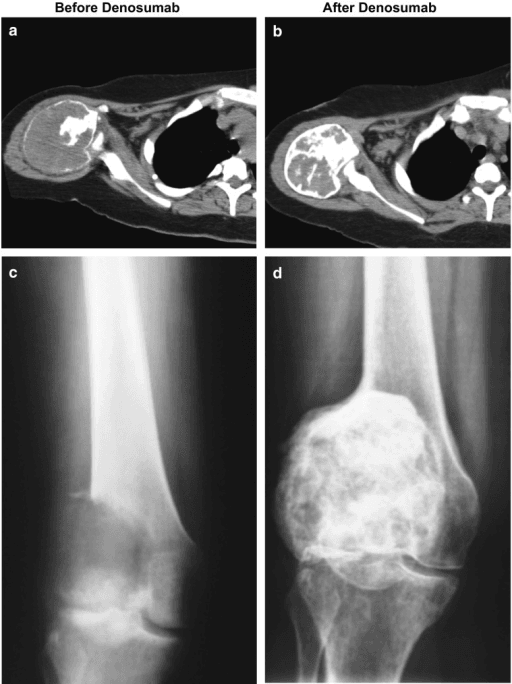
Imaging Response of Giant Cell Tumour of Bone to Denosumab (Review)
- Denosumab inhibits the RANK / RANKL pathway that drives osteoclast-like giant cells in giant cell tumour of bone
- Imaging response includes a new sclerotic neocortex, matrix osteosclerosis, and reconstitution of subarticular bone
- Reduced FDG-PET avidity is an early sensitive sign of response
- Local recurrence after stopping denosumab and rare malignant transformation mean close specialist follow-up is needed