Most Common Fracture | Volar Plate | Restore Alignment | Watch for Instability
- Normal radiographic parameters: Volar tilt 11-15°, radial inclination 22°, radial length 11-12mm
- Instability criteria: Over 20° dorsal tilt, over 5mm shortening, intra-articular involvement
- Volar locking plate is gold standard for unstable fractures
- Median nerve at risk - monitor for acute carpal tunnel
- EPL rupture late complication - avoid prominent dorsal hardware
- “DRUJ stability crucial - assess after fracture fixation
- “Volar Barton = shear fracture, needs buttress plate
- “Die-punch = lunate facet, associated with DRUJ injury
- “Elderly osteoporotic - consider augmentation techniques
Know the normal values: Volar tilt 11-15°, Radial inclination 22°, Radial length 11-12mm, Ulnar variance neutral. Loss of these = instability.
Median nerve symptoms require urgent attention. If present with swollen wrist and severe pain, consider emergent carpal tunnel release with fracture fixation.
Test DRUJ stability after every fixation. Unstable DRUJ may indicate TFCC or ulnar styloid base fracture. May need separate treatment.
Late complication (weeks post-injury). Occurs from Lister's tubercle irritation. Avoid prominent dorsal hardware. Treat with EIP-to-EPL transfer.
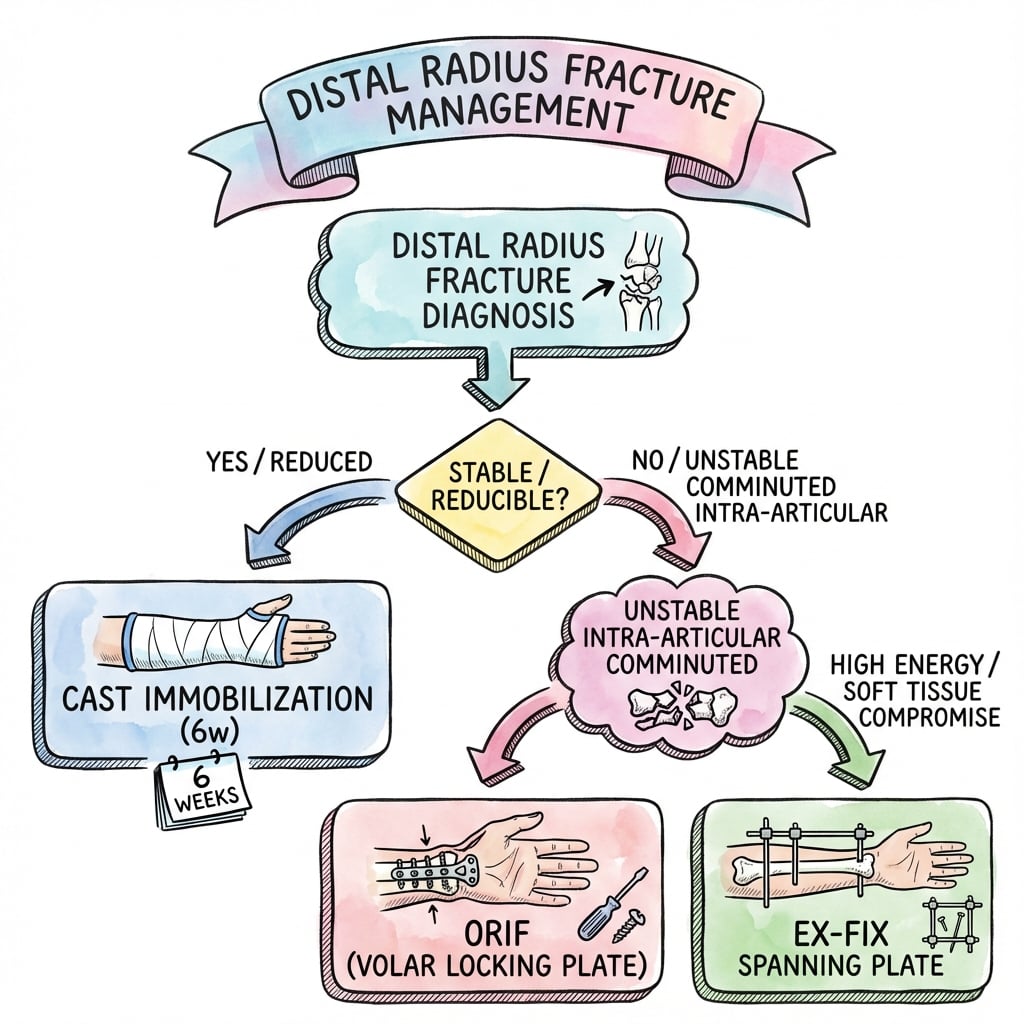
- Stable?
- Yes
- Treatment
- Cast immobilization 6 weeks
- Stable?
- No
- Treatment
- Volar locking plate
- Stable?
- No
- Treatment
- ORIF - restore articular surface
- Stable?
- No
- Treatment
- Volar buttress plate
- Stable?
- No
- Treatment
- Volar plate (buttress mode)
- Stable?
- No
- Treatment
- ORIF, elevate fragment, check DRUJ
- Stable?
- Emergency
- Treatment
- Urgent debridement, fasciotomy, fixation
RADIUSInstability Criteria
Hook:RADIUS fracture instability - if any of these, consider fixation!
VRIRadiographic Parameters
Hook:VRI - Volar tilt, Radial inclination, Index (length)!
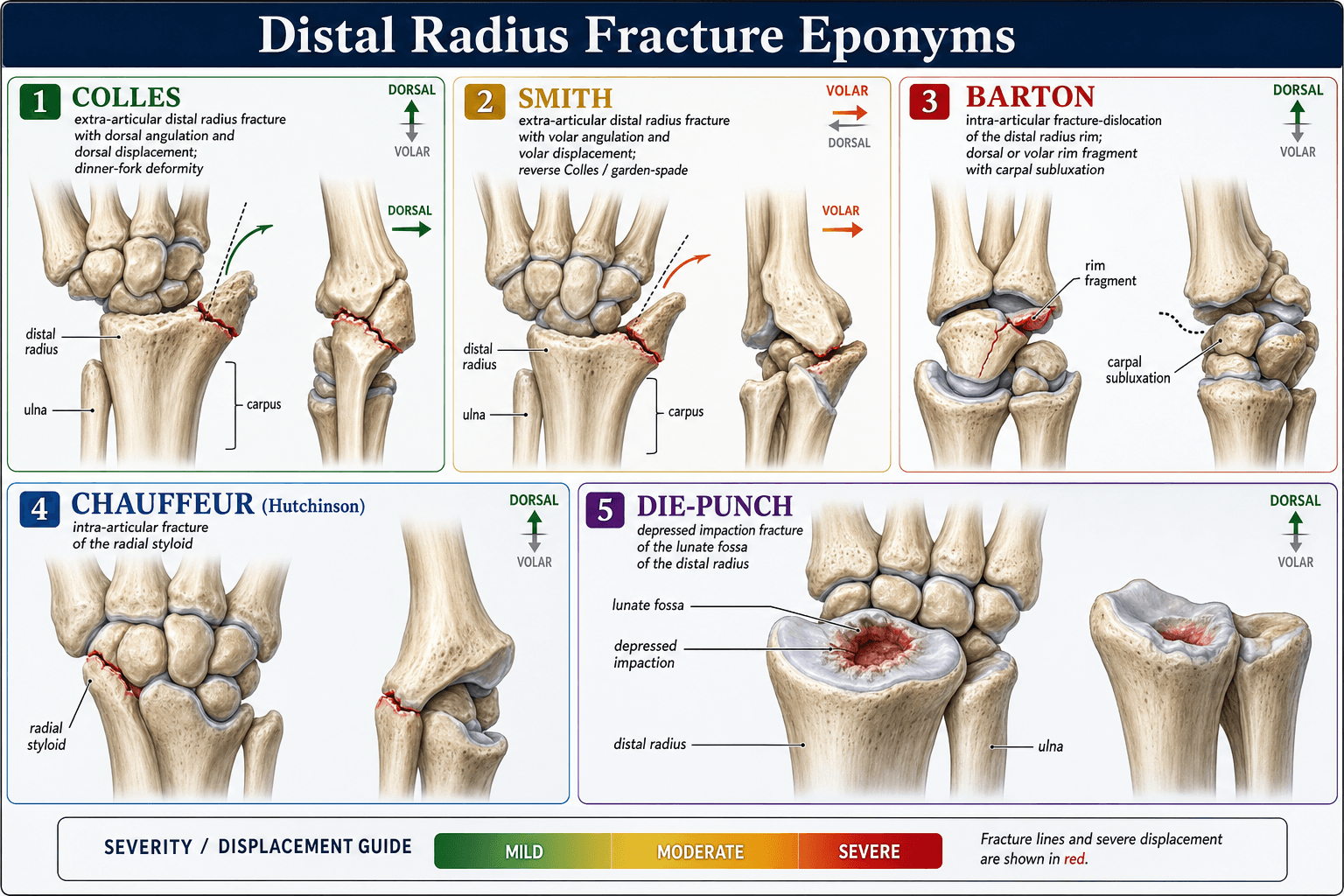
COLLESFracture Types
Hook:Remember COLLES and its variations for exam classification questions!
COMPLEXComplications
Hook:COMPLEX complications - watch for all of these post-DRF!
Overview and Epidemiology
Demographics
- Young adults: High-energy trauma (sports, MVA)
- Elderly (over 50): Low-energy falls (osteoporotic)
- Most common fracture treated by orthopaedic surgeons
- Over 640,000 annually in USA
- Peak incidence: 60-69 years in women
- Increasing with aging population
These demographic patterns inform screening and prevention strategies.
Anatomy
Distal Radius Anatomy
- Scaphoid fossa: Articulates with scaphoid
- Lunate fossa: Articulates with lunate
- Sigmoid notch: Articulates with ulna (DRUJ)
- Lister's tubercle: Dorsal prominence, EPL passes around it
- Radial styloid: Most radial projection
- Radiocarpal joint (scaphoid, lunate)
- DRUJ (distal radioulnar joint)
- Both must be addressed in treatment
Anatomic restoration of these articulations is essential for optimal function.
Classification
Historic Classifications
- Description
- Dorsal angulation, extra-articular
- Key Feature
- Dinner fork deformity
- Description
- Volar angulation (reverse Colles)
- Key Feature
- Garden spade deformity
- Description
- Volar lip with carpal subluxation
- Key Feature
- Shear mechanism
- Description
- Dorsal lip with carpal subluxation
- Key Feature
- Less common
- Description
- Radial styloid fracture
- Key Feature
- Intra-articular, ligament avulsion
- Description
- Lunate facet depression
- Key Feature
- Associated DRUJ injury
History
History Taking
- FOOSH (fall on outstretched hand) - classic
- High-energy vs low-energy
- Hand position at impact (extension vs flexion)
- Pain and swelling
- Deformity (dinner fork)
- Numbness (median nerve)
- Weakness
- Age and hand dominance
- Occupation and hobbies
- Functional demands
- Osteoporosis history
Patient factors strongly influence treatment decisions.
Examination
Physical Examination
- Deformity (dorsal dinner fork, volar garden spade)
- Swelling extent
- Skin integrity (open fracture?)
- Ecchymosis
- Point tenderness at fracture site
- Carpal bones (scaphoid especially)
- DRUJ (tenderness = injury)
- Ulnar styloid
- Median nerve (thenar sensation, thumb opposition)
- Ulnar nerve (small finger sensation, interossei)
- Radial artery pulse
- Capillary refill
Document neurovascular status before and after any reduction attempt.
Differential Diagnosis
A painful, swollen wrist after a fall is not always a distal radius fracture. Consider these mimics, which change management.
- Key Distinguishing Feature
- Anatomical snuffbox and scaphoid tubercle tenderness; may be radiographically occult
- Why It Matters
- Missed fracture risks non-union and AVN; needs dedicated views or MRI
- Key Distinguishing Feature
- Disrupted carpal arcs and 'spilled teacup' on lateral; high-energy mechanism
- Why It Matters
- Surgical emergency; commonly missed on initial films
- Key Distinguishing Feature
- Salter-Harris pattern at the open physis
- Why It Matters
- Growth-arrest risk; different management from the adult fracture
- Key Distinguishing Feature
- Radial shaft fracture with DRUJ disruption
- Why It Matters
- DRUJ must be addressed; not an isolated wrist injury
- Key Distinguishing Feature
- Ulnar-sided pain, DRUJ instability, normal radius
- Why It Matters
- Stability and TFCC, not bone, drive treatment
- Key Distinguishing Feature
- No fracture line, focal soft-tissue tenderness
- Why It Matters
- Diagnosis of exclusion after occult fracture ruled out
Investigations
Standard Radiographs
- PA (posteroanterior) wrist
- True lateral wrist
- Oblique views if needed
- Volar tilt (lateral view)
- Radial inclination (PA view)
- Radial length/ulnar variance (PA view)
- Articular step-off
- DRUJ congruity
Standard radiographs are sufficient for most treatment decisions.




Management
The named, examinable rule for predicting that a fracture will redisplace after a closed reduction is the Lafontaine classification of instability - quote it by name:
- Five Lafontaine risk factors: (1) initial dorsal angulation greater than 20 degrees; (2) dorsal metaphyseal comminution; (3) intra-articular involvement (radiocarpal); (4) associated ulnar (styloid) fracture; (5) age over 60 years.
- The rule: the presence of three or more of these factors predicts secondary displacement / loss of reduction in a cast, and should prompt closer surveillance or a lower threshold for primary surgical fixation.
- How it relates to the RADIUS mnemonic above: the in-house RADIUS list is essentially the Lafontaine factors; the exam expects the eponym - "this fracture has [X] Lafontaine criteria, so it is at high risk of redisplacement."
Exam point: Lafontaine = dorsal tilt over 20 degrees + dorsal comminution + intra-articular + ulnar fracture + age over 60; three or more predicts cast failure and supports operative fixation.
Conservative Treatment
- Stable, minimally displaced fractures
- Acceptable alignment (see criteria below)
- Low functional demand patients
- Contraindications to surgery
- Volar tilt loss under 10° (slight dorsal tilt OK)
- Radial shortening under 3mm
- Radial inclination loss under 5°
- No articular step over 2mm
- Congruent DRUJ
- Closed reduction under hematoma block
- Below-elbow cast or sugar-tong splint
- 6 weeks immobilization
- Weekly X-rays for first 2-3 weeks
Close follow-up is essential to detect loss of reduction early.
Surgical Technique
Volar Locking Plate - Standard Approach
FCR (Flexocarpal Radialis) Approach:
Step-by-Step Technique
5-6cm longitudinal incision along FCR tendon. Retract FCR ulnarly, flexor pollicis longus radially. Incise pronator quadratus in L-shape at radial border and elevate subperiosteally ulnarly to expose fracture site.
Clear fracture site of hematoma. Use ligamentotaxis by longitudinal traction. Reduce volar tilt using freer elevator or bone tamp to elevate dorsal cortex. Provisional K-wire fixation to hold reduction. Check on C-arm PA and lateral.
Position volar locking plate on volar surface. Plate must be proximal to watershed line (volar lip of radius). Insert proximal cortical screw first to attach plate. Check alignment. Insert distal locking screws - aim for subchondral bone.
Critical views: PA - screws not in joint, radial inclination restored. Lateral - volar tilt restored, screws not beyond dorsal cortex. Skyline view (20° tilted lateral) - confirm no dorsal screw prominence.
The volar approach provides excellent exposure while protecting critical dorsal structures.
Complications
Early Complications
- Median nerve compression from swelling/hematoma
- May occur at presentation or post-reduction
- Urgent release if progressive
- Forearm compartments at risk
- Monitor closely post-injury
- Fasciotomy if diagnosed
- Common in unstable patterns
- Weekly X-rays important
- May need operative stabilization
Early recognition allows timely intervention.
A specific, examinable late consequence of a malunited distal radius fracture is ulnar impaction (ulnocarpal abutment) syndrome - distinct from DRUJ instability:
- The mechanism: radial shortening (and loss of radial inclination) leaves the ulna relatively long - positive ulnar variance - so the ulnar head abuts and overloads the ulnar carpus (lunate and triquetrum) and the TFCC.
- The presentation: ulnar-sided wrist pain, worse with gripping and ulnar deviation/pronation; X-rays show positive ulnar variance with cystic/sclerotic change in the ulnar lunate and ulnar head; MRI shows TFCC wear and lunate oedema (the Palmer degenerative TFCC spectrum).
- The management: address the variance - a distal radius corrective osteotomy (to re-lengthen the radius) when the malunion is the driver, or an ulnar-shortening osteotomy (or arthroscopic wafer procedure) to offload the ulnocarpal joint; TFCC debridement as an adjunct.
- The prevention message: this is exactly why restoring radial length at the index operation matters - tolerating shortening to "save an operation" can convert a healed fracture into a painful ulnocarpal abutment.
Exam point: ulnar-sided wrist pain after a healed but shortened distal radius fracture = ulnar impaction from relative positive ulnar variance - treat by correcting the variance (radial corrective or ulnar-shortening osteotomy).
Postoperative Care
First 2 Weeks
- Volar splint in neutral position
- Elevation to reduce swelling
- Ice application
- Finger ROM exercises (immediate)
- Check dressing at 2-3 days
- Suture removal at 10-14 days
- Monitor for infection signs
- No lifting with affected hand
- Active finger exercises hourly
- Shoulder and elbow ROM to prevent stiffness
Early finger movement is essential to prevent stiffness.
Outcomes and Prognosis
Expected Outcomes
- Conservative
- 95%
- Volar Plate
- 98%
- Conservative
- Variable
- Volar Plate
- 85-90% of normal
- Conservative
- 8-12 weeks
- Volar Plate
- 6-8 weeks
- Conservative
- Higher malunion
- Volar Plate
- Hardware related
- Conservative
- Good (stable)
- Volar Plate
- Excellent
Prognostic Factors
- Extra-articular fracture
- Anatomic reduction achieved
- Young patient with good bone
- Stable pattern
- Compliant with therapy
- Intra-articular comminution
- Articular step over 2mm
- Osteoporotic bone
- Malunion
- Associated DRUJ injury
Guidelines, Registries & Global Practice
Global Epidemiology
The distal radius is among the most commonly fractured bones worldwide, with a bimodal age distribution: a peak in children and adolescents from sport and play, and a second osteoporotic peak in older adults (predominantly women). Population data over the past 40 years show a rising prevalence in both the paediatric and elderly groups, driven by ageing populations and activity patterns. [Nellans, Hand Clin 2012, PMID 22554654]
Major Guidelines Side by Side
- Core Recommendation
- Operative fixation suggested when post-reduction radial shortening over 3mm, dorsal tilt over 10°, or intra-articular step/gap over 2mm; rigid immobilisation if non-operative; supplemental vitamin C does not reliably prevent CRPS
- Evidence Basis
- Multiple RCTs; many recommendations limited/moderate strength
- Core Recommendation
- Manipulate displaced fractures promptly; offer surgery only if alignment unacceptable after reduction; K-wire or plate both acceptable; rehabilitation without routine formal physiotherapy for most
- Evidence Basis
- Informed by DRAFFT and DRAFFT2 RCTs
- Core Recommendation
- Classify by 2R3 (AO/OTA); reduction and stable fixation to restore articular congruity and alignment; volar locking plate as workhorse for unstable patterns
- Evidence Basis
- Expert consensus + comparative trials
- Core Recommendation
- Individualise by fracture pattern, bone quality and patient demand; anatomical reduction less critical in low-demand elderly
- Evidence Basis
- Arora RCT and pooled data
Registry & Trial Evidence
- Best Evidence
- Arora RCT (PMID 22159849)
- Bottom Line
- No functional difference at 12 months; more complications with surgery
- Best Evidence
- DRAFFT RCT (PMID 25716883)
- Bottom Line
- Equivalent PRWE; K-wire cheaper
- Best Evidence
- DRAFFT2 RCT (PMID 35045969)
- Bottom Line
- Equivalent at 1 year, but 13% of casts redisplace and need surgery
- Best Evidence
- Williksen RCT (PMID 23890493)
- Bottom Line
- Plate better for C2/C3 patterns; similar complication rates
Practice Variation
Management genuinely differs by region and resource setting. In high-resource systems, volar locking plate use has risen steeply over two decades despite trial data showing no consistent functional advantage over cast or K-wires in older patients. In limited-resource settings, closed reduction and casting or K-wire fixation remain mainstays because they are effective and low cost. Day-case surgery and wide-awake local anaesthetic no tourniquet (WALANT) technique are expanding internationally as cost-conscious options. The recurring exam message is that radiographic restoration does not equal functional benefit in the low-demand elderly.
- Document neurovascular status before and after reduction
- Explain that anatomy may not equal function in older patients
- Consent for CRPS, stiffness and need for therapy
- Warn about EPL rupture even after minor fractures
- Infection, nerve injury, tendon irritation/rupture
- Hardware removal possibility
- Loss of reduction if treated in cast
- Stiffness requiring hand therapy
MCQ Practice Points
Q: What are the normal radiographic parameters of the distal radius?
A: VRI - Volar tilt 11-15°, Radial inclination 22° (15-25°), radial length (Index) 11-12mm. Ulnar variance should be neutral.
Q: What parameters indicate an unstable distal radius fracture?
A: RADIUS - Radial shortening over 5mm, Angulation over 20°, Dorsal comminution, Intra-articular step over 2mm, Ulnar fracture, Sixty and older.
Q: What is a volar Barton fracture and how is it treated?
A: A shear fracture of the volar lip of the distal radius with carpal subluxation. Treated with volar buttress plate - the plate prevents the fragment (and carpus) from displacing.
Q: A patient presents 5 weeks after distal radius fracture unable to extend their thumb IP joint. What is the diagnosis and treatment?
A: EPL rupture from attritional wear at Lister's tubercle. Treatment is EIP-to-EPL tendon transfer.
Q: What structures stabilize the DRUJ and how is stability assessed?
A: Primary stabilizer is the TFCC. Assess by stabilizing the radius and translating the ulna dorsally and volarly. Compare to opposite side. Increased translation = instability.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman fell on her outstretched hand. X-rays show a dorsally angulated distal radius fracture with 20° dorsal tilt, 4mm shortening, and no intra-articular extension. She is otherwise healthy and lives independently.”
“A 45-year-old male motorcyclist has a distal radius fracture with volar rim involvement. The X-ray shows the carpus subluxed volarly with the volar rim fragment.”
“A 58-year-old woman had a minimally displaced distal radius fracture treated in cast 6 weeks ago. She now presents unable to extend her thumb at the IP joint. The fracture has healed.”
Normal Parameters (VRI)
- Volar tilt: 11-15°
- Radial inclination: 22° (15-25°)
- Radial length: 11-12mm
- Ulnar variance: Neutral
Instability Criteria (RADIUS)
- Radial shortening over 5mm
- Angulation over 20°
- Dorsal comminution
- Intra-articular step over 2mm
- Ulnar fracture
- Sixty and older
Fracture Types
- Colles: Dorsal angulation (dinner fork)
- Smith: Volar angulation (reverse Colles)
- Barton: Rim fracture + carpal subluxation
- Die-punch: Lunate facet depression
- Chauffeur: Radial styloid
Treatment Principles
- Stable, aligned: Cast 6 weeks
- Unstable: Volar locking plate
- Barton: Buttress plate
- Check DRUJ after fixation
Key Complications
- Acute carpal tunnel: Urgent release
- EPL rupture: EIP transfer
- Malunion: Corrective osteotomy
- CRPS: Early therapy
DRUJ Assessment
- Always test after fixation
- Compare translation to opposite side
- TFCC is primary stabilizer
- Ulnar styloid base fracture = instability marker
Evidence Base
K-wires vs Volar Locking Plate (DRAFFT Trial)
- Multicentre RCT of 461 adults with a dorsally displaced distal radius fracture requiring surgery. No clinically relevant difference in PRWE score at 12 months between percutaneous K-wire fixation and volar locking-plate fixation (difference -1.3, 95% CI -4.5 to 1.8). K-wire fixation was cheaper and quicker.
Volar Locking Plate vs Cast in the Elderly (Arora RCT)
- 73 patients aged 65 or older with displaced, unstable fractures randomised to volar locking plate or cast. No difference in PRWE, DASH, range of motion or pain at 12 months despite better radiographic alignment with plating. Grip strength was better with plating but complications were significantly higher in the operative group (13 vs 5).
Cast vs K-wire Fixation (DRAFFT2 Trial)
- 500 adults with a manipulated dorsally displaced distal radius fracture randomised to moulded cast or K-wire fixation. No difference in PRWE at 12 months (mean difference -0.34, 95% CI -4.33 to 3.66). However, 13% of the cast group required surgery for loss of position within six weeks versus less than 1% of the K-wire group.
Articular Step-off and Osteoarthritis (Knirk & Jupiter)
- 43 intra-articular fractures in 40 young adults (mean age 27.6). Post-traumatic arthritis developed in 91% of joints that healed with residual radiocarpal incongruity versus 11% of congruous joints. Accurate articular restoration was the single most critical factor in outcome.
External Fixation vs Volar Plate (Williksen RCT)
- 111 unstable fractures randomised to external fixation with adjuvant pins or volar locking plate. No significant difference in QuickDASH at one year, but plating gave a higher Mayo wrist score (90 vs 85), better supination and less radial shortening; the advantage was greatest for AO type C2/C3 patterns. Complication rates were similar (29% vs 30%).
EPL Rupture After Distal Radius Fracture
- EPL rupture is a recognised delayed complication of distal radius fracture with reported incidence ranging from 0.07% to 5%, more commonly seen in adults after nondisplaced fractures (attritional rupture at Lister's tubercle) than displaced ones.
Associated Intra-articular Soft-tissue Lesions (Lindau)
- Arthroscopy of 50 displaced fractures in young adults found TFCC tears in 78% (correlated with ulnar styloid fractures), scapholunate ligament tears in 54% and chondral lesions in 32%. Associated soft-tissue injury may explain poor outcomes after radiographically well-healed fractures.