Small Round Cell Tumor | Second Most Common Pediatric Bone Malignancy | Multimodal Treatment Required
- Second most common primary bone malignancy in children (after osteosarcoma)
- EWS-FLI1 translocation t(11;22) present in 85% - diagnostic hallmark
- Onion-skin periosteal reaction classic radiographic finding
- Multimodal treatment mandatory: chemotherapy + surgery ± radiation
- Poor response to chemotherapy (under 90% necrosis) is worst prognostic factor
- “Fever and elevated inflammatory markers mimic infection - biopsy essential
- “VDC-IE protocol: Vincristine, Doxorubicin, Cyclophosphamide alternating with Ifosfamide, Etoposide
- “Surgical margins more important than degree of necrosis for local control
- “Metastases to lung, bone, bone marrow - whole-body staging required
t(11;22) translocation creating EWS-FLI1 fusion. Present in 85% of cases. Small round blue cells on histology with CD99 strong diffuse membrane staining.
Adolescent with painful diaphyseal lesion, fever, elevated ESR. Mimics osteomyelitis. Femur and pelvis most common sites (60% of cases).
Neoadjuvant chemotherapy first, then surgery. VDC-IE protocol for 14-17 cycles. Surgery or radiation for local control. Response to chemo predicts survival.
Tumor volume under 200ml, under 90% necrosis post-chemo, metastases at presentation. 5-year survival: 70% localized, 30% metastatic.
- Staging
- IB or IIB, over 90% necrosis
- Treatment
- Wide excision + reconstruction
- Key Pearl
- Limb salvage in 85% - margins matter more than necrosis
- Staging
- IIB extracompartmental
- Treatment
- Chemotherapy + radiation (surgery if resectable)
- Key Pearl
- Radiation for unresectable sites - 55.8 Gy standard dose
- Staging
- Stage III with lung mets
- Treatment
- Intensive chemotherapy + local control + lung surgery
- Key Pearl
- Whole lung radiation if unresectable - survival drops to 30%
VDC-IEVDC-IE Chemotherapy Protocol
Hook:VDC-IE cycles: VDC for cycles 1,3,5 then IE for cycles 2,4,6 - alternating reduces resistance!
Overview and Epidemiology
Ewing sarcoma is the second most common primary bone malignancy in children and adolescents (after osteosarcoma), representing 10-15% of all primary bone tumors. It is a highly aggressive small round cell tumor that requires urgent multimodal treatment. Before the advent of chemotherapy in the 1970s, 5-year survival was under 10%. Modern protocols combining chemotherapy, surgery, and radiation have improved survival to 70% for localized disease.
- Peak age: 10-20 years (75% of cases)
- Second peak: 20-30 years (15% of cases)
- Rare over age 30: 10% of cases
- Gender: Male greater than Female (1.5:1 ratio)
- Race: 85% white, rare in African/Asian populations
- Femur: 25% (most common single site)
- Pelvis: 20% (worst prognosis due to size)
- Tibia/fibula: 15%
- Humerus: 10%
- Ribs: 10%
- Axial skeleton: 20% (vertebrae, scapula)
The diaphysis of long bones is involved in 90% of extremity cases, distinguishing Ewing from osteosarcoma (which favors metaphysis). Pelvic tumors are often large at presentation due to deep location and delayed symptoms.
Although this topic centres on bone, true Ewing sarcoma is one member of the Ewing sarcoma family of tumours (ESFT) — a group unified by the same EWSR1-ETS fusion (and the same CD99/NKX2-2 phenotype) regardless of where it arises. The members are skeletal Ewing sarcoma, extraskeletal (extraosseous) Ewing sarcoma arising primarily in soft tissue with no bone of origin, the Askin tumour (Ewing of the chest wall / thoracopulmonary region), and peripheral primitive neuroectodermal tumour (pPNET), the more neurally-differentiated end of the same spectrum. The practical points: extraskeletal Ewing tends to occur in slightly older patients and in axial / paraspinal / chest-wall sites, it is treated on the same multi-agent chemotherapy backbone as bone Ewing, but local control follows soft-tissue sarcoma surgical principles (wide excision of the soft-tissue mass, with radiotherapy where margins are constrained). The unifying concept for a viva: the Ewing family is defined by its molecular fusion, not by whether it started in bone.
Pathophysiology and Molecular Biology
t(11;22)(q24;q12) translocation creates the EWS-FLI1 fusion oncogene in 85% of Ewing sarcoma cases. The remaining 15% have variant translocations (e.g., EWS-ERG). This fusion protein acts as an aberrant transcription factor, driving uncontrolled proliferation of primitive neuroectodermal cells. FISH or RT-PCR for EWS rearrangement is mandatory for diagnosis - this confirms Ewing sarcoma and distinguishes it from other small round cell tumors.
Primitive neuroectodermal cells (mesenchymal stem cells). Cells are small, round, and blue with high nuclear-to-cytoplasmic ratio. PAS-positive glycogen in cytoplasm. Cells express CD99 (MIC2) strongly - diffuse membrane staining pattern.
Highly aggressive. Permeative growth through bone marrow spaces. Extensive soft tissue extension common. Lytic destruction of cortex with periosteal reaction (onion-skin or sunburst pattern). Early hematogenous spread to lungs, bones, bone marrow.
- Osteosarcoma
- Age: 10-20 years (peak 16)
- Lymphoma
- Age: Bimodal (10-20, over 60)
- Osteosarcoma
- Location: Metaphysis
- Lymphoma
- Location: Metaphysis/diaphysis
- Osteosarcoma
- Histology: Pleomorphic, osteoid production
- Lymphoma
- Histology: Lymphoid cells, CD20/CD3 positive
- Osteosarcoma
- Genetics: Complex karyotype, TP53 mutations
- Lymphoma
- Genetics: Various B/T-cell markers
A small round blue cell tumour that looks like Ewing, and may even be CD99-positive, is not necessarily Ewing. The current WHO classification separates true Ewing sarcoma (defined by an EWSR1-ETS fusion, classically EWS-FLI1) from a group of "Ewing-like" undifferentiated round cell sarcomas that are EWSR1-FISH-negative and driven by different genetics — principally CIC-rearranged sarcomas (usually CIC-DUX4) and BCOR-rearranged sarcomas. This matters because these mimics have variable, patchy CD99, distinct immunoprofiles (CIC sarcomas are often WT1/ETV4-positive; BCOR sarcomas BCOR/SATB2-positive), tend to be more soft-tissue and axial, and carry a worse prognosis with a poorer response to standard Ewing chemotherapy. The exam point answers the classic distractor "small round blue cells but EWSR1-negative (or CD99-negative)" — that tumour is a Ewing-LIKE sarcoma, not Ewing, which is exactly why molecular confirmation of an EWSR1 rearrangement (not CD99 alone) is required before committing a patient to a Ewing protocol.
Classification and Staging
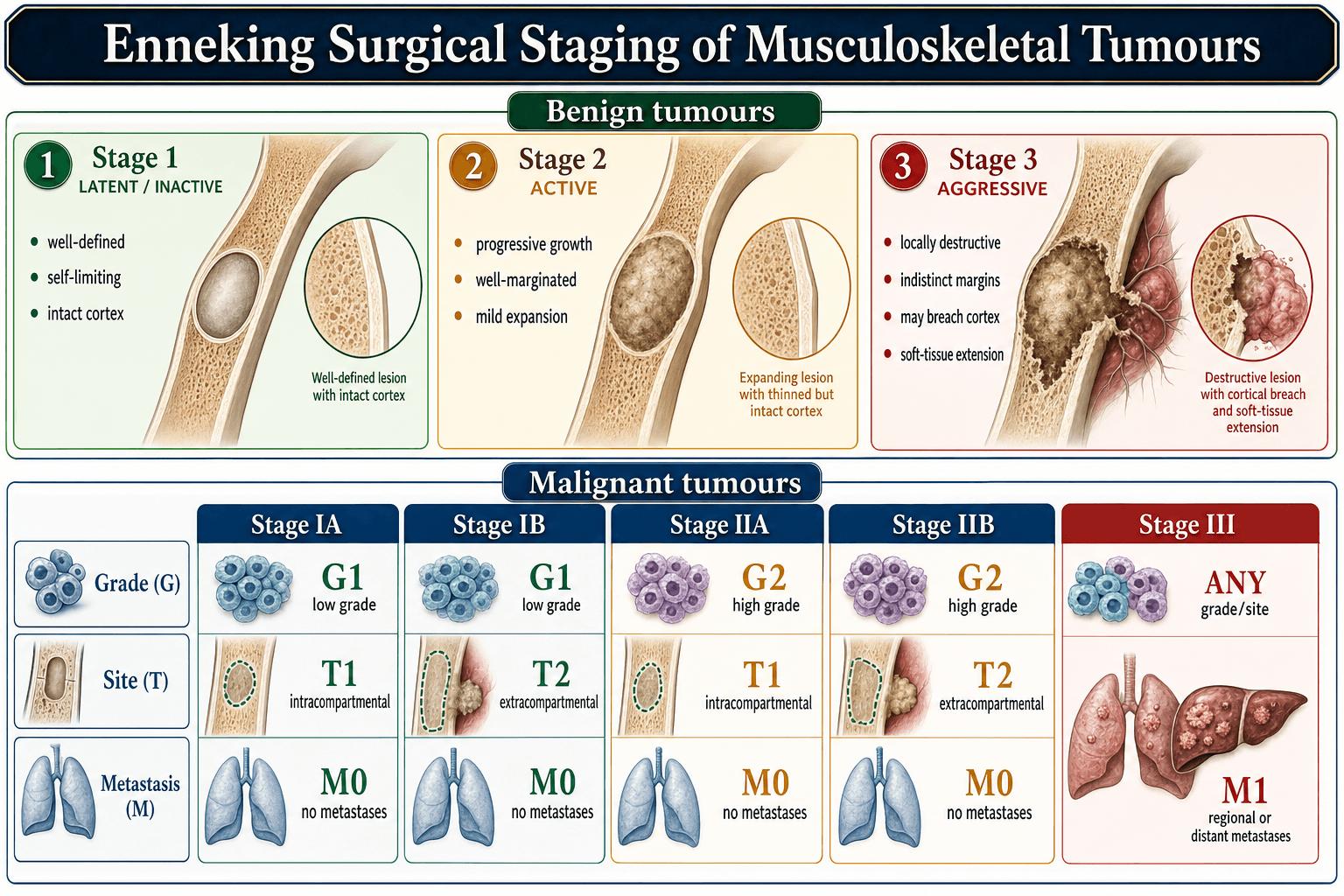
Enneking Surgical Staging System
Gold standard for bone sarcomas. Based on tumor grade, local extent, and metastases.
- Grade
- Low-grade
- Extent
- Intracompartmental
- Metastases
- None
- 5-Year Survival
- Not applicable (Ewing always high-grade)
- Grade
- High-grade
- Extent
- Intracompartmental
- Metastases
- None
- 5-Year Survival
- 70-75%
- Grade
- Low-grade
- Extent
- Extracompartmental
- Metastases
- None
- 5-Year Survival
- Not applicable (Ewing always high-grade)
- Grade
- High-grade
- Extent
- Extracompartmental
- Metastases
- None
- 5-Year Survival
- 65-70%
- Grade
- Any grade
- Extent
- Any extent
- Metastases
- Present (regional or distant)
- 5-Year Survival
- 25-30%
Ewing sarcoma is ALWAYS high-grade, so only stages IB, IIB, and III are relevant.
Intracompartmental: Tumor confined within bone cortex or within a single anatomic compartment (e.g., anterior thigh). Extracompartmental: Tumor extends beyond bone cortex into soft tissues OR crosses anatomic barriers (e.g., joint, neurovascular bundle). Most Ewing sarcomas at presentation are Stage IIB (high-grade, extracompartmental, no metastases).
Clinical Presentation
- Pain: Localized bone pain (90%) - progressive, worse at night
- Swelling: Palpable soft tissue mass (60%)
- Systemic symptoms: Fever (30%), weight loss, malaise
- Duration: Symptoms 2-6 months before diagnosis (average 3 months)
- Trauma history: 30% report antecedent trauma (coincidental, not causative)
- Inspection: Visible swelling, skin erythema, venous distension
- Palpation: Warm, tender mass; soft tissue extension common
- Function: Limp if lower extremity; restricted ROM
- Neurovascular: Usually intact (invasion rare)
- Lymph nodes: Regional nodes rarely involved (unlike soft tissue Ewing)
30% of patients present with fever, elevated WBC, and elevated ESR, leading to initial misdiagnosis as osteomyelitis. Key distinguishing features: Ewing typically has a longer symptom duration (months vs weeks), diaphyseal location (osteomyelitis favors metaphysis), and large soft tissue mass. Always biopsy a suspected infection that does not respond to antibiotics within 48-72 hours.
- Ewing Sarcoma
- Months (average 3)
- Osteomyelitis
- Days to weeks
- Ewing Sarcoma
- Low-grade, intermittent
- Osteomyelitis
- High-grade, persistent
- Ewing Sarcoma
- Diaphysis
- Osteomyelitis
- Metaphysis
- Ewing Sarcoma
- Large, firm
- Osteomyelitis
- Small or absent
- Ewing Sarcoma
- None
- Osteomyelitis
- Improves within 48-72 hours
- Typical age
- 10-20 years
- Distinguishing histology / IHC
- Uniform small round cells, PAS-positive glycogen, strong diffuse membranous CD99, NKX2-2 positive
- Key genetics
- EWSR1-FLI1 t(11;22) (85%); EWSR1-ERG variant
- Typical age
- 10-20 years
- Distinguishing histology / IHC
- Malignant osteoid production by tumour cells; SATB2 positive
- Key genetics
- Complex karyotype, TP53/RB1 alterations
- Typical age
- Bimodal (older adults)
- Distinguishing histology / IHC
- Larger cells, LCA/CD45 positive, CD20 (B) or CD3 (T) positive; CD99 negative
- Key genetics
- Various B/T-cell rearrangements
- Typical age
- Under 5 years
- Distinguishing histology / IHC
- Rosettes, neuropil, PHOX2B / synaptophysin positive; raised urinary catecholamines
- Key genetics
- MYCN amplification
- Typical age
- Children
- Distinguishing histology / IHC
- Rhabdomyoblasts; desmin, myogenin, MyoD1 positive
- Key genetics
- PAX3/7-FOXO1 (alveolar)
- Typical age
- Any
- Distinguishing histology / IHC
- Neutrophilic inflammation, organisms on culture; no clonal tumour cells
- Key genetics
- Not applicable
Investigations
Diagnostic Imaging Protocol
AP and lateral views of affected bone plus joint above and below. Classic findings: Permeative lytic lesion in diaphysis; moth-eaten bone destruction; onion-skin periosteal reaction (lamellated layers); Codman triangle (elevated periosteum); large soft tissue mass. Sunburst pattern less common than osteosarcoma.
Gold standard for local extent. Defines intramedullary involvement, soft tissue extension, neurovascular relationship, skip lesions. Essential for surgical planning. T1: Low signal in marrow. T2: High signal tumor and edema. Contrast: Heterogeneous enhancement of viable tumor.
High-resolution CT chest to detect pulmonary metastases. Present in 15% at diagnosis. Nodules may be small (under 5mm). Follow-up CT every 3 months during treatment.
PET-CT or bone scan to detect skeletal metastases. Bone metastases in 10% at diagnosis. PET-CT also useful for assessing response to chemotherapy (decreased SUV indicates good response).
Bilateral iliac crest marrow aspirate and biopsy to detect marrow involvement (5% at diagnosis). Presence of marrow disease portends poor prognosis (similar to metastatic disease).
Biopsy planning is critical. Perform incisional or core needle biopsy along longitudinal axis of limb, in line with planned surgical incision. Avoid transverse incisions. Contaminated biopsy tract must be excised en bloc with tumor. Send fresh tissue for: 1) Cytogenetics (FISH for EWS rearrangement), 2) Flow cytometry, 3) Microbiology if infection suspected. Coordinate with oncology and pathology before biopsy.
- CBC: Anemia (30%), leukocytosis (25%)
- ESR/CRP: Elevated in 50% (non-specific)
- LDH: Elevated in 60% (prognostic marker)
- Alkaline phosphatase: Normal or mildly elevated
- Renal/hepatic function: Baseline for chemotherapy
- Morphology: Sheets of small round blue cells, uniform size
- PAS stain: Positive for glycogen (diastase-sensitive)
- CD99 (MIC2): Strong diffuse membrane staining (95%)
- Cytogenetics: EWS-FLI1 fusion by FISH or RT-PCR (85%)
- Differential: Negative for LCA (vs lymphoma), desmin (vs rhabdomyosarcoma)


EWINGEwing Sarcoma Diagnostic Features
Hook:EWING cells are small and angry - they look like infection but have the EWS-FLI1 fusion signature!
Management: Multimodal Treatment Paradigm
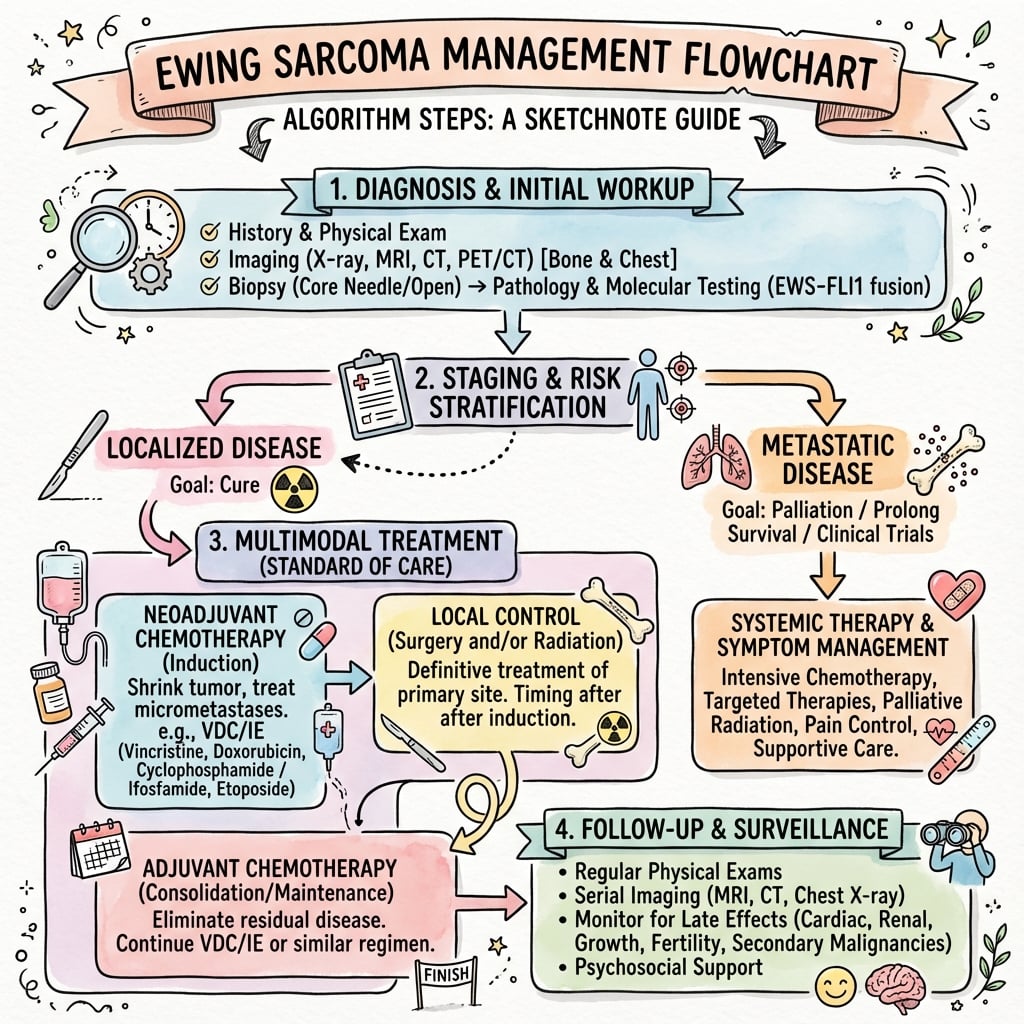
Ewing sarcoma requires neoadjuvant chemotherapy FIRST. Surgery or radiation is performed after 10-14 weeks of induction chemotherapy. This approach: 1) Treats micrometastases early, 2) Reduces tumor size for easier resection, 3) Assesses chemotherapy response (over 90% necrosis = good prognosis). Operating first is a critical error that worsens survival and increases morbidity.
Multimodal Treatment Timeline
Biopsy confirmation. Complete staging (MRI, CT chest, PET-CT, bone marrow biopsy). Multidisciplinary tumor board review. Counsel patient and family. Central line placement.
VDC-IE protocol: Vincristine, Doxorubicin, Cyclophosphamide alternating with Ifosfamide, Etoposide. Typically 5-6 cycles over 10-14 weeks. Monitor for toxicity (cardiotoxicity, hemorrhagic cystitis, neutropenia). Restaging MRI at week 10 to assess response.
Preferred: Wide surgical excision with negative margins. Alternative: Radiation therapy (55.8 Gy) for unresectable tumors (pelvis, spine). Pathology assessment of percent necrosis (over 90% = good responder).
Continue VDC-IE for total of 14-17 cycles (approximately 48 weeks total treatment). If good response (over 90% necrosis): standard protocol. If poor response (under 90% necrosis): consider intensified regimen or clinical trial.
Years 0-2: CT chest and MRI local site every 3 months. Years 2-5: Every 6 months. After 5 years: Annual imaging. Monitor for late effects (cardiac, pulmonary, secondary malignancies).
Standard VDC-IE Protocol
VDC cycles (Weeks 1, 7, 13, etc.):
- Vincristine 2 mg/m² IV (max 2 mg) on Day 1
- Doxorubicin 75 mg/m² IV over 48 hours on Days 1-2
- Cyclophosphamide 1200 mg/m² IV on Day 1
IE cycles (Weeks 4, 10, 16, etc.):
- Ifosfamide 1800 mg/m² IV daily for 5 days (Days 1-5)
- Etoposide 100 mg/m² IV daily for 5 days (Days 1-5)
- Mesna (uroprotection for ifosfamide) 1800 mg/m² IV daily
Total duration: 48 weeks (approximately 14-17 cycles depending on protocol)
Doxorubicin cardiotoxicity: Monitor with ECHO or MUGA at baseline, 6 months, and end of treatment. Cumulative dose limit 450-550 mg/m². Ifosfamide hemorrhagic cystitis: Prevented with mesna (binds acrolein metabolite). Neutropenic fever: G-CSF support. Secondary malignancies: Etoposide increases risk of acute myeloid leukemia (AML) at 2-5 years.
Prognostic Factors
- Favorable
- Localized disease
- Unfavorable
- Metastatic (lung, bone, marrow)
- Impact on 5-Year Survival
- 70% vs 25-30%
- Favorable
- Over 90% necrosis
- Unfavorable
- Under 90% necrosis
- Impact on 5-Year Survival
- 75% vs 50%
- Favorable
- Under 200 ml
- Unfavorable
- Over 200 ml
- Impact on 5-Year Survival
- 70% vs 50%
- Favorable
- Extremity (distal)
- Unfavorable
- Pelvis, axial skeleton
- Impact on 5-Year Survival
- 75% vs 50%
- Favorable
- Under 15 years
- Unfavorable
- Over 15 years
- Impact on 5-Year Survival
- 70% vs 55%
- Favorable
- Normal
- Unfavorable
- Elevated
- Impact on 5-Year Survival
- 70% vs 55%
Over 90% tumor necrosis after neoadjuvant chemotherapy is the single most important modifiable prognostic factor. Patients with over 90% necrosis have 75% 5-year survival vs 50% for under 90% necrosis. This finding guides adjuvant therapy: good responders continue standard protocol, poor responders may be enrolled in intensified regimens or clinical trials. However, surgical margins are more important than necrosis for local control.
Surgical Technique
Principles of Limb Salvage Surgery
- Wide surgical margins (tumor-free tissue surrounding specimen)
- En bloc resection of tumor with intact pseudocapsule
- Reconstruction to restore function
- Facilitate adjuvant chemotherapy (wound healing)
- Intralesional - through tumor (inadequate)
- Marginal - through reactive zone (high recurrence)
- Wide - through normal tissue (goal for cure)
- Radical - entire compartment (rarely needed)
- 10-12 weeks of chemotherapy before surgery
- Shrinks tumor, allows assessment of response
- May convert borderline cases to limb salvage
- Reduces micrometastatic disease
- After recovery from chemotherapy toxicity
- When counts adequate (platelets greater than 100, WBC greater than 3)
- Usually 2-3 weeks after last chemotherapy cycle
- Coordinate with oncology team
Key Surgical Principles
- Biopsy tract must be excised en bloc with specimen
- Prior incisional or needle biopsy site included in resection
- Contaminated tissue must not remain
- 2-3 cm soft tissue margin where possible
- Normal muscle cuff around tumor
- Sacrifice adjacent contaminated structures
- Neurovascular preservation if possible (if not encased)
- Endoprosthetic replacement - modular tumor prostheses
- Allograft reconstruction - structural allograft
- Allograft-prosthetic composite - combination
- Vascularized fibula - for intercalary defects
- Rotationplasty - specialized limb-sparing option
Exam Viva Point: "What are the principles of surgical resection in Ewing sarcoma?" Answer: Wide en bloc resection with 2-3 cm margins. Include biopsy tract. Surgery performed after neoadjuvant chemotherapy (10-12 weeks). Limb salvage possible in 80-90% with modern techniques. Specimen assessed for percent necrosis.
Limb salvage surgery achieves equivalent oncological outcomes to amputation with modern techniques and multimodal therapy.
Complications
Chemotherapy Complications
- Incidence
- 5-10% (clinical), 30% (subclinical)
- Causative Agent
- Doxorubicin (cumulative dose)
- Management
- Baseline and serial ECHO; dexrazoxane cardioprotection; limit cumulative dose
- Incidence
- 10-30% without mesna
- Causative Agent
- Ifosfamide
- Management
- Mesna uroprotection; aggressive hydration; monitor urinalysis
- Incidence
- 40-60%
- Causative Agent
- Myelosuppression (all agents)
- Management
- G-CSF support; prophylactic antibiotics; urgent admission if fever
- Incidence
- 1-2% at 10 years
- Causative Agent
- Etoposide, alkylating agents
- Management
- Long-term surveillance; no prevention available
Surgical Complications
- Incidence
- 5-15%
- Risk Factors
- Chemotherapy-induced neutropenia, endoprosthesis
- Management
- Antibiotics; irrigation and debridement; prosthesis retention vs removal
- Incidence
- 5-10%
- Risk Factors
- Positive margins, poor chemo response
- Management
- Re-excision or radiation; metastatic workup
- Incidence
- Variable
- Risk Factors
- Skeletally immature patients
- Management
- Expandable prosthesis; contralateral epiphysiodesis
Radiation Complications
- Growth arrest: Radiation to growth plates in skeletally immature patients
- Radiation-induced sarcoma: 1-2% at 10 years (latency 5-20 years)
- Pathologic fracture: Radiation-weakened bone (5-10%)
- Soft tissue fibrosis: Chronic pain, reduced ROM
Modern IMRT and proton therapy reduce these complications significantly compared to older techniques.
Postoperative Care
Immediate Postoperative Care
- Closed suction drainage (remove when output less than 30 mL/24h)
- Daily wound inspection for hematoma, infection
- Chemotherapy may delay wound healing
- Avoid tension on closure
- Perioperative antibiotics (24-48 hours)
- Clean dressing technique
- Monitor for signs of infection
- Higher infection risk due to immunosuppression
- Weight-bearing as per reconstruction type
- Range of motion exercises when wound stable
- Physical therapy referral
- Occupational therapy for upper limb tumors
- Protected weight-bearing if endoprosthesis
- May need assistive devices initially
- Progress per surgeon protocol
Coordination with Oncology
- Continue adjuvant chemotherapy 2-4 weeks post-surgery
- When wound healing adequate and counts recovered
- Coordinate timing with oncology team
- Total treatment duration approximately 12 months
- Histopathological analysis of resected tumor
- Percent necrosis reported (response to chemotherapy)
- Margin status documented
- Guides subsequent therapy
Exam Viva Point: "What is the postoperative care after Ewing sarcoma surgery?" Answer: Wound management (higher infection risk). Resume adjuvant chemotherapy within 2-4 weeks when healed. Specimen assessed for percent necrosis (over 90% = good responder). Rehabilitation tailored to reconstruction. Ongoing surveillance for local recurrence and metastasis.
Postoperative care focuses on wound healing, rehabilitation, and seamless transition to adjuvant chemotherapy.
Outcomes
Survival Outcomes
Prognostic Factors
- Good Prognosis
- Localized disease
- Poor Prognosis
- Metastatic disease (worst factor)
- Good Prognosis
- Over 90% necrosis after chemo
- Poor Prognosis
- Under 90% necrosis (poor responder)
- Good Prognosis
- Wide negative margins
- Poor Prognosis
- Positive or marginal margins
- Good Prognosis
- Under 8 cm
- Poor Prognosis
- Over 8 cm
- Good Prognosis
- Extremity (distal)
- Poor Prognosis
- Axial (pelvis, spine)
- Good Prognosis
- Younger patients
- Poor Prognosis
- Older patients (over 18)
Key Outcome Determinants:
- Metastatic disease at presentation is the single worst prognostic factor
- Percent tumor necrosis is the most important modifiable factor
- Surgical margins critical for local control
- Chemotherapy completion essential for systemic control
Exam Viva Point: "What is the prognosis for Ewing sarcoma?" Answer: Localized disease: 70% 5-year survival. Metastatic at diagnosis: 25-30% (worst prognostic factor). Over 90% tumor necrosis post-chemotherapy associated with better outcomes. Complete multimodal therapy (chemo + surgery + radiation) is essential.
With modern multimodal therapy, most patients with localized Ewing sarcoma are cured, but metastatic disease remains a significant challenge.
MELTSEwing Sarcoma Prognosis Factors
Hook:MELTS away your prognosis - avoid these factors!
Guidelines, Registries & Global Practice
Global Epidemiology
Ewing sarcoma is the second most common primary bone malignancy in children and adolescents, with an annual incidence of approximately 1 to 3 per million in populations of European ancestry. It is markedly less common in populations of African and East Asian ancestry, a disparity now attributed in part to germline variation at the EGR2 locus and ancestry-related differences in regulatory microsatellites. Population-based registry data (SEER) confirm a male predominance and a peak in the second decade, and identify pelvic/axial site, tumour size over 8cm, older age and metastatic extent as the principal adverse-risk factors (Shi 2020).
- Local control
- Wide surgical excision preferred; definitive RT for unresectable axial sites; post-op RT for close/positive margins or poor response
- Systemic therapy
- Neoadjuvant VDC-IE, interval-compressed (q2-weekly) for localised disease
- Evidence level
- Category 1 / 2A (RCT-backed)
- Local control
- Surgery where adequate margins achievable; RT for inoperable sites or as adjuvant; combined surgery+RT for marginal margins/poor response
- Systemic therapy
- VIDE / VDC-IE backbone; busulfan-melphalan high-dose consolidation for selected high-risk (EE2008/R2 evidence)
- Evidence level
- Grade A/B
- Local control
- Management exclusively in designated supraregional bone-sarcoma centres; MDT decision on surgery vs RT
- Systemic therapy
- Euro Ewing protocol chemotherapy within national trials
- Evidence level
- Expert consensus + RCT
- Local control
- Treatment at tertiary paediatric/sarcoma centres; surgery preferred, RT for axial sites
- Systemic therapy
- Standard VDC-IE agents within international protocols
- Evidence level
- Consensus / adopted RCT
- Contribution
- Established VDC-IE backbone for localised disease
- Key result
- 5-yr EFS 69% vs 54% with addition of ifosfamide/etoposide
- Contribution
- Established interval compression (q2-weekly)
- Key result
- 5-yr EFS 73% vs 65%; durable at 10 years
- Contribution
- Defined local-control hierarchy
- Key result
- Local failure 7.5% surgery vs 26.3% definitive RT
- Contribution
- Population-level risk stratification
- Key result
- Pelvic site OR 2.49 and size over 8cm OR 1.91 for metastasis
Practice Variation
The principal axis of international variation is high-dose chemotherapy with autologous stem-cell rescue: European protocols (EE2008/R2) incorporate busulfan-melphalan consolidation for selected high-risk localised patients, whereas North American practice has not adopted routine high-dose consolidation. Interval-compressed chemotherapy is standard in paediatric North American practice but is applied more selectively in adults. Relapsed/refractory disease is increasingly managed within the international rEECur platform, which is establishing the most active salvage regimen. Across all systems, care is mandated within designated bone-sarcoma reference centres with a specialist multidisciplinary team (orthopaedic oncologist, paediatric/medical oncologist, radiation oncologist, radiologist, pathologist).
- Histological + molecular confirmation (EWSR1 rearrangement) before starting therapy
- Neoadjuvant chemotherapy before any local treatment
- Biopsy planned by the resecting surgeon (tract excised en bloc)
- Fertility preservation discussed before alkylating chemotherapy
- Informed consent for chemotherapy (cardiotoxicity, hemorrhagic cystitis, infertility, secondary malignancy risks)
- Informed consent for surgery (infection, local recurrence, limb length discrepancy, neurovascular injury)
- Tumor board documentation of treatment plan
- Pathology confirmation of EWS-FLI1 fusion before starting chemotherapy
- Discussion of fertility preservation (sperm banking for males, oocyte preservation for females) before starting chemotherapy - alkylating agents cause infertility
- Long-term surveillance plan documented (cardiac monitoring, secondary malignancy screening)
- Delayed diagnosis (misdiagnosed as osteomyelitis or sports injury)
- Operating before chemotherapy (incorrect sequencing)
- Inadequate surgical margins leading to local recurrence
- Failure to discuss fertility preservation before chemotherapy
MCQ Practice Points
Q: What is the most common chromosomal translocation in Ewing sarcoma? A: t(11;22)(q24;q12) creating the EWS-FLI1 fusion oncogene, present in 85% of cases. The remaining 15% have variant translocations (e.g., EWS-ERG). This fusion is detected by FISH or RT-PCR and is diagnostic for Ewing sarcoma, distinguishing it from other small round cell tumors.
Q: What immunohistochemical marker is most sensitive for Ewing sarcoma? A: CD99 (MIC2) with strong diffuse membrane staining, positive in 95% of Ewing sarcomas. However, CD99 is not entirely specific (can be positive in lymphoblastic lymphoma, synovial sarcoma). The combination of CD99 positivity, PAS-positive glycogen, and EWS-FLI1 fusion confirms the diagnosis.
Q: What is the correct sequence of treatment for localized Ewing sarcoma? A: Neoadjuvant chemotherapy → Local control (surgery or radiation) → Adjuvant chemotherapy. Total treatment duration is approximately 48 weeks. Operating before chemotherapy is a critical error that worsens outcomes by failing to treat micrometastases and assess chemotherapy response.
Q: What is the most important modifiable prognostic factor in Ewing sarcoma? A: Percent tumor necrosis after neoadjuvant chemotherapy. Patients with over 90% necrosis have 75% 5-year survival vs 50% for under 90% necrosis. This finding guides adjuvant therapy intensity. However, surgical margins are more important than necrosis for local control.
Q: How do you differentiate Ewing sarcoma from osteomyelitis clinically? A: Key features: Ewing has longer symptom duration (months vs weeks), diaphyseal location (osteomyelitis favors metaphysis), large soft tissue mass, and no response to antibiotics. Always biopsy a suspected infection that does not improve within 48-72 hours of antibiotics, especially with lytic diaphyseal lesion and soft tissue mass.
Q: What percentage of Ewing sarcoma patients present with metastatic disease, and what are the most common sites? A: 25% present with metastases. Most common sites: Lungs (15%), bone (10%), and bone marrow (5%). Metastatic disease at presentation reduces 5-year survival from 70% to 25-30%. Complete staging includes CT chest, PET-CT or bone scan, and bilateral bone marrow biopsy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old boy presents with a 3-month history of progressive right thigh pain and swelling. He has had intermittent fevers. X-ray shows a permeative lytic lesion in the mid-femoral diaphysis with an onion-skin periosteal reaction and soft tissue mass. ESR is elevated. His GP started him on antibiotics 2 weeks ago with no improvement. What is your assessment and management?”
“A 16-year-old girl with biopsy-proven Ewing sarcoma of the distal femur has completed 14 weeks of VDC-IE chemotherapy. Restaging MRI shows excellent response with 60% reduction in soft tissue mass. The tumor remains 2cm from the distal femoral physis. She is skeletally immature (Risser 2). Discuss your approach to local control.”
“A 17-year-old presents with Ewing sarcoma of the proximal humerus. Staging workup reveals 4 pulmonary nodules (5-12mm) on CT chest and bone marrow involvement (5% tumor cells on bilateral iliac crest biopsy). How would you manage this patient?”
Key Pathology
- EWS-FLI1 fusion t(11;22) in 85% - diagnostic hallmark
- Small round blue cells, PAS-positive glycogen
- CD99 strong diffuse membrane staining (95%)
- High-grade malignancy, early hematogenous spread
Clinical Presentation
- Age 10-20 years, diaphysis of long bones (90%)
- Painful swelling, fever (30%), elevated ESR - mimics infection
- Femur and pelvis most common (60% of cases)
- 25% present with metastases (lung, bone, marrow)
Staging Workup
- MRI local site - assess extent, soft tissue involvement
- CT chest - detect lung metastases (15% at diagnosis)
- PET-CT or bone scan - skeletal metastases (10% at diagnosis)
- Bilateral bone marrow biopsy - marrow involvement (5%)
Treatment Algorithm
- Neoadjuvant chemo FIRST (VDC-IE protocol, 10-14 weeks)
- Local control: Wide excision (preferred) or radiation (55.8 Gy)
- Adjuvant chemo to complete 48 weeks total (14-17 cycles)
- Assess percent necrosis: over 90% = good prognosis
Surgical Pearls
- Limb salvage in 85-90% of extremity tumors
- Wide margins (2cm healthy tissue) more important than necrosis
- Excise biopsy tract en bloc with tumor
- Expandable prosthesis for skeletally immature patients
Prognostic Factors
- Metastases at diagnosis: 70% vs 25-30% survival (localized vs metastatic)
- Over 90% necrosis post-chemo: 75% vs 50% survival
- Tumor volume under 200ml: Better prognosis
- Pelvic tumors: Worse prognosis (large, difficult resection)
Evidence Base and Key Trials
INT-0091 (Grier): Addition of Ifosfamide and Etoposide
- Multi-centre RCT: 518 eligible patients with Ewing sarcoma / PNET of bone
- Standard VACD (vincristine, doxorubicin, cyclophosphamide, dactinomycin) alternating with ifosfamide-etoposide (IE) vs VACD alone
- Non-metastatic disease (n=398): 5-year EFS 69% (IE arm) vs 54% (standard), P=0.005; OS 72% vs 61%, P=0.01
- No benefit from IE in the 120 patients with metastatic disease at diagnosis
CESS/EICESS: Local Therapy in Localised Ewing Tumours (Schuck)
- Pooled analysis of 1058 patients from CESS 81, CESS 86 and EICESS 92 trials
- Local failure: 7.5% after surgery (with or without post-operative RT) vs 26.3% after definitive radiotherapy (P=0.001)
- Pre-operative RT achieved 5.3% local failure (comparable to surgery)
- Irradiated patients were a negatively selected group with unfavourable (axial) sites
AEWS0031 (Womer): Interval-Compressed Chemotherapy
- RCT (Children's Oncology Group): 568 eligible patients with localised Ewing sarcoma randomised to standard (every 21 days) vs interval-compressed (every 14 days) VDC-IE
- 5-year EFS: 73% (compressed) vs 65% (standard), P=0.048
- Toxicity similar between the two arms with filgrastim support
- 10-year follow-up (Cash 2023) confirmed durable benefit: 10-year EFS 70% vs 61%, OS 76% vs 69%, no excess second malignancies
Picci: Chemotherapy-Induced Necrosis as Prognostic Factor
- 118 patients with localised extremity Ewing sarcoma treated with pre-operative chemotherapy then surgery
- Histological grading of response: grade III (no viable tumour) 5-year DFS 95% vs grade II 68% vs grade I (macroscopic viable tumour) 34% (P less than 0.0001)
- Histological response had the strongest correlation with outcome of all parameters tested
- Method identifies poor responders who may benefit from intensified adjuvant therapy
May: EWS-FLI1 is a Transforming Chimeric Transcription Factor
- The t(11;22) translocation fuses the EWS transactivation domain to the FLI1 DNA-binding (ETS) domain
- EWS-FLI1 transformed NIH 3T3 cells (focus formation, anchorage-independent growth) - demonstrating oncogenic activity
- Deletion of either the EWS domain or the FLI1 DNA-binding domain abolished transformation
- Established the molecular mechanism: a chimeric aberrant transcription factor drives tumourigenesis
Shi: Population-Based Risk Factors for Metastasis and Prognosis (SEER)
- Large SEER population-based cohort of Ewing sarcoma patients
- Pelvic primary (OR 2.49) and tumour over 8cm (OR 1.91) independently predicted metastasis at diagnosis
- Worse overall survival with older age, larger size, pelvic site, black race (HR 2.10) and metastatic extent (HR 3.26)
- Chemotherapy was strongly associated with improved survival (HR 0.47)