Benign Intramedullary Cartilage Tumor | Most Common Hand Tumor | Malignant Transformation Risk
DISTRIBUTION TYPES
Critical Must-Knows
- Most common tumor of hand bones - 90% in phalanges and metacarpals
- Lobulated hyaline cartilage with calcifications creating rings-and-arcs pattern on X-ray
- Solitary lesions have 1-2% malignant transformation; Ollier/Maffucci 25-30%
- Pathological fracture through enchondroma is common presentation in hand
- Pain in absence of fracture suggests malignant transformation to chondrosarcoma
Clinical Pearls
- "Key differentiator: asymptomatic enchondroma vs painful chondrosarcoma
- "Rings-and-arcs calcification pattern pathognomonic for cartilage tumors
- "Ollier disease shows unilateral distribution; if bilateral consider Maffucci syndrome
- "Treatment of hand enchondroma: curettage and bone grafting after pathological fracture
Clinical Imaging
Imaging Gallery

Critical Enchondroma Exam Points
Malignant Transformation
Pain without trauma in known enchondroma suggests transformation to chondrosarcoma. Solitary lesions 1-2% risk; Ollier disease 25-30%; Maffucci syndrome up to 100% lifetime risk. MRI shows cartilage cap greater than 2cm and irregular enhancement.
Location Significance
Hand enchondromas are common and benign (50% of hand tumors). Axial or proximal long bone enchondromas have higher malignant potential and require closer surveillance with MRI.
Imaging Diagnosis
Rings-and-arcs calcification on X-ray is pathognomonic. Central medullary location. May cause endosteal scalloping (less than 2/3 cortical thickness is benign). No periosteal reaction unless pathological fracture.
Management Principles
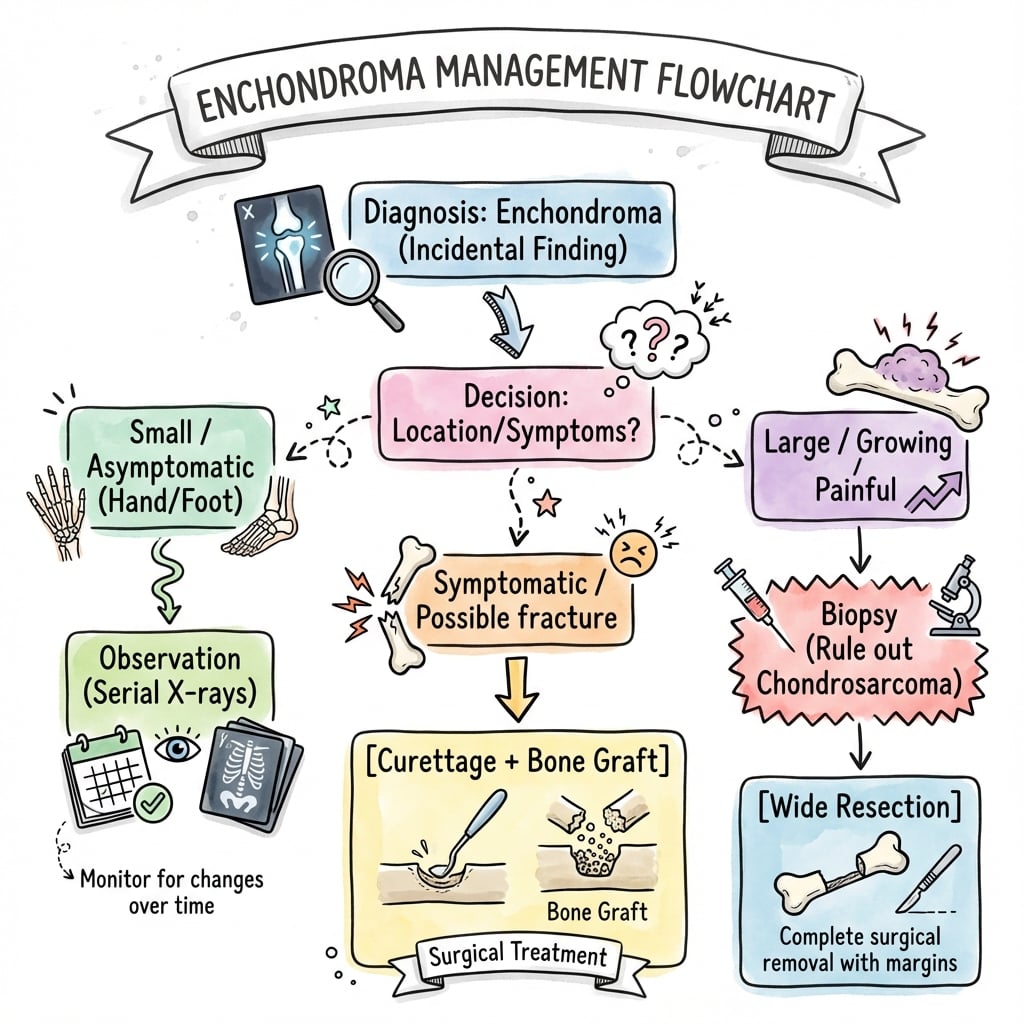
Asymptomatic hand lesions: observe. Pathological fracture: treat fracture, then curettage and bone graft after healing. Suspected malignancy: wide excision with margins.
Enchondroma vs Chondrosarcoma: Key Differentiators
| Feature | Enchondroma (Benign) | Low-Grade Chondrosarcoma | Management |
|---|---|---|---|
| Pain | Painless or only with fracture | Pain without trauma | Symptom assessment critical |
| Location | Hand, foot (90% in hand) | Pelvis, femur, humerus (axial) | Location guides suspicion |
| Cortical thickness | Under 2/3 scalloping | Over 2/3 or breakthrough | Measure on CT |
| Soft tissue mass | Absent | Present on MRI | MRI essential for axial lesions |
At a Glance
Enchondroma is a benign intramedullary cartilage tumour and the most common tumour of hand bones (50%), typically affecting phalanges and metacarpals in adults aged 20-40 years. X-ray shows characteristic rings-and-arcs calcification pattern with central medullary location and endosteal scalloping (under 2/3 cortical thickness if benign). Solitary lesions have 1-2% malignant transformation risk; Ollier disease (multiple, unilateral) has 25-30%; Maffucci syndrome (plus hemangiomas) approaches 100%. Pain without fracture is the key red flag suggesting transformation to chondrosarcoma—requires urgent MRI and biopsy. Asymptomatic hand lesions are observed; pathological fractures are treated conservatively first, then curettage and bone grafting after union.
CENTRALEnchondroma Key Features
| C | Cartilage tumor (hyaline) Lobulated hyaline cartilage in medullary cavity |
| E | Endosteal scalloping Under 2/3 cortical thickness is benign |
| N | No pain (unless fracture) Asymptomatic or pain only with pathological fracture |
| T | Tubular bones of hand 50% of all hand bone tumors, 90% in phalanges/metacarpals |
| R | Rings-and-arcs calcification Pathognomonic pattern on X-ray |
| A | Age 20-40 years Peak incidence in young to middle-aged adults |
| L | Low malignant risk (solitary) 1-2% transformation to chondrosarcoma |
| C | Cartilage tumor (hyaline) Lobulated hyaline cartilage in medullary cavity | T | Tubular bones of hand 50% of all hand bone tumors, 90% in phalanges/metacarpals | L | Low malignant risk (solitary) 1-2% transformation to chondrosarcoma |
| E | Endosteal scalloping Under 2/3 cortical thickness is benign | R | Rings-and-arcs calcification Pathognomonic pattern on X-ray | ||
| N | No pain (unless fracture) Asymptomatic or pain only with pathological fracture | A | Age 20-40 years Peak incidence in young to middle-aged adults |
Hook:CENTRAL location (medullary cavity), CENTRAL finding (rings-and-arcs), most CENTRAL to hand tumors!
PAINSRed Flags for Malignant Transformation
| P | Pain without trauma New onset pain in previously asymptomatic lesion |
| A | Axial or proximal location Pelvis, femur, humerus have higher risk than hand |
| I | Increasing size Progressive enlargement on serial imaging |
| N | New soft tissue mass Soft tissue component on MRI suggests malignancy |
| S | Scalloping greater than 2/3 Cortical erosion over 2/3 thickness or breakthrough |
| P | Pain without trauma New onset pain in previously asymptomatic lesion | N | New soft tissue mass Soft tissue component on MRI suggests malignancy |
| A | Axial or proximal location Pelvis, femur, humerus have higher risk than hand | S | Scalloping greater than 2/3 Cortical erosion over 2/3 thickness or breakthrough |
| I | Increasing size Progressive enlargement on serial imaging |
Hook:If patient has PAINS, think malignant transformation to chondrosarcoma!
OMMultiple Enchondromatosis Syndromes
| O | Ollier disease Multiple enchondromas, unilateral, 25-30% malignancy risk |
| M | Maffucci syndrome Enchondromas plus hemangiomas, nearly 100% malignancy risk |
| O | Ollier disease Multiple enchondromas, unilateral, 25-30% malignancy risk |
| M | Maffucci syndrome Enchondromas plus hemangiomas, nearly 100% malignancy risk |
Hook:OM = Ollier and Maffucci - both have multiple enchondromas, increasing malignancy risk!
Overview and Epidemiology
Clinical Significance
Enchondroma is a benign intramedullary cartilage tumor that represents the most common bone tumor of the hand (50% of all hand bone tumors). It consists of hyaline cartilage located centrally within the medullary cavity, typically discovered incidentally on X-rays or after pathological fracture. The key clinical challenge is distinguishing benign enchondroma from low-grade chondrosarcoma, particularly in axial or proximal long bone locations where malignant transformation risk is higher.
Demographics
- Age: Peak 20-40 years (range 10-60)
- Sex: Equal male to female distribution
- Location: 90% in tubular bones of hands and feet
- Most common sites: Proximal phalanx, metacarpal, middle phalanx
Distribution Patterns
- Solitary: 90% of cases, sporadic, low malignancy risk
- Ollier disease: Multiple unilateral, 25-30% malignancy
- Maffucci syndrome: Enchondromas plus hemangiomas, nearly 100% lifetime malignancy
- Metachondromatosis: Rare, enchondromas plus osteochondromas
Pathophysiology and Pathology
Pathogenesis
Enchondromas arise from persistent rests of growth plate cartilage that fail to undergo normal enchondral ossification. These cartilage islands remain within the medullary cavity and may slowly enlarge over time. The exact molecular mechanism is unclear, but mutations in isocitrate dehydrogenase (IDH1 and IDH2) genes have been identified in both enchondromas and secondary chondrosarcomas.
Malignant Transformation Mechanism
Enchondromas can transform into secondary chondrosarcomas, particularly in axial or proximal long bone locations. Transformation is heralded by new pain, progressive enlargement, cortical breakthrough, and soft tissue mass. IDH mutations are present in both benign and malignant lesions, suggesting other genetic changes drive malignant transformation. Risk is 1-2% for solitary lesions but 25-30% for Ollier disease and up to 100% for Maffucci syndrome.
Gross and Histological Features
Macroscopic Appearance
- Location: Central medullary cavity
- Appearance: Lobulated translucent blue-gray tissue
- Consistency: Firm hyaline cartilage
- Calcification: Punctate white calcifications throughout
- Size: Variable, typically 1-5cm in hand bones
Microscopic Features
- Cellularity: Hypocellular hyaline cartilage
- Chondrocytes: Small uniform cells in lacunae
- Nuclei: Small, regular, single nuclei
- Matrix: Abundant hyaline cartilage matrix
- Calcification: Dystrophic calcification common
- Cellularity: Low cellularity (key benign feature)
Histology Pearl for Malignancy
Distinguishing enchondroma from low-grade chondrosarcoma histologically is CHALLENGING. Key malignant features include: increased cellularity (hypercellularity), nuclear atypia (enlarged hyperchromatic nuclei), binucleate cells, myxoid degeneration, and permeation into surrounding bone. However, clinical and radiological correlation is ESSENTIAL - pain, axial location, and soft tissue mass are more reliable indicators of malignancy than subtle histological changes.
Classification
WHO Classification of Cartilaginous Tumours
Enchondroma is classified under benign chondrogenic tumours in the WHO Classification of Tumours of Soft Tissue and Bone.
WHO Classification of Cartilaginous Tumours
| Category | Tumour Type | Behaviour | Location |
|---|---|---|---|
| Benign | Enchondroma | Benign, no metastatic potential | Medullary cavity |
| Benign | Osteochondroma | Benign, 1% malignant transformation | Surface (metaphysis) |
| Benign | Chondroblastoma | Locally aggressive, rare metastasis | Epiphysis |
| Intermediate | Chondromyxoid fibroma | Locally aggressive | Metaphysis |
| Malignant | Chondrosarcoma Grade 1 | Low-grade malignant | Central medullary |
| Malignant | Chondrosarcoma Grade 2-3 | High-grade malignant | Central or periosteal |
Distribution Classification
Enchondroma Distribution Patterns
| Pattern | Definition | Malignancy Risk | Surveillance |
|---|---|---|---|
| Solitary | Single isolated lesion | 1-2% lifetime | Minimal - patient education only |
| Ollier disease | Multiple enchondromas, unilateral predominance | 25-30% by age 40 | Annual clinical review, imaging of symptomatic lesions |
| Maffucci syndrome | Multiple enchondromas plus soft tissue hemangiomas | Nearly 100% lifetime | Aggressive surveillance, low threshold for biopsy |
Classification Pearl
Distribution classification is clinically important because it determines surveillance requirements and malignant transformation risk. Solitary hand enchondromas require minimal follow-up, while Ollier disease and Maffucci syndrome require lifelong surveillance with low threshold for biopsy of any changing lesion.
Clinical Presentation
Common Presentations
- Incidental finding: Asymptomatic, discovered on X-ray for other reasons (50%)
- Pathological fracture: Most common symptomatic presentation in hand
- Painless swelling: Slow-growing firm mass in hand
- Deformity: Angular deformity or limb length discrepancy (Ollier disease)
Red Flag Symptoms
- Pain without trauma: Suggests malignant transformation
- Rapid enlargement: Progressive size increase on imaging
- New mass: Palpable soft tissue extension
- Systemic symptoms: Weight loss, fatigue (rare, suggests malignancy)
Physical Examination
Systematic Hand Examination
- Swelling: Diffuse expansion of affected bone
- Deformity: Angular deformity if large lesion
- Skin: Normal overlying skin (no erythema or warmth)
- Comparison: Compare to contralateral hand
- Mass: Firm, fixed to bone, non-tender
- Tenderness: Absent unless fracture present
- Temperature: Normal (not warm)
- Neurovascular: Check radial/ulnar pulses, sensation
- Active ROM: May be limited if fracture or large lesion
- Passive ROM: Similar to active (no mechanical block)
- Strength: Reduced if pathological fracture
- Function: Assess pinch and grip strength
When to Suspect Malignancy
Any enchondroma with NEW PAIN in absence of trauma requires urgent MRI and biopsy consideration. Pain is the single most important clinical red flag distinguishing benign enchondroma from malignant transformation. Other concerning features: axial/proximal location, progressive enlargement, palpable soft tissue mass, patient age over 40 years at new diagnosis.
Investigations and Imaging
Plain Radiography
Plain X-rays are the diagnostic gold standard for enchondroma. The characteristic appearance is an intramedullary lytic lesion with punctate calcifications creating a rings-and-arcs or popcorn pattern.
Radiographic Features
Central medullary cavity - lesion arises from center of bone, expanding radially. Distinguishes from periosteal chondroma (surface) or bone infarct (serpiginous).
Rings-and-arcs or popcorn calcification - stippled calcifications reflecting calcified cartilage matrix. This pattern is pathognomonic for cartilage tumors (enchondroma, chondrosarcoma).
Endosteal scalloping - benign lesions cause scalloping of less than 2/3 cortical thickness. Scalloping greater than 2/3 or cortical breakthrough suggests malignancy.
No periosteal reaction in uncomplicated enchondroma. Periosteal reaction indicates pathological fracture or malignant transformation.
Radiographic Pearl
Rings-and-arcs calcification pattern represents calcified cartilage lobules (rings) with intervening uncalcified fibrous septa (arcs). This pattern is seen in ALL cartilage tumors (enchondroma, chondrosarcoma, chondroblastoma) but does NOT distinguish benign from malignant. Clinical correlation (pain, location) is essential.


CT Scan
CT is useful for quantifying cortical destruction and assessing extent of scalloping in equivocal cases, particularly for axial or proximal long bone lesions.
CT Assessment of Cortical Involvement
| Cortical Scalloping | Percentage | Interpretation | Management |
|---|---|---|---|
| Minimal scalloping | Under 1/3 thickness | Benign enchondroma | Observation if asymptomatic |
| Moderate scalloping | 1/3 to 2/3 thickness | Likely benign, observe | Close surveillance, MRI if symptoms |
| Severe scalloping | Over 2/3 thickness | Concerning for malignancy | MRI and biopsy required |
| Cortical breakthrough | 100% (through cortex) | Highly suspicious for chondrosarcoma | Wide excision with margins |
MRI - Gold Standard for Malignancy Assessment
MRI is mandatory for all symptomatic enchondromas and those in axial or proximal long bone locations to assess for soft tissue extension and marrow involvement.
Benign MRI Features
- T1 signal: Low to intermediate (cartilage)
- T2 signal: Very high (hyaline cartilage)
- Enhancement: Peripheral enhancement of lobules only
- Soft tissue: No soft tissue component
- Size: Typically under 5cm
- Margins: Well-defined lobulated contour
Malignant MRI Features
- T1 signal: Heterogeneous with areas of low signal
- T2 signal: Heterogeneous (myxoid degeneration)
- Enhancement: Intense irregular enhancement
- Soft tissue: Soft tissue mass present
- Size: Typically over 5cm
- Margins: Ill-defined infiltrative pattern
MRI Limitations
Even with MRI, distinguishing enchondroma from low-grade chondrosarcoma can be impossible based on imaging alone. Biopsy is often required but carries risk of upgrading tumor grade due to sampling error. Clinical correlation (pain, patient age, lesion location) is paramount. In equivocal cases, serial imaging over 6 months to assess stability may be safer than biopsy.
Biopsy
Biopsy is indicated for symptomatic lesions (pain without fracture) or radiologically suspicious lesions (axial location, soft tissue mass, cortical breakthrough).
Biopsy Considerations
| Scenario | Biopsy Indication | Technique | Risk |
|---|---|---|---|
| Asymptomatic hand enchondroma | No biopsy needed | Diagnosis by imaging alone | None |
| Pathological fracture hand | Curettage at surgery | Send curettings for histology | Low risk |
| Painful axial lesion | Biopsy required | CT-guided core needle | Tumor seeding, upgrade risk |
| Suspected chondrosarcoma | Biopsy before resection | Excisable trajectory, multiple cores | Tumor seeding, sampling error |
Differential Diagnosis
Key Differentials for Intramedullary Cartilage Lesions
| Entity | Age | Location | Pain | X-ray Features |
|---|---|---|---|---|
| Enchondroma | 20-40y | Hand, foot (90%) | Painless unless fracture | Rings-and-arcs, under 2/3 scalloping |
| Low-grade chondrosarcoma | Over 40y | Pelvis, femur, humerus | Pain without trauma | Over 2/3 scalloping, soft tissue mass |
| Bone infarct | Any age | Metaphysis/diaphysis | Painless | Serpiginous calcification, sclerotic rim |
| Chondroblastoma | Under 20y | Epiphysis | Painful | Eccentric lytic, thin sclerotic rim |
| Chondromyxoid fibroma | 10-30y | Metaphysis tibia | Mild pain | Eccentric lytic, scalloped, sclerotic rim |
Enchondroma vs Bone Infarct
Key distinguishing features:
Enchondroma: Rings-and-arcs calcification (organized lobular pattern), central location, expands bone, may scallop cortex.
Bone infarct: Serpiginous (snake-like) calcification following vascular distribution, dense peripheral sclerotic rim, does NOT expand bone or scallop cortex, often multiple lesions.
Exam answer: "While both show central calcification, enchondroma has rings-and-arcs pattern reflecting cartilage lobules, while bone infarct has serpiginous calcification following vascular channels with a dense peripheral rim. Bone infarcts do not expand or scallop the bone."
Management Algorithm
Asymptomatic Hand Lesions
Management: Observation only. No surgery required for incidentally discovered asymptomatic enchondromas of the hand.
Observation Protocol
- Plain X-rays to confirm diagnosis
- No further imaging if classic appearance
- Educate patient about benign nature
- Counsel about pathological fracture risk
- No routine follow-up required
- Patient returns if new pain or fracture
- Re-X-ray only if symptoms develop
When NOT to Operate
Asymptomatic hand enchondromas should NOT be prophylactically excised. They have extremely low malignant potential (under 1%), and surgery carries risks of stiffness, infection, and neurovascular injury. Observation is safe and appropriate. Surgery is indicated only for: (1) pathological fracture, (2) progressive deformity, or (3) rare development of pain suggesting malignancy.
Pathological Fracture Management
Fracture Treatment Algorithm
- Immobilize in splint or cast
- X-ray to confirm fracture and assess alignment
- Conservative fracture treatment (casting)
- Allow fracture to heal (4-6 weeks)
- Curettage of lesion through cortical window
- Thorough removal of all cartilage
- Bone grafting (autograft or allograft)
- Send curettings for histology to confirm enchondroma
- Early mobilization (finger exercises day 1)
- Progressive strengthening
- Return to function by 3 months
Surgical Pearls
Curettage technique for hand enchondroma:
- Wait for fracture to heal before curettage (reduces risk of re-fracture)
- Create cortical window away from previous fracture site
- Thorough curettage with curette - remove ALL cartilage
- High-speed burr to cavity walls (optional adjuvant)
- Bone graft to fill defect (autograft from distal radius or allograft)
- Recurrence rate under 5% with complete curettage
Surgical Technique
Curettage and Bone Grafting for Hand Enchondroma
Curettage Technique Steps
Regional or local anaesthesia with arm tourniquet. Position hand on hand table. Mark cortical window site away from previous fracture site if applicable.
Dorsal longitudinal incision over affected phalanx or metacarpal. Protect extensor mechanism by splitting between central slip and lateral band. Create cortical window with oscillating saw (5-8mm).
Thorough curettage of all cartilage with curettes of various sizes. Inspect cavity to ensure no residual cartilage remains. Optional: high-speed burr to cavity walls to remove 1mm of additional tissue.
Pack cavity with autograft (distal radius preferred) or allograft chips. Ensure complete filling of defect to facilitate radiographic surveillance for recurrence.
No cortical window closure needed. Repair extensor mechanism if split. Skin closure with interrupted nylon. Bulky dressing with finger extension splint.
Technical Pearls
Keys to successful curettage:
- Wait for pathological fracture to heal before curettage (reduces re-fracture risk)
- Create window on dorsal surface away from flexor tendons
- Use curettes and not high-speed burr alone (burr smears cartilage)
- Send ALL curettings for histology to confirm diagnosis
- Complete filling with bone graft aids recurrence detection
Bone Graft Options
Autograft: Distal radius (Lister's tubercle), iliac crest for larger defects. Best biological properties but donor site morbidity.
Allograft: Cancellous chips, no donor morbidity, readily available. Equivalent outcomes to autograft for hand enchondromas.
Synthetic: Calcium phosphate or calcium sulfate. Option for small defects but may obscure recurrence detection.
Complications
Treatment-Related Complications
Complications After Curettage
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Recurrence | Under 5% (hand), 10-20% (axial) | Incomplete curettage, residual cartilage | Revision curettage or wide excision |
| Pathological fracture post-op | 2-5% | Large defect, inadequate bone graft | Immobilization, consider internal fixation |
| Finger stiffness | 10-15% | Prolonged immobilization, adhesions | Aggressive physiotherapy, tenolysis if needed |
| Wound infection | 2-3% | Contamination, poor vascularity | Antibiotics, debridement if needed |
| Digital nerve injury | Under 1% | Iatrogenic during dissection | Primary repair if identified |
Disease-Related Complications
Pathological Fracture
- Incidence: 38% of hand enchondromas present with fracture
- Mechanism: Cortical thinning weakens bone
- Sites: Proximal phalanx most common (40%)
- Management: Immobilize, allow healing, delayed curettage
- Prevention: Cannot be prevented; educate about fracture risk
Malignant Transformation
- Risk: 1-2% solitary, 25-30% Ollier, nearly 100% Maffucci
- Presentation: New pain without trauma
- Diagnosis: MRI shows soft tissue mass, biopsy confirms
- Treatment: Wide excision with negative margins
- Prognosis: 90% 5-year survival for low-grade chondrosarcoma
Recognizing Malignant Transformation
Red flags requiring urgent investigation:
- New onset pain in previously asymptomatic lesion
- Progressive enlargement on serial imaging
- Development of soft tissue mass on examination
- Cortical breakthrough on X-ray or CT
- Patient age over 40 with new diagnosis in axial skeleton
Management: MRI to assess soft tissue extent, CT-guided biopsy with excisable trajectory, wide excision if chondrosarcoma confirmed. Do NOT perform curettage for suspected malignancy - inadequate treatment.
Prevention of Recurrence
Key technical points to minimize recurrence:
- Thorough curettage - remove ALL visible cartilage with sharp curette
- High-speed burr - optional adjuvant to remove 1mm of cavity wall
- Inspect cavity - ensure no residual cartilage fragments
- Adequate bone graft - fill defect completely to detect recurrence on X-ray
- Send curettings - histology confirms diagnosis
Recurrence under 5% for hand lesions with complete curettage. Higher (10-20%) for axial lesions due to difficult access.
Postoperative Care
Postoperative Rehabilitation Protocol
Bulky dressing with finger extension splint. Elevate hand above heart level. Active ROM of uninvolved fingers. Ice for swelling control.
Reduce dressing to light compressive bandage. Begin active ROM exercises of involved finger within pain tolerance. Buddy tape to adjacent finger for support.
Gentle active and passive ROM exercises. Focus on full extension and flexion. Hand therapy referral if stiffness developing.
Progressive strengthening with putty and grip exercises. Light functional activities permitted. X-ray at 6 weeks to assess graft incorporation.
Full activity including manual work by 3 months. No restrictions long-term. Final X-ray to confirm healing and no recurrence.
Follow-up Protocol
Hand enchondroma after curettage:
- X-ray at 6 weeks and 3 months to confirm graft incorporation
- No routine long-term follow-up needed (recurrence under 5%)
- Patient education: return if new pain develops
Axial lesions after curettage:
- Serial imaging every 6 months for 2 years
- Annual imaging thereafter for 5 years
- MRI if concern for recurrence
Outcomes and Prognosis
Surgical Outcomes
Hand enchondroma curettage: Excellent outcomes with under 5% recurrence, minimal functional impact, return to full function by 3 months.
Axial/proximal enchondroma: Higher recurrence (10-20%) due to incomplete excision. Wide excision for chondrosarcoma has 5-year survival 90% for Grade 1 lesions.
Long-term Prognosis
Solitary Enchondroma
- Malignancy risk: 1-2% lifetime (very low)
- Hand lesions: Excellent prognosis, benign behavior
- Axial lesions: Higher risk, require surveillance
- After curettage: Low recurrence, cure expected
Multiple Enchondromatosis
- Ollier disease: 25-30% malignant transformation
- Maffucci syndrome: Nearly 100% malignancy by age 40
- Surveillance: Lifelong, multiple imaging studies
- Quality of life: Impaired by deformities and surgeries
Evidence Base and Key Studies
Chondrosarcoma Risk in Ollier Disease and Maffucci Syndrome (Landmark Multicentre Cohort)
- International multicentre study of 161 patients (144 Ollier disease, 17 Maffucci syndrome) from 13 European centres
- Overall observed incidence of secondary chondrosarcoma was 40% (age-dependent, rising as a lifelong risk)
- Disease confined to hands and feet only (18% of patients) carried the lowest risk - chondrosarcoma in just 15%
- Pelvic enchondromas markedly increased malignant risk (odds ratio 3.8) - patients with long-bone or axial lesions need regular screening
- Maffucci syndrome patients carry additional risk of vascular malignancy alongside chondrosarcoma
Enchondroma vs Chondrosarcoma in the Appendicular Skeleton: Differentiating Features
- Large series of 187 appendicular lesions (92 enchondromas, 95 chondrosarcomas) with multimodality imaging review
- Lesion-related pain, deep endosteal scalloping (greater than two-thirds cortical thickness), cortical destruction and soft-tissue mass all strongly favoured chondrosarcoma
- Periosteal reaction on radiographs and marked radionuclide uptake (greater than anterior iliac crest) also discriminated malignancy
- Combined clinical and imaging criteria distinguished appendicular enchondroma from chondrosarcoma in at least 90% of cases
Somatic Mosaic IDH1/IDH2 Mutations in Enchondromatosis (Defining Molecular Study)
- Somatic heterozygous IDH1 (predominant) or IDH2 mutations found in 87% of enchondromas and 70% of spindle cell haemangiomas
- Mutations were somatic mosaic, not germline - explaining the non-hereditary, mosaic pattern of Ollier disease and Maffucci syndrome
- 81% of Ollier and 77% of Maffucci patients carried IDH1/IDH2 mutations; identical mutations were present across separate lesions in the same patient
- IDH mutation drove DNA hypermethylation and gene downregulation; the same mutations also occurred in 40% of solitary central cartilage tumours and chondrosarcoma cell lines
Curettage and Allograft for Hand Enchondroma: Range of Motion and Recurrence
- Retrospective series of 111 hand enchondromas in 104 patients treated by curettage and cancellous allograft without internal fixation or adjuvant
- 81% of patients achieved full range of motion; preoperative pathological fracture predicted worse postoperative extension (reduced ROM in 28% vs 15%)
- Local recurrence developed in 5 of 50 (10%) patients with at least 2 years follow-up
- Recurrence was concentrated in giant-form (Takigawa) lesions (43%) and Ollier disease (23%); 16% of the cohort had Ollier disease
Hand Enchondroma Curettage Without Void Augmentation: Series and Systematic Review
- Systematic review of 22 studies (591 patients, 609 lesions) plus an institutional series of 26 lesions
- Complication rates were low and did not differ significantly between curettage alone, autograft, osteoconductive substitute, or cement augmentation (0.7% to 3.5%)
- Recurrence rates were not significantly different across void-management strategies
- Curettage alone is an effective, inexpensive option for most hand enchondromas
Incidental Enchondromas on Knee MRI: Population Prevalence
- Incidental enchondromas were present on 2.9% of 449 consecutive routine knee MRI examinations
- Most common in the distal femur (2.0%), then proximal tibia (0.7%) and proximal fibula (0.2%)
- Average lesion size 1.9 cm; 57% were under 1 cm and 92% lay in the metaphysis or diaphysis
- MRI prevalence far exceeded the historical autopsy figure (0.2%), reflecting greater MRI sensitivity; no aggressive features suggesting chondrosarcoma were seen
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Incidental Hand Enchondroma
"A 25-year-old office worker presents with an incidentally discovered 2cm lytic lesion with rings-and-arcs calcification in the proximal phalanx of the middle finger on X-ray taken after minor trauma. The lesion is asymptomatic with no fracture. What is your diagnosis and management?"
Scenario 2: Pathological Fracture Through Hand Enchondroma
"A 30-year-old manual laborer presents with acute pain and swelling of the right ring finger after lifting a heavy box. X-ray shows a displaced fracture through a 2.5cm lytic lesion with rings-and-arcs calcification in the proximal phalanx. How do you manage this patient?"
Scenario 3: Painful Proximal Femur Lesion - Enchondroma vs Chondrosarcoma
"A 45-year-old woman presents with 3 months of progressive thigh pain with no trauma. X-ray shows a 6cm intramedullary lytic lesion with rings-and-arcs calcification in the proximal femur with cortical scalloping over 2/3 thickness. MRI shows high T2 signal with some soft tissue component. How do you proceed?"
MCQ Practice Points
Clinical Pearl
Q: What is the most common location for enchondroma and what are its characteristic imaging features?
A: Most common in small bones of the hands and feet (50%), followed by proximal humerus and femur. Imaging: Well-defined lytic lesion in medullary cavity; Chondroid matrix calcification ("rings and arcs," "popcorn" pattern); Endosteal scalloping (less than 2/3 cortical thickness); No periosteal reaction or cortical destruction; Size usually less than 5cm. In long bones, located in metaphysis or metadiaphysis.
Clinical Pearl
Q: How do you differentiate benign enchondroma from low-grade chondrosarcoma?
A: Features favoring malignancy: Size greater than 5cm; Location in axial skeleton or proximal limb girdle; Endosteal scalloping greater than 2/3 cortical thickness; Cortical destruction or soft tissue mass; Pain at rest (not related to pathological fracture); Interval growth on serial imaging; Periosteal reaction. MRI: Enchondroma has peripheral/septal enhancement only; Chondrosarcoma shows diffuse enhancement. When uncertain, biopsy may not differentiate - close surveillance or wide excision based on clinical concern.
Clinical Pearl
Q: What is Ollier disease and Maffucci syndrome, and what is the malignancy risk?
A: Ollier disease: Multiple enchondromas (enchondromatosis), non-hereditary, asymmetric distribution. Maffucci syndrome: Multiple enchondromas + soft tissue hemangiomas. Malignancy risk: Ollier: commonly quoted 25-30% lifetime risk of chondrosarcoma (a large multicentre cohort found 40% overall and higher with axial/pelvic disease); Maffucci: lifelong risk approaching 100%, with additional vascular and visceral malignancies (e.g. ovarian, brain tumours). Both are driven by somatic mosaic IDH1/IDH2 mutations. Surveillance: clinical review with imaging of any new or symptomatic lesion; any pain or growth warrants investigation for malignant transformation.
Clinical Pearl
Q: What is the standard treatment for solitary enchondroma in the hand?
A: Asymptomatic enchondroma: Observation with serial radiographs. Symptomatic (pain, pathological fracture risk) or post-fracture: Curettage and bone grafting. Technique: Allow fracture to heal first (4-6 weeks), then curettage through cortical window, thorough removal of cartilage, bone graft or cement. Recurrence rate: Less than 5%. Pathological fracture: May treat fracture first, then staged curettage, or combined if stable fixation achievable.
Clinical Pearl
Q: What histological features differentiate enchondroma from chondrosarcoma?
A: Enchondroma: Hypocellular with small, uniform nuclei; Cells in lacunae with minimal atypia; No mitoses; Minimal myxoid change; Lobular architecture with peripheral enchondral ossification. Chondrosarcoma: Hypercellularity; Nuclear atypia, pleomorphism, binucleation; Mitotic figures (in higher grades); Myxoid matrix change; Permeation of surrounding bone trabeculae. Important: Histology alone may not differentiate Grade 1 chondrosarcoma from enchondroma - requires clinico-radiological correlation.
Guidelines, Registries & Global Practice
Global Epidemiology
Enchondroma is among the commonest bone tumours worldwide, but its true frequency is far higher than symptomatic series suggest. Population imaging studies repeatedly find incidental cartilage lesions in roughly 3% of adults, and modern terminology now separates benign enchondroma from atypical cartilaginous tumour (ACT) / grade 1 chondrosarcoma in long bones.
Population Prevalence and Malignant Risk (PubMed-Backed)
| Measure | Figure | Source / Cohort |
|---|---|---|
| Incidental enchondroma on routine knee MRI | 2.9% (distal femur 2.0%) | Walden 2008, AJR (PMID 18492914) |
| Incidental cartilage tumours on knee MRI (NEO cohort, age 45-65) | 2.8% (some proved ACT/CS1) | Stomp/Bovée 2015, Eur Radiol (PMID 25994192) |
| Historical autopsy prevalence | ~0.2% | Cited in Walden 2008 (PMID 18492914) |
| Secondary chondrosarcoma, enchondromatosis (overall) | 40% (lifelong risk higher) | Verdegaal 2011, Oncologist (PMID 22147000) |
| Chondrosarcoma, hand/foot-only enchondromatosis | 15% | Verdegaal 2011 (PMID 22147000) |
| Pelvic enchondroma malignant risk | Odds ratio 3.8 | Verdegaal 2011 (PMID 22147000) |
Side-by-Side Guidance: Diagnosis and Surveillance of Long-Bone Cartilage Tumours
There is no single randomised-trial-based guideline; international practice rests on bone-tumour society consensus and large referral-centre series. The major bodies converge on active surveillance for asymptomatic, imaging-benign lesions and referral of any red-flag lesion to a sarcoma unit.
International Guidance Comparison
| Body / Region | Core Position on Solitary Cartilage Tumours | Evidence Level |
|---|---|---|
| ESMO / EURACAN-PaedCan (Europe) | Refer suspected bone sarcoma to a specialist sarcoma centre before biopsy; biopsy through an excisable track; MDT decision-making | Consensus guideline (expert) |
| BSG / BOOS (UK, British Orthopaedic Oncology Society) | Asymptomatic, imaging-typical enchondroma needs no biopsy; suspicious long-bone lesions referred to a bone-tumour unit | Consensus / national pathway |
| EMSOS / EFORT (Europe) | Active surveillance acceptable for ACT/grade 1 lesions of long bones; intralesional curettage preferred over wide resection for low-grade central tumours | Consensus + observational evidence |
| AAOS / MSTS (North America) | Clinico-radiological correlation; biopsy reserved for symptomatic or atypical lesions; emphasises pain and deep scalloping as triggers | Consensus / appropriate-use |
| WHO Classification of Bone Tumours (5th ed, global) | Defines enchondroma (benign) vs ACT/CS1 (locally aggressive, long bones) - terminology standard underpinning all guidance | Reference standard |
Convergent Global Principle
Across AAOS, BOOS, ESMO and EMSOS the message is identical: an asymptomatic enchondroma with classic imaging needs reassurance, not biopsy, while any painful, enlarging, deeply scalloping or axial cartilage lesion must be referred to a sarcoma multidisciplinary team before intervention. The shift toward active surveillance for ACT/grade 1 long-bone lesions is the main recent change in practice.
Registries and Practice Variation
There is no dedicated international enchondroma registry. Outcome data derive from sarcoma-unit cohorts and national bone-tumour referral databanks (e.g. the European Musculoskeletal Oncology Society network underpinning Verdegaal 2011). Practice still varies:
- Bone-void management after hand curettage (autograft vs allograft vs cement vs nothing) shows no proven difference in recurrence or complications (Bachoura 2015, PMID 26330779) - choice is surgeon-dependent.
- Long-bone ACT/grade 1: increasing international move from wide resection toward active surveillance or intralesional curettage, but thresholds differ between centres.
- IDH1/IDH2 mutation testing is available in tertiary molecular pathology laboratories and supports diagnosis in difficult cases but is not yet a routine global standard.
Documentation and Referral Essentials (Any Health System)
- Record a clear pain assessment - the single most important malignancy discriminator.
- Document endosteal scalloping depth (proportion of cortex) on the imaging report.
- Obtain MRI for any symptomatic or axial/proximal lesion before intervention.
- Ensure any biopsy track is excisable at definitive surgery and ideally performed at the treating sarcoma unit.
- Reassure patients with classic hand enchondroma about benign behaviour; advise return if new pain develops.
ENCHONDROMA
Clinical summary
Key Facts
- •Most common hand bone tumor (50%), benign intramedullary cartilage
- •Peak age 20-40 years, equal male-female
- •90% in tubular bones of hands and feet (phalanges, metacarpals)
- •Rings-and-arcs calcification pathognomonic on X-ray
Diagnosis
- •X-ray: central medullary lytic with rings-and-arcs calcification
- •Endosteal scalloping under 2/3 cortical thickness is benign
- •MRI for symptomatic/axial lesions: high T2 signal cartilage
- •Biopsy only if pain, axial location, or suspicious features
Red Flags for Malignancy
- •Pain without trauma (key clinical red flag)
- •Axial or proximal long bone location (pelvis, femur, humerus)
- •Cortical scalloping greater than 2/3 or breakthrough
- •Soft tissue mass on MRI, size over 5cm
Management
- •Asymptomatic hand: observation only, no surgery
- •Pathological fracture: immobilize, delayed curettage after healing
- •Curettage technique: cortical window, thorough curettage, bone graft
- •Suspected chondrosarcoma: wide excision with 5-10mm margins
Multiple Enchondromatosis
- •Ollier disease: multiple unilateral, 25-30% malignancy risk
- •Maffucci syndrome: enchondromas plus hemangiomas, nearly 100% malignancy
- •Lifelong surveillance required for both syndromes
- •IDH1/IDH2 mutations in 87% of enchondromas and chondrosarcomas
Key Outcomes
- •Hand curettage: under 5% recurrence, excellent function
- •Solitary enchondroma: 1-2% lifetime malignant transformation
- •Low-grade chondrosarcoma: 90% 5-year survival with wide excision
- •Chondrosarcoma does NOT respond to chemotherapy or radiation