Bisphosphonates
Bisphosphonates are pyrophosphate analogues that bind bone mineral and are swallowed by osteoclasts during resorption. Nitrogen-containing agents then inhibit farnesyl pyrophosphate synthase, the osteoclast loses its ruffled border and undergoes apoptosis, and resorption falls. This is the classic basic-science viva answer.
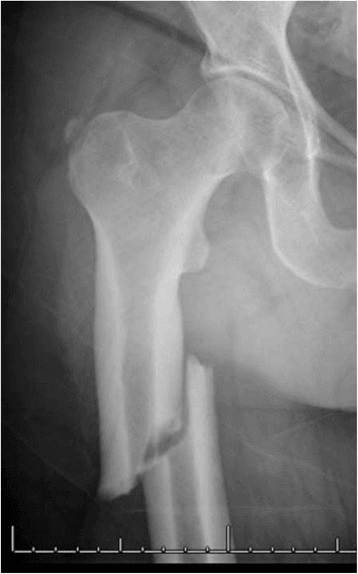
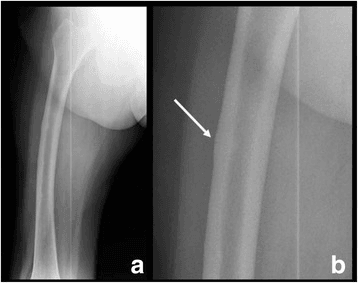
Subtrochanteric or diaphyseal, transverse fracture with lateral cortical thickening (beaking), often a medial spike, frequently bilateral, and preceded by thigh pain. New thigh pain on a bisphosphonate means radiograph BOTH femurs.
Exposed necrotic jaw bone for more than 8 weeks in a patient on an antiresorptive with no prior jaw radiotherapy. Risk is far higher with intravenous / oncology dosing and after dental extraction - dental review before starting.
Check and correct calcium and vitamin D (hypocalcaemia risk), assess renal function (avoid zoledronate if eGFR less than 35), and counsel on oral administration to avoid oesophagitis.
Overview
Bisphosphonates are the most widely used anti-resorptive drugs in orthopaedic and metabolic bone practice. They reduce bone turnover by inhibiting osteoclasts, which slows bone loss, raises bone mineral density, and lowers fracture risk. They are first-line treatment for osteoporosis and are also used in Paget disease, hypercalcaemia of malignancy, bone metastases and multiple myeloma, and paediatric osteogenesis imperfecta.
For the exam, three threads matter and recur throughout this topic: how they work (a clean basic-science mechanism), what they prevent (fractures, with strong randomised evidence), and what can go wrong (the rare but heavily examined complications of atypical femoral fracture and osteonecrosis of the jaw, and the drug-holiday concept that follows from them).
Indications
Postmenopausal, male, and glucocorticoid-induced osteoporosis - the commonest indication and first-line pharmacological therapy for fracture prevention.
Reduce pain and disordered bone turnover. A single zoledronic acid infusion gives durable suppression of the elevated alkaline phosphatase.
Hypercalcaemia of malignancy, and reduction of skeletal-related events in bone metastases and multiple myeloma (usually higher, more frequent dosing than in osteoporosis).
Osteogenesis imperfecta - cyclical intravenous pamidronate reduces fracture rate and bone pain in moderate to severe disease.
Mechanism of Action
Bisphosphonates are stable synthetic analogues of pyrophosphate, in which the central oxygen is replaced by a carbon atom (the P-C-P backbone). That carbon makes them resistant to enzymatic breakdown, and two side chains determine behaviour: one side chain (usually a hydroxyl) gives high affinity for bone mineral, while the second side chain determines anti-resorptive potency.

How they reach and act on the osteoclast:
- After absorption, bisphosphonates rapidly bind hydroxyapatite at sites of active bone remodelling, where mineral is exposed.
- During resorption the osteoclast ingests bone mineral and, with it, the bound bisphosphonate.
- Inside the osteoclast the drug disrupts function, the ruffled border is lost, and the cell undergoes apoptosis.
- Net effect: osteoclast-mediated resorption falls, the remodelling space closes, secondary mineralisation continues, and bone mineral density rises.
Two chemical classes with different intracellular targets:
- Non-nitrogen (older)
- Etidronate, clodronate, tiludronate
- Nitrogen-containing (modern)
- Alendronate, risedronate, ibandronate, zoledronate
- Non-nitrogen (older)
- Incorporated into non-hydrolysable ATP analogues that poison the osteoclast
- Nitrogen-containing (modern)
- Inhibit farnesyl pyrophosphate synthase in the mevalonate pathway
- Non-nitrogen (older)
- Direct cytotoxicity to the osteoclast
- Nitrogen-containing (modern)
- Loss of GTPase prenylation (Ras, Rho, Rac), so the osteoclast cannot ruffle or survive
- Non-nitrogen (older)
- Lower potency, largely historical
- Nitrogen-containing (modern)
- High potency, first-line agents today
The mevalonate-pathway step is the high-yield detail: nitrogen-containing bisphosphonates block farnesyl pyrophosphate synthase, so the small GTPases that the osteoclast depends on are never prenylated (lipid-anchored to the membrane). Statins act on the same pathway higher up (HMG-CoA reductase), which is a favourite linking question.
Agents, Potency and Routes
- Class
- Nitrogen-containing
- Typical route and dose
- Oral 70mg weekly
- Notes
- Most widely used first-line oral agent
- Class
- Nitrogen-containing
- Typical route and dose
- Oral 35mg weekly
- Notes
- Alternative oral agent, similar efficacy
- Class
- Nitrogen-containing
- Typical route and dose
- IV 5mg once yearly (osteoporosis)
- Notes
- Most potent, useful if oral not tolerated
- Class
- Nitrogen-containing
- Typical route and dose
- IV infusion
- Notes
- Paget disease, hypercalcaemia, paediatric osteogenesis imperfecta
- Class
- Non-nitrogen
- Typical route and dose
- Oral
- Notes
- Older agent, can impair mineralisation if used continuously
Relative potency runs zoledronate greater than risedronate greater than ibandronate greater than alendronate greater than etidronate, reflecting both binding affinity for bone mineral and how strongly each inhibits the target enzyme.
Pharmacokinetics
The pharmacokinetics explain three things examiners link together — the strict oral dosing, the renal caution, and the drug holiday:
- Very low oral bioavailability — under about 1 per cent — and it is further abolished by food, calcium, and other cations (which chelate the drug). This is the pharmacological reason for the empty-stomach, plain-water, nothing-else-for-30-to-60-minutes regimen (the "WAVE" rules); poor administration is the commonest cause of treatment failure and intolerance.
- Not metabolised. Bisphosphonates are not biotransformed — there is no hepatic metabolism and no cytochrome interaction.
- Two fates for absorbed drug: roughly half is rapidly taken up by bone at sites of active remodelling, and the remainder is excreted unchanged by the kidney. Renal clearance is why zoledronate is avoided at a low eGFR and given as a slow, well-hydrated infusion.
- The plasma half-life is short, but the skeletal half-life is extremely long — years (alendronate's is estimated at up to roughly a decade) — because the drug is buried in bone and only slowly liberated during later remodelling.
- This long skeletal residence is the BASIS of the drug holiday: fracture-protection persists for a period after stopping because the bone-bound drug keeps acting, which is exactly why a planned pause is feasible — and, by contrast, why a non-bone-bound agent such as denosumab cannot be simply stopped (see below).
Complications
- Who and when
- Oral agents, poor administration
- Key point
- Empty stomach, full glass of water, stay upright 30 to 60 minutes
- Who and when
- First IV dose
- Key point
- Flu-like fever and myalgia for 1 to 3 days - warn and pre-hydrate
- Who and when
- Vitamin D deficient or untreated
- Key point
- Correct calcium and vitamin D before starting
- Who and when
- IV zoledronate
- Key point
- Avoid if eGFR is less than 35, infuse slowly, ensure hydration
- Who and when
- Long-duration use
- Key point
- Subtrochanteric or diaphyseal, transverse, thigh-pain prodrome
- Who and when
- IV / oncology dosing, dental work
- Key point
- Exposed necrotic jaw bone for more than 8 weeks
Atypical Femoral Fracture (AFF)
AFFs occur in the subtrochanteric region or femoral diaphysis and have a characteristic look: a transverse or short-oblique fracture line that begins at the lateral cortex, focal thickening (beaking) of that lateral cortex, a medial spike, minimal comminution, and frequent bilateral involvement. Many patients describe prodromal thigh or groin pain for weeks to months. The absolute risk is low and the fracture-prevention benefit greatly outweighs it for most patients, but the risk rises with treatment duration.
New or worsening thigh pain in a patient on a bisphosphonate is an atypical femoral fracture until proven otherwise - image BOTH femurs (full-length views). An incomplete AFF with pain often needs prophylactic intramedullary nailing; a complete fracture needs fixation.
Medication-Related Osteonecrosis of the Jaw (MRONJ)
MRONJ Definition and Management (AAOMS Position Paper, 2022 Update)
- MRONJ: exposed jaw bone, or bone probed through a fistula, persisting for more than 8 weeks
- Occurs in a patient on antiresorptive or antiangiogenic therapy with no history of jaw radiotherapy
- Risk is markedly higher with intravenous and oncology-dose therapy and after dental extraction
- Prevention centres on dental assessment and treatment before starting therapy where feasible
The Drug Holiday
Because the rare complications (AFF and MRONJ) are linked to cumulative duration, while the fracture benefit persists for a time after stopping (bisphosphonate stays bound to bone), guidelines suggest reassessing after about 3 to 5 years of oral therapy or 3 years of intravenous therapy:
- Lower risk patients (good bone density gain, no recent fracture): consider a drug holiday and reassess every 1 to 3 years.
- Higher risk patients (previous hip or vertebral fracture, very low bone density, ongoing steroids): continue treatment, as the fracture-prevention benefit dominates.
- The holiday is a pause with planned review, not permanent cessation - bone density and fracture risk are reassessed and treatment restarted when indicated.
Where Bisphosphonates Sit Among Osteoporosis Drugs
Examiners frequently ask you to place bisphosphonates within the wider armamentarium and to contrast them with denosumab — the comparison that most often catches candidates out.
- Class / mechanism
- Anti-resorptive — FPP synthase inhibition
- Bound to bone?
- Yes
- Key exam point
- Effect persists after stopping; drug holiday possible
- Class / mechanism
- Anti-resorptive — monoclonal antibody to RANKL (blocks osteoclast formation)
- Bound to bone?
- No
- Key exam point
- Reversible; stopping causes a REBOUND with multiple vertebral fractures — no drug holiday
- Class / mechanism
- Anti-resorptive — selective oestrogen-receptor modulator
- Bound to bone?
- No
- Key exam point
- Reduces vertebral (not hip) fracture; lowers breast-cancer risk but raises VTE
- Class / mechanism
- Anabolic — PTH / PTHrP analogue (intermittent dosing builds bone)
- Bound to bone?
- No
- Key exam point
- For severe/high-risk disease; limited course (about 2 years); follow with an anti-resorptive
- Class / mechanism
- Dual — sclerostin monoclonal antibody (builds bone and reduces resorption)
- Bound to bone?
- No
- Key exam point
- Potent for very high risk; cardiovascular caution; follow with an anti-resorptive
Denosumab has NO drug holiday — this is the contrast examiners want. Because denosumab is a circulating antibody and is not bound to bone, its effect reverses completely on cessation: stopping (or even delaying) a dose triggers a rebound surge in bone turnover and a risk of multiple spontaneous vertebral fractures within months. Denosumab must therefore be continued indefinitely or, if stopped, followed promptly by a bisphosphonate to lock in the gains. Bisphosphonates are the exception precisely because they are buried in bone — which is why a planned holiday is safe for them but not for denosumab. (Anabolic agents — teriparatide, abaloparatide, romosozumab — must likewise be followed by an anti-resorptive, or their gains are lost.)
Clinical Relevance
Bisphosphonates appear across every part of the exam and daily practice. In fracture clinic and fracture liaison services they are the backbone of secondary prevention after a fragility fracture. In basic-science vivas the mevalonate-pathway mechanism is a classic ask. In trauma and arthroplasty the recognition and management of atypical femoral fractures, and the dental implications of osteonecrosis of the jaw, are common scenarios. Knowing when to start, when to pause (drug holiday), and what to warn patients about is the practical core that examiners probe.
Guidelines, Registries and Global Practice
- Osteoporosis guidelines (for example AAOS/AOA bone-health initiatives, NICE/NOGG in the UK, and endocrine society guidance) consistently place bisphosphonates as first-line pharmacological therapy for fracture prevention, with intravenous zoledronate favoured where oral agents are not tolerated or adherence is poor.
- Fracture liaison services and bone-health programmes worldwide use bisphosphonates as the backbone of secondary fracture prevention after a fragility fracture.
- The drug holiday concept is endorsed across major guidelines as a way to balance long-term fracture benefit against the duration-dependent risks of AFF and MRONJ, with high-risk patients continued on therapy.
- MRONJ guidance (AAOMS position paper) standardises the definition, staging, and the emphasis on pre-treatment dental optimisation across settings.
Memory aids
GROANBisphosphonate Complications
Hook:Patients GROAN about bisphosphonates - GI, Renal, Osteonecrosis of jaw, Atypical fracture, Need calcium check.
STAMPAtypical Femoral Fracture Features
Hook:STAMP out atypical fractures - thigh pain plus a transverse subtrochanteric line with lateral beaking means image both femurs.
WAVESafe Oral Dosing
Hook:Ride the WAVE - Water, After waking, Vertical, Everything else waits.

Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman with postmenopausal osteoporosis is started on weekly alendronate. The examiner asks you to explain how it works and what you would check and counsel before prescribing.”
“A 74-year-old woman on alendronate for 8 years reports several weeks of dull right thigh pain with no injury. She is still walking but the pain is worse on weight-bearing. How do you proceed?”
Mechanism
- Pyrophosphate analogues - bind hydroxyapatite, taken up by osteoclasts
- Nitrogen-containing: inhibit farnesyl pyrophosphate synthase (mevalonate pathway)
- Non-nitrogen: form toxic ATP analogues
- Net effect: less resorption, higher bone mineral density
Key Efficacy
- Zoledronic acid: vertebral fracture down about 70 percent, hip about 41 percent
- Alendronate: guideline-standard oral first-line agent
- First-line for osteoporosis fracture prevention
Before Prescribing
- Correct calcium and vitamin D
- Check renal function - avoid zoledronate if eGFR less than 35
- Oral: empty stomach, full glass of water, upright 30 to 60 minutes
- Arrange dental review where feasible
Red Flags
- Thigh pain on long-term therapy - image both femurs for AFF
- Exposed jaw bone for more than 8 weeks - MRONJ
- First IV dose flu-like acute phase reaction
- Reassess for a drug holiday at 3 to 5 years
Evidence for Fracture Prevention
Once-Yearly Zoledronic Acid Reduces Fractures (HORIZON-PFT)
- Double-blind RCT, 7765 postmenopausal women, annual 5mg zoledronic acid infusion vs placebo over 3 years
- Morphometric vertebral fracture reduced by about 70 percent (3.3 vs 10.9 percent)
- Hip fracture reduced by about 41 percent (1.4 vs 2.5 percent)
- Serious atrial fibrillation occurred more often with zoledronic acid (50 vs 20 patients)
Alendronate as the Standard Active Comparator (ARCH)
- RCT in 4093 high-risk postmenopausal women using oral alendronate 70mg weekly as the active comparator
- Confirms alendronate as an effective, guideline-standard anti-resorptive for fracture prevention
- Romosozumab followed by alendronate lowered new vertebral fracture by 48 percent versus alendronate alone
- Adjudicated osteonecrosis of the jaw and atypical femoral fracture were rare events in both arms