IMN Gold Standard | Early Fixation | Rotation Check | Screen for Neck Fx
- Intramedullary nailing is gold standard (reamed, locked)
- Screen for ipsilateral neck fracture - 5% incidence, easily missed
- Early fixation (under 24h) reduces pulmonary complications in polytrauma
- 1-1.5L blood loss expected - resuscitate before and during surgery
- Rotation alignment - check clinically, compare to contralateral side
- “Antegrade for most; retrograde for floating knee, bilateral, pregnancy, obesity
- “Piriformis entry: risk of AVN in young - trochanteric entry safer
- “Damage control: external fixation if physiologically unstable
- “Check rotation intraoperatively - ER malrotation is most common error
5% have ipsilateral femoral neck fracture - easily missed on initial imaging. Get dedicated hip views or CT before nailing. Missing this is a major exam red flag.
Fixation within 24 hours reduces pulmonary complications (ARDS, fat embolism) in polytrauma. Unless physiologically unstable, do not delay definitive fixation.
ER malrotation is most common error. Check rotation intraoperatively: cortical diameter matching, compare to opposite leg, trochanter-patella relationship.
If physiologically unstable (hypothermia, coagulopathy, acidosis), apply external fixation as temporary stabilization. Convert to IMN when stable (24-72h).
- Entry Point
- Antegrade (trochanteric preferred)
- Nail Length
- Long nail
- Key Consideration
- Check for neck fracture
- Entry Point
- Retrograde femur
- Nail Length
- Long nail
- Key Consideration
- Nail tibia separately
- Entry Point
- Retrograde both
- Nail Length
- Long nails
- Key Consideration
- Position supine, easier access
- Entry Point
- Retrograde
- Nail Length
- Long nail
- Key Consideration
- Reduces radiation to pelvis
- Entry Point
- External fixation
- Nail Length
- N/A
- Key Consideration
- Damage control, convert later
- Entry Point
- Antegrade
- Nail Length
- Long nail
- Key Consideration
- Piriformis or trochanteric entry
- Entry Point
- Retrograde or antegrade
- Nail Length
- Long nail
- Key Consideration
- Retrograde gives better distal control
RETROGRADEAntegrade vs Retrograde
Hook:Think RETROGRADE for pregnancy, obesity, bilateral, distal, or floating knee!
SCREENCheck for Neck Fracture
Hook:SCREEN for neck fracture before every femoral shaft nailing!
CORTICESRotation Assessment
Hook:CORTICES - Check rotation intraoperatively, ER malrotation is most common error!
ENTRYEntry Point Choice
Hook:ENTRY point: Trochanteric is safest for most, avoid piriformis in young!
Overview and Epidemiology
Demographics
- Young adults (15-44): High-energy trauma (MVA, motorcycle, GSW)
- Elderly (over 65): Low-energy falls, pathological fractures
- 10-20 per 100,000 population per year
- Male predominance (2:1) in high-energy
- Associated injuries common in polytrauma (50%)
- Motor vehicle accidents (most common)
- Motorcycle crashes
- Falls from height
- Gunshot wounds
- Pedestrian vs vehicle
High-energy mechanisms predominate in the young, low-energy falls in the elderly.
Anatomy and Biomechanics
Femoral Shaft Anatomy
- From 5cm below lesser trochanter
- To supracondylar metaphyseal flare
- Approximately 40-50cm in length
- Anterior bow (apex anterior, radius approximately 120cm)
- Isthmus: narrowest point (9-12mm diameter)
- Linea aspera: posterior ridge (muscle attachments)
- Cortical bone throughout
- Anterior: Quadriceps (encase anterior femur)
- Medial: Adductors
- Posterior: Hamstrings
Understanding muscle attachments helps predict deformity patterns.
Classification
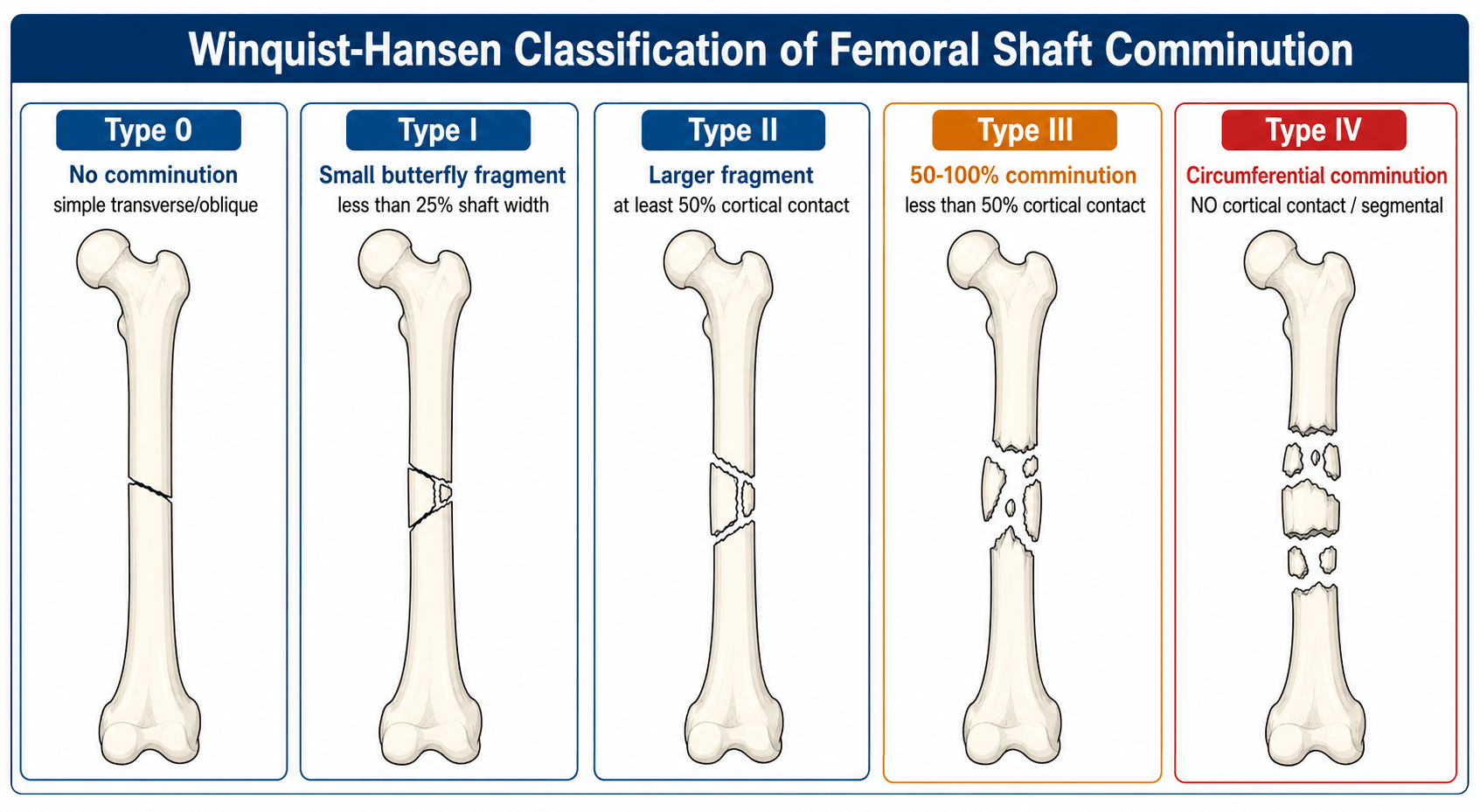
Winquist-Hansen Classification
Describes comminution and guides locking strategy:
- Description
- No comminution
- Stability
- Stable
- Locking
- Dynamic possible
- Description
- Small butterfly (under 25%)
- Stability
- Stable
- Locking
- Dynamic possible
- Description
- Butterfly 25-50%
- Stability
- Moderate
- Locking
- Static preferred
- Description
- Butterfly over 50%
- Stability
- Unstable
- Locking
- Static required
- Description
- Circumferential loss
- Stability
- Very unstable
- Locking
- Static, may need graft
- Dynamic locking: One end unlocked, allows axial compression with weight-bearing. For stable patterns (Grade 0-I).
- Static locking: Both ends locked. For unstable patterns (Grade II-IV). Most femoral shaft fractures should be statically locked initially.
History
History Taking
- High vs low energy
- Direction of force
- Associated injuries likely?
- Position at time of injury
- Age and baseline function
- Comorbidities
- Anticoagulation status
- Previous surgery on this limb
- Social circumstances (recovery needs)
A thorough history guides treatment decisions and expectations.
Examination
Physical Examination
- Thigh swelling (blood loss indicator)
- Shortening and rotation
- Deformity visible
- Skin condition (open vs closed)
- Distal pulses (DP, PT)
- Motor: dorsiflexion, plantarflexion, toe movements
- Sensory: all dermatomes of foot
- Compartments: thigh has 3 compartments
- Hip: pain, ROM if possible
- Knee: effusion, ligament stability (exam under anesthesia often needed)
- ATLS for polytrauma
Document baseline neurovascular status carefully before any intervention.
Investigations
Radiographic Protocol
- Full-length femur (AP and lateral) - MUST include hip and knee
- AP pelvis - screen hip, compare sides
- AP and lateral knee - assess for extension, ligament injury
- Suspicion of ipsilateral neck fracture
- Complex fracture pattern assessment
- Pre-operative planning for difficult cases
- Occult neck fracture if CT inconclusive
- Knee ligament injury assessment
- Usually delayed, not acute
MRI is rarely needed acutely but valuable for occult injuries.

Management

Core Management Principles
- Locked intramedullary nailing for virtually all femoral shaft fractures
- Reamed, locked technique
- Early fixation (within 24 hours if physiologically stable)
- Restore length, alignment, and rotation
- Stable fixation for early mobilization
- Preserve biology where possible
- Stable patient: Definitive IMN within 24 hours
- Unstable patient: Damage control (external fixation), convert when stable
- Early fixation reduces pulmonary complications (ARDS, fat embolism)
Early stabilization is both safe and beneficial in appropriately resuscitated patients.
Surgical Technique

Antegrade Intramedullary Nailing - Standard Approach
- Fracture table with traction (most common)
- OR lateral decubitus on radiolucent table
- Ensure adequate C-arm access
- Piriformis fossa: standard trochanteric tip
- Greater trochanter: for trochanteric entry nails
- Medial to tip of GT, in line with femoral canal
- Position and prep entire limb
- Make 3-5cm incision proximal to GT
- Split gluteus medius in line with fibers
- Identify entry point with awl under fluoro
- Open canal with reamer or awl
- Pass guidewire across fracture
- Ream in 0.5mm increments to 1-1.5mm above nail diameter
- Insert nail over exchange guidewire
- Lock proximally (targeting jig)
- Verify length and rotation
- Lock distally (freehand or jig)
- Final imaging all planes
The antegrade approach is preferred for most femoral shaft fractures due to excellent biomechanical properties.
Complications

Intraoperative Complications
- Most common error (especially ER)
- Prevention: careful intraoperative assessment
- Check cortical diameter, compare to other side
- Avoid excessive force
- Ensure wire doesn't kink in canal
- Retrieve broken hardware
- Can occur during nail insertion
- Maintain reduction during reaming and insertion
- Use fracture table traction
- Entry point comminution
- Distal fracture at nail tip
- Avoid oversized nails in narrow canals
Careful technique and appropriate implant selection minimize these risks.
Postoperative Care
Immediate Postoperative (Days 0-14)
- Neurovascular checks hourly for 4 hours
- Pain management: multimodal analgesia
- DVT prophylaxis: LMWH started 6-12h post-op
- Check post-op X-rays for implant position
- Sit out of bed with physio
- Commence range of motion exercises
- Weight-bearing as per fixation stability
- Most IMN: WBAT (weight-bearing as tolerated)
- Wound care and suture removal at 10-14 days
- Continue DVT prophylaxis (4-6 weeks total)
- Progress mobility with physio supervision
- Monitor for wound complications
Early mobilization is critical to prevent complications and optimize outcomes.
Outcomes and Prognosis
Union Rates
- Result
- 95-98%
- Notes
- Excellent with reamed locked nailing
- Result
- 3-4 months
- Notes
- Simple patterns faster
- Result
- 4-6 months
- Notes
- Depends on occupation
- Result
- 5-15%
- Notes
- Often under 10 degrees, well tolerated
- Result
- 2-5%
- Notes
- Higher in open, comminuted
Prognostic Factors
- Simple fracture pattern
- Closed injury
- Early fixation
- Good reduction
- Compliant patient
- Open fracture (especially Gustilo III)
- Segmental or highly comminuted
- Infection
- Delayed fixation
- Smoking
Differential Diagnosis
The diagnosis of a displaced femoral shaft fracture is usually obvious, but the key clinical task is distinguishing it from injuries that change the surgical plan, and identifying the underlying cause in low-energy or atypical presentations.
- Distinguishing Features
- Often non-displaced, subtle; groin pain; seen on fine-cut CT not always on plain film
- Why It Matters
- Occurs in 1-9% (Tornetta); must fix neck first to avoid osteonecrosis
- Distinguishing Features
- Proximal location; flexed-abducted-ER proximal fragment; needs cephalomedullary device
- Why It Matters
- Different implant and reduction strategy than mid-shaft
- Distinguishing Features
- Apex-posterior gastrocnemius pull; intra-articular extension on CT
- Why It Matters
- May favour retrograde nail or distal locking plate
- Distinguishing Features
- Low-energy mechanism, prodromal pain, lytic/blastic lesion, abnormal bone
- Why It Matters
- Requires staging, biopsy considerations, possible stabilisation of whole bone
- Distinguishing Features
- Lateral cortical beaking, transverse subtrochanteric/diaphyseal line, thigh prodrome, often bilateral
- Why It Matters
- Stop antiresorptive, image contralateral femur, full-length nail
- Distinguishing Features
- Fracture around hip/knee implant; Vancouver/Su classification applies
- Why It Matters
- Implant stability dictates revision vs fixation
- Distinguishing Features
- Knee swelling between two diaphyseal fractures; high vascular/ligament injury rate
- Why It Matters
- Sequenced fixation; screen vascular status
Guidelines, Registries & Global Practice
Global Epidemiology
Femoral shaft fractures follow a bimodal age and mechanism pattern that is consistent across high-income settings: high-energy trauma in young men (road traffic and motorcycle crashes, falls from height) and low-energy fragility or atypical fractures in older, predominantly female patients. In low- and middle-income countries the burden is dominated by road-traffic trauma in young adults, where access to timely intramedullary fixation and image intensification is the principal determinant of outcome.
- Position on Femoral Shaft Fractures
- Reamed locked intramedullary nailing is the reference standard; AO/OTA 32 classification used for description and research
- Evidence Basis
- Expert consensus + RCT data (COTS, Bone)
- Position on Femoral Shaft Fractures
- Early definitive fixation of the diaphyseal femur once resuscitated; lactate/base-deficit-guided 'Early Appropriate Care'
- Evidence Basis
- Level I-III (Bone; Vallier)
- Position on Femoral Shaft Fractures
- Stabilisation by an appropriate team within agreed trauma-network timelines; damage control for the physiologically deranged
- Evidence Basis
- BOAST standards + trauma-network audit
- Position on Femoral Shaft Fractures
- Fix long-bone fractures to allow early mobilisation; manage within a major trauma network; VTE prophylaxis per NG89
- Evidence Basis
- Guideline (GRADE-appraised)
- Position on Femoral Shaft Fractures
- IM nailing standard; trochanteric entry increasingly favoured; retrograde for defined indications
- Evidence Basis
- Cohort + registry data
Registry and Trial Evidence on Timing
The early-fixation paradigm rests on Bone's 1989 randomised trial and has since been refined by the damage-control vs early-total-care debate. The John Hunter Hospital Level-1 trauma centre series (Balogh group) found that a predominantly early-total-care strategy in stable and borderline femoral shaft fracture patients produced fewer ICU and ventilator days and fewer septic complications than the comparator randomised cohort, supporting individualised, resuscitation-driven decision-making rather than reflex damage control.
Thromboprophylaxis and Access to Care
VTE prophylaxis after major lower-limb trauma uses LMWH (e.g. enoxaparin) as the standard agent, typically continued for several weeks, with mechanical prophylaxis as an adjunct and early mobilisation as the cornerstone; precise duration follows regional trauma and thromboprophylaxis guidance. Across well-resourced systems, modern reamed locked nailing achieves union in roughly 95-98% of closed fractures with most patients returning to pre-injury function within about six months; outcome disparities globally are driven chiefly by access to fluoroscopy, sterile implants, and timely surgery rather than by technique selection.
MCQ Practice Points
Q: What is the recommended timing for femoral shaft fracture fixation in a polytrauma patient?
A: Within 24 hours if the patient is physiologically stable. Early fixation reduces pulmonary complications (ARDS, fat embolism). If unstable, damage control with external fixation.
Q: What is the main concern with piriformis entry for antegrade femoral nailing in a young patient?
A: Risk of AVN (avascular necrosis) of the femoral head. The entry violates the blood supply to the femoral head. Trochanteric entry is preferred to avoid this risk.
Q: What associated injury must be screened for in all femoral shaft fractures?
A: Ipsilateral femoral neck fracture - occurs in 5% of cases and is easily missed. Get dedicated hip views or CT before nailing. If present, fix neck first.
Q: What is the most common rotational malalignment error in femoral nailing?
A: External rotation. Up to 5-15% of cases have some malrotation. ER is more common than IR. Check rotation intraoperatively using cortical diameter matching and comparison to contralateral side.
Q: When is retrograde femoral nailing preferred over antegrade?
A: Floating knee (ipsilateral tibia fracture), bilateral femur fractures (easier positioning), pregnancy (less pelvic radiation), morbid obesity (easier access), and some distal third fractures.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old male presents after motorcycle accident with closed femoral shaft fracture, pelvic fracture, and moderate head injury (GCS 13). BP 110/70 after resuscitation. How do you manage the femoral shaft?”
“A 32-year-old female has femoral shaft fracture and ipsilateral tibial shaft fracture after being hit by a car. What is your approach?”
“You are about to nail a femoral shaft fracture when your registrar shows you the CT scan that was done for abdominal trauma - there is a non-displaced femoral neck fracture on the same side. What is your plan?”
Gold Standard Treatment
- Reamed locked intramedullary nailing
- Early fixation (under 24h) in polytrauma
- Long nail preferred for most cases
- Static locking for comminuted patterns
Screen for Neck Fracture (SCREEN)
- 5% have ipsilateral neck fracture
- Easily missed if non-displaced
- CT scan if X-ray unclear
- If present: fix neck FIRST
Entry Point Selection
- Trochanteric: Preferred for most (less AVN risk)
- Piriformis: Avoid in young (AVN risk)
- Retrograde: Floating knee, bilateral, pregnancy, obesity
Rotation Check (CORTICES)
- Cortical diameter matching on fluoro
- Opposite limb comparison
- Trochanter-patella relationship
- ER malrotation most common error
Damage Control Indications
- Hypothermia, coagulopathy, acidosis
- Massive transfusion ongoing
- Apply external fixator temporarily
- Convert to IMN when stable (24-72h)
Evidence Base
Bone (1989): Early vs Delayed Fixation in Polytrauma
- Prospective randomised study of 178 adults comparing early (under 24h) vs delayed reduction and stabilisation of acute femoral fractures.
- In multiply injured patients, delayed stabilisation increased pulmonary complications (ARDS, fat embolism, pneumonia), ICU days, and hospital stay.
- Hospital costs were significantly higher with delayed treatment across all patients.
Vallier (2013): Early Appropriate Care Protocol
- 1443 adults with pelvis, acetabulum, spine, or femur fractures; definitive fixation within 24-48h after resuscitation reduced pulmonary complications.
- Lactate was the most specific predictor of complications; correction of pH to greater than 7.25 within 8 hours reduced pulmonary morbidity.
- Chest injury, number of fractures, and timing of fixation were the key independent variables.
Nicholas/Balogh (2010): Damage Control vs Early Total Care
- Level-1 trauma centre series from John Hunter Hospital of 66 femoral shaft fracture patients categorised by Pape physiology into stable and borderline groups.
- A predominantly early-total-care strategy (used in 98% of stable and 86% of borderline patients) was associated with fewer ICU and ventilator hours and fewer septic complications than the comparator randomised cohort.
- Borderline patients managed with early total care showed a tendency to lower ARDS and multiple-organ-failure rates.