Bowler's Thumb and Beyond
Clinical Entities
Critical Must-Knows
- Bowler's Thumb (Jewell's Neuritis) is the most common form.
- It presents as a palpable, tender nodule on the ulnar side of the thumb (Neuroma-in-continuity).
- It is caused by the edge of the bowling ball hole compressing the nerve.
- Treatment is primarily non-operative: Protective shield (Thumb shell) and hole modification.
- Surgery (Neurolysis/Transposition) is reserved for severe failure and often has poor outcomes if activity continues.
- Neurectomy is a last resort.
Clinical Pearls
- "Do NOT biopsy the 'nodule' - it is the nerve itself (Neuroma-in-continuity/Fibrosis).
- "Cutting it out creates a stump neuroma which is worse.
- "The Ulnar digital nerve of the thumb is most vulnerable due to the grip pattern.
Clinical Imaging
Imaging Gallery




Digital Nerve Anatomy
Anatomical Overview
The Trap: The 'Tumor'
The Presentation
Palpable Mass Patients present with a firm, tender lump on the thumb. It feels like a cyst or tumor. WARNING: Do not excise it without thinking!
The Reality
It's the Nerve This is perineural fibrosis (Neuroma-in-continuity). Excising it causes permanent anesthesia and a painful stump neuroma. Diagnosis is clinical (Tinel's positive over the mass).
| Feature | Bowler's Thumb | Ganglion Cyst | Giant Cell Tumor |
|---|---|---|---|
| Pathology | Nerve Fibrosis | Mucinous Cyst | Synovial Tumor |
| Tenderness | Severe (Electric) | Mild/Ache | Mild |
| Tinel's | Positive +++ | Negative | Negative |
| Mobility | Mobile (Side-side) | Fixed to sheath | Fixed/Mobile |
| Transillumination | Negative | Positive | Negative |
BOWLBowler's Thumb Features
| B | Ball Caused by Bowling ball hole edge. |
| O | Out Ulnar side (Inner aspect of grip). |
| W | Welling Swelling (Nodule) is palpable. |
| L | Leave it Don't excise the nodule! |
| B | Ball Caused by Bowling ball hole edge. | W | Welling Swelling (Nodule) is palpable. |
| O | Out Ulnar side (Inner aspect of grip). | L | Leave it Don't excise the nodule! |
Hook:Don't cut the lump when you BOWL.
SPAREManagement
| S | Stop Stop bowling (temporarily). |
| P | Protect Protective shell/guard. |
| A | Alter Alter hole pitch/bevel. |
| R | Release Neurolysis (Rare). |
| E | Excision Neurectomy (Never first line). |
| S | Stop Stop bowling (temporarily). | R | Release Neurolysis (Rare). |
| P | Protect Protective shell/guard. | E | Excision Neurectomy (Never first line). |
| A | Alter Alter hole pitch/bevel. |
Hook:SPARE the nerve.
VDNDigital Nerve Anatomy
| V | Vary Variable branching. |
| D | Dorsal Dorsal branches supply nail bed. |
| N | Nerve Nerve is volar to the artery. |
| V | Vary Variable branching. |
| D | Dorsal Dorsal branches supply nail bed. |
| N | Nerve Nerve is volar to the artery. |
Hook:Nerve is Palmar (Volar) to Artery.
Overview
Definition
Digital Nerve Compression refers to the chronic irritation and subsequent fibrosis of a proper digital nerve due to repetitive external pressure. The classic example is "Bowler's Thumb" (Ulnar Digital Nerve of the Thumb).
The condition represents a "Neuroma-in-continuity", where the nerve fibers remain intact but are surrounded by dense scar tissue, creating a palpable and tender nodule.
Pathophysiology and Anatomy
Digital Nerve Anatomy
- Position: Volar to the digital artery.
- Thumb: The Ulnar Digital Nerve (UDN) is most prominent at the MP joint level.
- Blood Supply: Vasa nervorum. Check for digital ischemia (e.g. Hypothenar Hammer).
- Origin: The UDN of the thumb arises from the median nerve (via branches from the palmar digital nerve).
- Course: Runs along the ulnar border of the thumb from the MCP joint to the tip.
The nerve is tethered by Cleland's and Grayson's ligaments, preventing it from escaping pressure.
Classification Systems
Clinical Grading (Dobyns)
- Mild: Paresthesia with activity only. No palpable mass.
- Moderate: Persistent paresthesia. Small palpable mass. Tinel's positive.
- Severe: Constant pain at rest. Large mass. Measurable sensory deficit.
Progression depends on continued exposure. Early recognition allows conservative management.
Differential Diagnosis
| Condition | Features | Key Differentiator |
|---|---|---|
| Bowler's Thumb | Tender mass, Tinel's+++, Bowling history | Mobile mass ON the nerve |
| Ganglion Cyst | Cystic, transilluminates, painless | Arises from tendon sheath |
| GCTTS | Firm, slow-growing, painless | Fixed to flexor sheath |
| Schwannoma | Eccentric, mobile side-to-side only | MRI shows nerve origin |
| Trigger Finger | Snapping, nodule at A1 pulley | Tendon not nerve |
| De Quervain's | 1st compartment pain, Finkelstein + | Tendon not digital nerve |
Clinical Pearls for Differentiation
- Tinel's Test: The key discriminator. Positive only in nerve pathology.
- Transillumination: Positive in ganglion, negative in nerve tumor.
- Mobility: Nerve tumors move side-to-side only (Paul-McSweeney sign).
- Location: Ganglions arise from joints/sheaths, nerve tumors from the nerve.
Clinical Presentation
History Taking
- Pain Character: Localized, sharp, electric-like tenderness at the mass.
- Numbness: Distal to the compression site, often intermittent initially.
- Lump: "I have a bump on my thumb" - key presenting complaint.
- Activity: Specific question about hobbies (Bowling, tool use, music).
- Duration: How long? Chronic exposure (months to years) is typical.
- Aggravating Factors: Gripping, bowling, specific activities.
- Relieving Factors: Rest, avoiding the activity.
- Occupation: Manual workers, musicians, athletes.
- Previous Treatment: Splints, rest, medications tried.
Symptoms improve with rest but recur immediately with activity. The pattern of improvement with rest and recurrence with activity is pathognomonic.
Examination
Physical Examination
- Inspection: Callus may be present overlying the nerve. Look for skin changes.
- Palpation: Firm, rubbery, tender fusiform mass (2-3mm to 1cm).
- Tinel's: Strongly positive. "Zing" or electric sensation to the tip.
- Sensation: 2PD may be normal or reduced (greater than 6mm) in severe cases.
- Motor: Normal (Digital nerves are purely sensory).
- Provocative Tests: Pressure on mass reproduces symptoms.
- Allen's Test: Rule out vascular contribution (Hypothenar Hammer).
Always compare with the contralateral thumb for baseline.
Imaging and Electrodiagnostics
Ultrasound
- Finding: Hypoechoic swelling of the nerve. Loss of fascicular pattern.
- Comparison: Compare diameter with contralateral digit.
- Doppler: Hypervascularity suggests active inflammation.
- Cross-sectional area: Increased CSA at the site of compression.
- Mobility: Reduced nerve gliding on dynamic assessment.
Essential to distinguish from Ganglion. US is the first-line imaging modality.
Management Algorithm
The "Splint and Spare" Approach
- Modification: Change the grip. Increase bevel of the hole. Move trigger finger.
- Protection: Custom molded thermoplastic thumb shell ("Thimble").
- Rest: 3-6 months off bowling.
- Success: High (if compliant). Mass may persist but become painless.
Changing the mechanics of the grip is the most sustainable solution.
Surgical Technique
Neurolysis & Transposition
- Incision: Mid-lateral or zig-zag over the mass.
- Dissection: Identify nerve proximal and distal to mass.
- Release: Carefully dissect scar from epineurium (Magnification!).
- Transposition: Create a bed dorsal to the Adductor mechanism.
- Fat Graft: Consider wrapping with vein or fat to prevent adhesion.
This is technically demanding in the small space of the thumb.
Complications
- Recurrence: Scar tissue reforms. Pain returns.
- Hypersensitivity: Site remains tender.
- Numbness: From neurectomy or damage during neurolysis.
- Stump Neuroma: If neurectomy is done poorly (not buried).
- CRPS: Always a risk with digital nerve surgery.
Rehabilitation
- Splint: Protective dressing and light splint.
- Elevation: Reduce edema and swelling.
- Wound Care: Keep clean and dry.
- Exercises: Gentle AROM of uninvolved joints.
- Pain Control: Ice, NSAIDs as needed.
- Scar Massage: Key to preventing recurrence and adhesions.
- Nerve Gliding: Specific exercises to mobilize the nerve.
- Desensitization: Texture grading (silk to rough fabric).
- Activity: Return to light ADLs.
- Strengthening: Gradual grip strengthening.
No bowling or sport-specific activity for 3 months post-op.
- Sport-Specific: Gradual return to bowling with protection.
- Shell Fitting: Custom protective guard fabrication.
- Technique: Review and modify grip technique.
- Monitoring: Watch for symptom recurrence.
- Full Activity: By 12 weeks if asymptomatic.
Hand Therapy Principles
- Early Motion: Prevents adhesions around the nerve.
- Scar Management: Silicone sheets, massage, compression.
- Nerve Gliding: Differential gliding of nerve relative to surrounding tissues.
- Sensory Re-education: For persistent numbness after neurectomy.
- Activity Modification: Long-term changes to technique and equipment.
Prognosis
- Conservative: Excellent for symptom control. The nodule may not disappear but becomes painless.
- Surgical: Mixed results overall.
- Neurolysis: ~60-70% pain relief. High recurrence rate if activity continues.
- Transposition: Better long-term outcomes for athletes returning to sport.
- Neurectomy: 90% relief of pain, but 100% numbness. Definitive option.
- Career: Many professional bowlers use a protective shell permanently.
- Recurrence: High without behavior modification. Most important prognostic factor.
- Stump Neuroma: A risk of neurectomy if proximal end not properly buried.
- CRPS: A risk of any hand surgery, especially nerve procedures.
- Return to Sport: 4-6 weeks for conservative, 3-6 months for surgical.
Prognostic Factors
- Duration of Symptoms: Longer duration = worse prognosis.
- Severity of Fibrosis: Severe scarring (Stage 3) = worse surgical outcomes.
- Compliance: Continued activity without protection = guaranteed failure.
- Occupation/Sport: Professional bowlers may need to change technique or retire.
Evidence Base
Reading the evidence
Bowler's thumb has no randomised trials — the literature is case reports and small surgical series. The landmark descriptions and surgical principles below are the examinable evidence. All claims are verified against PubMed.
Original Description — Perineural Fibrosis
- Classic description establishing 'bowler's thumb' as perineural fibrosis of the digital nerve
- Localised to the ulnar digital nerve of the thumb in bowlers
- Defined the lesion as fibrosis, NOT a true tumour
- Recognised it as a chronic repetitive-trauma neuropathy
Two Lesion Types — MRI Differentiation
- Two surgically treated cases: nodular neuroma vs epineural mass
- MRI distinguished the two morphological types pre-operatively
- Surgical outcome in active bowlers remains unpredictable
- Post-operative protection from repetitive trauma is essential
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Lump
"A 30-year-old man presents with a painful lump on his thumb. He wants it cut out. He is a bowler."
Scenario 2: The Numb Tip
"A patient presents with a numb tip of the index finger after a long weekend of DIY using pliers."
Scenario 3: The Recurrent Pain
"A patient had a neurolysis for Bowler's thumb 6 months ago. The pain is back and worse. Tinel's is ++."
MCQ Practice Points
Pathology
Q: What is the pathological nature of the nodule in Bowler's Thumb? A: Neuroma-in-continuity (Perineural fibrosis).
Anatomy
Q: Which nerve is affected in Bowler's Thumb? A: The Ulnar Digital Nerve of the Thumb.
Management
Q: What is the preferred surgical treatment for recurrent Bowler's thumb if preservation is desired? A: Neurolysis and Transposition (deep to Adductor Pollicis).
Prognosis
Q: What is the consequence of excising the nodule? A: Permanent sensory loss and potential stump neuroma.
Eponymous Conditions
Q: Name specific digital nerve compression syndromes. A: Bowler's Thumb (ulnar digital nerve thumb), Trigger Thumb Digital Nerve (compression at A1 pulley), and Digital Nerve Compression in index finger (woodworking/tool use).
Guidelines, Registries & Global Practice
Why no formal guideline?
Digital nerve compression is too rare for any orthopaedic society (AAOS, BOA, AO, EFORT, ASSH, IFSSH) to publish a dedicated guideline or for any registry to track it. The "evidence" is consensus from hand-surgery texts and case series. Examiners therefore test reasoning, not a protocol — recognise the entity, avoid biopsy, exhaust pressure-relief before surgery.
Global Epidemiology
- Sport/recreation: Classically ten-pin bowling (the eponym); also reported with golf, cricket, racquet sports and rock climbing where grip concentrates pressure on a digital nerve.
- Occupational: Repetitive tool use (pliers, scissors, screwdrivers, secateurs) — radial digital nerve of the index finger is typical ("scissors palsy", gardener's/hedge-trimmer neuropathy).
- Musicians: String and harp players (radial digital nerve of index/long), flautists — a recognised performing-arts-medicine entity worldwide.
- Demographics: Predominantly middle-aged adults in high-repetition activities; true incidence is unknown because most cases are managed without referral.
How the Major Bodies Frame Management
| Theme | Consensus across hand-surgery sources (ASSH/IFSSH/BSSH texts, AO) |
|---|---|
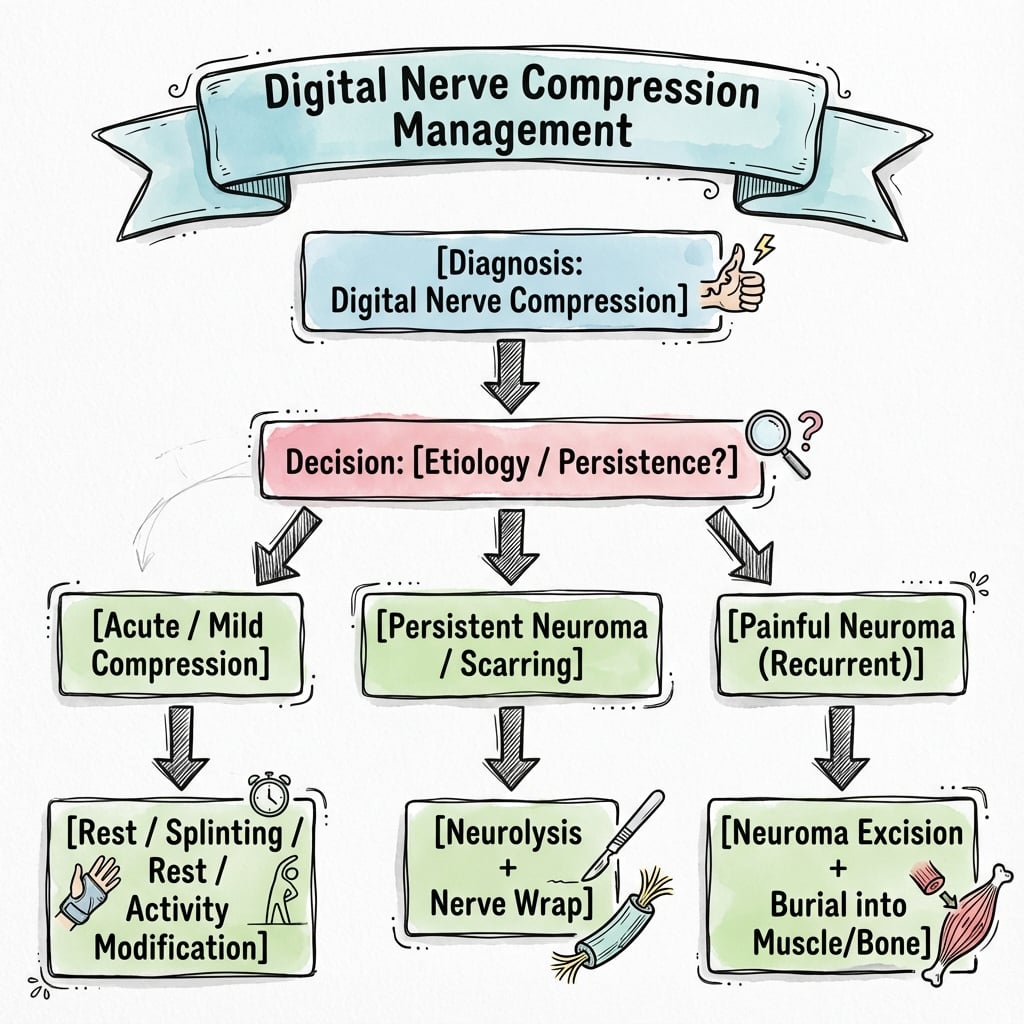
| Diagnosis | Clinical — tender mass + positive Tinel's; imaging (US first, MRI if uncertain) confirms and excludes mimics |
| First-line | Activity/equipment modification, pressure relief, protective rigid shell — uniformly recommended before any surgery |
| Biopsy | Avoid excisional biopsy of the "mass" (it is the nerve) — universal teaching |
| Nerve-preserving surgery | Neurolysis +/- transposition deep to adductor pollicis when conservative care fails |
| Salvage | Neurectomy with stump burial in muscle/bone, only after a diagnostic block confirms acceptable numbness |
There is no genuine inter-society disagreement here — the management ladder is consistent globally, which itself is an examinable point.
Practice Variation: High- vs Limited-Resource Settings
- High-resource: Ready access to high-resolution ultrasound and MRI, certified hand therapists for custom thermoplastic shells, and microsurgical neurolysis/transposition. Reconstruction options (processed nerve allograft, conduits) available if neurectomy gaps need bridging.
- Limited-resource: Diagnosis is clinical; the priority is the cheapest, highest-value intervention — modifying the offending activity/equipment and a simple protective splint, which resolves most cases. Imaging is reserved for atypical masses where malignancy must be excluded. Microsurgical transposition may be unavailable, making activity cessation the mainstay.
Controversies and Areas of Uncertainty
What is genuinely unsettled
The whole field rests on case reports — these are the honest grey areas an examiner may probe.
- Surgery vs prolonged conservative care: No comparative data. Many lesions become painless with pressure relief even though the nodule persists, so the threshold for operating is opinion-based.
- Neurolysis vs transposition: Simple neurolysis is criticised for re-scarring, and transposition deep to adductor pollicis is favoured by tradition (De Smet) — but no series compares them head-to-head. The role of nerve wraps to prevent re-fibrosis (Halsey) is unproven beyond case reports.
- Neurectomy vs nerve-preserving surgery: Neurectomy reliably abolishes pain but guarantees numbness; Dellon and Mackinnon showed digital sites have the worst outcomes after resection/burial, so it remains a last resort despite being "definitive".
- Reconstruct or accept numbness: If a neurectomy leaves a gap, the MATCH data favour allograft over conduit — but whether to reconstruct a single ulnar-digital-nerve of the thumb at all (versus simple burial) is unsettled given the limited functional cost.
- Return to the offending activity: Outcomes in athletes/musicians who continue the provoking activity are unpredictable; whether equipment modification alone allows durable return is not established by any controlled study.
Clinical summary
Diagnosis
- •Palpable painful nodule
- •Ulnar side of thumb
- •Tinel's Positive
- •History of Bowling/Tools
Anatomy
- •Ulnar Digital Nerve (Thumb = Bowler's thumb)
- •Tethered by Cleland/Grayson ligaments
- •Compressed against phalanx bone
- •Nerve courses volar to artery in digits
- •Fixed position makes it vulnerable to repetitive trauma
Treatment
- •1. Stop activity
- •2. Protective Shell/Guard
- •3. Neurolysis + Transposition
- •4. Neurectomy (Salvage)