Calcium Homeostasis & Metabolic Bone Disease
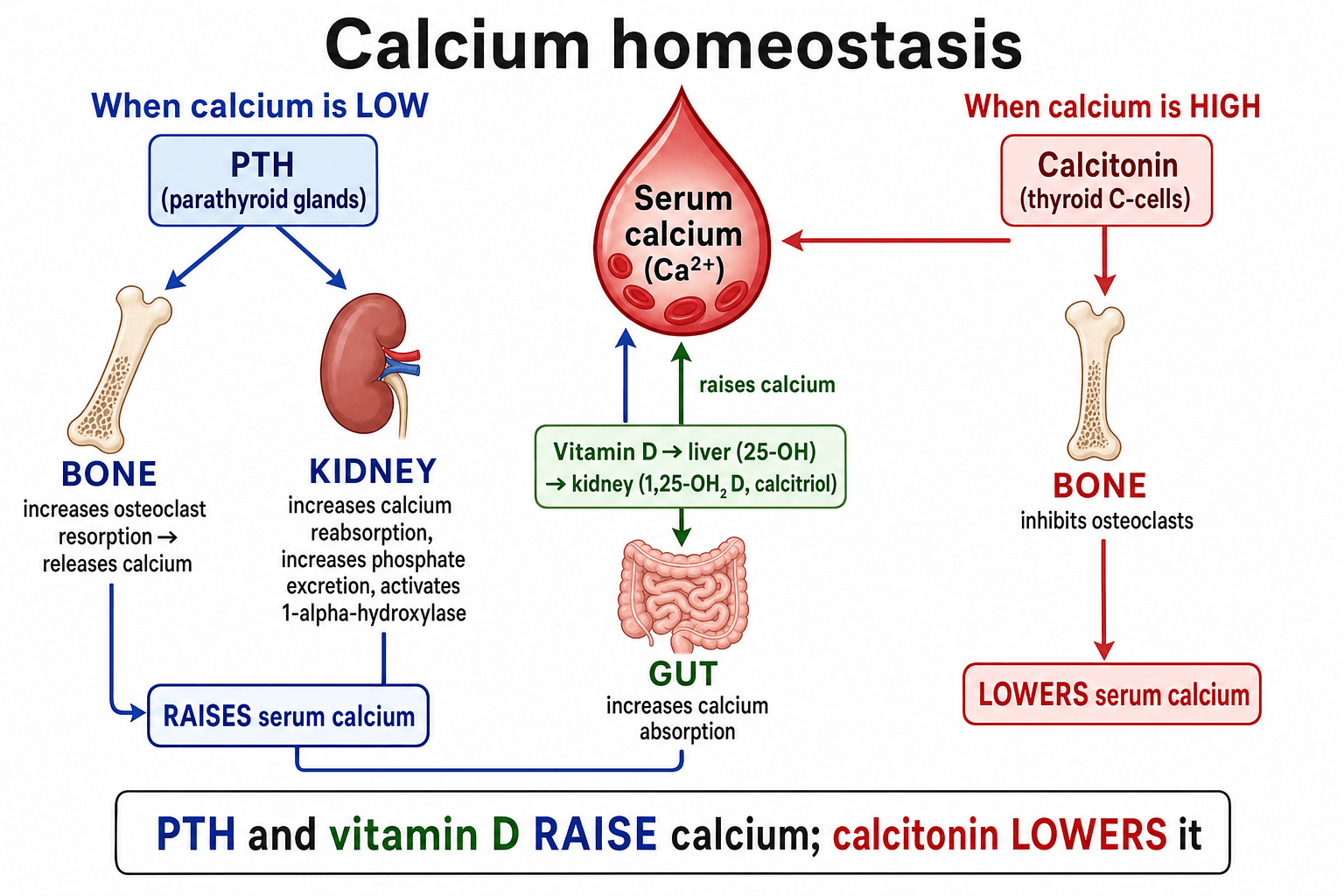
A fall in calcium triggers PTH release. PTH raises calcium by resorbing bone, increasing renal calcium reabsorption (while losing phosphate), and activating vitamin D in the kidney, which then boosts gut calcium absorption. Knowing this loop cold answers most calcium vivas.
Osteomalacia is defective mineralisation - soft bone, Looser zones, high alkaline phosphatase, often low calcium, phosphate and vitamin D. Osteoporosis is reduced bone mass with normal mineral and normal routine biochemistry. Do not confuse the two.
In a well outpatient, think primary hyperparathyroidism. In an unwell or known-cancer patient, think malignancy (PTH suppressed). Check PTH early: high or inappropriately normal PTH points to the parathyroids, a low PTH points elsewhere.
Skin and diet give inactive vitamin D, the liver makes 25-OH-D (measured to assess status), and the kidney makes active 1,25-(OH)2-D (calcitriol). Renal failure means little calcitriol, low calcium, and secondary hyperparathyroidism.
Overview
Serum calcium is held in a very narrow range (about 2.2 to 2.6 mmol/L) because it is essential for nerve and muscle function, clotting, and as a building block of bone. The body achieves this with three hormones acting on three organs: parathyroid hormone, active vitamin D (calcitriol) and calcitonin acting on bone, gut and kidney. Bone is both the largest calcium store and a tissue under constant remodelling, so calcium balance and skeletal health are inseparable.
Metabolic bone diseases are the conditions that arise when this system goes wrong or when bone turnover itself is disordered. For the exam, the high-value distinctions are simple to state but easy to muddle: osteoporosis is too little bone of normal quality, osteomalacia and rickets are bone that is normal in amount but poorly mineralised, hyperparathyroidism is too much PTH, and Paget disease is chaotic, accelerated remodelling. This topic builds the calcium axis first, then uses it to make sense of each disease and its biochemistry.
Physiology of the Calcium Control System
About 99 percent of body calcium is stored in bone as hydroxyapatite. The small fraction in blood exists in three forms: ionised (the active, regulated fraction, about half), protein-bound (mostly to albumin), and complexed with anions. Because only ionised calcium is biologically active, a low albumin lowers total calcium without making the patient hypocalcaemic - this is why we correct calcium for albumin or measure ionised calcium.
The three hormones:
- Source
- Parathyroid chief cells
- Main actions
- Resorbs bone, increases renal calcium reabsorption, loses phosphate, activates vitamin D in kidney
- Net effect on calcium
- Raises calcium
- Source
- Kidney (final step)
- Main actions
- Increases gut absorption of calcium and phosphate, supports bone mineralisation
- Net effect on calcium
- Raises calcium and phosphate
- Source
- Thyroid C cells
- Main actions
- Inhibits osteoclasts
- Net effect on calcium
- Lowers calcium (minor role in humans)
- A fall in ionised calcium is sensed by the calcium-sensing receptor on parathyroid cells, which release PTH.
- PTH acts on bone to stimulate osteoclastic resorption (indirectly, through RANKL on osteoblasts) and on the kidney to reabsorb more calcium while excreting phosphate.
- PTH also switches on renal 1-alpha-hydroxylase, converting 25-OH-D to active calcitriol, which increases gut absorption of calcium.
- As calcium rises, PTH secretion is suppressed - a classic negative feedback loop.
PTH is phosphaturic, so high PTH tends to give a high calcium and a low phosphate, while calcitriol raises both. Tracking calcium, phosphate, PTH and alkaline phosphatase together is what lets you read any metabolic bone picture.
The classic teaching of "three hormones" handles calcium well but understates phosphate, which is governed chiefly by fibroblast growth factor 23 (FGF23) — a hormone examiners increasingly ask about. FGF23 is secreted by osteocytes and osteoblasts in response to a phosphate load and to calcitriol, and acts on the kidney using the obligatory co-receptor Klotho. Its two actions both lower phosphate and lower calcitriol: it is strongly phosphaturic (it down-regulates the proximal-tubule sodium-phosphate cotransporters NaPi-IIa and NaPi-IIc) and it suppresses renal 1-alpha-hydroxylase while up-regulating 24-hydroxylase — so it opposes PTH on vitamin D activation but shares PTH's phosphaturic effect. FGF23 rises very early in chronic kidney disease, often the first measurable abnormality of CKD-MBD before phosphate or PTH change, and excess FGF23 drives the hereditary and tumour-induced phosphate-wasting forms of rickets and osteomalacia (loss of FGF23 activity instead causes hyperphosphataemic tumoral calcinosis).
The Vitamin D Pathway
Vitamin D begins as an inactive precursor: cholecalciferol (D3) made in skin under UVB light or taken in the diet, and ergocalciferol (D2) from plants. It then passes through two hydroxylation steps:
- Liver: adds a hydroxyl at carbon 25 to make 25-hydroxyvitamin D (25-OH-D). This is the stable, abundant storage form and is the one measured to assess vitamin D status.
- Kidney: adds a hydroxyl at carbon 1 (by 1-alpha-hydroxylase, stimulated by PTH and low phosphate) to make active 1,25-dihydroxyvitamin D (calcitriol).
Calcitriol then increases intestinal absorption of calcium and phosphate, supports normal bone mineralisation, and feeds back to suppress PTH. Two clinical consequences follow directly: liver disease impairs the first step, and kidney disease impairs the activating second step, so chronic kidney disease produces low calcitriol, low calcium and secondary hyperparathyroidism (renal osteodystrophy).
Measure 25-OH-D to judge vitamin D status, not calcitriol. Calcitriol has a short half-life and can be kept normal by a high PTH even when stores are low, so it is a poor marker of deficiency.
The Metabolic Bone Diseases
Reading the biochemistry
The single most useful exam skill is reading the calcium / phosphate / PTH / alkaline phosphatase pattern. The table below summarises the classic pictures.
- Calcium
- Normal
- Phosphate
- Normal
- PTH
- Normal
- Alk phos
- Normal
- Calcium
- Low or low-normal
- Phosphate
- Low
- PTH
- High (secondary)
- Alk phos
- High
- Calcium
- High
- Phosphate
- Low
- PTH
- High or inappropriately normal
- Alk phos
- High or normal
- Calcium
- Low or normal
- Phosphate
- High
- PTH
- High
- Alk phos
- High
- Calcium
- Normal
- Phosphate
- Normal
- PTH
- Normal
- Alk phos
- Very high (isolated)
Osteoporosis
Osteoporosis is reduced bone mass with deteriorated microarchitecture, so bone is normal in composition but there is simply less of it, raising fragility-fracture risk. Mineralisation and routine biochemistry are normal, which is the key distinction from osteomalacia. Diagnosis is by DXA (a T-score of -2.5 or lower at hip or spine) or by a low-trauma fragility fracture. Management combines lifestyle measures, calcium and vitamin D sufficiency, and bone-active drugs (anti-resorptives such as bisphosphonates and denosumab, or anabolic agents such as teriparatide and romosozumab in high-risk patients).
Osteomalacia and Rickets
Osteomalacia is defective mineralisation of osteoid in the adult skeleton; in the growing child the same defect at the growth plate is called rickets. The usual cause is vitamin D deficiency (low sunlight, poor intake, malabsorption), but it also follows chronic kidney disease, certain anticonvulsants, and rare phosphate-wasting disorders. Patients have bone pain, proximal muscle weakness and fractures; children develop bowing, metaphyseal widening and growth failure. The radiographic hallmark is the Looser zone (pseudofracture) - a transverse lucent band where unmineralised osteoid has accumulated, as shown in the imaging above. Treatment is vitamin D and calcium replacement, correcting the underlying cause.
Rickets and osteomalacia are a final common pathway of defective mineralisation, and examiners expect the aetiological split into a calcium/vitamin D group and a phosphate-wasting group.
Calcipenic (vitamin D / calcium pathway) — the common group: nutritional vitamin D (or dietary calcium) deficiency; vitamin-D-dependent rickets type 1 (1-alpha-hydroxylase deficiency, so 25-OH-D is normal but calcitriol is low — responds to calcitriol); and vitamin-D-dependent rickets type 2 (end-organ resistance from a vitamin D receptor mutation, so calcitriol is high, classically with alopecia). These share a biochemistry of low or low-normal calcium with a secondary high PTH and low phosphate.
Phosphopenic (phosphate-wasting) — renal phosphate loss, usually FGF23-mediated: X-linked hypophosphataemic rickets (the commonest heritable form, a PHEX mutation raising FGF23 — treated with phosphate plus calcitriol, or the anti-FGF23 antibody burosumab); tumour-induced (oncogenic) osteomalacia (an FGF23-secreting mesenchymal tumour, curable by excision); and renal tubular disorders such as Fanconi syndrome and renal tubular acidosis. These show normal calcium with a normal or only mildly raised PTH and an isolated low phosphate — the key discriminator from the calcipenic group.
Hyperparathyroidism
- Mechanism
- Autonomous adenoma (most), hyperplasia or carcinoma
- Calcium
- High
- PTH
- High or inappropriately normal
- Mechanism
- Gland responds to low calcium (often renal failure or vitamin D deficiency)
- Calcium
- Low or normal
- PTH
- High
- Mechanism
- Long-standing secondary becomes autonomous (often after years of renal disease)
- Calcium
- High
- PTH
- Very high
Primary hyperparathyroidism is the classic cause of high calcium in the well outpatient, usually from a single adenoma, and may be silent or cause stones, bone disease and the wider hypercalcaemia symptoms. Severe disease can produce osteitis fibrosa cystica (brown tumours, subperiosteal resorption, salt-and-pepper skull). Parathyroidectomy is the definitive treatment when criteria are met.
Paget Disease of Bone
Paget disease is disordered, accelerated remodelling producing structurally weak, enlarged bone. It often affects the pelvis, spine, skull and long bones, and may be silent or cause bone pain, deformity (bowing), deafness and rarely high-output cardiac failure or sarcomatous change. Biochemistry shows an isolated, often very high alkaline phosphatase with normal calcium and phosphate. Bisphosphonates, especially a single zoledronic acid infusion, suppress the high turnover and relieve pain.
Clinical Relevance
Calcium homeostasis underpins much of orthopaedic and exam practice. In fracture clinic and fracture liaison services, recognising and correcting vitamin D deficiency and osteoporosis is central to secondary prevention. In basic-science vivas, the PTH-vitamin D axis and the biochemical patterns of metabolic bone disease are classic asks. In trauma and elective surgery, poorly mineralised or low-density bone changes fixation strategy and healing. And in perioperative care, both severe hypercalcaemia and symptomatic hypocalcaemia are emergencies. Being able to read a calcium / phosphate / PTH / alkaline phosphatase panel and act on it is the practical core that examiners reward.
Calcium Emergencies
- Typical features
- Confusion, polyuria, dehydration, arrhythmia (short QT)
- Immediate management
- Aggressive IV fluids, then IV bisphosphonate; treat the cause
- Typical features
- Tetany, perioral and digital paraesthesia, Chvostek and Trousseau signs, long QT, seizures
- Immediate management
- IV calcium gluconate with cardiac monitoring, then correct cause and magnesium
- Typical features
- Profound hypocalcaemia after parathyroidectomy as bone rapidly remineralises
- Immediate management
- Aggressive calcium and active vitamin D replacement
Calcium above about 3.5 mmol/L, or any patient with confusion, marked dehydration or arrhythmia, needs urgent treatment. Start with generous intravenous fluid rehydration to restore volume and promote calcium excretion, then give an intravenous bisphosphonate, and treat the underlying cause. Loop diuretics are only added once the patient is fully rehydrated.
Guidelines, Registries and Global Practice
- Osteoporosis and bone-health guidance worldwide (for example AAOS/AOA bone-health initiatives, NICE/NOGG in the UK, and endocrine society guidance) recommends ensuring calcium and vitamin D sufficiency as the foundation on which bone-active drug therapy is added.
- Vitamin D supplementation evidence supports targeted replacement of those who are deficient or at high risk rather than blanket high-dose use in healthy, replete older adults.
- Primary hyperparathyroidism consensus guidelines list bone protection (low bone density or fragility fracture), high calcium, young age and renal involvement among the recognised indications for parathyroidectomy.
- Renal bone disease (CKD-MBD) guidance frames management around controlling phosphate, providing active vitamin D analogues, and managing secondary hyperparathyroidism, with the aim of protecting both bone and the cardiovascular system.
Memory aids
PHEXWhat PTH Does
Hook:PTH does PHEX - Phosphate out, High calcium, Eats bone, eXtra vitamin D.
CHIMPANZEESCauses of Hypercalcaemia
Hook:CHIMPANZEES covers the causes of high calcium - the big two are hyperParaThyroidism and Malignancy.
BONESSymptoms of Hypercalcaemia
Hook:Stones, BONES, abdominal moans and psychic groans - the classic picture of hypercalcaemia.


Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows you a normal serum calcium and asks how the body keeps calcium in such a narrow range. Take me through the control system.”
“A 62-year-old woman has widespread bone pain and proximal muscle weakness. Calcium is low-normal, phosphate is low, alkaline phosphatase is high and PTH is elevated. What is the diagnosis and how would you manage her?”
The Axis
- PTH raises calcium, lowers phosphate (phosphaturic)
- Calcitriol raises gut absorption of calcium and phosphate
- Calcitonin lowers calcium (minor role in humans)
- Organs: bone (resorption), kidney (reabsorb + activate vit D), gut (absorb)
Vitamin D
- Liver makes 25-OH-D (storage form, measured)
- Kidney makes active 1,25-(OH)2-D (calcitriol)
- Renal failure: low calcitriol, low calcium, secondary hyperparathyroidism
Read the Biochemistry
- Osteoporosis: all normal, low bone density
- Osteomalacia: low phosphate, high alk phos, secondary high PTH
- Primary hyperparathyroidism: high calcium, low phosphate, high PTH
- Paget: isolated very high alkaline phosphatase
Red Flags
- Severe hypercalcaemia - fluids first, then IV bisphosphonate
- Tetany / long QT - symptomatic hypocalcaemia needs IV calcium
- Looser zones - radiographic hallmark of osteomalacia
- Correct calcium for albumin or measure ionised calcium
Evidence for Calcium and Vitamin D
Every citation below has been checked against its source record in PubMed. The pairing is deliberate: calcium PLUS vitamin D reduces fractures (Weaver/NOF), but vitamin D ALONE in already-replete healthy elders does not (DO-HEALTH) — so the message is targeted replacement, not blanket high-dose supplementation. The parathyroidectomy data show surgery also protects the skeleton.
Calcium plus Vitamin D Reduces Fractures (NOF Meta-analysis)
- Meta-analysis of 8 randomised controlled trials, 30,970 participants
- Calcium plus vitamin D supplementation cut total fractures by about 15 percent (relative risk 0.85)
- Hip fractures were reduced by about 30 percent (relative risk 0.70)
- Benefit seen in both community-dwelling and institutionalised middle-aged to older adults
Vitamin D Alone Does Not Improve Outcomes in Healthy Elderly (DO-HEALTH)
- Double-blind RCT, 2157 generally healthy adults aged 70 or older, 3-year follow-up
- Vitamin D3 2000 IU/day, omega-3, and exercise tested alone and in combination
- No significant benefit on nonvertebral fractures, blood pressure, physical performance or cognition
- Suggests routine high-dose vitamin D does not help robust, replete older adults
Parathyroidectomy for Normocalcemic Primary Hyperparathyroidism is Associated with Improved Bone Mineral Density Regardless of Postoperative PTH
- Single-centre cohort of 661 parathyroidectomies for primary hyperparathyroidism, of whom 68 had the normocalcaemic variant (28 with paired bone-density data)
- The normocalcaemic patients gained bone density at the lumbar spine (about 1.8 percent) and total hip (about 1.6 percent) at 18 months
- Bone density improved even when postoperative PTH remained persistently elevated
- Supports surgery for bone protection in selected (including normocalcaemic) primary hyperparathyroidism