Teriparatide
Teriparatide is recombinant human parathyroid hormone, the 1-34 fragment - the active N-terminal portion of the 84-amino-acid hormone. It is given as a once-daily subcutaneous injection. This is the textbook definition examiners want first.
It is the main anabolic osteoporosis drug: intermittent PTH stimulates osteoblasts, increasing bone formation more than resorption, so bone mass and architecture improve. Contrast this directly with bisphosphonates, which are anti-resorptive.
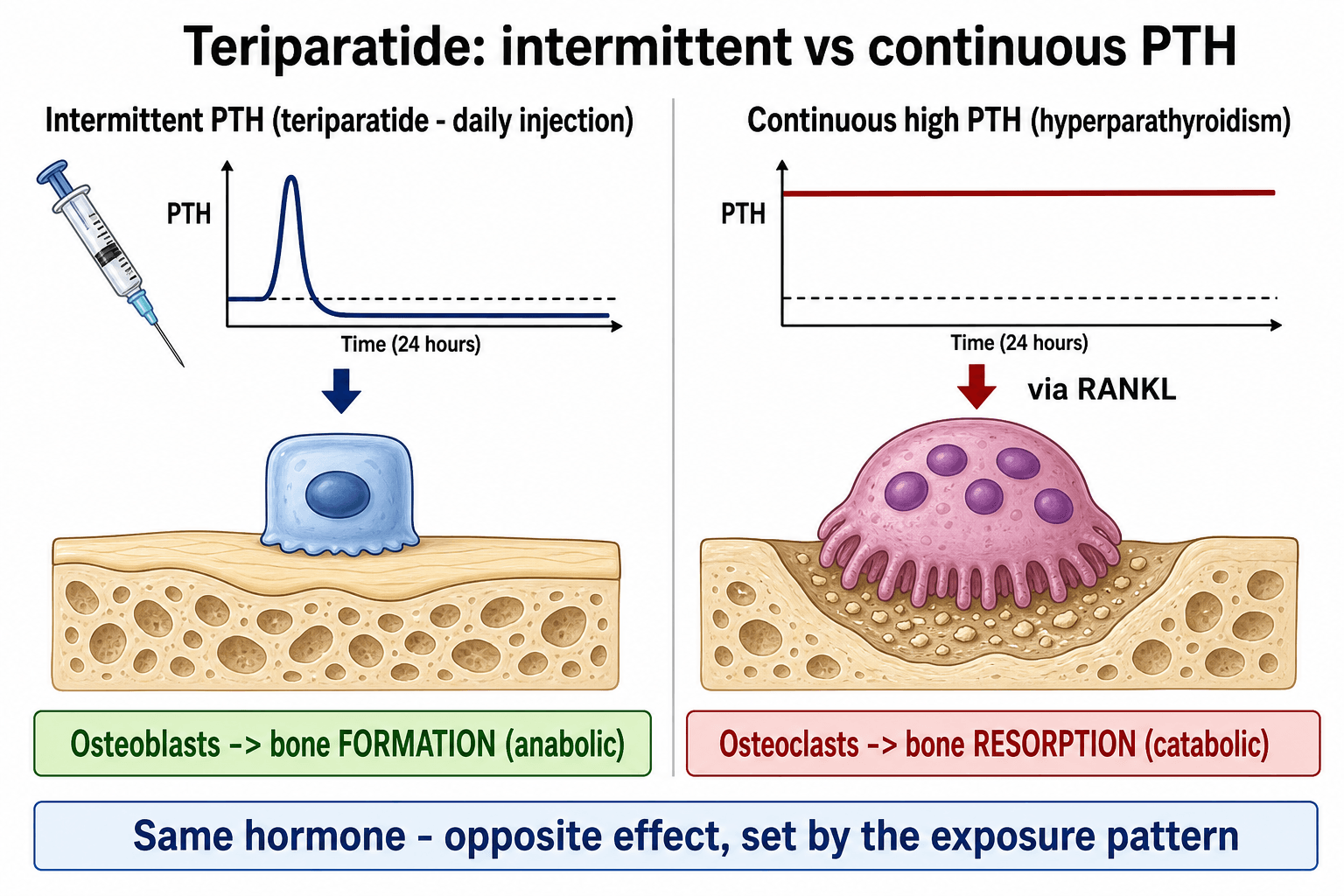
The paradox: brief daily pulses build bone, but continuously raised PTH (as in primary hyperparathyroidism) destroys bone. The same molecule has opposite effects depending on the exposure pattern - a classic viva trap.
Capped at 24 months lifetime with a historical osteosarcoma signal in rats. The gains are temporary, so always follow with an anti-resorptive (bisphosphonate or denosumab) to preserve the new bone.
Overview
Teriparatide is the first and best-known anabolic (bone-building) drug for osteoporosis. Almost every other osteoporosis treatment is anti-resorptive - it slows the cells that break bone down. Teriparatide does the opposite: it switches on the cells that build bone up, so it can rebuild a depleted skeleton rather than simply preserving what remains.
Chemically it is recombinant human parathyroid hormone (PTH) 1-34 - the first 34 amino acids of natural PTH, which is the part that carries the hormone's activity. It is given as a once-daily subcutaneous injection for a limited period.
For the exam, three threads recur throughout this topic: how an anabolic drug differs from the anti-resorptives you already know, the intermittent-versus-continuous PTH paradox that explains why it works, and how it is used in practice - who gets it, the evidence behind it, the 24-month limit, and the essential follow-on with an anti-resorptive.
Principles: How Teriparatide Builds Bone
Parathyroid hormone is the body's main regulator of calcium. Its effect on the skeleton depends entirely on how the bone is exposed to it, and this is the single most important concept in the topic.
- Intermittent PTH (teriparatide)
- Brief daily pulse from one injection, then levels fall
- Continuous high PTH (e.g. hyperparathyroidism)
- Persistently elevated hormone all day
- Intermittent PTH (teriparatide)
- Favours osteoblast activity and survival - net formation
- Continuous high PTH (e.g. hyperparathyroidism)
- Drives osteoclast activity through RANKL - net resorption
- Intermittent PTH (teriparatide)
- Bone mass and architecture improve (anabolic)
- Continuous high PTH (e.g. hyperparathyroidism)
- Bone is lost, cortices thin (catabolic)
- Intermittent PTH (teriparatide)
- Once-daily teriparatide for osteoporosis
- Continuous high PTH (e.g. hyperparathyroidism)
- Primary hyperparathyroidism causing osteoporosis and brown tumours
What happens at the cell level with intermittent dosing:
- A daily injection produces a short spike of PTH that quickly clears.
- This brief pulse acts on osteoblasts (the bone-forming cells) through the PTH/PTHrP receptor, increasing their number and activity and reducing their programmed death.
- The result is a burst of new bone formation that outpaces resorption, so bone mass rises and trabecular architecture is rebuilt - genuinely new bone, not just preserved old bone.
- Because the level falls again between doses, the prolonged signal that would otherwise switch on osteoclasts (through RANKL on osteoblasts) is avoided.
By contrast, when PTH stays high all the time - as in primary hyperparathyroidism - the same receptor signalling sustains RANKL expression, osteoclasts dominate, and bone is steadily resorbed. Same hormone, opposite outcome, decided by the timing of exposure.
This anabolic action also explains the "anabolic window": bone formation rises immediately, while resorption catches up only later, so the early months of treatment give the greatest net gain. Starting with teriparatide before an anti-resorptive (rather than after) tends to make the most of that window.
The intermittent-versus-continuous paradox is really a pharmacokinetic story:
- Subcutaneous teriparatide is rapidly absorbed (peak at about 30 minutes) and rapidly cleared (plasma half-life roughly 1 hour) by hepatic and renal peptide degradation. So a single daily injection produces a brief pulse that has fallen back to baseline long before the next dose — that transient exposure is exactly what favours the osteoblastic/anabolic response and avoids the sustained RANKL-driven resorption of continuous PTH excess. The short half-life literally creates the pulse.
- The calcium physiology explains the transient post-dose hypercalcaemia. PTH increases distal-tubular calcium reabsorption and phosphate excretion (phosphaturia) in the kidney, stimulates renal 1-alpha-hydroxylase → calcitriol → increased gut calcium absorption, and mobilises calcium from bone. Each dose therefore causes a small, transient rise in serum calcium (peaking a few hours after injection and normalising by the next day) and mild hypercalciuria.
- Practical consequences: check baseline calcium and do not start in a hypercalcaemic patient; pre-existing hyperparathyroidism/hypercalcaemia is a contraindication; use caution with active urolithiasis; and it is generally avoided in severe renal impairment. No routine dose titration is needed otherwise.
The Drug in Practice
- Detail
- Recombinant human PTH 1-34
- Why it matters
- The active fragment of the natural hormone
- Detail
- 20 micrograms once daily, subcutaneous
- Why it matters
- Self-injected, usually into the thigh or abdomen
- Detail
- Maximum 24 months in a lifetime
- Why it matters
- Driven by the osteosarcoma signal and waning benefit
- Detail
- Anabolic (bone-building)
- Why it matters
- Opposite of the anti-resorptive bisphosphonates and denosumab
- Detail
- Follow with an anti-resorptive
- Why it matters
- New bone is lost without a follow-on agent
A closely related anabolic agent, abaloparatide, is a PTH-related protein analogue with a similar profile. Romosozumab (an anti-sclerostin antibody) is another bone-building option but works by a different mechanism. For the exam, teriparatide is the prototype anabolic drug and the one to discuss by default.
Indications
Teriparatide is reserved for severe or high-risk osteoporosis rather than first-line use, because of its cost, the daily injection, and the duration limit.
Postmenopausal women and men with very low bone density or multiple or recurrent fragility fractures, especially vertebral fractures - the group with the most to gain from rebuilding bone.
Patients who fracture or keep losing bone despite an anti-resorptive - switching to an anabolic agent that builds bone is a logical next step.
High-dose, long-term steroid users at high fracture risk, where teriparatide has shown strong bone-density gains compared with bisphosphonates.
Off-label interest in stalled or fragile fracture healing (for example certain osteoporotic pelvic or atypical femoral fractures and nonunions), supported by smaller studies rather than large trials.
Clinical Relevance
Teriparatide turns up across the exam and orthopaedic practice precisely because it is the odd one out. In basic-science vivas it is the go-to example of an anabolic drug and the home of the intermittent-versus-continuous PTH paradox - a favourite way to test whether a candidate truly understands bone biology rather than memorising drug names. In the fracture and metabolic-bone clinic it is the escalation option for severe osteoporosis and treatment failure, and it forces the candidate to discuss drug sequencing (build then preserve). In trauma, it appears in discussions of atypical femoral fractures and difficult or fragile fracture healing, where its bone-building action is attractive. Knowing what it is, why intermittent dosing matters, who to give it to, and what to do afterwards is the practical core examiners probe.
Safety, Limits and How It Compares
Lifelong use is not allowed. Treatment is capped at 24 months because high-dose lifelong teriparatide caused osteosarcoma in rats. Although this has not been borne out as a clinically meaningful risk in humans at therapeutic doses, the limit and the contraindications (Paget disease, prior skeletal radiotherapy, unexplained high alkaline phosphatase, open growth plates, bone metastases or skeletal malignancy) remain in force.
Common, usually minor side effects include nausea, headache, dizziness, leg cramps, and a transient small rise in serum calcium after each dose. Check that the patient is not hypercalcaemic before starting.
- Teriparatide
- Anabolic - builds bone
- Bisphosphonates
- Anti-resorptive - slows bone loss
- Teriparatide
- Stimulates osteoblasts
- Bisphosphonates
- Inhibits osteoclasts
- Teriparatide
- Daily subcutaneous injection
- Bisphosphonates
- Oral weekly or intravenous, intermittently
- Teriparatide
- Severe or high-risk osteoporosis, treatment failure
- Bisphosphonates
- First-line for most osteoporosis
- Teriparatide
- Gains lost unless followed by an anti-resorptive
- Bisphosphonates
- Effect persists for a time (drug stays bound to bone)
The sequence matters: build, then preserve. Use teriparatide to add bone, then switch to a bisphosphonate or denosumab to keep it. Stopping teriparatide and giving nothing lets the newly formed bone be resorbed - and stopping denosumab without a follow-on can cause rebound vertebral fractures, so never leave a high-risk patient on no treatment.
"Build then preserve" is the headline; the deeper, frequently-tested point is that the order and what comes before teriparatide change the result:
- A prior potent anti-resorptive blunts the early teriparatide response. Patients pre-treated with a long-acting bisphosphonate show an attenuated and delayed bone-density gain on teriparatide (especially at the hip), because the suppressed, low-turnover skeleton cannot mount the full anabolic burst. So in the treatment-naïve high-risk patient, an anabolic-first strategy captures the fullest response.
- Go anabolic FIRST, then anti-resorptive — not the reverse. Switching from denosumab to teriparatide can cause a transient or progressive loss of bone density (notably at the hip) in the first year (the DATA-Switch study), because the anabolic agent cannot immediately offset the high-turnover rebound after denosumab is withdrawn. Giving an anti-resorptive after teriparatide instead consolidates and adds to the gains.
- Combination can beat monotherapy. Teriparatide plus denosumab together (the DATA study) raised bone density more than either drug alone — an option in selected very-high-risk patients, though cost and injection burden keep it non-routine.
The rule: in the highest-risk patient, give the anabolic FIRST and then lock in with an anti-resorptive; do not expect an immediate gain when switching denosumab to teriparatide; and never leave a high-risk patient on no treatment.
Guidelines, Registries and Global Practice
- Major osteoporosis guidelines (for example the Endocrine Society, AACE, NOGG in the UK, and bone-health initiatives endorsed by AAOS/AOA) position teriparatide as a treatment for severe or very high fracture-risk osteoporosis and for patients who fracture or lose bone despite an anti-resorptive, rather than as a first-line agent.
- Anabolic-first sequencing is increasingly endorsed for the highest-risk patients (those with recent or multiple vertebral fractures), reflecting head-to-head trial evidence that anabolic therapy reduces vertebral fractures more than oral bisphosphonates in this group.
- Guidance consistently stresses the mandatory follow-on anti-resorptive after stopping teriparatide to preserve bone gained, and the 24-month lifetime limit.
- Global practice variation is driven mainly by cost and access - the daily injection and price mean teriparatide is reserved for selected high-risk patients in most health systems, while the underlying principles (build then preserve, reserve for severe disease) are consistent worldwide.
Memory aids
BUILDWhy Teriparatide Is Special
Hook:Teriparatide is here to BUILD - Bone-building, Use 24 months, Intermittent pulses, Lock in the gains, Daily injection.
PROUDWhen to Avoid Teriparatide
Hook:Do not be PROUD to prescribe it here - Paget, Radiotherapy, Open physes, Unexplained high ALP, Disease with hypercalcaemia or bone cancer.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 71-year-old woman with severe osteoporosis and two vertebral fractures is started on teriparatide after failing a bisphosphonate. The examiner asks what teriparatide is, how it works, and how it differs from the drug she was on.”
“A 68-year-old man has a new vertebral fracture and a very low bone density T-score despite two years of alendronate. The examiner asks how you would treat him and what cautions apply to teriparatide.”
What It Is
- Recombinant human PTH 1-34 (the active fragment)
- Anabolic - the bone-building osteoporosis drug
- 20 micrograms once daily, subcutaneous
- Opposite of anti-resorptive bisphosphonates
Mechanism
- Intermittent daily pulse stimulates osteoblasts - bone forms
- Continuous high PTH drives osteoclasts (RANKL) - bone lost
- Same hormone, opposite effect, set by exposure pattern
- Early 'anabolic window' gives the biggest net gain
Use and Evidence
- For severe or high-risk osteoporosis and treatment failure
- Neer 2001: new vertebral fractures cut by about two-thirds
- VERO 2018: beat risedronate for vertebral fracture in severe disease
- Some evidence for accelerating fragile fracture healing
Limits and Red Flags
- Maximum 24 months lifetime - osteosarcoma signal in rats
- Avoid: Paget, prior skeletal radiotherapy, high ALP, open physes, bone cancer
- Always follow with an anti-resorptive to preserve gains
- Minor: nausea, headache, leg cramps, transient calcium rise
Evidence Base
Every trial below has been checked against its source record in PubMed. Two landmark RCTs anchor the topic — Neer 2001 established that teriparatide reduces fractures, and VERO (Kendler) was the first head-to-head trial powered on incident fractures to show an anabolic beat an oral anti-resorptive. Wagner's small crossover RCT is the human signal behind its off-label fracture-healing interest.
Teriparatide Reduces Fractures - the Landmark Trial (Neer)
- Randomised trial of 1637 postmenopausal women with prior vertebral fractures, daily PTH 1-34 (20 or 40 micrograms) versus placebo over a median of 21 months
- New vertebral fractures fell from 14 percent on placebo to 5 percent on the 20 microgram dose (relative risk about 0.35)
- New non-vertebral fragility fractures roughly halved (relative risk about 0.47)
- Lumbar spine bone mineral density rose markedly; side effects were minor (occasional nausea and headache)
Teriparatide Beats Risedronate for Vertebral Fracture in Severe Osteoporosis (VERO)
- Double-blind, double-dummy RCT of 1360 postmenopausal women with severe osteoporosis (at least two moderate or one severe vertebral fracture), teriparatide versus risedronate over 24 months (680 per group)
- New vertebral fractures: 5.4 percent with teriparatide versus 12.0 percent with risedronate (risk ratio 0.44)
- Clinical fractures: 4.8 percent versus 9.8 percent (hazard ratio 0.48)
- The first head-to-head trial powered on incident fractures to favour an anabolic over an anti-resorptive agent
Teriparatide Accelerates New Bone Mineralisation (Distraction Osteogenesis RCT)
- Randomised crossover study of 16 patients during the consolidation phase after tibial bone segment transport (distraction osteogenesis)
- Eight weeks of daily subcutaneous teriparatide roughly doubled the rate of bone mineralisation of the regenerate compared with no treatment (ratio about 2.4)
- Adjusted analysis showed an additional bone mineral density gain attributable to teriparatide (about 0.19 g per square centimetre, p less than 0.001)
- Provides direct human evidence that teriparatide stimulates new bone formation in a healing setting