Quadriceps Tendon | Patellar Tendon | Primary Repair vs Allograft
- Acute rupture (under 6 weeks): Primary repair with Krackow weave - 85-95% success rate
- Chronic rupture (over 6 weeks): Achilles allograft reconstruction - 60-80% success rate
- Gap size threshold: Under 2cm = primary repair, over 2cm = allograft reconstruction
- Patellar height critical: Insall-Salvati ratio 0.8-1.2 - overtightening causes patella baja and stiffness
- Tension setting: Knee in full extension, confirm patellar height on image intensifier
- “Extensor mechanism rupture = inability to perform straight leg raise (pathognomonic)
- “Quadriceps rupture more common in older patients (over 40), patellar tendon in younger (under 40)
- “Primary repair for acute ruptures (under 6 weeks, gap under 2cm) - excellent outcomes
- “Achilles allograft for chronic ruptures (over 6 weeks, gap over 2cm) - good outcomes but lower than primary repair
Inability to perform straight leg raise = complete extensor mechanism rupture. This is pathognomonic. Partial ruptures may have extensor lag (10-90 degrees). Always test straight leg raise in suspected cases.
Acute (under 6 weeks, gap under 2cm): Primary repair with Krackow weave - 85-95% success. Chronic (over 6 weeks, gap over 2cm): Achilles allograft reconstruction - 60-80% success. Timing and gap size determine treatment.
Insall-Salvati ratio 0.8-1.2 - must restore normal patellar height. Overtightening causes patella baja and stiffness. Undertightening causes patella alta and weakness. Set tension with knee in full extension.
Achilles allograft is gold standard - provides calcaneal bone block for tibial tubercle fixation (bone-to-bone healing) and adequate length (15-18cm). Alternative: extensor mechanism allograft for massive defects.
- Location
- Superior to patella
- Age Group
- Over 40 years
- Treatment
- Primary repair (acute) or allograft (chronic)
- Location
- Inferior to patella
- Age Group
- Under 40 years
- Treatment
- Primary repair (acute) or allograft (chronic)
- Location
- Under 6 weeks, gap under 2cm
- Age Group
- Any age
- Treatment
- Primary repair with Krackow weave
- Location
- Over 6 weeks, gap over 2cm
- Age Group
- Any age
- Treatment
- Achilles allograft reconstruction
RUPTUREExtensor Mechanism Rupture Features
Hook:RUPTURE: Cannot Raise leg (pathognomonic), Urgent repair better, Patellar height critical, Tension in Extension, Under 2cm gap = repair, Reconstruction for chronic!
ACUTEPrimary Repair Indications
Hook:ACUTE repair for Acute injury, Close gap, Uncomplicated case, good Tissue quality, Early timing!
CHRONICAllograft Reconstruction Indications
Hook:CHRONIC cases need allograft: Chronic injury, Huge gap, Revision, Old tissue, No length, Insufficient tissue, Complex case!
Overview and Epidemiology
Extensor mechanism ruptures involve disruption of the quadriceps tendon, patellar tendon, or both, resulting in loss of active knee extension. These injuries can be acute traumatic ruptures or chronic degenerative failures. Treatment depends on timing (acute vs chronic), gap size, and tissue quality.
Mechanism of Injury
Quadriceps tendon rupture:
- Eccentric contraction: Sudden quadriceps contraction against resistance (falling, jumping)
- Age factor: More common in patients over 40 (tendon degeneration)
- Risk factors: Steroids, diabetes, renal disease, quinolone antibiotics
- Location: Usually at insertion on superior pole of patella
Patellar tendon rupture:
- Eccentric contraction: Sudden quadriceps contraction with knee flexion
- Age factor: More common in patients under 40 (athletic activity)
- Risk factors: Previous patellar tendonitis, Osgood-Schlatter disease, steroids
- Location: Usually at insertion on inferior pole of patella or tibial tubercle
Inability to perform straight leg raise = complete extensor mechanism rupture. This is pathognomonic. Partial ruptures may have extensor lag (10-90 degrees). Always test straight leg raise in suspected cases - if patient cannot lift heel off bed, rupture is complete.
Epidemiology
- Incidence: 1-2% of knee injuries
- Quadriceps tendon: Peak age 40-60 years, male predominance
- Patellar tendon: Peak age 20-40 years, male predominance
- Bilateral: Rare (5-10%), usually associated with systemic disease (renal failure, steroids)
- Associated injuries: Patellar fractures, tibial tubercle avulsions (pediatric)
Anatomy and Pathophysiology
Extensor Mechanism Anatomy
The extensor mechanism consists of:
- Quadriceps muscle: Vastus medialis, vastus lateralis, vastus intermedius, rectus femoris
- Quadriceps tendon: Inserts on superior pole of patella
- Patella: Sesamoid bone, improves mechanical advantage
- Patellar tendon: Inserts on tibial tubercle
- Medial/lateral retinaculum: Secondary extensors
Blood supply:
- Superior: Descending genicular artery (quadriceps tendon)
- Inferior: Anterior tibial recurrent artery (patellar tendon)
- Patella: Peripatellar plexus (vulnerable to injury)
Pathophysiology
Acute rupture:
- Traumatic: Sudden eccentric contraction
- Tissue quality: Usually good (healthy tendon)
- Gap size: Usually under 2cm (can be approximated)
- Healing potential: Excellent with primary repair
Chronic rupture:
- Degenerative: Progressive tendon weakening
- Tissue quality: Poor (degenerated, friable)
- Gap size: Usually over 2cm (cannot be approximated)
- Healing potential: Poor - requires allograft reconstruction
Risk factors for rupture:
- Systemic: Steroids, diabetes, renal disease, quinolone antibiotics
- Local: Previous tendonitis, Osgood-Schlatter disease, patellar tendinopathy
- Age: Quadriceps (over 40), patellar tendon (under 40)
The patella has a tenuous blood supply through the peripatellar plexus. Extensive dissection or multiple surgeries can compromise blood supply, leading to avascular necrosis. Preserve retinaculum and minimize dissection when possible.
Classification Systems
Location-Based Classification
Quadriceps tendon rupture:
- Superior to patella
- More common in older patients (over 40)
- Usually at insertion on superior pole
- May extend into muscle belly (rare)
Patellar tendon rupture:
- Inferior to patella
- More common in younger patients (under 40)
- Usually at insertion on inferior pole or tibial tubercle
- May be midsubstance (rare)
Combined rupture:
- Both quadriceps and patellar tendon
- Usually high-energy trauma
- Requires extensive reconstruction
Location-based classification helps guide surgical approach and reconstruction strategy.
Clinical Assessment
History
Mechanism: Eccentric quadriceps contraction
- Falling with knee flexion
- Jumping/landing
- Sudden change in direction
- Direct trauma (rare)
Symptoms:
- Immediate pain and swelling
- Inability to extend knee actively
- "Pop" or "snap" sensation
- Inability to bear weight
- Knee "giving way"
Physical Examination
Inspection:
- Knee effusion (hemarthrosis)
- Visible/palpable defect (superior or inferior to patella)
- Patellar position: Alta (patellar tendon rupture) or baja (quadriceps rupture)
- Ecchymosis (acute ruptures)
- Previous surgical scars
Palpation:
- Quadriceps rupture: Gap superior to patella
- Patellar tendon rupture: Gap between patella and tibial tubercle
- Tenderness at rupture site
- Patellar position assessment
Range of Motion:
- Passive: Usually full (pain-limited)
- Active: Cannot extend (complete rupture) or extensor lag (partial rupture)
- Flexion: May be limited by pain
Special Tests:
- Straight leg raise: Pathognomonic - inability to perform = complete rupture
- Extensor lag: Measure angle of lag (10-90 degrees = partial rupture)
- Patellar height: Insall-Salvati ratio (normal 0.8-1.2)
Straight leg raise test is pathognomonic for complete extensor mechanism rupture. If patient cannot lift heel off bed, rupture is complete. Partial ruptures may have extensor lag (10-90 degrees). Always test straight leg raise in suspected cases.
Differential Diagnosis
The "cannot extend the knee" presentation has several causes. Distinguish them by the level of the palpable gap, patellar height, and radiographs.
- Key Distinguishing Feature
- Gap superior to patella; older patient, fall
- Patellar Height
- Patella baja
- Confirmatory Test
- Ultrasound/MRI shows supra-patellar discontinuity
- Key Distinguishing Feature
- Gap inferior to patella; younger athlete
- Patellar Height
- Patella alta
- Confirmatory Test
- Ultrasound/MRI shows infra-patellar discontinuity
- Key Distinguishing Feature
- Bony crepitus, palpable fracture gap
- Patellar Height
- Variable
- Confirmatory Test
- Radiograph shows fracture line
- Key Distinguishing Feature
- Adolescent, distal bony fragment
- Patellar Height
- Patella alta
- Confirmatory Test
- Lateral radiograph (Ogden classification)
- Key Distinguishing Feature
- Extension blocked by pain not anatomy; SLR possible with analgesia
- Patellar Height
- Normal
- Confirmatory Test
- Aspiration and re-examination restores SLR
- Key Distinguishing Feature
- Weak quads but tendons intact; sensory deficit
- Patellar Height
- Normal
- Confirmatory Test
- Neurological exam, EMG; imaging tendons intact
Imaging
Radiographs:
- AP and lateral knee: Assess patellar height (Insall-Salvati ratio)
- Patella alta: Suggests patellar tendon rupture
- Patella baja: Suggests quadriceps rupture
- Avulsion fractures: May see bony avulsion at insertion sites
Ultrasound:
- Can visualize tendon discontinuity
- Assess gap size
- Evaluate tissue quality
- Useful for diagnosis but MRI preferred
MRI:
- Gold standard for diagnosis
- Shows exact location and extent of rupture
- Assesses gap size
- Evaluates tissue quality
- Identifies associated injuries
Imaging Atlas
Investigations
Standard X-ray Protocol
Views: AP and lateral knee.
Key findings:
- Patellar height: Insall-Salvati ratio (normal 0.8-1.2)
- Patella alta: Suggests patellar tendon rupture
- Patella baja: Suggests quadriceps rupture
- Avulsion fractures: Bony avulsion at insertion sites
- Associated fractures: Patellar fractures, tibial tubercle avulsions
Lateral view is critical - shows patellar height and any avulsion fractures.
Bilateral and Spontaneous Rupture: the Missed Diagnosis and the Systemic Work-up
The epidemiology flags that bilateral rupture is rare (roughly 5-10% of cases) and "usually associated with systemic disease," and the global-practice section lists the metabolic red flags - but the clinical trap and the mandatory work-up deserve to be spelled out, because this is where bilateral cases are lost.
Why bilateral rupture is missed. When both knees fail symmetrically there is no normal contralateral limb to compare against. The patient presents simply "unable to stand or walk," and is easily mislabelled as neurological weakness, generalised deconditioning, or bilateral knee effusions. A substantial proportion of bilateral ruptures are missed at first presentation for exactly this reason. The discipline is identical to the unilateral case: test the straight leg raise on each side independently - bilateral loss of active extension with palpable supra- or infra-patellar gaps is diagnostic, and radiographs will typically show patella alta or baja on both sides.
The systemic work-up is not optional. A bilateral or truly spontaneous (atraumatic) rupture is a red flag for systemic tendinopathy, and the underlying disease directly predicts poor tendon healing and re-rupture, so it must be sought and optimised around surgery. The recognised associations are chronic kidney disease / dialysis (renal osteodystrophy and secondary hyperparathyroidism weaken the osteotendinous junction), primary hyperparathyroidism, gout and pseudogout, diabetes, SLE and other connective-tissue disease, chronic corticosteroid and anabolic-steroid use, and fluoroquinolone (and, more weakly, statin) exposure. Practically, check renal function, calcium and phosphate, PTH, urate and inflammatory markers, and review the drug history.
Management. Both sides should generally be repaired or reconstructed - usually in the same setting - because leaving one side leaves the patient without a functional extensor on that limb. Counsel that healing is less reliable and re-rupture more likely than after an isolated traumatic tear because the tendon substance is intrinsically diseased, and optimise the modifiable contributors (steroid dose, glycaemic control, smoking cessation) identified in the risk-factor evidence above.
"Bilateral" or "spontaneous" extensor mechanism rupture is systemic disease until proven otherwise, not bad luck. Test each straight leg raise separately (there is no normal side to compare against), and work up renal failure, hyperparathyroidism, gout, corticosteroids and fluoroquinolones before writing it off as a simple tendon injury.
Management Algorithm
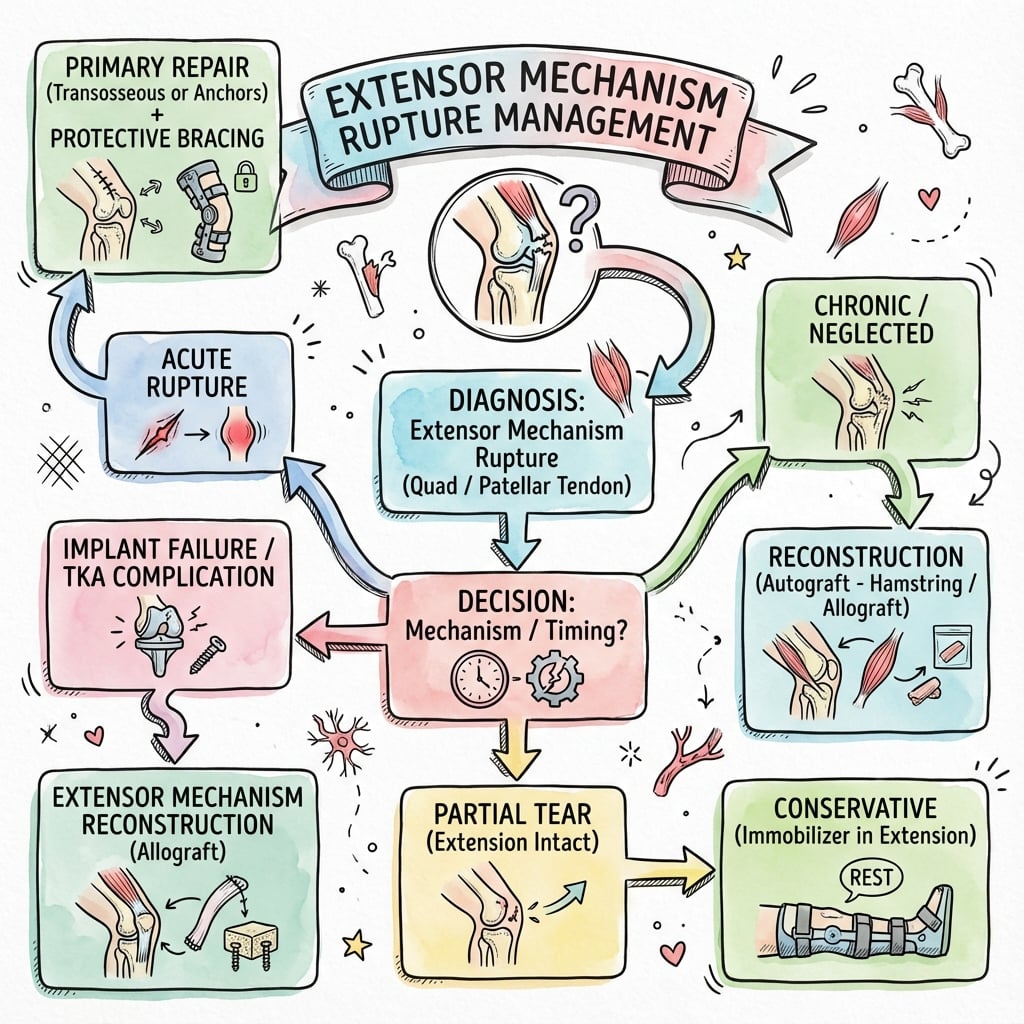
Management Pathway
Extensor Mechanism Rupture Management
Determine location (quadriceps vs patellar tendon), timing (acute vs chronic), gap size (under vs over 2cm), and tissue quality.
If gap under 2cm and good tissue quality, primary repair with Krackow weave. Excellent outcomes (85-95% success).
If gap over 2cm or poor tissue quality, Achilles allograft reconstruction. Good outcomes (60-80% success).
Immobilize in extension for 4-6 weeks. Begin ROM at 2-4 weeks. No active extension for 8-12 weeks. Progressive strengthening.
Surgical Technique
Primary Repair Technique
Indications:
- Acute rupture (under 6 weeks)
- Gap under 2cm after mobilization
- Good tissue quality
- First-time rupture
Patient Positioning:
- Supine on standard table
- Tourniquet on thigh
- Bump under ipsilateral hip
- Contralateral leg abducted
Incision:
- Midline anterior incision
- Extend as needed for exposure
- Full-thickness flaps
Exposure:
- Evacuate hematoma
- Identify rupture edges
- Assess tissue quality
- Mobilize tendon edges
Repair Technique:
- Krackow weave: No. 5 non-absorbable suture (Ethibond or Fiberwire)
- Quadriceps rupture: 3-4 throws each side, pass through patellar tunnels, tie over inferior pole
- Patellar tendon rupture: 3-4 throws each side, pass through patellar tunnels, tie over superior pole
- Augmentation: Side-to-side sutures, retinacular repair
- Tensioning: Knee in full extension, confirm Insall-Salvati ratio 0.8-1.2
Closure: Layered closure, hinged brace locked in extension.
Insall-Salvati ratio must be 0.8-1.2 - this is critical for function. Overtightening causes patella baja and stiffness. Undertightening causes patella alta and weakness. Always set tension with knee in full extension and confirm patellar height on image intensifier before closing.
Complications
- Incidence
- 5-10%
- Risk Factors
- Inadequate fixation, early active extension
- Prevention/Management
- Secure fixation, protect for 8-12 weeks
- Incidence
- 10-20%
- Risk Factors
- Overtightening, prolonged immobilization
- Prevention/Management
- Proper tension, early ROM (2-4 weeks)
- Incidence
- 15-25%
- Risk Factors
- Undertightening, incomplete rehabilitation
- Prevention/Management
- Proper tension, complete rehabilitation
- Incidence
- 5-10%
- Risk Factors
- Improper tension setting
- Prevention/Management
- Confirm Insall-Salvati ratio 0.8-1.2
- Incidence
- 2-5%
- Risk Factors
- Open injury, comorbidities
- Prevention/Management
- Aseptic technique, antibiotics
- Incidence
- Less than 5%
- Risk Factors
- Poor fixation, poor tissue quality
- Prevention/Management
- Secure fixation, good tissue apposition
Re-rupture
5-10% incidence:
- Cause: Inadequate fixation, early active extension, poor tissue quality
- Prevention: Secure fixation, protect for 8-12 weeks (no active extension)
- Management: Revision repair or allograft reconstruction
Stiffness
10-20% incidence:
- Cause: Overtightening, prolonged immobilization, arthrofibrosis
- Prevention: Proper tension (Insall-Salvati 0.8-1.2), early ROM (2-4 weeks)
- Management: Manipulation under anesthesia, arthroscopic lysis of adhesions
Weakness
15-25% incidence:
- Cause: Undertightening, incomplete rehabilitation, muscle atrophy
- Prevention: Proper tension, complete rehabilitation program
- Management: Revision repair if undertightened, continued rehabilitation
Postoperative Care
Immediate Postoperative
- Immobilization: Hinged knee brace locked in extension (4-6 weeks)
- Weight bearing: Non-weight bearing initially (2-3 weeks)
- ROM: Begin passive ROM at 2-4 weeks (unlock brace)
- PT: Quadriceps sets, straight leg raises (immediate)
Rehabilitation Protocol
Weeks 0-2:
- Brace locked in extension
- Non-weight bearing
- Quadriceps sets, straight leg raises
- Ice and elevation
Weeks 2-4:
- Unlock brace for passive ROM (0-90 degrees)
- Progressive weight bearing (partial to full)
- Continue quadriceps strengthening
- No active extension (protect repair)
Weeks 4-6:
- Full passive ROM
- Full weight bearing
- Continue quadriceps strengthening
- No active extension (still protecting repair)
Weeks 6-8:
- Begin active extension (gradual)
- Progressive strengthening
- Balance and proprioception
Weeks 8-12:
- Full active extension
- Progressive resistance training
- Sport-specific training
- Return to sport (when strength adequate)
Return to Sport
Criteria:
- Full ROM (equal to contralateral)
- Quadriceps strength greater than 90% of contralateral
- No extensor lag
- Functional testing passed
Timeline: Usually 4-6 months postoperatively.
Outcomes and Prognosis
Overall Outcomes
Acute primary repair:
- Success rate: 85-95%
- Functional outcomes: 80-90% return to pre-injury level
- Complications: 10-20% (stiffness, weakness, re-rupture)
Chronic allograft reconstruction:
- Success rate: 60-80%
- Functional outcomes: 60-70% return to pre-injury level
- Complications: 20-30% (stiffness, weakness, re-rupture)
Functional Outcomes
Return to sport:
- Timeline: 4-6 months postoperatively
- Rate: 70-80% return to pre-injury level
- Factors: Age, sport level, rehabilitation compliance
Functional testing:
- Quadriceps strength: 90%+ of contralateral
- No extensor lag
- Full ROM
Long-Term Prognosis
Re-rupture risk:
- Acute repair: 5-10% (usually with inadequate fixation or early active extension)
- Allograft reconstruction: 10-15% (higher due to chronicity and tissue quality)
Stiffness risk:
- Acute repair: 10-15% (usually with overtightening)
- Allograft reconstruction: 15-20% (higher due to chronicity)
Weakness risk:
- Acute repair: 10-15% (usually with undertightening or incomplete rehabilitation)
- Allograft reconstruction: 20-25% (higher due to chronicity and muscle atrophy)
Factors Affecting Outcomes
Positive factors:
- Early repair (within 2 weeks)
- Good tissue quality
- Secure fixation
- Proper tension (Insall-Salvati 0.8-1.2)
- Complete rehabilitation
Negative factors:
- Delayed repair (over 6 weeks)
- Poor tissue quality
- Inadequate fixation
- Improper tension (patella baja/alta)
- Incomplete rehabilitation
Prevention and Return to Sport
Prevention
Primary prevention:
- Proper landing technique (knee flexion, not hyperextension)
- Strength training (quadriceps, hamstrings)
- Flexibility training
- Avoid sudden eccentric loading
Secondary prevention (after injury):
- Complete rehabilitation before return to sport
- Continued strength and conditioning
- Gradual return to activity
- Sport-specific training
Return to Sport Criteria
Clinical:
- Full ROM (equal to contralateral)
- Quadriceps strength greater than 90% of contralateral
- No extensor lag
- No effusion
Functional:
- Single-leg hop test (greater than 90% of contralateral)
- Agility testing passed
- Sport-specific drills completed
Timeline: Usually 4-6 months postoperatively, depending on sport and level.
Guidelines, Registries & Global Practice
Global Epidemiology
- Quadriceps tendon rupture incidence approximately 1.4 per 100,000 per year; patellar tendon rupture rarer. Both are far less common than Achilles rupture.
- Strong male predominance (roughly 4-8:1). Quadriceps ruptures cluster in patients over 40 (degenerate insertion, simple fall); patellar tendon ruptures in athletic patients under 40 (eccentric jumping load).
- Bilateral or spontaneous rupture is a red flag for systemic disease: chronic kidney disease/dialysis, hyperparathyroidism, diabetes, gout, SLE, chronic corticosteroid or fluoroquinolone use.
Side-by-Side Society Guidance
No single society publishes a dedicated extensor-mechanism-rupture guideline; practice is consensus- and registry-informed. Points of genuine agreement and divergence:
- Position on Acute Repair
- Early operative repair for complete ruptures; transosseous or anchor fixation acceptable
- Position on Chronic / TKA Failure
- Allograft or autograft reconstruction; counsel on higher failure
- Emphasis
- Functional restoration, return-to-sport metrics
- Position on Acute Repair
- Prompt surgical fixation of acute extensor disruption; early supervised rehab
- Position on Chronic / TKA Failure
- Specialist/revision-arthroplasty referral for periprosthetic failure
- Emphasis
- Timely diagnosis, avoiding missed SLR deficit
- Position on Acute Repair
- Krackow/transosseous repair, tension in full extension, protected early motion
- Position on Chronic / TKA Failure
- Bridging allograft with bone block; fix graft tight in extension
- Emphasis
- Construct biomechanics and tensioning
- Position on Acute Repair
- Operative repair standard; ultrasound widely used first-line for diagnosis
- Position on Chronic / TKA Failure
- Allograft equivalence (Achilles vs full EM) accepted
- Emphasis
- Imaging access, graft selection
Registry & Resource-Setting Notes
- No dedicated tendon-rupture registry exists; the best comparative data on chronic/periprosthetic extensor failure come from arthroplasty registries (NJR, AJRR, AOANJRR) reporting extensor mechanism disruption in roughly 0.1-2.5 percent of TKAs, and from pooled allograft series.
- High-resource settings: MRI/ultrasound on demand, fresh-frozen Achilles allograft available, synthetic mesh/Marlex augmentation for revision, structured physiotherapy.
- Limited-resource settings: diagnosis is clinical (palpable gap, lost straight-leg-raise) supported by plain radiographs showing patella alta/baja; allograft is often unavailable, so autograft (semitendinosus/gracilis loop, fascia lata, contralateral tendon) and primary repair with cerclage/wire augmentation dominate. The diagnostic priority everywhere is the same: do not miss a complete rupture by attributing the SLR deficit to pain.
Controversies and Areas of Uncertainty
Anchors are faster and avoid patellar tunnels, but the pooled evidence (Mehta 2020) shows no functional advantage and more complications with anchors. The "best" construct remains unsettled and largely surgeon preference.
Cerclage wire, suture tape or synthetic augmentation may protect the repair and allow earlier motion, but high-level comparative data are lacking and hardware-related reoperation (wire removal) is a trade-off.
Traditional protocols immobilise in extension for weeks; emerging accelerated/early-motion protocols may reduce stiffness without raising re-rupture, but optimal timing of active extension is not defined by trial evidence.
For isolated patellar tendon rupture the two are statistically equivalent (Balato 2022). Full extensor mechanism allograft may reduce reliance on walking aids but carries graft-availability and sizing limits.
Extensor mechanism ruptures are a common viva topic. Know the pathognomonic sign (inability to perform straight leg raise), acute vs chronic treatment (primary repair vs allograft), gap size threshold (2cm), patellar height (Insall-Salvati 0.8-1.2), and allograft selection (Achilles allograft). Be ready to defend a construct choice and acknowledge the controversies above.
Combined (Simultaneous) Quadriceps and Patellar Tendon Rupture
The classification names a combined rupture - simultaneous disruption of the quadriceps tendon (or its patellar insertion) and the patellar tendon in the same limb - but it is worth developing because it behaves quite differently from an isolated single-tendon injury. Here the patella is effectively untethered at both poles, and if a transverse patella fracture coexists the extensor mechanism is completely disconnected.
When it happens. It is genuinely rare and is almost always either high-energy (dashboard injury, motorcycle trauma, fall from height) or occurs in a systemically compromised tendon (chronic corticosteroids, chronic kidney disease, connective-tissue disease). Suspect it when the mechanism is violent or when tissue quality is obviously poor.
Recognition. There is complete loss of active extension with a palpable gap both superior and inferior to the patella, and the patella itself may be abnormally mobile. The usual radiographic shortcut fails: because the patella is anchored at neither end, it does not sit in reliable alta (the patellar-tendon-rupture cue) or baja (the quadriceps-rupture cue) - it simply drifts. Ultrasound or MRI confirms discontinuity above and below.
Reconstruction principles. This is more demanding than a single-tendon repair because there is no intact anchor at either pole to tension against. Establish a stable base first: repair or reconstruct one end (usually the pole with better tissue) to create a fixed point, then tension the second tendon to it. Restore patellar height by templating against the normal contralateral knee (patellar tendon length / Insall-Salvati) rather than relying on the alta/baja rules, which do not apply when both tendons are gone. If native tissue is inadequate at either pole, the salvage is a whole extensor mechanism allograft spanning tibial tubercle to quadriceps in one construct, rather than two separate grafts. As with every construct here, fix in full extension. The single-tendon operative detail is developed in the dedicated quadriceps tendon rupture and patellar tendon rupture topics.
When both tendons rupture, the examiner's favourite shortcut - "alta means patellar tendon, baja means quadriceps" - breaks down, because a patella anchored at neither pole gives no reliable height cue. Template the reconstruction against the normal contralateral knee, build off one repaired pole as a fixed base, and reach for a whole extensor mechanism allograft if tissue is inadequate at either end.
MCQ Practice Points
Q: What is the pathognomonic sign of complete extensor mechanism rupture? A: Inability to perform straight leg raise - If patient cannot lift heel off bed, rupture is complete. Partial ruptures may have extensor lag (10-90 degrees).
Q: What is the treatment for an acute extensor mechanism rupture (under 6 weeks, gap under 2cm)? A: Primary repair with Krackow weave - Acute repairs achieve 85-95% success rate. Chronic ruptures (over 6 weeks, gap over 2cm) require allograft reconstruction (60-80% success).
Q: What gap size threshold determines primary repair vs allograft reconstruction? A: 2cm - Gap under 2cm allows primary repair. Gap over 2cm requires allograft reconstruction. Gap size is key determinant of treatment.
Q: What is the normal Insall-Salvati ratio and why is it critical? A: 0.8-1.2 - Overtightening causes patella baja and stiffness. Undertightening causes patella alta and weakness. Patellar height is critical for function.
Q: What is the gold standard allograft for extensor mechanism reconstruction? A: Achilles allograft - Provides calcaneal bone block for tibial tubercle fixation (bone-to-bone healing) and adequate length (15-18cm) to bridge gaps.
Q: What is the optimal timing for acute extensor mechanism repair? A: Within 2 weeks - Early repair has better outcomes than delayed repair. Acute repairs (under 6 weeks) achieve 85-95% success vs 60-80% for chronic (over 6 weeks).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents to ED after falling down stairs. He cannot extend his knee or perform a straight leg raise. Examination shows a palpable defect superior to the patella and patella baja. X-ray shows patella baja. MRI shows complete quadriceps tendon rupture with a 1.5cm gap.”
“A 35-year-old athlete presents 3 months after a patellar tendon rupture that was initially missed. He has persistent extensor lag of 30 degrees and cannot return to sport. Examination shows a palpable defect between patella and tibial tubercle, patella alta, and quadriceps atrophy. MRI shows chronic patellar tendon rupture with a 4cm gap and poor tissue quality.”
“A 68-year-old woman who had a total knee replacement 14 months ago presents with sudden loss of active extension after a stumble. She has an extensor lag of 40 degrees, a palpable infrapatellar gap and patella alta. Components appear well-fixed on radiographs. She has diabetes and is a current smoker.”
Key Anatomy
- Extensor mechanism: Quadriceps → quadriceps tendon → patella → patellar tendon → tibial tubercle
- Insall-Salvati ratio: Normal 0.8-1.2 (patellar length / patellar tendon length)
- Patella alta: Suggests patellar tendon rupture
- Patella baja: Suggests quadriceps rupture
Classification
- By location: Quadriceps tendon (over 40) vs patellar tendon (under 40)
- By timing: Acute (under 6 weeks) vs chronic (over 6 weeks)
- By gap size: Under 2cm (primary repair) vs over 2cm (allograft)
- By tissue quality: Good (primary repair) vs poor/degenerated (allograft)
- Subacute (4-8 weeks): Gray zone - assess gap and tissue quality
Treatment Algorithm
- Acute (under 6 weeks, gap under 2cm): Primary repair with Krackow weave
- Chronic (over 6 weeks, gap over 2cm): Achilles allograft reconstruction
- Gap size threshold: 2cm (key determinant)
- Timing: Early repair (within 2 weeks) has better outcomes
Surgical Pearls
- Krackow weave: No. 5 non-absorbable suture, 3-4 throws each side
- Patellar height critical: Insall-Salvati ratio 0.8-1.2
- Tension setting: Knee in full extension, confirm on image intensifier
- Achilles allograft: Bone block for tibial fixation, adequate length (15-18cm)
Complications
- Re-rupture: 5-10% (prevent with secure fixation, protect 8-12 weeks)
- Stiffness: 10-20% (prevent with proper tension, early ROM)
- Weakness: 15-25% (prevent with proper tension, complete rehabilitation)
- Patella baja/alta: 5-10% (prevent with proper tension setting)
Evidence Base
Primary Repair: Systematic Review of Outcomes
- 319 patients pooled; mean age 57 years, most often after a simple fall
- Overall re-rupture rate 2 percent; most regain good or excellent ROM
- Type of repair did not change outcome; delayed repair gave the worst results
Achilles vs Extensor Mechanism Allograft (Meta-analysis)
- Pooled allograft failure ~23-24 percent (i.e. roughly three-quarters succeed)
- Achilles and whole extensor mechanism allograft equivalent for patellar tendon ruptures
- Persistent extensor lag (over 20 degrees) is the dominant failure mode
Transosseous Tunnel vs Suture Anchor Fixation
- No clinically meaningful functional difference between the two fixation methods
- Suture-anchor repairs had significantly more complications (9.3 vs 1.3 percent)
- Transosseous tunnels remain a safe, low-cost default construct
Risk Factors for Poor Outcome After Repair
- Smoking (OR 15.4) and retinacular involvement (OR 9.6) drive complications
- Older age and higher BMI predict residual extensor lag and stiffness
- Overall revision rate low at 3.2 percent
Outcomes in Younger Patients (40 years and under)
- Even in young patients, return to sport is only ~63 percent at ~9 months
- Youth does not guarantee superior outcome vs older controls
- About one third report persistent pain or stiffness long term
Management of Extensor Mechanism Disruption After TKA
- Extensor mechanism disruption complicates 0.1-2.5 percent of TKAs
- Chronic failure needs flaps or allograft, not primary repair
- Graft must be tensioned in full extension to avoid late lag
Insall-Salvati Ratio (Patellar Height Reference)
- Defines the most widely used radiographic index of patellar height
- Normal 0.8-1.2; alta over 1.2, baja under 0.8
- Used intra-operatively to confirm correct repair tension