Multiple Enchondromas | IDH Mutations | High Malignancy Risk | Lifelong Surveillance Required
ENCHONDROMATOSIS SYNDROMES
Critical Must-Knows
- Ollier disease - multiple unilateral enchondromas, 25-30% malignant transformation by age 40
- Maffucci syndrome - enchondromas plus hemangiomas, nearly 100% lifetime malignancy risk
- IDH1 and IDH2 somatic mutations found in 87% of enchondromas and secondary chondrosarcomas
- Lifelong surveillance required with annual clinical exam and imaging of symptomatic lesions
- Pain, growth, or soft tissue mass in any lesion requires urgent MRI and biopsy consideration
Clinical Pearls
- "Ollier disease is sporadic (somatic IDH mutations), NOT inherited - low recurrence risk
- "Maffucci syndrome patients develop both chondrosarcoma (from enchondromas) and angiosarcoma (from hemangiomas)
- "Deformities common: limb length discrepancy, angular deformity, pathological fractures
- "Low threshold for biopsy - any changing lesion is malignant until proven otherwise
Critical Enchondromatosis Exam Points
Malignant Transformation Risk
Ollier disease carries 25-30% risk of chondrosarcoma by age 40. Maffucci syndrome has nearly 100% lifetime malignancy risk - both chondrosarcoma from enchondromas and angiosarcoma from hemangiomas. Any new pain, growth, or soft tissue mass requires urgent MRI and biopsy.
Unilateral Distribution
Ollier disease shows unilateral or predominantly one-sided distribution of enchondromas. If bilateral and symmetric, consider Maffucci syndrome (if hemangiomas present) or metachondromatosis (if osteochondromas present).
IDH Mutations
IDH1 and IDH2 somatic mutations found in 87% of enchondromas and chondrosarcomas in Ollier/Maffucci. These are NOT germline mutations - disease is sporadic, not inherited. Mutations disrupt cartilage differentiation leading to multiple cartilage rests.
Surveillance Protocol
Annual clinical examination with skeletal survey. MRI any symptomatic lesion - pain, growth, or palpable mass. Low threshold for biopsy of suspicious lesions. Early detection of malignant transformation is critical for limb salvage and survival.
Ollier Disease vs Maffucci Syndrome vs Solitary Enchondroma
| Feature | Solitary Enchondroma | Ollier Disease | Maffucci Syndrome |
|---|---|---|---|
| Number of lesions | Single lesion | Multiple (5 or more typical) | Multiple plus hemangiomas |
| Distribution | Usually hand/foot | Unilateral or asymmetric | Asymmetric, any bone |
| Malignancy risk | 1-2% lifetime | 25-30% by age 40 | Nearly 100% lifetime |
| Genetics | Sporadic, usually no mutation | Somatic IDH1/IDH2 (87%) | Somatic IDH1/IDH2 (87%) |
| Surveillance | None required if asymptomatic | Annual exam and imaging | Aggressive annual surveillance |
| Deformities | Rare | Common (LLD, angulation) | Common plus vascular lesions |
At a Glance
Enchondromatosis encompasses multiple enchondroma syndromes with high malignant transformation risk. Ollier disease features multiple unilateral enchondromas with 25-30% chondrosarcoma transformation by age 40. Maffucci syndrome combines enchondromas with soft tissue hemangiomas and carries nearly 100% lifetime malignancy risk—both chondrosarcoma (from cartilage) and angiosarcoma (from hemangiomas). Both are caused by somatic IDH1/IDH2 mutations (87%)—sporadic, not inherited. Lifelong surveillance is mandatory: annual clinical examination, low threshold for MRI of any symptomatic lesion, and urgent biopsy consideration for pain, growth, or soft tissue mass. Common skeletal complications include limb length discrepancy, angular deformity, and pathological fractures.
OLLIEROllier Disease Features
| O | One-sided (unilateral) Unilateral or predominantly asymmetric distribution |
| L | Limb deformity Limb length discrepancy and angular deformities common |
| L | Lesions multiple Multiple enchondromas (5 or more typical) |
| I | IDH mutations Somatic IDH1/IDH2 mutations in 87% of lesions |
| E | Enchondromas only NO hemangiomas (distinguishes from Maffucci) |
| R | Risk of sarcoma 25-30% malignant transformation to chondrosarcoma |
| O | One-sided (unilateral) Unilateral or predominantly asymmetric distribution | L | Lesions multiple Multiple enchondromas (5 or more typical) | E | Enchondromas only NO hemangiomas (distinguishes from Maffucci) |
| L | Limb deformity Limb length discrepancy and angular deformities common | I | IDH mutations Somatic IDH1/IDH2 mutations in 87% of lesions | R | Risk of sarcoma 25-30% malignant transformation to chondrosarcoma |
Hook:OLLIER disease = One-sided Lesions with high malignancy Risk!
MAFFUCCIMaffucci Syndrome Red Flags
| M | Multiple enchondromas Numerous cartilage tumors in bones |
| A | Angiosarcoma risk Hemangiomas can transform to angiosarcoma |
| F | Frightening prognosis Nearly 100% lifetime malignancy risk |
| F | Fractures pathological Weakened bones from multiple lesions |
| U | Ugly deformities Severe skeletal and soft tissue deformities |
| C | Chondrosarcoma common Enchondromas transform to chondrosarcoma |
| C | Cutaneous hemangiomas Visible soft tissue vascular lesions |
| I | IDH mutations present Somatic IDH1/IDH2 drive both lesions |
| M | Multiple enchondromas Numerous cartilage tumors in bones | F | Fractures pathological Weakened bones from multiple lesions | C | Cutaneous hemangiomas Visible soft tissue vascular lesions |
| A | Angiosarcoma risk Hemangiomas can transform to angiosarcoma | U | Ugly deformities Severe skeletal and soft tissue deformities | I | IDH mutations present Somatic IDH1/IDH2 drive both lesions |
| F | Frightening prognosis Nearly 100% lifetime malignancy risk | C | Chondrosarcoma common Enchondromas transform to chondrosarcoma |
Hook:MAFFUCCI syndrome = Multiple tumors with Frightening malignancy risk!
WATCHSurveillance Protocol - WATCH
| W | Whole body skeletal survey Annual X-rays of all affected areas at baseline |
| A | Annual clinical examination Check for new pain, masses, deformities yearly |
| T | Threshold low for MRI Any symptomatic lesion gets MRI immediately |
| C | Consider biopsy early Low threshold for biopsy of changing lesions |
| H | Hemangiomas also monitor In Maffucci, watch for angiosarcoma transformation |
| W | Whole body skeletal survey Annual X-rays of all affected areas at baseline | C | Consider biopsy early Low threshold for biopsy of changing lesions |
| A | Annual clinical examination Check for new pain, masses, deformities yearly | H | Hemangiomas also monitor In Maffucci, watch for angiosarcoma transformation |
| T | Threshold low for MRI Any symptomatic lesion gets MRI immediately |
Hook:WATCH closely for malignant transformation - patient's life depends on it!
Overview and Epidemiology
Definition and Classification
Enchondromatosis refers to syndromes characterized by multiple enchondromas. The two main types are:
Ollier disease: Multiple enchondromas with unilateral or asymmetric distribution, NO soft tissue hemangiomas.
Maffucci syndrome: Multiple enchondromas PLUS soft tissue hemangiomas (spindle cell hemangiomas).
Both are sporadic conditions caused by somatic mutations in IDH1 or IDH2 genes, NOT inherited. Recurrence risk in offspring is very low.
Ollier Disease Epidemiology
- Incidence: Approximately 1 in 100,000 live births
- Age at presentation: Childhood (under 10 years typical)
- Sex distribution: Equal male to female
- Distribution: Unilateral or markedly asymmetric
- Malignancy risk: 25-30% by age 40 years
Maffucci Syndrome Epidemiology
- Incidence: Even rarer than Ollier (1 in 1,000,000)
- Age at presentation: Childhood, often younger than Ollier
- Hemangiomas: Spindle cell type, visible as soft tissue masses
- Malignancy risk: Nearly 100% lifetime risk
- Tumor types: Chondrosarcoma AND angiosarcoma
Historical Context
The term Ollier disease was named after French surgeon Louis Ollier who described multiple enchondromatosis in 1899. Maffucci syndrome was described by Italian pathologist Angelo Maffucci in 1881 who recognized the association between enchondromas and hemangiomas.
Historically, these conditions were poorly understood and outcomes were dismal. Modern understanding of IDH mutations (discovered 2011) and improved surveillance protocols have enabled earlier detection of malignant transformation and improved survival.
Pathophysiology
IDH1 and IDH2 Mutations
Critical Discovery - IDH Mutations
In 2011, Pansuriya et al discovered that 87% of enchondromas and secondary chondrosarcomas in Ollier disease and Maffucci syndrome harbor somatic mutations in IDH1 (most common) or IDH2 genes. These are:
- Somatic mutations (NOT germline) - explains sporadic occurrence
- Mosaic distribution - mutations occur early in development affecting specific tissue populations
- Present in BOTH benign and malignant lesions - suggests additional genetic hits required for malignant transformation
- Same mutations seen in gliomas - explains increased brain tumor risk in Maffucci syndrome
Key point: IDH mutations are present in enchondromas from birth but malignant transformation requires additional genetic changes (TP53, RB1 mutations) that accumulate over time.
Pathogenesis of Enchondromatosis
Somatic IDH mutation occurs in mesenchymal stem cell during early development. Mutation causes abnormal accumulation of 2-hydroxyglutarate (2-HG) which disrupts cartilage differentiation and normal enchondral ossification.
Multiple cartilage rests persist in medullary cavity instead of ossifying. These appear as enchondromas on X-ray. Growth plate abnormalities lead to limb length discrepancy and angular deformities as child grows.
Accumulation of additional mutations (TP53, RB1, CDKN2A) in some lesions drives malignant transformation. Pain, growth, cortical breakthrough, and soft tissue mass indicate transformation to chondrosarcoma.
For Maffucci syndrome patients, hemangiomas may also transform to angiosarcoma. Multiple tumor sites possible. Prognosis poor due to multifocal disease and late presentation.
Histopathology
Benign Enchondroma (Ollier/Maffucci)
- Cellularity: Hypocellular hyaline cartilage
- Chondrocytes: Small uniform cells in lacunae
- Nuclei: Single, regular, small nuclei
- Matrix: Abundant hyaline cartilage matrix
- Calcification: Dystrophic calcification common
- Growth pattern: Lobular architecture preserved
Secondary Chondrosarcoma (Transformed)
- Cellularity: Hypercellular (increased cell density)
- Chondrocytes: Enlarged cells, irregular distribution
- Nuclei: Enlarged hyperchromatic nuclei, binucleation
- Matrix: Myxoid degeneration areas
- Permeation: Infiltration into surrounding bone
- Atypia: Moderate to severe nuclear atypia
Histological Challenges
Distinguishing benign from malignant lesions histologically is extremely difficult in enchondromatosis patients. Key challenges:
- Enchondromas in Ollier/Maffucci may show higher cellularity than solitary enchondromas (still benign)
- Low-grade chondrosarcoma may have minimal atypia (subtle changes)
- Sampling error common - biopsy may miss malignant areas in heterogeneous tumors
Clinical and radiological correlation is ESSENTIAL. Pain, growth, cortical destruction, and soft tissue mass are more reliable indicators of malignancy than histology alone. Expert musculoskeletal pathologist review mandatory.
Classification
Types of Enchondromatosis
Classification of Enchondromatosis Syndromes
| Syndrome | Key Features | Extra-Skeletal Findings | Malignancy Risk |
|---|---|---|---|
| Ollier Disease | Multiple enchondromas, predominantly unilateral distribution, limb shortening | None | 25-30% lifetime risk of chondrosarcoma |
| Maffucci Syndrome | Multiple enchondromas + multiple soft tissue hemangiomas | Spindle cell hemangiomas (pathognomonic) | Higher risk (40-50%), plus risk of other malignancies |
| Metachondromatosis | Enchondromas + osteochondromas (exostoses) | None | Low |
| Genochondromatosis | Generalized enchondromatosis, autosomal dominant | None | Unknown |
Distribution Patterns
Ollier Disease Distribution:
- Typically unilateral or predominantly affects one side
- Commonly affects hands and feet
- Long bones of lower limb frequently involved
- May cause significant limb length discrepancy
Maffucci Syndrome Distribution:
- Similar enchondroma distribution to Ollier
- Plus spindle cell hemangiomas (soft tissue masses)
- Hemangiomas may be in soft tissues or viscera
- Higher overall malignancy risk
Clinical Pearl
Exam Viva Point: "How do you differentiate Ollier disease from Maffucci syndrome?" Answer: Maffucci syndrome = enchondromas + soft tissue hemangiomas (spindle cell type). Both have IDH mutations as underlying cause. Maffucci has higher malignancy risk (40-50% vs 25-30%) and increased risk of non-skeletal malignancies (gliomas, ovarian tumors).
Classification is based on presence or absence of extra-skeletal features, particularly soft tissue hemangiomas.
Clinical Presentation
Typical Presentation Patterns
Early Childhood Presentation
- Limb deformity noticed by parents (leg length difference)
- Palpable masses in hands or feet (cartilage enlargement)
- Gait abnormality due to limb length discrepancy
- Incidental X-ray finding for minor trauma
- Angular deformity (varus/valgus) of long bones
Adolescent/Adult Presentation
- Pathological fracture through weakened bone
- Progressive deformity worsening with growth
- Pain in lesion (RED FLAG - malignant transformation)
- Palpable soft tissue mass (chondrosarcoma with soft tissue extension)
- Functional impairment from severe deformities
Skeletal Deformities
Common Deformities in Enchondromatosis
| Deformity Type | Mechanism | Location | Management |
|---|---|---|---|
| Limb length discrepancy | Asymmetric growth plate involvement | Lower limbs most common | Epiphysiodesis or lengthening |
| Angular deformity | Metaphyseal enchondromas disrupt growth | Tibia, femur, forearm | Corrective osteotomy when severe |
| Hand deformities | Multiple phalangeal enchondromas | Fingers shortened and widened | Curettage after fractures only |
| Pathological fracture | Cortical thinning from lesions | Any involved bone | Stabilize, then curettage after healing |
Red Flag Symptoms - Malignant Transformation
Signs of Malignant Transformation
Any of these symptoms in a known enchondromatosis patient requires URGENT MRI and biopsy consideration:
- New onset pain in previously asymptomatic lesion (MOST IMPORTANT)
- Progressive enlargement on serial X-rays
- Palpable soft tissue mass on examination
- Cortical breakthrough on X-ray or CT
- Rapid functional decline (new weakness, limited motion)
- Night pain or pain at rest
- Constitutional symptoms (rare - weight loss, fatigue)
Management: MRI of affected area, CT chest to rule out metastases, CT-guided biopsy with excisable trajectory, multidisciplinary tumor board discussion. Do NOT delay - early detection critical for limb salvage.
Physical Examination
Systematic Examination of Enchondromatosis Patient
- Limb lengths: Measure leg lengths (ASIS to medial malleolus)
- Angular deformities: Assess varus/valgus alignment of limbs
- Hand deformities: Note shortened digits, expanded phalanges
- Soft tissue masses: Look for hemangiomas (Maffucci) or soft tissue extension of tumors
- Gait: Observe for limp, Trendelenburg gait
- Bony masses: Palpate all visible/palpable lesions
- Tenderness: Any tender lesion is RED FLAG for malignancy
- Soft tissue masses: Palpate for extraosseous extension
- Hemangiomas: Compressible soft tissue masses (Maffucci)
- Temperature: Warm areas suggest active tumor growth
- Joint range of motion: Check all major joints
- Limb rotation: Assess for rotational deformities
- Functional assessment: Grip strength, walking distance
- Neurovascular exam: Check pulses, sensation in all limbs
- Skeletal diagram: Map all known lesions
- Photography: Document visible deformities and hemangiomas
- Measurements: Record limb lengths and joint angles
- Pain assessment: Document any painful lesions for urgent MRI
Investigations and Imaging
Baseline Skeletal Survey
At diagnosis, patients require complete skeletal survey to document all lesions and establish baseline for surveillance.
Initial Imaging Protocol
- All extremities: AP and lateral views
- Pelvis and femurs: AP views
- Spine: AP and lateral if symptomatic
- Hands and feet: PA views
- Document: number of lesions, size, cortical involvement, deformities
- Proximal long bones: Femur, humerus (high malignancy risk sites)
- Painful lesions: Any lesion with new pain
- Large lesions: Greater than 5cm or significant cortical thinning
- Assess: soft tissue extension, marrow involvement, cortical integrity
- Clinical photos: All visible deformities
- Limb length measurements: Scanogram or CT scanogram
- Angular measurements: Long-leg alignment films if needed
Radiographic Features of Enchondromas (Ollier/Maffucci)
Radiographic Characteristics
| Feature | Appearance | Location | Significance |
|---|---|---|---|
| Matrix calcification | Rings-and-arcs or stippled pattern | Within medullary cavity | Pathognomonic for cartilage tumor |
| Cortical thinning | Endosteal scalloping, expansion | Circumferential in severe cases | Pathological fracture risk |
| Growth plate involvement | Metaphyseal location, crosses physis | Long bones near joints | Causes growth disturbance and deformity |
| Distribution | Multiple lesions, unilateral predominance | Entire limb or hemibody | Diagnostic for Ollier disease |
MRI Assessment for Malignancy
MRI is the gold standard for detecting malignant transformation. Key features:
Benign Enchondroma on MRI
- T1 signal: Low to intermediate (cartilage)
- T2 signal: Very high (hyaline cartilage water content)
- Enhancement: Peripheral septal enhancement only
- Soft tissue: No extraosseous component
- Margins: Well-defined lobulated contour
- Size: Variable but stable on serial imaging
Chondrosarcoma on MRI (Transformed)
- T1 signal: Heterogeneous with low signal areas
- T2 signal: Heterogeneous (myxoid areas)
- Enhancement: Intense irregular enhancement
- Soft tissue: Soft tissue mass PRESENT
- Margins: Ill-defined, infiltrative pattern
- Size: Progressive enlargement on serial MRI
MRI Pearl - Soft Tissue Component
Presence of soft tissue mass on MRI is the SINGLE MOST RELIABLE indicator of malignant transformation in enchondromatosis patients. Benign enchondromas do NOT break through cortex and extend into soft tissue. If you see soft tissue component, assume chondrosarcoma until proven otherwise and proceed with biopsy and wide excision.
Imaging Gallery


Surveillance Imaging Protocol
Lifelong Surveillance Strategy
| Age/Stage | Clinical Exam | Imaging | Frequency |
|---|---|---|---|
| Childhood (under 18) | Annual full exam, measure limbs | Skeletal survey every 2-3 years | More frequent if growing deformities |
| Young adult (18-40) | Annual exam, document new symptoms | X-rays of symptomatic areas only | Annual clinical, imaging as needed |
| Older adult (over 40) | Annual exam with high suspicion | Low threshold for MRI if any symptoms | Annual, more aggressive imaging |
| Any age with symptoms | Urgent clinical evaluation | MRI of affected area, CT chest | Immediate workup for malignancy |
Biopsy Decision-Making
When to Biopsy in Enchondromatosis
Perform biopsy if:
- New pain in previously asymptomatic lesion
- Progressive enlargement on serial imaging
- Soft tissue mass on MRI
- Cortical breakthrough on CT
- Patient age over 40 with new symptoms in axial skeleton
Technique: CT-guided core needle biopsy with excisable trajectory (plan for wide excision through same approach if malignant).
Discuss at tumor board:
- Large lesion (over 5cm) in proximal long bone
- Moderate cortical destruction (over 2/3 thickness)
- Heterogeneous enhancement on MRI (equivocal)
- Patient anxiety about specific lesion
Balance risk of tumor seeding against diagnostic benefit.
Safe to observe:
- Small asymptomatic hand/foot lesions
- Stable size on serial imaging (2+ years)
- Classic benign MRI features if MRI performed
- Young patient with no concerning features
Serial imaging every 6-12 months safer than biopsy.
Biopsy Risks in Enchondromatosis
Specific considerations for biopsy in Ollier/Maffucci patients:
- Tumor seeding: Risk of seeding biopsy tract with malignant cells
- Sampling error: Heterogeneous tumors may show benign areas in biopsy but malignant areas elsewhere
- Histological overlap: Even expert pathologists struggle to distinguish benign from low-grade malignant
- Multiple lesions: Difficult to biopsy every concerning lesion
Recommendation: Reserve biopsy for lesions where clinical/imaging strongly suggests malignancy AND where result will change management (i.e., proceed with wide excision if confirmed chondrosarcoma).
Differential Diagnosis
Multiple Cartilage Lesion Syndromes
| Syndrome | Cartilage Lesions | Other Features | Malignancy Risk |
|---|---|---|---|
| Ollier disease | Multiple enchondromas, unilateral | Deformities, NO hemangiomas | 25-30% chondrosarcoma |
| Maffucci syndrome | Multiple enchondromas | Soft tissue hemangiomas present | Nearly 100% (chondrosarcoma + angiosarcoma) |
| Metachondromatosis | Enchondromas + osteochondromas | Autosomal dominant, PTPN11 mutation | Low malignancy risk |
| Multiple osteochondromas | Osteochondromas only (NO enchondromas) | Autosomal dominant, EXT1/EXT2 | 1-5% malignant transformation |
Key Differentiators
Ollier vs Maffucci: Look for soft tissue hemangiomas (visible, compressible masses). If present, it's Maffucci with nearly 100% malignancy risk. If absent, it's Ollier with 25-30% risk.
Enchondromas vs Osteochondromas: Enchondromas are INTRAMEDULLARY (inside bone) with rings-and-arcs calcification. Osteochondromas are SURFACE lesions (exostoses) with cartilage cap pointing away from joint. Metachondromatosis has BOTH types.
Ollier vs Metachondromatosis: Metachondromatosis is autosomal dominant (family history), has both enchondromas and osteochondromas, and has MUCH lower malignancy risk than Ollier.
Management Algorithm
Lifelong Surveillance Protocol
Goal: Early detection of malignant transformation to enable limb-salvage surgery and improve survival.
Annual Surveillance Visit
- Pain assessment: Any new pain in any lesion? Character, duration, severity
- Functional change: New weakness, limited motion, gait change?
- Visible changes: New masses, enlarging lesions?
- Constitutional symptoms: Weight loss, fatigue, night sweats?
- Fractures: Any new pathological fractures since last visit?
- Inspect all limbs: Look for new deformities, masses, asymmetry
- Palpate all accessible lesions: Check for tenderness (RED FLAG)
- Measure limb lengths: Document progression of discrepancy
- Assess deformities: Angular deformities, rotational abnormalities
- Check hemangiomas: In Maffucci, assess for changes (angiosarcoma)
- X-rays: Any symptomatic areas or areas of concern on exam
- MRI: LOW threshold - any painful lesion or palpable change
- Comparison: Compare to previous imaging for subtle growth
- CT chest: If chondrosarcoma suspected (staging)
- Warning signs: Teach patient red flags (pain, swelling, growth)
- Self-examination: How to palpate accessible lesions monthly
- Urgent reporting: Instruct to report new symptoms immediately
- Prognosis: Honest discussion of malignancy risk
Surveillance Saves Lives
Early detection of malignant transformation is CRITICAL. Studies show that chondrosarcomas detected early (small size, no metastases) have 90% 5-year survival with wide excision. Late detection (large size, metastatic) has under 30% survival. Aggressive surveillance and low threshold for MRI/biopsy are essential.
Surveillance Imaging Schedule
Recommended Imaging Frequency
| Patient Age | Baseline Imaging | Follow-up Imaging | Indications |
|---|---|---|---|
| Under 18 years | Skeletal survey at diagnosis | Repeat skeletal survey every 2-3 years | Monitor growth, detect new lesions |
| 18-40 years | Update skeletal survey if not recent | X-rays of symptomatic areas annually | Peak age for malignant transformation |
| Over 40 years | Skeletal survey if new symptoms | MRI any new pain or growth immediately | Very high suspicion for malignancy |
This completes the surveillance section.
Surgical Technique
Surgical Indications
Indications for Surgery
- Pathological fracture (after healing for curettage)
- Symptomatic lesions causing pain or dysfunction
- Angular deformity affecting function
- Limb length discrepancy greater than 2cm
- Suspected malignant transformation
- Cosmetically unacceptable deformity
Contraindications/Caution
- Asymptomatic lesions (surveillance preferred)
- Active malignancy without staging workup
- Poor soft tissue envelope
- Multiple procedures planned (stage appropriately)
- Growing skeleton (consider timing)
Curettage and Bone Grafting
Standard Curettage Technique
| Step | Technique | Key Points |
|---|---|---|
| Exposure | Adequate cortical window for complete visualization | Window 2/3 length of lesion, hinge on one side for closure |
| Curettage | Systematic removal of all cartilaginous tissue | Start centrally, work to periphery; curettes of various sizes |
| Extended curettage | High-speed burr to remove residual tissue | Extends margins 1-2mm into normal bone |
| Adjuvant (if needed) | Phenol, hydrogen peroxide, or cryotherapy | For aggressive lesions or recurrences; protect soft tissues |
| Bone grafting | Fill defect with autograft, allograft, or substitute | Autograft preferred for large defects; calcium phosphate for small lesions |
| Stabilization | Internal fixation if fracture risk high | Prophylactic plating for large defects in weight-bearing bones |
Hand Enchondroma Surgery
Phalangeal/Metacarpal Technique
- Incision: Dorsal longitudinal or mid-lateral
- Window: Rectangular cortical window (preserve for closure)
- Curettage: Complete removal with small curettes
- Grafting: Often not required for small defects (fibrous healing)
- Fixation: K-wire only if unstable fracture
- Early motion: Begin at 2-4 weeks
Special Considerations
- Multiple lesions: Stage surgeries 6-8 weeks apart
- Pathological fracture: Allow healing (4-6 weeks) before curettage
- Digital nerve: Protect during exposure
- Tendon adherence: Meticulous soft tissue handling
- No adjuvant: Rarely needed in hand
Deformity Correction
Angular Deformity Management
| Deformity Type | Procedure | Timing Considerations |
|---|---|---|
| Mild varus/valgus (less than 15°) | Guided growth with 8-plate if growing | Remove at skeletal maturity or correction |
| Moderate deformity (15-30°) | Acute corrective osteotomy | Wait until near skeletal maturity if possible |
| Severe deformity (greater than 30°) | Gradual correction with external fixator | Taylor Spatial Frame or Ilizarov |
| Combined angular + length | Osteotomy with lengthening | Address both simultaneously with circular fixator |
Limb Length Discrepancy Management
Epiphysiodesis
- Indication: Predicted discrepancy 2-5cm at maturity
- Timing: Based on growth remaining (Paley multiplier)
- Technique: Percutaneous drill or 8-plate
- Advantage: Simple, outpatient procedure
- Limitation: Cannot correct existing discrepancy
Limb Lengthening
- Indication: Discrepancy greater than 5cm or skeletal maturity
- Rate: 1mm/day (0.25mm x 4 increments)
- External fixator: Ilizarov or TSF
- Internal lengthening nail: PRECICE, FITBONE
- Consolidation index: ~36 days/cm
Malignant Transformation
Any lesion with pain at rest, rapid growth, cortical destruction, or soft tissue mass requires biopsy BEFORE definitive surgery. Suspected chondrosarcoma needs wide resection, NOT curettage.
Complications and Outcomes
Disease-Related Complications
Major Complications in Enchondromatosis
| Complication | Incidence | Impact | Management |
|---|---|---|---|
| Malignant transformation | 25-30% Ollier, 100% Maffucci | Life-threatening, requires wide excision | Surveillance, early detection, wide resection |
| Pathological fracture | 30-40% of patients | Pain, disability, may require surgery | Immobilize, heal, then curettage and graft |
| Limb length discrepancy | 60-70% with lower limb involvement | Gait abnormality, back pain, cosmetic | Epiphysiodesis or lengthening |
| Angular deformity | 40-50% with metaphyseal lesions | Joint malalignment, arthritis risk | Guided growth or corrective osteotomy |
| Functional impairment | Variable (20-80%) | Limited activities, reduced quality of life | Physiotherapy, adaptive equipment, surgery |
Treatment-Related Complications
Curettage Complications
- Recurrence: 5-15% after curettage (incomplete removal)
- Re-fracture: 5-10% if large defect not adequately grafted
- Infection: 2-3% (standard surgical site infection risk)
- Stiffness: 10-20% in hand surgery without early mobilization
Reconstruction Complications
- Allograft nonunion: 10-20% at host-graft junction
- Allograft fracture: 5-10% years after surgery
- Prosthetic loosening: 5-10% at 10 years for endoprosthesis
- Infection: 5-15% for major reconstructions
- Limb length discrepancy: May persist after reconstruction
Long-Term Outcomes
Quality of Life Considerations
Enchondromatosis patients face lifelong challenges:
Physical: Multiple surgeries (fractures, deformities, malignancy), chronic pain, functional limitations, cosmetic concerns.
Psychological: Anxiety about cancer risk, depression from chronic illness, body image issues, social isolation.
Social: Missed school/work for appointments and surgeries, financial burden of lifelong care, relationship challenges.
Management: Multidisciplinary approach including orthopedic surgery, oncology, physiotherapy, psychology, genetic counseling, and social work. Patient support groups valuable.
Postoperative Care
Post-Curettage Care
Recovery Protocol After Curettage
| Phase | Duration | Key Activities | Precautions |
|---|---|---|---|
| Immediate | 0-2 weeks | Wound care, pain control, elevation | Restrict weight-bearing if lower limb |
| Early mobilization | 2-6 weeks | Gentle ROM exercises, edema control | Avoid heavy lifting; protect surgical site |
| Progressive loading | 6-12 weeks | Gradual return to activity, physiotherapy | Serial X-rays to confirm graft incorporation |
| Full recovery | 12+ weeks | Return to full activities, sport | Ongoing surveillance for recurrence |
Hand Surgery Rehabilitation
Early Phase (0-4 weeks)
- Week 1: Bulky dressing, elevation, finger ROM out of splint
- Week 2: Remove bulky dressing, begin active exercises
- Week 3-4: Gentle grip strengthening, scar massage
- Splinting: Volar resting splint at night only if needed
- Edema control: Coban wrap, elevation, retrograde massage
Late Phase (4-12 weeks)
- Week 4-6: Progressive strengthening, putty exercises
- Week 6-8: Return to light work activities
- Week 8-12: Full return to sport/manual work
- Follow-up: Radiographs at 6 weeks, 3 months, 6 months
- Recurrence watch: Any pain, swelling, or new deformity
Weight-Bearing Progression
Post-Curettage Weight-Bearing Protocol
| Site | Initial | Progression | Full WB |
|---|---|---|---|
| Upper extremity | Sling comfort only | Immediate ROM | 2-4 weeks |
| Femur/Tibia (small lesion) | Touch-down WB | Progressive at 4-6 weeks | 6-8 weeks |
| Femur/Tibia (large lesion/plate) | Non-weight bearing | TDWB at 6 weeks | 8-12 weeks |
| Foot (metatarsal/phalanx) | Heel walking/cast boot | Progressive at 4 weeks | 6-8 weeks |
Surveillance Protocol
Imaging Schedule
- Post-op X-ray: Immediate (baseline)
- 6 weeks: Confirm healing, graft incorporation
- 3 months: Assess for recurrence
- 6 months: Check remodeling
- Annually: Lifelong (malignancy surveillance)
- MRI: If pain or suspicious changes
Clinical Assessment
- Wound healing: Complete by 2 weeks
- Pain: Should improve progressively
- Function: Full ROM by 6-8 weeks (hand)
- Red flags: Night pain, new mass, rapid growth
- Other lesions: Monitor all known enchondromas
Patient Education
Patients and families must understand that enchondromatosis requires LIFELONG follow-up even after successful surgery. New lesions can develop, existing lesions can recur, and malignant transformation remains a risk throughout life.
Outcomes
Overall Prognosis
Surgical Outcomes by Procedure
Outcomes After Common Procedures
| Procedure | Success Rate | Recurrence | Key Outcomes |
|---|---|---|---|
| Hand enchondroma curettage | 95%+ | 5-10% | Excellent function, minimal complications |
| Long bone curettage | 85-90% | 10-15% | Good results; may need repeat surgery |
| Corrective osteotomy | 80-90% | N/A | Deformity correction achieved; may lose correction with growth |
| Epiphysiodesis (LLD) | 90%+ | N/A | Predictable if timed correctly |
| Limb lengthening | 70-85% | N/A | Good outcomes but high complication rate (30-50%) |
| Wide resection (chondrosarcoma) | Variable | 10-20% | Depends on grade, margins, and metastatic status |
Functional Outcomes
Upper Limb Function
- Hand: Generally excellent after isolated curettage
- DASH scores: Near normal with single lesions
- Multiple lesions: May have residual weakness
- Work capacity: Usually maintained
- Fine motor: Preserved unless multiple digit involvement
Lower Limb Function
- Ambulation: Most achieve community ambulation
- Leg length discrepancy: Managed with shoe raise or surgery
- Hip/Knee function: Depends on juxta-articular involvement
- Sport: Often modified activities recommended
- Walking aids: Required in 10-20% with severe disease
Quality of Life Factors
Physical Aspects
- Multiple surgeries (average 3-5 over lifetime)
- Chronic pain in 20-40% of patients
- Functional limitations in severe cases
- Cosmetic concerns (limb asymmetry, scars)
- Fatigue from chronic disease burden
Psychosocial Aspects
- Cancer anxiety (lifelong malignancy risk)
- Body image issues (especially adolescents)
- Educational/vocational impact
- Healthcare burden (frequent appointments)
- Financial impact of lifelong care
Evidence Base and Key Studies
Discovery of IDH Mutations in Enchondromatosis
- Somatic heterozygous IDH1 (R132C, R132H) or IDH2 (R172S) mutations identified in 87% of enchondromas and 70% of spindle cell haemangiomas
- Across the cohort, 81% of Ollier disease and 77% of Maffucci syndrome subjects carried IDH1 (98%) or IDH2 (2%) mutations in their tumours
- Immunohistochemistry suggested intraneoplastic and somatic mosaicism, explaining the sporadic, non-hereditary, mosaic distribution
- IDH1 mutations were associated with DNA hypermethylation and downregulated gene expression (epigenetic dysregulation)
- Mutations were also detected in 40% of solitary central cartilage tumours and in chondrosarcoma cell lines
Incidence and Predictors of Chondrosarcoma in Ollier/Maffucci
- International multicentre study of 161 patients (144 Ollier, 17 Maffucci) from 13 European centres and one national databank
- Overall observed incidence of secondary chondrosarcoma was 40% (likely higher as a lifelong, age-dependent risk)
- Risk varied by distribution: 15% for hand/foot-only disease (group I) versus 43-46% when long/flat bones were involved (groups II-III)
- Pelvic enchondromas markedly increased chondrosarcoma risk (odds ratio 3.8, p = 0.001)
- Patients with long-bone or axial (especially pelvic) enchondromas were identified as the group needing regular screening
Maffucci Syndrome - Functional and Neoplastic Significance
- Case report and review of the world literature on Maffucci syndrome from its original description onward
- Documented frequent malignant transformation, including chondrosarcoma arising from enchondromas
- Highlighted association with non-skeletal malignancies including ovarian neoplasms and other primary tumours
- Emphasised the markedly elevated lifelong malignancy risk that distinguishes Maffucci from Ollier disease
- Reinforced that spindle cell (cutaneous/soft tissue) haemangiomas are the pathognomonic feature of Maffucci syndrome
Curettage and Adjuvant for Low-Grade (Grade 1) Chondrosarcoma
- Retrospective series of 113 patients with low-grade (grade 1 / atypical cartilaginous) chondrosarcoma of the appendicular skeleton
- Treated with extended curettage, liquid-nitrogen cryoadjuvant, polymethylmethacrylate cement filling and prophylactic fixation
- Local recurrence occurred in only 3 patients (2.7%) at a mean follow-up of 110 months
- Non-oncological complications in 5.3%; mean MSTS functional score 95% with no metastases or disease-related mortality
- Grade 1 chondrosarcoma (in non-syndromic appendicular sites) can be controlled with joint-sparing intralesional surgery
Metachondromatosis is Caused by Germline PTPN11 Mutations
- Whole-genome sequencing of a single proband plus linkage analysis identified the metachondromatosis gene
- An 11-bp frameshift deletion in exon 4 of PTPN11 segregated with the phenotype
- A second family carried an independent exon 4 nonsense mutation, confirming PTPN11 loss-of-function as causal
- No protein-truncating PTPN11 variants were found in 469 controls, supporting pathogenicity
- Metachondromatosis (OMIM 156250) is an autosomal dominant disorder, genetically distinct from IDH-driven Ollier/Maffucci
Ivosidenib (Mutant IDH1 Inhibitor) in Advanced Chondrosarcoma
- Phase I multicentre dose-escalation/expansion study of oral ivosidenib monotherapy in 21 patients with advanced IDH1-mutant chondrosarcoma
- Toxicity was mostly grade 1-2; only one grade 3 or higher event (hypophosphataemia) was treatment related
- Plasma 2-hydroxyglutarate fell substantially in all patients (14-94%), to levels seen in healthy individuals
- Median progression-free survival was 5.6 months with a 6-month PFS rate of 39.5%
- 11 of 21 patients (52%) achieved stable disease, supporting targeting of the IDH/2-HG axis
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: New Diagnosis of Ollier Disease
"A 7-year-old girl presents with limb length discrepancy (left leg 3cm shorter than right). X-rays show multiple enchondromas in the left femur, tibia, and foot. Right leg is normal. Parents ask about diagnosis and prognosis. What is your diagnosis and how do you counsel the family?"
Scenario 2: Suspected Malignant Transformation
"A 32-year-old woman with known Ollier disease presents with 3 months of progressive right groin pain. She has multiple enchondromas in the right femur documented since childhood. X-ray shows 8cm lesion in proximal femur with cortical thinning. MRI shows heterogeneous T2 signal with small soft tissue component. How do you proceed?"
Scenario 3: Maffucci Syndrome with Dual Malignancy Risk
"A 28-year-old man with Maffucci syndrome (multiple enchondromas plus hemangiomas) presents for annual surveillance. He is asymptomatic. Physical exam reveals stable enchondromas in hands and feet, but one hemangioma on his left calf has doubled in size over 6 months and feels firm. How do you manage this patient?"
MCQ Practice Points
Clinical Pearl
Q: What is the difference between Ollier disease and Maffucci syndrome?
A: Both are non-hereditary enchondromatosis syndromes. Ollier disease: Multiple enchondromas with asymmetric distribution, typically unilateral predominance; No associated soft tissue lesions. Maffucci syndrome: Multiple enchondromas PLUS soft tissue hemangiomas (venous malformations, phleboliths on X-ray). Maffucci has higher malignancy risk (40-50% vs 25-30% for Ollier). Both present in childhood with limb deformity, shortening, and pathological fractures.
Clinical Pearl
Q: What is the malignancy risk in Ollier disease and how do you monitor for malignant transformation?
A: Lifetime chondrosarcoma risk is 25-30% (much higher than solitary enchondroma which is less than 1%). Warning signs for transformation: New or increasing pain (especially at rest); Rapid growth on serial imaging; Size greater than 5cm; Soft tissue mass on MRI; Cortical destruction. Surveillance: Clinical review annually; Imaging of symptomatic lesions; Low threshold for biopsy/resection of suspicious lesions. Transformation usually occurs in adulthood (3rd-4th decade).
Clinical Pearl
Q: What are the clinical features and natural history of Ollier disease?
A: Presents in early childhood (first decade) with limb shortening, angular deformity, and palpable bony swelling. Typically asymmetric distribution, often with unilateral predominance. Common sites: hands, feet, long bones. Complications: Pathological fractures (heal normally); Progressive deformity; Limb length discrepancy. Natural history: Lesions may stabilize after skeletal maturity but remain at risk for malignant transformation throughout life.
Clinical Pearl
Q: What is the typical imaging appearance of enchondromas in Ollier disease?
A: Multiple well-defined lytic lesions with chondroid matrix (rings and arcs calcification). Distribution: Metaphyseal, extending toward physis in immature skeleton. May cause expansion and cortical thinning without destruction. Characteristic: Streaky or columnar appearance extending from physis (reflecting origin from growth plate cartilage). MRI: High T2 signal (cartilage), lobular architecture. CT best for matrix calcification and cortical integrity assessment.
Clinical Pearl
Q: How is limb deformity and length discrepancy managed in Ollier disease?
A: Conservative: Shoe lifts for mild LLD (less than 2cm). Surgical options: (1) Epiphysiodesis of contralateral limb for moderate LLD; (2) Lengthening procedures (distraction osteogenesis) for severe LLD; (3) Corrective osteotomy for angular deformity; (4) Curettage and grafting for symptomatic lesions. Timing: Defer elective surgery until skeletal maturity if possible due to high recurrence risk in immature skeleton. Amputation rarely needed but considered for severe, recurrent deformity.
Guidelines, Registries & Global Practice
Global Epidemiology
Enchondromatosis is rare and almost universally sporadic. Ollier disease has an estimated prevalence in the order of 1 in 100,000, and Maffucci syndrome is considerably rarer. Both are caused by post-zygotic somatic mosaic IDH1/IDH2 mutations and are therefore non-hereditary, with the same mutational spectrum seen worldwide (no consistent ethnic or geographic predilection). According to PubMed, in the largest international multicentre series (161 patients across 13 European centres) the cross-sectional incidence of secondary chondrosarcoma was 40%, rising with long-bone, flat-bone and especially pelvic involvement (Verdegaal et al, The Oncologist 2011) DOI. The defining IDH1/IDH2 mutation prevalence of 87% in enchondromas is consistent across populations (Pansuriya et al, Nature Genetics 2011) DOI.
Guideline & Society Guidance (Side-by-Side)
There is no disease-specific international guideline for enchondromatosis; management is extrapolated from cartilage-tumour and sarcoma frameworks. The table summarises how the major bodies frame the relevant cartilage-tumour pathway.
How Major Bodies Frame Cartilage-Tumour / Chondrosarcoma Care
| Body (region) | Relevant Guidance | Evidence Level |
|---|---|---|
| ESMO / EURACAN (Europe) | Bone sarcoma guideline: suspected chondrosarcoma referred to a sarcoma reference centre before biopsy; grade 1 / atypical cartilaginous tumour of long bones may be managed by curettage, higher-grade by wide resection; chondrosarcoma is chemo/radio-resistant | Expert consensus, graded recommendations |
| NICE / BSG (UK) | Suspected sarcoma referral pathways and specialist MDT (sarcoma advisory group) review; imaging-led triage with biopsy only after staging at the treating centre | Guideline-based pathway |
| NCCN (USA) | Bone cancer guideline: multidisciplinary management at sarcoma centres, wide excision for conventional chondrosarcoma, active surveillance or intralesional surgery for atypical cartilaginous tumour of the appendicular skeleton | Category 2A consensus |
| AOA / ANZ sarcoma groups (Australasia) | Centralised referral of suspected primary bone sarcoma to designated sarcoma services with MDT governance | Service-standard consensus |
Registry & High-Volume Evidence
What the Cohorts Show
- International EMSOS cohort (n=161): 40% chondrosarcoma incidence; pelvic disease OR 3.8 (Verdegaal 2011)
- Appendicular grade 1 series (n=113): 2.7% local recurrence after extended curettage + cryoadjuvant, MSTS 95% (El Masry 2022)
- Genetic cohorts: IDH1/IDH2 mutations in 87% of enchondromas (Pansuriya 2011)
- No dedicated national enchondromatosis registry exists; data come from sarcoma-centre cohorts and rare-disease networks
Practice Variation
- Curettage vs wide resection for grade 1 lesions varies by centre and remains debated, but appendicular tumours are increasingly managed by joint-sparing surgery
- Surveillance intensity is non-standardised; most centres favour risk-stratified imaging (more aggressive for pelvic/long-bone and Maffucci disease)
- Genetic testing is performed on affected tissue (not blood), reflecting somatic mosaicism, but is not uniformly available
- Centralisation: high-income systems centralise sarcoma care; access and timeliness vary in lower-resourced settings
Referral, Genetic & Support Services (Australian Context)
Enchondromatosis is rare in Australia (broadly consistent with the global 1 in 100,000 order for Ollier disease). Initial diagnosis is typically at major paediatric hospitals (Royal Children's Hospital Melbourne, Sydney Children's Hospital, Queensland Children's Hospital), with lifelong surveillance coordinated through tertiary sarcoma services and multidisciplinary tumour boards (for example Peter MacCallum Cancer Centre, Chris O'Brien Lifehouse and other ANZ sarcoma services). Every suspected chondrosarcoma should be referred to a designated sarcoma centre before biopsy. Genetic counselling is available at major hospitals to explain the sporadic, non-hereditary nature of the disease, and rare-disease and limb-difference support organisations (such as Rare Voices Australia and limb-difference charities) provide patient resources alongside psychological support services.
ENCHONDROMATOSIS - OLLIER DISEASE AND MAFFUCCI SYNDROME
Clinical summary
Key Definitions
- •**Ollier disease**: Multiple unilateral enchondromas, sporadic, 25-30% malignancy risk
- •**Maffucci syndrome**: Enchondromas PLUS hemangiomas, nearly 100% malignancy risk
- •**IDH1/IDH2 somatic mutations**: Found in 87% of lesions, NOT inherited
- •**Chondrosarcoma**: Malignant cartilage tumor from enchondroma transformation
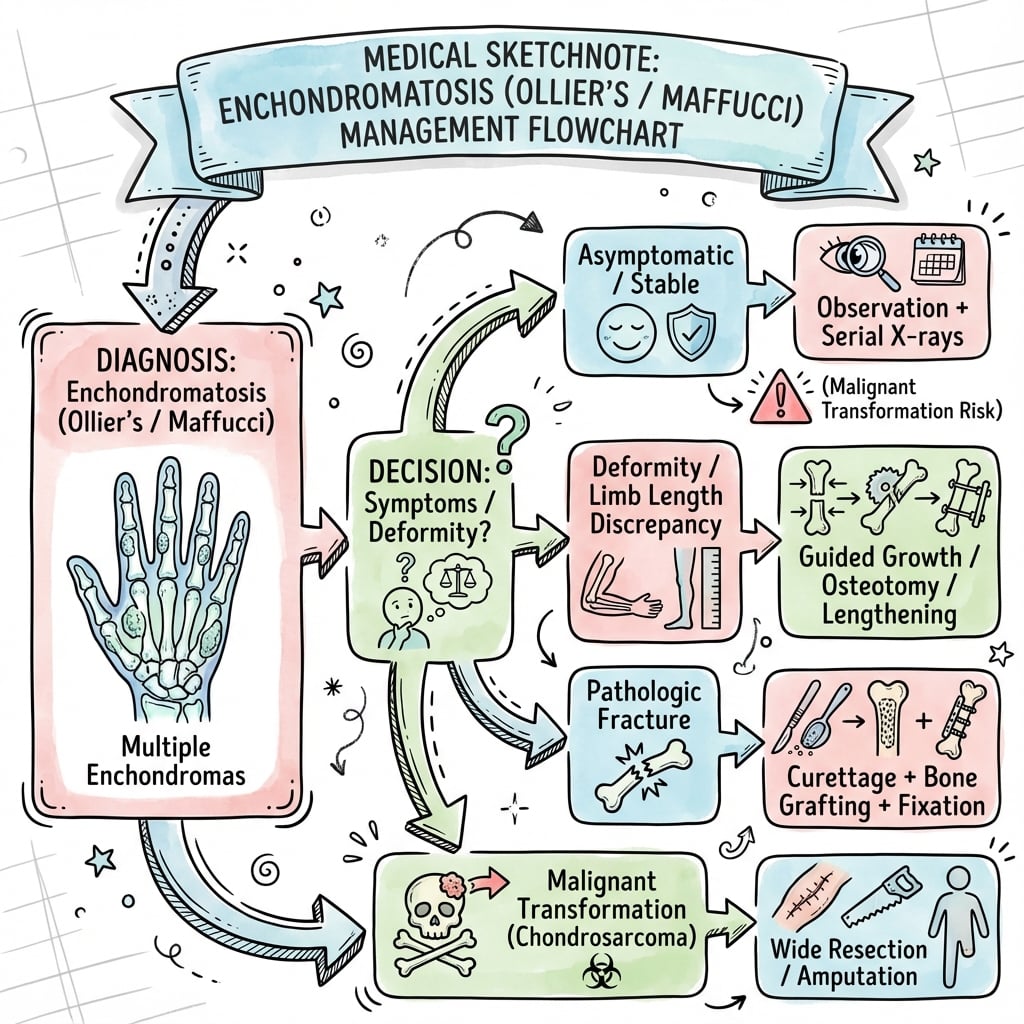
Clinical Presentation
- •Childhood: limb deformity, limb length discrepancy, palpable masses
- •Adolescence: pathological fractures, progressive deformities
- •Adulthood: pain in lesion (RED FLAG for malignancy), soft tissue mass
- •Maffucci: visible hemangiomas (soft compressible masses)
Diagnosis
- •**Skeletal survey**: Document all lesions at baseline (X-rays all limbs)
- •**MRI**: For large proximal lesions and any symptomatic lesion
- •**X-ray features**: Multiple enchondromas, rings-and-arcs calcification, unilateral
- •**Genetic testing**: IDH1/IDH2 mutation testing available but not routine
Red Flags for Malignancy
- •**Pain without trauma** - most important clinical sign (90% sensitivity)
- •Progressive enlargement on serial imaging
- •Soft tissue mass on MRI (highly specific for chondrosarcoma)
- •Cortical breakthrough on CT, lesion size over 5cm
Surveillance Protocol
- •**Annual clinical exam**: Check for pain, masses, deformities
- •**Skeletal survey**: Repeat every 2-3 years in childhood
- •**Low threshold for MRI**: Any painful lesion gets MRI immediately
- •**Biopsy if suspicious**: CT-guided with excisable trajectory
Management of Deformities
- •**Limb length discrepancy**: Epiphysiodesis (2-5cm) or lengthening (over 5cm)
- •**Angular deformity**: Guided growth or corrective osteotomy
- •**Pathological fracture**: Immobilize, heal, delayed curettage and graft
- •**MRI before elective surgery**: Rule out malignancy before deformity correction
Malignancy Treatment
- •**Chondrosarcoma**: Wide excision with 5-10mm margins (curettage inadequate)
- •**Reconstruction**: Allograft, endoprosthesis, or allograft-prosthetic composite
- •**Angiosarcoma (Maffucci)**: Wide excision, often requires amputation
- •**No chemo/radiation**: Chondrosarcoma does NOT respond; surgery only curative
Prognosis
- •**Ollier malignancy risk**: 25-30% develop chondrosarcoma by age 40
- •**Maffucci malignancy risk**: Nearly 100% lifetime (chondrosarcoma + angiosarcoma)
- •**Chondrosarcoma survival**: 90% 5-year for Grade 1 with wide excision
- •**Surveillance benefit**: Early detection enables limb salvage and better survival