Persistent or recurrent pain following anatomically successful lumbar spine surgery
- FBSS is a diagnosis of exclusion - must rule out infection, instability, recurrence
- Most common causes: Wrong diagnosis, inadequate decompression, recurrent pathology
- MRI with gadolinium: Scar (peripheral enhancement) vs recurrent disc (central mass)
- Multidisciplinary approach: Pain management, physical therapy, psychological support
- Spinal cord stimulation provides 50% pain reduction in selected patients
- “FBSS is NOT a specific diagnosis - it's a syndrome requiring systematic evaluation
- “Prevention is key: Correct diagnosis, appropriate surgery, proper level verification
- “Psychosocial factors strongly predict FBSS - screen preoperatively
- “Multiple surgeries worsen outcomes - avoid 'the next operation syndrome'
Failed Back Surgery Syndrome
FBSS vs Surgical Failure: FBSS occurs despite anatomically successful surgery. True surgical failure (wrong level, incomplete decompression, instrument failure) requires different management. Always verify surgical success first!
Scar vs Recurrence: Epidural scar enhances on EARLY post-gadolinium images (under 5 minutes) with PERIPHERAL pattern. Recurrent disc shows DELAYED central enhancement or NO enhancement. This is the gold standard imaging distinction!
Best Treatment is Prevention: Correct preoperative diagnosis, verify surgical level intraoperatively, avoid over-fusion, preserve posterior structures when possible, manage patient expectations, screen for psychosocial risk factors.
Very Selective: Only consider revision if clear structural pathology (recurrent disc, inadequate decompression, instability), failed conservative care 6-12 months, and favorable psychosocial profile. Outcomes worsen with each reoperation!
Overview and Definition
Failed back surgery syndrome (FBSS) represents one of the most challenging complications in spine surgery. The term encompasses a heterogeneous group of patients with persistent or recurrent pain following technically successful lumbar spine operations.
Definition and Terminology
Failed Back Surgery Syndrome (FBSS)
- Persistent or recurrent low back and/or leg pain following lumbar spine surgery
- Occurs despite anatomically successful surgical procedure
- Symptoms present beyond expected recovery period (typically 3-6 months)
- Also termed "post-laminectomy syndrome" or "persistent spinal pain syndrome type 2"
Key Distinction
- FBSS: Anatomically successful surgery with persistent symptoms
- Surgical Failure: Technical failure (wrong level, incomplete decompression, hardware failure)
Epidemiology
Incidence and Prevalence
- Value
- 10-40% post-lumbar surgery
- Notes
- Varies by indication and technique
- Value
- 5-15%
- Notes
- Lower rate with minimally invasive techniques
- Value
- 10-30%
- Notes
- Higher with extensive decompressions
- Value
- 15-40%
- Notes
- Highest rates with multi-level fusion
- Value
- 20-25% of referrals
- Notes
- Major burden on healthcare system
Risk Factors for FBSS
- Risk Factors
- Smoking, obesity, poor conditioning, workers' compensation, litigation
- Risk Factors
- Depression, anxiety, catastrophizing, poor coping strategies
- Risk Factors
- Wrong level, inadequate decompression, excessive tissue damage
- Risk Factors
- Multi-level disease, severe degeneration, instability
- Risk Factors
- Delayed mobilization, inadequate rehabilitation, poor compliance
Psychosocial factors are the strongest predictors of FBSS development. Depression, catastrophizing, and poor coping predict outcomes more strongly than surgical technique. Preoperative psychological screening is essential!
Pathophysiology
Understanding the causes of FBSS is critical for both prevention and management. Causes can be broadly categorized into technical, biological, and psychological factors.
Etiology
Technical Causes
Wrong Level Surgery
Epidemiology
- Incidence: 5-15% of primary operations
- More common in obesity, anatomical variants
- Preventable with proper technique
Contributing Factors
- Impact
- Transitional vertebrae, six lumbar vertebrae
- Impact
- Starting from wrong reference point
- Impact
- Failure to verify level intraoperatively
- Impact
- Difficulty palpating landmarks
Prevention
- Count from sacrum upward (most reliable)
- Obtain intraoperative imaging before incision
- Use radiopaque marker on skin over planned level
- Verify with AP and lateral fluoroscopy
- Document level verification in operative note
Wrong-site surgery is a never event! Always verify level with imaging before incision. Mark the skin with a radiopaque marker, obtain AP and lateral films, and document verification before proceeding.
This completes the wrong level surgery discussion.
Biological Causes
Epidural Fibrosis (Scar Tissue)
The most common cause of FBSS, occurring in 5-60% of postoperative patients.
- Details
- Excessive scar formation tethering nerve roots
- Details
- Develops 3-6 months postoperatively
- Details
- Radicular pain, worse with activity, burning quality
- Details
- Peripheral enhancement on early gadolinium images
- Details
- Conservative management, epidural injections, consider adhesiolysis
Recurrent Disc Herniation
- Details
- 5-15% following discectomy
- Details
- Can occur early (under 3 months) or late (over 2 years)
- Details
- Large annular defect, smoking, young age, heavy labor
- Details
- Radicular pain, often sudden onset with activity
- Details
- MRI with gadolinium (no enhancement or delayed central)
- Epidural Fibrosis (Scar)
- 3-6 months post-op
- Recurrent Disc Herniation
- Variable, often sudden
- Epidural Fibrosis (Scar)
- Gradual
- Recurrent Disc Herniation
- Often acute with activity
- Epidural Fibrosis (Scar)
- Burning, aching
- Recurrent Disc Herniation
- Sharp, radiating
- Epidural Fibrosis (Scar)
- Intermediate signal
- Recurrent Disc Herniation
- Hypointense
- Epidural Fibrosis (Scar)
- Variable signal
- Recurrent Disc Herniation
- Hyperintense
- Epidural Fibrosis (Scar)
- EARLY peripheral enhancement
- Recurrent Disc Herniation
- NO enhancement or DELAYED central
- Epidural Fibrosis (Scar)
- Minimal
- Recurrent Disc Herniation
- Moderate to severe
- Epidural Fibrosis (Scar)
- Generally ineffective
- Recurrent Disc Herniation
- May benefit from revision
Adjacent Segment Disease
Degeneration at levels adjacent to fusion, occurring in 5-25% by 10 years.
- Description
- Increased stress on adjacent mobile segments
- Description
- Long fusion construct, sagittal malalignment, preexisting degeneration
- Description
- New onset back/leg pain at new dermatomal level
- Description
- Disc degeneration, stenosis at adjacent level
- Description
- Initially conservative; consider extension of fusion if severe
Arachnoiditis
Inflammatory reaction causing nerve root clumping and scarring.
- Details
- Rare (under 5%), more common with multiple surgeries
- Details
- Intrathecal blood, infection, myelography contrast (historical)
- Details
- Clumped nerve roots, "empty thecal sac" sign, central cord
- Details
- Generally poor, progressive symptoms
- Details
- Pain management, avoid further surgery
MRI gadolinium timing is critical: Scar enhances EARLY (under 5 minutes) with PERIPHERAL pattern. Recurrent disc shows NO enhancement or DELAYED CENTRAL enhancement. Always specify timing of post-contrast imaging!
Psychological Factors
Central Sensitization
Maladaptive neuroplastic changes resulting in chronic pain syndrome.
- Description
- Altered CNS pain processing, lowered pain threshold
- Description
- Widespread pain, hyperalgesia, allodynia
- Description
- Clinical diagnosis, often disproportionate to pathology
- Description
- Multidisciplinary pain program, medications, CBT
Psychosocial Risk Factors
The "Yellow Flags" predicting poor outcomes:
- Depression and anxiety
- Catastrophizing and fear-avoidance beliefs
- Poor coping strategies
- Secondary gain (compensation, litigation)
- Job dissatisfaction
- Social isolation
Clinical Assessment
Systematic evaluation is essential to identify treatable causes and guide management.
History
Pain Characterization
- Purpose
- When did symptoms start relative to surgery?
- Purpose
- Any relief post-surgery before recurrence?
- Purpose
- Back predominant, leg predominant, or equal?
- Purpose
- Sharp/shooting (nerve) vs aching/burning (scar/chronic)?
- Purpose
- Positional, activity-related, constant?
- Purpose
- Rest, position changes, medications?
Red Flags Requiring Urgent Evaluation
Immediate investigation required:
- New onset bowel/bladder dysfunction (cauda equina)
- Progressive motor weakness
- Fever, wound drainage (infection)
- Severe unremitting pain unresponsive to medications
- New sensory level (thoracic symptoms)
Functional Assessment
- Walking distance and tolerance
- Sleep disruption
- Activities of daily living impact
- Work status and disability
- Medication requirements and escalation
- Previous pain management interventions
Psychosocial Screening
Use validated tools:
- Oswestry Disability Index (ODI)
- Visual Analog Scale (VAS) for pain
- SF-36 for quality of life
- Depression screening (PHQ-9)
- Opioid Risk Tool (ORT)
Physical Examination
Inspection
- Surgical scar assessment (well-healed, keloid, drainage)
- Spinal alignment (coronal and sagittal balance)
- Gait pattern and assistive devices
- Muscle wasting in affected myotome
Palpation
- Tenderness over surgical site
- Paraspinal muscle spasm
- Trigger points
- Sacroiliac joint assessment
Range of Motion
- Lumbar flexion and extension
- Note pain reproduction with movement
- Assess for compensation patterns
Neurological Examination
- Assessment
- Myotomal strength testing
- Significance
- New weakness vs pre-existing deficit
- Assessment
- Dermatomal mapping
- Significance
- Compare to preoperative examination
- Assessment
- Knee jerk (L4), ankle jerk (S1)
- Significance
- May be absent post-surgery
- Assessment
- Straight leg raise, femoral stretch
- Significance
- Positive suggests neural irritation
- Assessment
- Non-organic signs
- Significance
- Over 3 suggests psychosocial component
Vascular Examination
- Peripheral pulses (exclude vascular claudication)
- Skin changes, hair loss, temperature
- Ankle-brachial index if vascular suspected
Differential Diagnosis
FBSS is a diagnosis of exclusion. Many conditions mimic persistent post-operative pain, and several arise outside the operated spinal level. Systematically exclude the following before attributing pain to FBSS itself.
- Discriminating Features
- Pain-free interval then acute radicular recurrence, same dermatome, mass effect
- Key Investigation
- Gadolinium MRI (non-enhancing/central-enhancing mass)
- Discriminating Features
- Gradual burning radicular pain, no mass effect
- Key Investigation
- Gadolinium MRI (early peripheral enhancement)
- Discriminating Features
- Fever, raised CRP/ESR, rest and night pain, wound drainage
- Key Investigation
- CRP/ESR, gadolinium MRI, blood cultures
- Discriminating Features
- Mechanical back pain after fusion, worse with load
- Key Investigation
- Fine-cut CT, dynamic radiographs
- Discriminating Features
- New pain at a different dermatome above/below fusion
- Key Investigation
- MRI of adjacent levels
- Discriminating Features
- Pain below L5, positive provocation tests, FABER
- Key Investigation
- Diagnostic SIJ block
- Discriminating Features
- Axial pain, worse on extension/rotation, no true radiculopathy
- Key Investigation
- Diagnostic medial branch block
- Discriminating Features
- Groin pain, limited internal rotation, positive impingement test
- Key Investigation
- Hip radiograph, intra-articular block
- Discriminating Features
- Pain unrelated to spinal posture, absent pulses, relieved by standing still
- Key Investigation
- ABI, arterial duplex
- Discriminating Features
- Stocking distribution, distal symmetrical, metabolic cause
- Key Investigation
- Nerve conduction studies, HbA1c
- Discriminating Features
- New bladder/bowel dysfunction, saddle anaesthesia, bilateral leg symptoms
- Key Investigation
- Urgent MRI
Diagnostic Workup
Systematic imaging and diagnostic procedures to identify treatable pathology.

Imaging Protocol
MRI with Gadolinium Contrast
The gold standard for FBSS evaluation.
Sequences Required
- Purpose
- Baseline anatomy, fat signal
- Purpose
- Disc hydration, stenosis, neural compression
- Purpose
- Distinguish scar vs recurrent disc
- Purpose
- Enhance inflammatory changes
Interpretation - Scar vs Recurrence
- Epidural Scar
- Intermediate signal
- Recurrent Disc
- Hypointense
- Epidural Scar
- Variable
- Recurrent Disc
- Hyperintense (if hydrated)
- Epidural Scar
- EARLY peripheral enhancement
- Recurrent Disc
- NO or DELAYED central enhancement
- Epidural Scar
- Under 5 minutes
- Recurrent Disc
- Over 15 minutes or none
- Epidural Scar
- Minimal
- Recurrent Disc
- Present
- Epidural Scar
- Tethering
- Recurrent Disc
- Displacement away
Other MRI Findings
- Arachnoiditis: Clumped nerve roots, empty thecal sac
- Pseudomeningocele: CSF collection, dural tear
- Infection: Disc signal change, endplate edema, enhancement
- Stenosis: Residual or adjacent level canal narrowing
This MRI protocol is essential for surgical planning and diagnostic accuracy.
Diagnostic Interventions
Selective Nerve Root Blocks
- Technique
- Inject local anesthetic around suspected nerve root
- Interpretation
- Over 75% pain relief confirms level
- Technique
- Add steroid for therapeutic effect
- Interpretation
- May provide temporary or prolonged relief
- Technique
- Multi-level disease
- Interpretation
- Identify symptomatic level for decompression
Facet Joint Injections/Medial Branch Blocks
- Identify facetogenic pain source
- May guide radiofrequency ablation
- Diagnostic response: Over 80% relief with local anesthetic
Discography (Controversial)
- Details
- Identify painful disc in multi-level disease
- Details
- Provocative injection into disc nucleus
- Details
- Concordant pain reproduction at low pressure
- Details
- High false-positive rate, may accelerate degeneration
- Details
- Limited; mostly for fusion planning in young patients
Diagnostic blocks are valuable but not definitive. Placebo response rates are 30-40%. Confirmatory blocks with different local anesthetics (e.g., lidocaine then bupivacaine on separate days) increase specificity. Never operate based on blocks alone!

Management Algorithm
Treatment of FBSS requires a multidisciplinary, stepwise approach. Surgery is rarely first-line.
Conservative Management (First-Line)
Physical Therapy and Rehabilitation
Goals of Physical Therapy
- Restore function and mobility
- Strengthen core musculature
- Improve flexibility and posture
- Reduce fear-avoidance behaviors
- Facilitate return to activities
Program Components
- Duration
- Weeks 1-4
- Focus
- Pain control, gentle ROM, posture
- Duration
- Weeks 4-8
- Focus
- Core strengthening, endurance training
- Duration
- Weeks 8-12
- Focus
- Functional activities, work simulation
- Duration
- Ongoing
- Focus
- Home exercise program, activity pacing
Pharmacotherapy
Multimodal Analgesia Approach
- Examples
- Ibuprofen, naproxen
- Dosing
- As needed or scheduled
- Considerations
- GI protection if chronic use
- Examples
- Paracetamol
- Dosing
- 1g TDS-QID
- Considerations
- Max 4g/day, hepatotoxicity risk
- Examples
- Gabapentin, pregabalin
- Dosing
- Titrate to effect
- Considerations
- Sedation, dizziness common
- Examples
- Duloxetine, amitriptyline
- Dosing
- Start low, increase slowly
- Considerations
- Dual benefit: pain and mood
- Examples
- Cyclobenzaprine
- Dosing
- Short-term use
- Considerations
- Sedation, dependence risk
- Examples
- Lidocaine patches, capsaicin
- Dosing
- Apply to painful area
- Considerations
- Localized effect, fewer systemic side effects
Opioids have LIMITED role in chronic FBSS: Evidence shows minimal benefit and high risk of dependence, hyperalgesia, and worsening outcomes. Avoid chronic opioid therapy when possible. If used, use structured agreement, monitor urine drug screens, assess using Opioid Risk Tool (ORT).
Psychological Interventions
Cognitive Behavioral Therapy (CBT)
- Goal
- Challenge catastrophizing, negative thoughts
- Goal
- Increase activity despite pain
- Goal
- Reduce muscle tension, anxiety
- Goal
- Avoid boom-bust cycles
- Goal
- Improve sleep quality
Multidisciplinary Pain Rehabilitation Programs
Intensive programs combining physical therapy, psychological therapy, medication optimization, occupational therapy, and vocational rehabilitation show best long-term functional outcomes for FBSS patients.
Interventional Pain Management
Epidural Steroid Injections
- Indication
- Central stenosis, broad distribution
- Success Rate
- 30-50% improve
- Duration
- 3-6 months
- Indication
- Radiculopathy, specific nerve root
- Success Rate
- 50-70% improve
- Duration
- 3-6 months
- Indication
- Multi-level, previous surgery
- Success Rate
- 30-40% improve
- Duration
- Variable
Radiofrequency Ablation
- Target: Facet joint medial branches or dorsal root ganglion
- Indication: Positive diagnostic blocks
- Duration: 6-12 months relief
- Repeatable if initial success
Neuromodulation
Spinal Cord Stimulation (SCS)
The most evidence-based intervention for FBSS with predominant leg pain.
Patient Selection Criteria
- Details
- Predominantly radicular leg pain
- Details
- At least 6 months appropriate treatment
- Details
- No untreated major depression, realistic expectations
- Details
- No correctable structural pathology
- Details
- Over 50% pain reduction during trial period
Evidence Base
- Findings
- SCS superior to conventional management at 6 months
- Findings
- 50-70% maintain over 50% pain reduction at 5 years
- Findings
- 70-80% would repeat procedure
- Findings
- Significant improvements in ODI, quality of life
SCS is evidence-based for FBSS: PROCESS trial showed SCS superior to reoperation for FBSS with radicular pain. Trial before permanent implant is mandatory. Predominantly leg pain responds better than back pain!
Traditional (low-frequency "tonic") spinal cord stimulation works by replacing pain with a paraesthesia and is best for leg rather than back pain. Newer modalities address its limitations. High-frequency SCS (10 kHz, the SENZA-RCT) and burst stimulation are paraesthesia-free and have shown improved relief of axial low back pain (the historically SCS-resistant component of FBSS), broadening the population that can benefit. Dorsal root ganglion (DRG) stimulation (the ACCURATE RCT) targets the DRG directly and is superior to traditional SCS for focal, dermatomal lower-limb neuropathic pain (including CRPS and a discrete radicular distribution), giving more precise, posture-stable coverage of a single territory. The exam point: SCS is no longer one thing — match the modality to the pain (tonic, high-frequency or burst for diffuse radicular with or without back pain; DRG for a focal dermatomal target), and remember that a successful trial before permanent implantation remains mandatory for all of them.
For the patient with refractory FBSS pain who has exhausted rehabilitation, interventional injections and (often) spinal cord stimulation, intrathecal drug delivery (ITDD) via an implanted pump is the next rung. By delivering analgesia directly into the CSF, it achieves pain control at a tiny fraction of the systemic dose, which is its main attraction in a population where chronic oral opioids do more harm than good. Agents include intrathecal opioids (e.g. morphine), ziconotide (a non-opioid calcium-channel blocker, useful where opioids are undesirable) and baclofen (where spasticity coexists). Like SCS it requires a trial and careful psychological/expectation screening first, and it carries real risks — catheter-tip inflammatory granuloma, infection/meningitis, pump or catheter malfunction, and respiratory depression with opioid dosing errors — so it is managed in a specialist pain service. The exam point: ITDD is a last-line, specialist option that exploits the dose advantage of the intrathecal route, not a routine FBSS treatment.
Surgical Management (Highly Selective)
Indications for Revision Surgery
Surgery is rarely indicated in FBSS. Consider ONLY if ALL criteria met:
- Clear structural pathology on imaging (recurrent disc, stenosis, instability)
- Symptoms correlate with imaging findings
- Failed 6-12 months of appropriate conservative care
- Reasonable surgical target identified
- Favorable psychosocial profile
- Patient has realistic expectations
Specific Surgical Indications
- Surgery
- Revision discectomy ± fusion
- Expected Success Rate
- 60-80% if clear recurrence
- Surgery
- Revision decompression
- Expected Success Rate
- 50-70% if residual compression
- Surgery
- Revision fusion
- Expected Success Rate
- 50-60% (decreases with each revision)
- Surgery
- Extension of fusion
- Expected Success Rate
- 40-60%
- Surgery
- Fusion
- Expected Success Rate
- 50-70%
Outcomes Decrease with Multiple Operations
- Success Rate
- 70-90%
- Success Rate
- 50-70%
- Success Rate
- 30-50%
- Success Rate
- Under 30%
The "next operation syndrome": Each subsequent operation has LOWER success rate and HIGHER complication rate. After 3 operations, success rate under 30%. Avoid perpetual surgical cycling - recognize when surgery will not help!
Complications
Understanding potential complications helps inform patient counseling and guide treatment decisions.
Complications of Conservative Treatment
Non-Interventional Complications
- Complication
- GI bleeding, cardiovascular events
- Incidence
- 1-5% with chronic use
- Management
- PPI prophylaxis, lowest effective dose
- Complication
- Sedation, dizziness, falls
- Incidence
- 10-30%
- Management
- Dose titration, fall precautions
- Complication
- Dependence, hyperalgesia, constipation
- Incidence
- 20-40% with chronic use
- Management
- Avoid when possible, bowel regimen
- Complication
- Acute injury, pain flare
- Incidence
- Under 5%
- Management
- Proper screening, gradual progression
Psychological Intervention Risks
- Emotional distress during CBT (initial worsening)
- Resistance to treatment
- Time and financial commitment
- Generally safe with skilled practitioners
Complications of Interventional Procedures
Epidural Steroid Injections
- Incidence
- 1-5%
- Management
- Bed rest, blood patch if persistent headache
- Incidence
- Under 1%
- Management
- Emergency MRI, surgical drainage, IV antibiotics
- Incidence
- Under 1%
- Management
- Emergency decompression if neurological deficit
- Incidence
- 2-5%
- Management
- Supportive care, fluids, observation
- Incidence
- 5-10%
- Management
- Usually resolves within 24-48 hours
Spinal Cord Stimulation
- Incidence
- 10-15%
- Management
- Revision, lead repositioning
- Incidence
- 2-5%
- Management
- Antibiotics; explant if severe
- Incidence
- 5-10%
- Management
- Battery replacement, lead revision
- Incidence
- 20-30% over time
- Management
- Reprogramming, lead revision, explant
- Incidence
- 5-10%
- Management
- Repositioning, smaller device
- Incidence
- Under 1%
- Management
- Conservative management, blood patch
Radiofrequency Ablation
- Incidence
- 5-10%
- Notes
- Usually temporary, resolves over weeks
- Incidence
- Under 1%
- Notes
- Proper grounding technique prevents
- Incidence
- Under 1%
- Notes
- Sterile technique essential
- Incidence
- Under 1%
- Notes
- Careful localization prevents
Complications of Revision Surgery
Intraoperative Complications
- Primary Surgery
- 3-10%
- Revision Surgery
- 10-20%
- Implications
- Higher risk due to scarring, usually repairable
- Primary Surgery
- 1-3%
- Revision Surgery
- 3-8%
- Implications
- More difficult dissection through scar tissue
- Primary Surgery
- Under 1%
- Revision Surgery
- 1-3%
- Implications
- Altered anatomy increases risk
- Primary Surgery
- 1-3%
- Revision Surgery
- 1-2%
- Implications
- Careful imaging verification essential
- Primary Surgery
- 5-10%
- Revision Surgery
- 10-15%
- Implications
- Scar tissue obscures anatomy
Early Postoperative Complications (Under 6 Weeks)
- Incidence
- 2-5%
- Prevention/Management
- Prophylactic antibiotics, sterile technique
- Incidence
- 1-3%
- Prevention/Management
- Emergency I&D, long-term IV antibiotics
- Incidence
- 2-5%
- Prevention/Management
- Meticulous hemostasis, drain placement
- Incidence
- 2-5%
- Prevention/Management
- Watertight dural closure, prone positioning
- Incidence
- 1-3%
- Prevention/Management
- Early mobilization, chemoprophylaxis
- Incidence
- 5-15%
- Prevention/Management
- Catheterization, alpha-blockers
Late Complications (Over 6 Weeks)
- Incidence
- 15-30% (revision fusion)
- Time Course
- 6-18 months
- Incidence
- 5-10%
- Time Course
- Variable, months to years
- Incidence
- 5-25%
- Time Course
- 5-10 years post-fusion
- Incidence
- 10-20%
- Time Course
- Variable, months to years
- Incidence
- 30-50%
- Time Course
- Ongoing
- Incidence
- 5-15% (long fusions)
- Time Course
- Years
Specific High-Risk Scenarios
Third or Subsequent Revision Surgery
- Complication rates exceed 40%
- Success rates under 30%
- Each revision increases scar tissue burden
- Neurological injury risk doubles with each procedure
- Consider non-surgical options preferentially
Revision in Setting of Active Litigation
- Outcomes significantly worse
- Psychological factors dominant
- Higher pain scores despite anatomical success
- Consider delaying surgery until litigation resolved
Revision with Concurrent Opioid Dependence
- Postoperative pain management extremely challenging
- Higher infection rates
- Delayed healing
- Require structured tapering program preoperatively
Complication rates INCREASE with each revision: First revision has 15-25% complication rate. Second revision 25-40%. Third or more over 40%. Always counsel patients about cumulative risk with multiple operations!
Prevention Strategies
Reducing Complications
- Impact
- Most important factor
- Impact
- Smoking cessation, weight loss, diabetes control
- Impact
- Minimize tissue trauma, adequate hemostasis
- Impact
- Reduces infection risk
- Impact
- Reduces VTE risk
- Impact
- Addresses all contributing factors
Prevention Strategies
The best treatment for FBSS is prevention. Systematic approach reduces incidence.
Preoperative Prevention
Correct Diagnosis
- Implementation
- Ensure MRI findings explain clinical picture
- Implementation
- Hip pathology, peripheral neuropathy, vascular
- Implementation
- 6-12 weeks unless red flags
- Implementation
- Poor outcomes without radiculopathy
Patient Selection and Education
Psychosocial Screening
- Depression and anxiety screening (PHQ-9, GAD-7)
- Catastrophizing assessment
- Litigation and compensation status
- Substance abuse history
- Social support assessment
Realistic Expectations
- Discuss achievable outcomes (improvement, not perfection)
- Explain recovery timeline (3-6 months full recovery)
- Review risks and alternative treatments
- Document shared decision-making
Risk Factor Modification
- Smoking cessation: 4-6 weeks preoperatively
- Weight optimization if BMI over 35
- Diabetes control: HbA1c under 7.5%
- Optimize nutrition status
- Discontinue NSAIDs and anticoagulants per protocol
Intraoperative Prevention
Surgical Technique
- Implementation
- Imaging confirmation BEFORE incision
- Implementation
- Decompress symptomatic levels completely
- Implementation
- Preserve under 50% of facet joints
- Implementation
- Use retractors judiciously, limit stripping
- Implementation
- Prevent hematoma formation
- Implementation
- Watertight closure if dural tear occurs
Specific Technical Points
Discectomy
- Remove loose fragments completely
- Avoid aggressive curettage of disc space
- Preserve annular integrity when possible
- Consider limited anular closure techniques
Decompression
- Decompress lateral recess adequately
- Undercut facet if foraminal stenosis
- Bilateral decompression for bilateral symptoms
- Preserve pars interarticularis
Fusion Decision
- Fuse if instability present (over 3-4mm translation)
- Fuse if over 50% facet resection required
- Consider fusion if degenerative spondylolisthesis
- Avoid unnecessary fusion (increases adjacent segment disease)
Level verification is NON-NEGOTIABLE: Always obtain AP and lateral intraoperative imaging BEFORE incision. Mark skin with radiopaque marker. Count from sacrum upward. Document verification in operative note. Wrong-site surgery is preventable!
Postoperative Prevention
Early Mobilization
- Activity
- Out of bed, walking with assistance
- Activity
- Independent ambulation, self-care
- Activity
- Progressive walking, light activities
- Activity
- Formal physical therapy, return to work (sedentary)
Pain Management
- Multimodal analgesia (minimize opioids)
- Scheduled NSAIDs (if no contraindication)
- Neuropathic pain agents if radicular pain persists
- Transition to oral medications by discharge
Physical Therapy
- Early referral (week 2-4)
- Core strengthening program
- Flexibility and posture training
- Ergonomic education
Follow-up Protocol
- Week 2: Wound check, pain assessment
- Week 6: Clinical evaluation, consider imaging if concerns
- Month 3: Functional assessment
- Month 6 and 12: Long-term outcome evaluation
Guidelines, Registries & Global Practice
FBSS — increasingly termed persistent spinal pain syndrome type 2 — is a global problem whose incidence has not fallen despite improvements in surgical technique. The world standard of care is interdisciplinary, evidence-led and conservative, with reoperation reserved for clearly defined structural targets.
Global epidemiology
- Figure
- ~1 in 5 patients within 2 years
- Source / population
- UK population (HES/CPRD), Weir et al. 2020
- Figure
- Rates of failed back surgery have not declined despite surgical advances
- Source / population
- Narrative review, Chan & Peng 2011
- Figure
- Instrumented fusion did NOT increase persistent pain rate vs decompression/discectomy, but did increase 2-year healthcare costs
- Source / population
- UK case-control, Weir et al. 2020
- Figure
- Considerable impact on patient quality of life and health systems (high cost of illness)
- Source / population
- Chan & Peng 2011
According to PubMed, the contemporary population estimate that roughly one in five patients develops persistent post-operative pain within two years comes from a UK Hospital Episode Statistics / CPRD analysis (Weir et al. 2020, DOI), and the observation that failure rates have not declined despite surgical progress is from the standard review (Chan & Peng 2011, DOI).
Major guidance, side by side
- Position on FBSS / persistent radicular pain
- Spinal cord stimulation recommended for chronic neuropathic pain that persists at least 6 months despite conventional medical management, after a successful trial of stimulation
- Evidence basis
- RCT evidence incl. PROCESS (Kumar 2007)
- Position on FBSS / persistent radicular pain
- Multidisciplinary assessment before any revision; SCS for predominant neuropathic leg pain after failed conservative care; reoperation only for clear structural lesion
- Evidence basis
- PROCESS (Kumar 2007), North 2005
- Position on FBSS / persistent radicular pain
- Trial-then-implant SCS pathway; predominant leg pain responds better than axial back pain; mandatory psychological screening
- Evidence basis
- Kumar 2007, North 2005
- Position on FBSS / persistent radicular pain
- Prevention first — correct diagnosis, intra-operative level verification, avoid unnecessary fusion; revision only for recurrent disc, residual stenosis, instability or pseudarthrosis
- Evidence basis
- Papadopoulos 2006, Chan & Peng 2011
Registry and trial evidence
- Two randomised controlled trials anchor neuromodulation practice: PROCESS (Kumar 2007, DOI) showed SCS superior to medical management for neuropathic leg pain, and the North trial (North 2005, DOI) showed SCS superior to repeat surgery for persistent radicular pain.
- Revision discectomy for a clearly identified true recurrence achieves outcomes comparable to primary discectomy in selected patients (Papadopoulos 2006, DOI).
- There is no dedicated international FBSS registry; epidemiology is derived from national administrative datasets (e.g. UK HES/CPRD) and the spine-surgery literature rather than an implant registry.
Global practice variation
- Access to neuromodulation is the dominant source of variation: SCS is widely available in high-income systems but device cost limits use in many limited-resource settings, where multidisciplinary rehabilitation and pharmacological management predominate.
- Terminology is shifting internationally from "failed back surgery syndrome" toward "persistent spinal pain syndrome", reflecting an attempt to remove the blame-laden framing and standardise classification.
- Psychosocial screening before revision surgery is universally endorsed but inconsistently implemented; where compensation or litigation systems exist, outcomes after revision are consistently poorer.
- Opioids have a limited role in chronic FBSS in all major guidance, with international movement toward reduced long-term opioid prescribing and real-time prescription monitoring.
MCQ Practice Points
Q: What are the most common causes of failed back surgery syndrome (FBSS)?
A: Recurrent or residual disc herniation (most common surgically treatable cause); Foraminal stenosis (especially lateral recess); Adjacent segment disease; Pseudarthrosis (failed fusion); Epidural fibrosis/scar tissue; Segmental instability; Wrong level surgery; Unrecognized spinal stenosis. Non-structural causes: Central sensitization, psychological factors, secondary gain, undiagnosed pain generator (SIJ, facet, hip).
Q: How do you evaluate a patient with persistent pain after lumbar spine surgery?
A: History: Pain timing (immediate vs delayed), character (radicular vs axial), response to previous surgery, red flags. Examination: Neurological assessment, provocative tests (SIJ, facet), hip examination. Imaging: MRI with gadolinium (differentiates scar from recurrent disc); CT for bony detail, fusion assessment; Standing X-rays for instability. Diagnostic injections: Selective nerve root blocks, facet blocks, SIJ injection, discography if indicated. Multidisciplinary pain assessment recommended.
Q: How do you differentiate epidural fibrosis from recurrent disc herniation on MRI?
A: Both can cause nerve compression post-discectomy. Recurrent disc herniation: Mass effect with peripheral enhancement on gadolinium (enhancing rim around non-enhancing disc material); Contiguous with disc space. Epidural fibrosis: Diffuse homogeneous enhancement throughout scar tissue; Retracts and conforms to dural sac rather than displacing it; May extend around nerve root. Clinical correlation essential - scar alone rarely causes significant symptoms.
Q: What is the role of spinal cord stimulation in FBSS?
A: Spinal cord stimulation (SCS) is evidence-based treatment for neuropathic leg pain in FBSS when conservative measures fail. Mechanism: Modulates pain transmission via dorsal column stimulation. Best results: Predominant radicular/neuropathic leg pain (greater than axial back pain); Failed conservative therapy; No surgically correctable pathology; Psychological screening passed. Trial stimulator first; Permanent implant if greater than 50% pain reduction. Less effective for predominantly axial back pain.
Q: What are the predictors of poor outcome after revision spine surgery for FBSS?
A: Poor prognostic factors: Multiple prior surgeries (success rate drops with each revision); Predominant axial back pain (vs radicular); Worker's compensation/litigation; Psychological comorbidities (depression, catastrophizing); Smoking; Chronic opioid use; Long duration of symptoms pre-revision; No clear anatomical pain generator identified. Patient selection is critical - multidisciplinary assessment recommended before revision surgery.
At a Glance
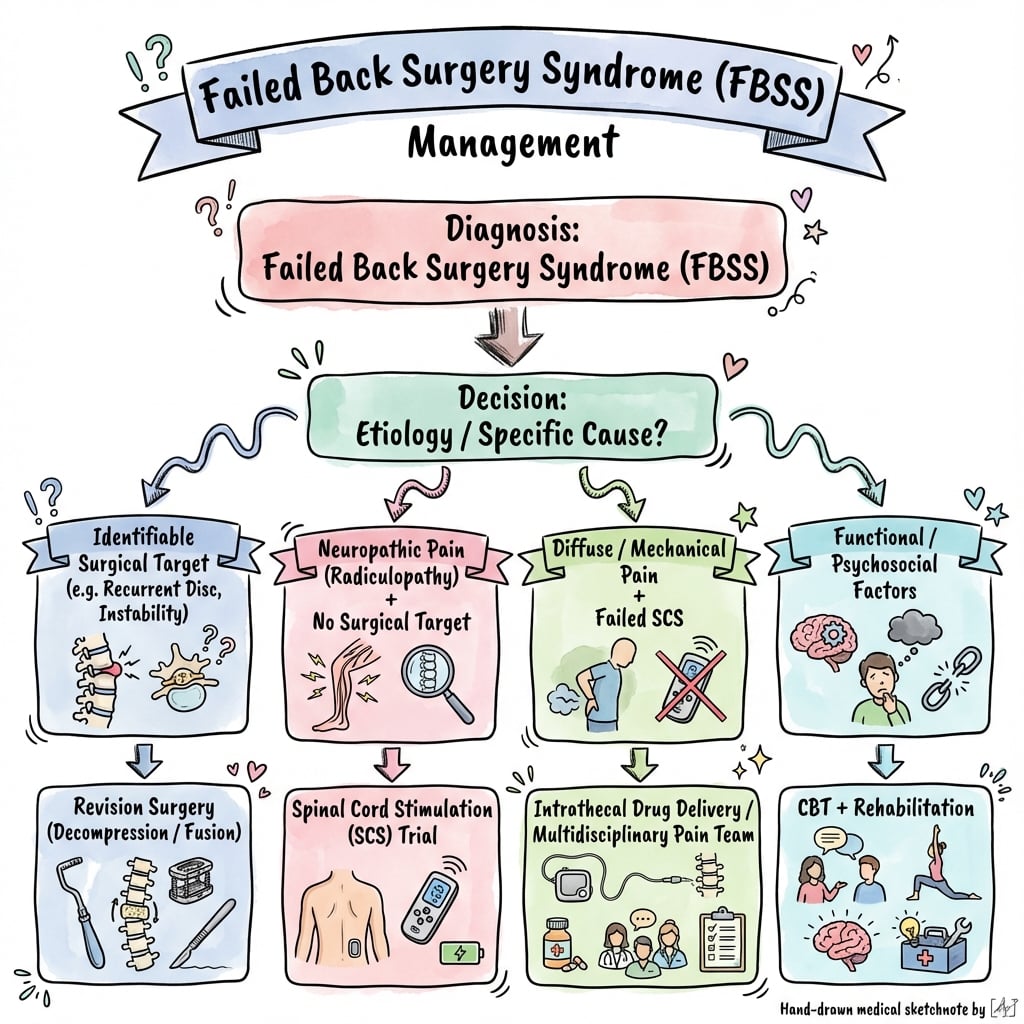
Failed back surgery syndrome (FBSS) is persistent or recurrent pain following anatomically successful lumbar spine surgery, affecting 10-40% of patients. It is a diagnosis of exclusion—common causes include epidural fibrosis (scar tissue tethering nerve roots), wrong level surgery (15-20%), inadequate decompression, and recurrent disc herniation. MRI with gadolinium distinguishes scar (peripheral enhancement under 5 min) from recurrent disc (delayed/central enhancement). Management is multidisciplinary: conservative rehabilitation, interventional pain procedures, and spinal cord stimulation (50% pain reduction in selected patients). Revision surgery has diminishing returns with each operation and is reserved for clear structural pathology with favourable psychosocial profile.
FAILEDFBSS Common Causes
Hook:Why the back surgery FAILED!
SCARSFBSS Evaluation Algorithm
Hook:Look for SCARS as causes of persistent pain!
PREVENTPrevention Strategies
Hook:How to PREVENT FBSS in the first place!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old male underwent L5-S1 microdiscectomy 6 months ago for right L5 radiculopathy. He had 2 weeks of improvement but now has recurrent right leg pain worse than preoperatively. MRI shows soft tissue in the epidural space at L5-S1. How would you evaluate and manage this patient?”
“A 60-year-old female underwent L4-5 decompression for neurogenic claudication 3 months ago. She has had no improvement in symptoms. Review of her postoperative MRI shows decompression was performed at L3-4, not L4-5. The patient is now consulting you for a second opinion. How do you manage this situation?”
“A 50-year-old male presents with chronic back and leg pain. He has had 3 previous lumbar surgeries: L5-S1 discectomy, then L4-5 decompression, then L4-S1 fusion. His pain never improved. He is on high-dose opioids and is requesting another operation. MRI shows solid fusion with no obvious structural pathology. How would you assess and manage this patient?”
Definition and Epidemiology
- FBSS: Persistent or recurrent pain post-lumbar surgery despite anatomical success
- Incidence: 10-40% depending on procedure (higher for fusion vs discectomy)
- NOT a specific diagnosis - heterogeneous syndrome requiring systematic evaluation
- Strongest predictors: Psychosocial factors (depression, catastrophizing)
Common Causes (Mnemonic: FAILED)
- F - Fibrosis (epidural scar) - most common chronic cause
- A - Adjacent segment disease (5-25% by 10 years post-fusion)
- I - Inadequate decompression (residual stenosis, retained disc fragment)
- L - Level wrong (5-15% incidence - never event)
- E - Epidural hematoma or infection (early complications)
- D - Disc recurrent herniation (5-15% following discectomy)
Diagnostic Imaging - MRI with Gadolinium
- Scar: EARLY enhancement (under 5 min) with PERIPHERAL pattern
- Recurrent disc: NO enhancement or DELAYED CENTRAL enhancement (over 15 min)
- Mass effect: Minimal with scar, present with recurrent disc
- Arachnoiditis: Clumped nerve roots, empty thecal sac sign
- Dynamic X-rays: Instability if over 3-4mm translation or over 10-15 degrees angulation
Management Algorithm
- First-line: Conservative (PT, neuropathic meds, CBT) - 40-60% improve
- Interventional: Epidural injections (50-70% for radicular pain), RFA for facets
- Neuromodulation: SCS for radicular pain - PROCESS trial shows 50% reduction
- Surgery: ONLY if clear structural pathology (recurrent disc, stenosis, instability)
- Success rates decrease: Primary 80%, 1st revision 60%, 2nd revision 40%, 3rd under 30%
Spinal Cord Stimulation
- Indications: Radicular leg pain, failed 6mo conservative care, no surgical lesion
- Trial mandatory: 5-7 days, success defined as over 50% pain reduction
- Evidence: PROCESS trial - SCS superior to conventional management at 6mo
- Outcomes: 50-70% achieve over 50% pain reduction long-term
- Better for leg pain than back pain, best with favorable psych profile
Prevention Strategies (Mnemonic: PREVENT)
- P - Psychosocial screening preoperatively
- R - Right diagnosis (correlate symptoms with imaging)
- E - Expectations managed (realistic goals discussion)
- V - Verify level intraoperatively (AP and lateral imaging BEFORE incision)
- E - Early mobilization (prevent deconditioning)
- N - Nerve protection (minimize retraction, preserve blood supply)
- T - Tissue preservation (limit dissection, preserve under 50% facets)
High-Yield Exam Points
- FBSS vs surgical failure: FBSS = anatomically successful, failure = technical error
- Gadolinium timing CRITICAL: Early peripheral (scar) vs delayed or none (disc)
- Psychosocial factors predict outcomes MORE than surgical technique
- Multidisciplinary pain programs: Best long-term functional outcomes
- Avoid next operation syndrome: Each surgery lower success, higher risk
- SCS evidence-based (PROCESS trial) for radicular pain post-surgery
Evidence Base
PROCESS Trial: SCS vs Conventional Management
- RCT of 100 FBSS patients with predominant neuropathic radicular leg pain randomised to SCS plus conventional medical management (CMM) versus CMM alone
- At 6 months (intention-to-treat): 24 SCS patients (48%) versus 4 CMM patients (9%) achieved 50% or greater leg pain relief (p under 0.001)
- SCS group had superior leg and back pain relief, quality of life, functional capacity and treatment satisfaction
- Between 6 and 12 months, 32 of the CMM patients crossed over to SCS while only 5 SCS patients crossed to CMM
- By 12 months, 27 SCS patients (32%) had experienced a device-related complication
Peridural Scar and Recurrent Radicular Pain (ADCON-L Study)
- Prospective, randomised, double-blind, multicentre trial of 197 patients after first-time single-level unilateral lumbar discectomy
- Gadolinium-enhanced MRI scar score at 6 months correlated with recurrent radicular pain
- Patients with extensive peridural scar were 3.2 times more likely to experience recurrent radicular pain than those with less scar
- Probability of recurrent radicular pain rose as the MRI peridural fibrosis score increased
- Established a quantifiable imaging link between epidural fibrosis and postoperative radicular pain
Outcomes of Revision Lumbar Discectomy for True Recurrence
- Case-control study comparing 27 patients undergoing revision discectomy for true same-level recurrent herniation with 30 matched primary discectomy controls (validated MODEMS outcome instrument)
- Improvement after revision discectomy was not statistically different from improvement after primary discectomy
- Revision patients had more residual leg numbness/tingling and more frequent back/buttock pain than primary patients
- Authors concluded revision discectomy is as efficacious as primary discectomy in carefully selected patients with clear recurrent herniation
- Supports operating only when a true recurrent disc is identified, not for scar alone
Presurgical Psychological Screening Predicts Spine Surgery Outcome
- Presurgical psychological screening (PPS) applied to 204 patients undergoing lumbar laminectomy/discectomy or fusion
- Combined psychological and 'medical' risk levels were significantly related to outcome; worst results in patients with both high psychological and high medical risk
- PPS surgical-prognosis accuracy for overall outcome was 82%
- Only 9 of 53 patients predicted to have a poor outcome actually achieved a fair or good result
- Authors recommend PPS as a routine part of evaluating chronic pain patients considered for spine surgery
SCS vs Reoperation for Persistent Radicular Pain
- Prospective RCT of 50 patients with persistent radicular pain after lumbosacral surgery, randomised to SCS or reoperation, with crossover permitted
- SCS was more successful than reoperation (9 of 19 versus 3 of 26 patients; p under 0.01)
- Patients randomised to SCS were significantly less likely to cross over than those randomised to reoperation (5 of 24 versus 14 of 26; p = 0.02)
- Reoperation patients required increased opioid analgesics significantly more often than SCS patients
- SCS obviated the need for reoperation in the great majority of patients
Failed Back Surgery Syndrome: Comprehensive Review
- Comprehensive narrative review of FBSS epidemiology, aetiology, evaluation and management
- Despite advances in surgical technology, rates of failed back surgery have not declined
- Contributing factors arise in the preoperative, intraoperative and postoperative periods
- Emphasises prevention and interdisciplinary evaluation as the best strategies to reduce incidence and morbidity
- Presents an evidence-based suggested management pathway incorporating spinal cord stimulation
References
-
Chan CW, Peng P. Failed back surgery syndrome. Pain Med. 2011;12(4):577-606. doi:10.1111/j.1526-4637.2011.01089.x
-
Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1-2):179-188. doi:10.1016/j.pain.2007.07.028
-
Ross JS, Robertson JT, Frederickson RC, et al. Association between peridural scar and recurrent radicular pain after lumbar discectomy: magnetic resonance evaluation. Neurosurgery. 1996;38(4):855-861. doi:10.1097/00006123-199604000-00053
-
Papadopoulos EC, Girardi FP, Sandhu HS, et al. Outcome of revision discectomies following recurrent lumbar disc herniation. Spine (Phila Pa 1976). 2006;31(13):1473-1476. doi:10.1097/01.brs.0000219872.43318.7a
-
Block AR, Ohnmeiss DD, Guyer RD, et al. The use of presurgical psychological screening to predict the outcome of spine surgery. Spine J. 2001;1(4):274-282. doi:10.1016/s1529-9430(01)00054-7
-
Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779-793. doi:10.1016/j.jpain.2006.08.005
-
North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98-107. doi:10.1227/01.neu.0000144839.65524.e0
-
Taylor RS, Ryan J, O'Donnell R, et al. The cost-effectiveness of spinal cord stimulation in the treatment of failed back surgery syndrome. Clin J Pain. 2010;26(6):463-469. doi:10.1097/AJP.0b013e3181daccec
-
Fritsch EW, Heisel J, Rupp S. The failed back surgery syndrome: reasons, intraoperative findings, and long-term results: a report of 182 operative treatments. Spine. 1996;21(5):626-633. doi:10.1097/00007632-199603010-00017
-
Burton CV, Kirkaldy-Willis WH, Yong-Hing K, Heithoff KB. Causes of failure of surgery on the lumbar spine. Clin Orthop Relat Res. 1981;(157):191-199.
-
Slipman CW, Shin CH, Patel RK, et al. Etiologies of failed back surgery syndrome. Pain Med. 2002;3(3):200-214. doi:10.1046/j.1526-4637.2002.02033.x
-
Flum AS, Hickey A, Flum DR. Understanding the psychological factors affecting failed back surgery syndrome: a systematic review. Healthcare (Basel). 2021;9(10):1275. doi:10.3390/healthcare9101275
-
Thomson S, Jacques L. Demographic characteristics of patients with severe neuropathic pain secondary to failed back surgery syndrome. Pain Pract. 2009;9(3):206-215. doi:10.1111/j.1533-2500.2009.00276.x
-
Hussain A, Erdek M. Interventional pain management for failed back surgery syndrome. Pain Pract. 2014;14(1):64-78. doi:10.1111/papr.12035
-
Kumar K, North R, Taylor R, et al. Spinal cord stimulation vs. conventional medical management: a prospective, randomized, controlled, multicenter study of patients with failed back surgery syndrome (PROCESS study). Neuromodulation. 2005;8(4):213-218. doi:10.1111/j.1525-1403.2005.00027.x