CAM vs Pincer vs Mixed | Alpha Angle Measurement | FADIR Test Gold Standard | Hip Arthroscopy
- CAM impingement from aspherical femoral head with decreased head-neck offset
- Pincer impingement from acetabular overcoverage (focal or global)
- Alpha angle greater than 55 degrees diagnostic for CAM morphology on MRI
- FADIR test (flexion-adduction-internal rotation) has 94-99% sensitivity
- Mixed morphology present in 85% of symptomatic FAI cases
- Labral tears in 86% of FAI patients requiring surgery
- “CAM = femoral problem, Pincer = acetabular problem, Mixed = both
- “Alpha angle measured on lateral femoral head-neck junction
- “Crossover sign indicates anterior acetabular overcoverage (pincer)
- “Hip arthroscopy gold standard for treatment - open surgery declining

CAM is a femoral problem - aspherical head-neck junction with decreased offset. Pincer is acetabular - overcoverage causing rim impingement. Mixed (both) occurs in 85% of symptomatic cases. Know the radiographic signs for each.
Alpha angle greater than 55 degrees indicates CAM morphology. Measured on lateral view (frog-leg or MRI axial oblique). Angle between femoral neck axis and line to point where head becomes aspherical. Critical diagnostic threshold.
Flexion-Adduction-Internal Rotation (FADIR) test has 94-99% sensitivity for FAI. Patient supine, hip flexed to 90 degrees, then adducted and internally rotated. Positive = anterior groin pain. Most sensitive clinical test.
86% of FAI patients have labral tears at time of surgery. CAM causes anterosuperior labral damage from shear forces. Pincer causes posteroinferior labral damage from levering. Address both morphology and labral tear.
- Morphology
- Asymptomatic CAM/pincer on X-ray
- Treatment
- Conservative: activity modification, physio
- Key Pearl
- Not all morphology needs surgery
- Morphology
- CAM morphology, alpha angle greater than 60°
- Treatment
- Hip arthroscopy: femoral osteoplasty
- Key Pearl
- Address CAM bump and labral tear
- Morphology
- Pincer with crossover sign
- Treatment
- Hip arthroscopy: rim trimming
- Key Pearl
- Don't over-resect - risk instability
- Morphology
- Mixed FAI with labral tear
- Treatment
- Hip arthroscopy: combined osteoplasty + labral repair
- Key Pearl
- Most common scenario (85%)
- Morphology
- FAI with Tonnis grade 2-3 arthritis
- Treatment
- Total hip arthroplasty
- Key Pearl
- Arthroscopy contraindicated with OA
CAMCAM - Femoral Morphology Features
Hook:CAM = Capital (femoral head) Asphericity in Males - think of a CAMera bump on the femoral neck
PINCERPINCER - Acetabular Morphology Features
Hook:PINCER pinches the femoral neck between acetabular walls like pincers
Overview and Epidemiology
Femoroacetabular impingement (FAI) is a mechanical hip disorder caused by abnormal contact between the femoral head-neck junction and the acetabular rim during hip motion. This repetitive impingement leads to labral and chondral damage, potentially progressing to early hip osteoarthritis.
Two distinct morphological types:
- CAM impingement: Aspherical femoral head with decreased head-neck offset
- Pincer impingement: Acetabular overcoverage (focal or global)
- Mixed impingement: Combination of both (85% of symptomatic FAI)
FAI is increasingly recognized as a major cause of early hip osteoarthritis in young active patients. Without treatment, repetitive impingement causes progressive labral and chondral damage. Early recognition and intervention may prevent or delay the development of osteoarthritis, though long-term data is still emerging.
Epidemiology:
- Peak age: 20-40 years for symptoms
- CAM type: 3:1 male predominance
- Pincer type: More common in middle-aged females
- Athletes: Higher prevalence in certain sports (soccer, hockey, dancing)
- Morphology prevalence: 10-15% general population (often asymptomatic)
- Activity limitation: Significant impact on young active patients
- Labral tears: Present in 86% of FAI requiring surgery
- Cartilage damage: Chondral lesions in 70% at arthroscopy
- OA progression: May account for 10-15% early hip OA cases
- Sports: Can be career-ending for athletes if untreated
Risk factors for developing symptomatic FAI:
- High-impact sports participation during skeletal development
- Repetitive hip flexion activities (dancers, martial artists)
- Underlying hip dysplasia or acetabular retroversion
- History of Perthes disease or slipped capital femoral epiphysis (SCFE)
- Genetic predisposition (familial clustering observed)
Pathophysiology and Mechanisms
Normal hip anatomy:
The hip is a ball-and-socket joint with exceptional range of motion. Normal anatomy includes:
- Femoral head: Spherical, covered by articular cartilage except at fovea
- Femoral neck: Offset from head creating concave waist at anterior-superior junction
- Head-neck offset: Normal anterior offset allows clearance during flexion and internal rotation
- Acetabulum: Horseshoe-shaped socket covering approximately 40% of femoral head
- Acetabular labrum: Fibrocartilaginous rim deepening socket and sealing joint
The anterior-superior femoral head-neck offset is critical for normal hip mechanics. During hip flexion and internal rotation, this offset allows the femoral neck to clear the acetabular rim. Loss of this offset (CAM morphology) causes abnormal contact and shear forces on the anterosuperior labrum and cartilage.
CAM morphology anatomy:
- Normal
- Spherical
- CAM Morphology
- Aspherical (pistol-grip deformity)
- Clinical Significance
- Loss of clearance during motion
- Normal
- Concave waist anteriorly
- CAM Morphology
- Decreased or absent offset
- Clinical Significance
- Alpha angle greater than 55°
- Normal
- None
- CAM Morphology
- Anterosuperior acetabulum
- Clinical Significance
- Outside-in chondral/labral damage
- Normal
- Smooth articulation
- CAM Morphology
- Shear forces on flexion-IR
- Clinical Significance
- Progressive cartilage delamination
Pincer morphology anatomy:
- Normal
- 40% femoral head coverage
- Pincer Morphology
- Excessive coverage (focal or global)
- Clinical Significance
- Premature rim contact
- Normal
- 15-20° anteversion
- Pincer Morphology
- Retroversion or coxa profunda
- Clinical Significance
- Crossover sign on AP pelvis
- Normal
- None
- Pincer Morphology
- Anterosuperior rim initially
- Clinical Significance
- Rim contact causes levering
- Normal
- None
- Pincer Morphology
- Posteroinferior from levering
- Clinical Significance
- Contre-coup labral tear pattern
CAM impingement causes outside-in damage - the aspherical head impacts the acetabular rim first, then shears into the labrum and cartilage like a snowplow. Pincer impingement causes inside-out damage - the acetabular rim impacts the femoral neck, causing levering and posteroinferior contre-coup labral damage. Understanding this distinction is critical for surgical planning.
Biomechanics of impingement:
The impingement occurs during specific hip positions:
- CAM: Worse with flexion and internal rotation (FADIR position)
- Pincer: Worse with flexion, adduction, external rotation (FABER position)
- Mixed: Symptoms in multiple positions
Normal vs pathological forces:
- Smooth spherical femoral head
- Adequate head-neck offset allows clearance
- Labrum acts as suction seal
- Cartilage experiences compression forces only
- Full range of motion without impingement
- Abnormal bony contact at extremes of motion
- Shear forces damage labrum and cartilage
- Repetitive microtrauma with each hip flexion
- Progressive delamination of cartilage
- Eventually leads to full-thickness cartilage loss
Femoral Version: The Other Side of the Impingement Equation
This topic measures acetabular version in detail (crossover sign, retroversion), but a complete impingement assessment also requires the femoral rotational profile. Femoral version is the rotation of the femoral neck axis relative to the posterior femoral condyles (normal roughly 10-20 degrees of anteversion).
- Reduced femoral anteversion or frank femoral retroversion brings the femoral neck closer to the anterior acetabular rim in flexion and internal rotation, reducing clearance and worsening (or even causing) anterior impingement when the alpha angle is only borderline; it also typically reduces internal rotation on examination.
- Excessive femoral anteversion increases anterior clearance but predisposes to posterior extra-articular impingement and anterior microinstability.
- The combined (McKibbin) index is the sum of femoral version and acetabular version - a low combined value indicates global anterior under-clearance and a high value the reverse - which is why the two must be read together, not in isolation.
Impingement clearance depends on both the femoral and the acetabular rotational profile. Femoral retroversion / reduced anteversion is an often-missed driver of persistent anterior impingement and of failure after an isolated cam osteoplasty - in marked cases a femoral derotation osteotomy, not arthroscopy, is the correct operation. Assess femoral version (CT or MRI rotational profile) alongside the acetabular crossover and centre-edge findings; the McKibbin combined index sums the two.
Classification Systems
FAI Type by Morphology
- Location
- Femoral head-neck
- Radiographic Signs
- Alpha angle greater than 55°
- Labral Pattern
- Anterosuperior tear
- Treatment
- Femoral osteoplasty
- Location
- Acetabular rim
- Radiographic Signs
- Crossover sign, coxa profunda
- Labral Pattern
- Posteroinferior tear
- Treatment
- Acetabular rim trimming
- Location
- Both femur and acetabulum
- Radiographic Signs
- Combined signs
- Labral Pattern
- Anterosuperior + posterior
- Treatment
- Combined osteoplasty
85% of symptomatic FAI cases are mixed type with both CAM and pincer components. Always look for both on imaging. The primary mechanism may be one or the other, but addressing only one component leads to persistent symptoms. Complete assessment requires evaluating both femoral and acetabular morphology.
Clinical Presentation and Assessment
History:
Patients with symptomatic FAI typically present with:
- Pain location: Deep anterior groin pain (85-90% of cases)
- Character: Activity-related, insidious onset
- Aggravating factors: Prolonged sitting (theater sign), getting out of car, squatting, climbing stairs
- Sports: Reduced performance in cutting, pivoting sports
- Mechanical symptoms: Clicking, catching, or giving way (if labral tear present)
- Demographics: Young males, athletes (soccer, hockey)
- Pain pattern: Deep groin pain with high-impact activity
- Movements affected: Hip flexion with internal rotation
- Sports limitation: Reduced ability to change direction quickly
- Progression: Gradual worsening over months to years
- Associated: May have labral tear causing clicking
- Demographics: Middle-aged females, endurance athletes
- Pain pattern: Anterior groin pain with prolonged activity
- Movements affected: Hip flexion, especially in adduction
- Theater sign: Pain after prolonged sitting with hip flexed
- Progression: Slower progression than CAM
- Associated: Posterior labral tears from levering
Physical examination:
- Technique
- Flexion 90°, adduction, internal rotation
- Positive Finding
- Anterior groin pain
- Sensitivity
- 94-99%
- Technique
- Flexion, abduction, external rotation
- Positive Finding
- Groin or lateral pain
- Sensitivity
- 70-80%
- Technique
- Prone, hip extended, measure IR
- Positive Finding
- Less than 20° suggests FAI
- Sensitivity
- Variable
- Technique
- Resisted hip flexion at 30°
- Positive Finding
- Anterior groin pain
- Sensitivity
- 60-70%
- Technique
- Supine, passive hip rotation
- Positive Finding
- Groin pain or clicking
- Sensitivity
- Variable
The FADIR test (Flexion-Adduction-Internal Rotation) is the single most sensitive clinical test for FAI with 94-99% sensitivity. Position the patient supine, flex hip to 90 degrees, then adduct across the body and internally rotate. Reproduction of anterior groin pain is a positive test. This position maximizes impingement at the anterosuperior acetabulum.
Range of motion findings:
- Normal Range
- 120-140°
- Typical FAI Finding
- 90-110°
- Clinical Significance
- Limited by pain at end range
- Normal Range
- 30-40°
- Typical FAI Finding
- Less than 20°
- Clinical Significance
- Most restricted motion in FAI
- Normal Range
- 40-50°
- Typical FAI Finding
- Often preserved
- Clinical Significance
- Helps distinguish from other pathology
- Normal Range
- 40-50°
- Typical FAI Finding
- Usually preserved
- Clinical Significance
- Not typically limited
- Normal Range
- 20-30°
- Typical FAI Finding
- May be painful
- Clinical Significance
- Pain with FADIR position
Gait and posture:
- Usually normal gait pattern (unless severe OA)
- May have antalgic gait with advanced disease
- Sitting posture: May sit with hip abducted and externally rotated to avoid impingement
The C-sign is highly specific for intra-articular hip pathology including FAI. Patient makes a "C" shape with thumb and fingers, placing it over the anterior and lateral hip to indicate deep groin and lateral pain. Distinguishes intra-articular pathology from extra-articular hip pain (bursitis, muscle strains).
Differential diagnosis:
- Hip dysplasia: May coexist with FAI or be separate entity
- Athletic pubalgia: Sports hernia, adductor pathology
- Labral tear without FAI: Traumatic labral injury
- Avascular necrosis: History, risk factors, MRI
- Hip OA: Age, X-ray changes, Tonnis grading
- Inflammatory arthritis: Systemic symptoms, labs
- Iliopsoas tendinitis: Snapping hip, different pain pattern
- Greater trochanteric pain syndrome: Lateral pain, not groin
- Adductor strain: Medial thigh pain
- Lumbar spine: L2-L3 radiculopathy can mimic groin pain
- Stress fracture: Femoral neck stress fracture in runners
- Typical patient
- Young active adult, athlete
- Discriminating features
- Deep groin pain, positive FADIR, reduced internal rotation, cam/pincer on imaging
- Key investigation
- AP pelvis + lateral, MRI/MR arthrogram
- Typical patient
- Young woman, may be active
- Discriminating features
- Lateral/groin pain with activity, apprehension, lateral centre-edge angle under 20-25°
- Key investigation
- AP pelvis, false-profile view
- Typical patient
- Male field-sport athlete
- Discriminating features
- Lower abdominal/adductor pain on resisted sit-up and adduction, no impingement sign
- Key investigation
- Dynamic ultrasound, MRI pubic symphysis
- Typical patient
- Runner, military recruit, RED-S risk
- Discriminating features
- Rest and night pain, antalgic gait, pain on hop test
- Key investigation
- MRI (X-ray often normal early)
- Typical patient
- Steroid/alcohol use, sickle cell, prior trauma
- Discriminating features
- Groin pain, preserved early X-ray, crescent sign late
- Key investigation
- MRI (most sensitive)
- Typical patient
- Older patient
- Discriminating features
- Stiffness, reduced global ROM, joint-space loss, osteophytes
- Key investigation
- Weight-bearing AP pelvis (Tonnis grade)
- Typical patient
- Any age; systemic features
- Discriminating features
- Rest pain, effusion, raised inflammatory markers, fever (septic)
- Key investigation
- ESR/CRP, aspiration if sepsis suspected
- Typical patient
- Any age, back history
- Discriminating features
- Pain not reproduced by hip manoeuvres, neurological signs
- Key investigation
- Lumbar spine MRI
Investigations
FAI Imaging Protocol
Standard views (mandatory):
- AP pelvis: Assess acetabular coverage, crossover sign, center-edge angle
- Frog-leg lateral: Alpha angle measurement, head-neck offset assessment
- False profile: Evaluate anterior coverage
Key measurements:
- Alpha angle (frog-leg lateral): Greater than 55° diagnostic for CAM
- Center-edge angle (AP): Greater than 40° suggests pincer overcoverage
- Crossover sign: Anterior wall crosses posterior wall (acetabular retroversion)
- Tonnis grading: Assess for osteoarthritis (Grade 0-1 for arthroscopy eligibility)
MRI arthrogram is the gold standard for FAI assessment:
- Alpha angle: Measured on axial oblique sequences (most accurate)
- Labral tears: 90% sensitivity with intra-articular gadolinium contrast
- Cartilage damage: Assess for chondral lesions (predictor of outcome)
- Cam deformity extent: Map the CAM lesion circumferentially
- Herniation pits: Synovial herniation into femoral neck (marker of FAI)
Typical MRI findings in FAI:
- Anterosuperior labral tear (CAM pattern)
- Anterosuperior cartilage delamination or defect
- Paralabral cysts (if labral tear present)
- Herniation pit at anterior femoral neck
CT indications (not routine):
- Surgical planning for complex acetabular morphology
- 3D reconstruction to map CAM lesion extent
- Assess bony anatomy when MRI contraindicated
- Measure version and coverage angles precisely
Less sensitive than MRI for soft tissue (labrum, cartilage) assessment.
Dynamic fluoroscopy (during examination under anesthesia):
- Assess impingement location during hip motion
- Guide extent of osteoplasty intraoperatively
- Confirm clearance after CAM resection
- Identify additional impingement sources
Radiographic signs summary:
- View
- Frog-leg lateral or MRI
- Finding
- Angle between neck axis and asphericity point
- Indicates
- CAM morphology
- View
- AP pelvis
- Finding
- Anterior wall lateral to posterior wall
- Indicates
- Acetabular retroversion (pincer)
- View
- AP pelvis
- Finding
- Posterior wall medial to femoral head center
- Indicates
- Relative anterior overcoverage
- View
- AP pelvis
- Finding
- Angle from femoral head center to lateral rim
- Indicates
- Global overcoverage (pincer)
- View
- MRI or frog-leg
- Finding
- Pit at anterior femoral neck
- Indicates
- Marker of chronic FAI
- View
- AP pelvis
- Finding
- Ossicle at anterosuperior rim
- Indicates
- Chronic pincer impingement
Diagnostic local anesthetic injection into the hip joint under fluoroscopy or ultrasound guidance can be very useful. Temporary relief of pain after injection confirms the hip joint as the pain source. Persistent pain suggests extra-articular pathology. Typically combine anesthetic (lidocaine or bupivacaine) with steroid for therapeutic benefit.
Laboratory investigations:
Generally not required unless ruling out inflammatory arthropathy:
- ESR, CRP if inflammatory arthritis suspected
- Rheumatoid factor, anti-CCP if RA suspected
- HLA-B27 if ankylosing spondylitis suspected
FADIRFADIR - Clinical Diagnosis
Hook:FADIR = Position that Forces Anterior impingement and Reproduces pain
Management Algorithm
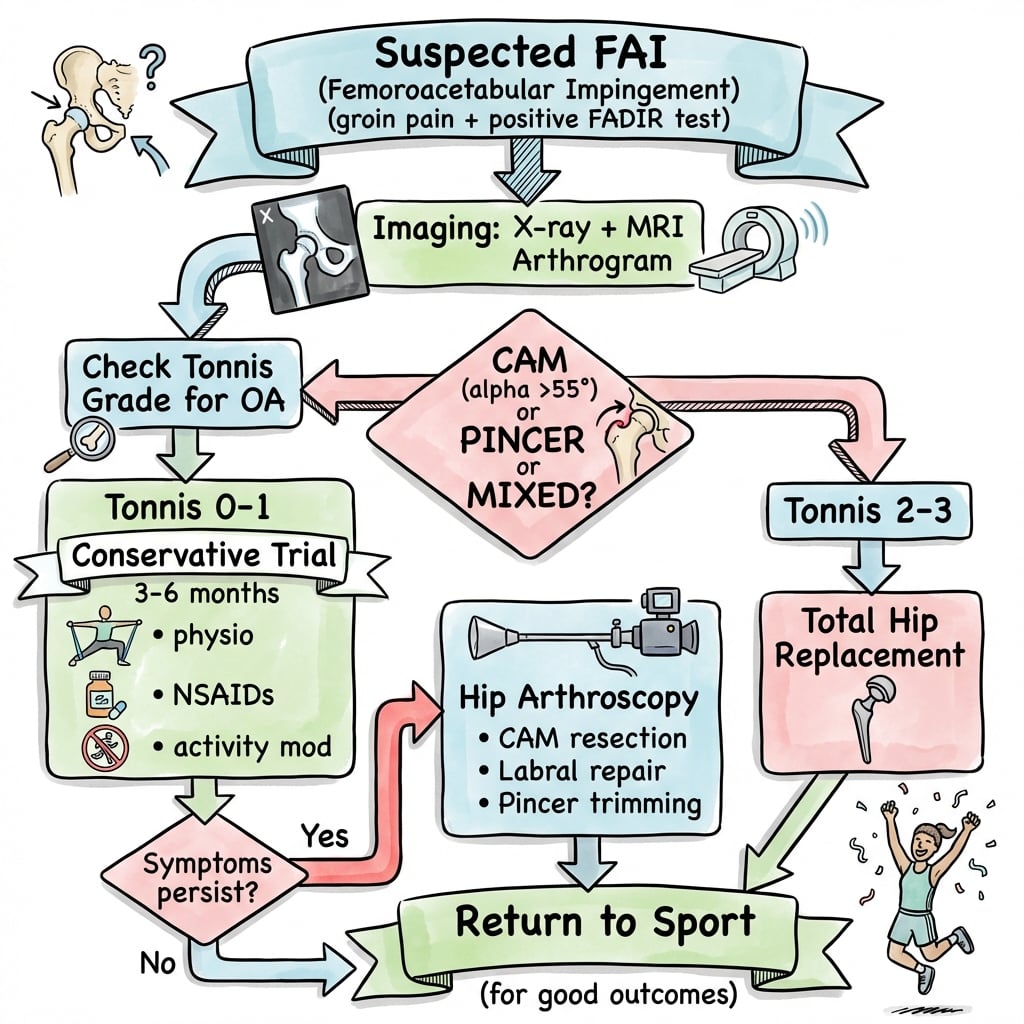
Non-Operative Treatment (First-Line)
All patients should trial conservative management for 3-6 months unless severe mechanical symptoms.
Conservative Treatment Protocol
- Avoid provocative positions: Limit deep flexion, internal rotation
- Modify sports: Reduce high-impact activities temporarily
- Lifestyle changes: Avoid prolonged sitting, low chairs
- Weight management: If overweight, weight loss reduces hip forces
- Education: Understand FAI and realistic expectations
Core strengthening and hip stabilization:
- Gluteal strengthening (avoid aggravating impingement)
- Core stability exercises
- Avoid deep hip flexion exercises
- Posterior chain strengthening
- Proprioception and balance training
Goals: Optimize hip mechanics, reduce compensatory patterns, improve functional capacity
- NSAIDs: Short courses for symptom control
- Paracetamol: Regular for baseline pain control
- Avoid long-term NSAIDs: Risk of gastrointestinal and cardiovascular effects
Not disease-modifying but provides symptom relief during rehabilitation.
Steroid injection (fluoroscopy or ultrasound-guided):
- Diagnostic and therapeutic
- Temporary relief (3-6 months typical)
- May allow participation in physiotherapy
- Can be repeated once if helpful
- Not a definitive treatment for FAI
Contraindications: Infection, severe OA, allergy
Conservative management succeeds in approximately 30-40% of symptomatic FAI patients. Success is more likely in patients with mild morphology (alpha angle 55-65°), no significant labral tear, and good compliance with activity modification and physiotherapy. Failure is indicated by persistent symptoms limiting activities after 3-6 months of appropriate conservative treatment.
Surgical Technique - Hip Arthroscopy

Pre-operative Planning
- Failure to improve symptoms: 15-20% (especially if cartilage damage present)
- Nerve injury: Pudendal, lateral femoral cutaneous (5% transient)
- Heterotopic ossification: 3-5% (usually asymptomatic)
- Infection: Less than 1%
- Conversion to arthroplasty: If severe cartilage damage found intraoperatively
- DVT/PE: Standard orthopedic surgery risk
- Hip arthroscopy traction table (with well-padded perineal post)
- Arthroscopic camera and equipment (30° and 70° scopes)
- Specialized instruments: Curved shavers, burrs, radiofrequency devices
- Fluoroscopy (C-arm positioned for AP and lateral views)
- Labral repair equipment: Suture anchors (2.3mm or smaller)
- CAM resection tools: High-speed burr, arthroscopic osteotomes
Patient Positioning
Setup for Hip Arthroscopy
Supine on specialized hip arthroscopy traction table:
- Well-padded perineal post positioned against medial groin
- Both feet secured in traction boots
- Contralateral leg abducted and secured to allow fluoroscopy
- Operative leg in neutral position initially
Critical padding points:
- Perineal post: Well-padded to prevent pudendal nerve injury
- Lateral femoral cutaneous nerve: Avoid compression at ASIS
- Contralateral leg: Padded at knee and ankle
- Arms: Secured across chest or on arm boards
Maximum traction time: Limit to 2 hours to prevent traction injury
Traction technique:
- Apply approximately 25-50 pounds of traction
- Distract joint 8-10mm (confirmed on fluoroscopy)
- Adequate distraction essential for safe portal placement
- Monitor throughout case, release periodically if greater than 2 hours
Pudendal nerve injury is a recognized complication of hip arthroscopy from excessive or prolonged traction. Risk factors include prolonged traction time (greater than 2 hours), excessive traction force, inadequate perineal post padding, and female gender. Limit traction time and release traction when working in peripheral compartment. Neurapraxia usually resolves within 6 months but can be permanent.
Portal Placement
Standard Hip Arthroscopy Portals
Established under fluoroscopy:
- Identify intersection of horizontal line from superior aspect of greater trochanter and vertical line from ASIS
- Insert spinal needle under fluoroscopy to confirm intra-articular position
- Incise skin, blunt dissection to capsule
- Insert arthroscope sheath and cannula
Primary viewing portal for central compartment
Established under direct visualization:
- Visualize anterolateral capsule with scope from AL portal
- Insert spinal needle from outside-in under direct vision
- Ensure safe distance from lateral femoral cutaneous nerve
- Create working portal with skin incision and blunt dissection
Primary working portal for labral repair and CAM resection
Posterolateral portal: For posterior labral access Distal anterolateral accessory: For peripheral CAM resection
Generally 2-3 portals sufficient for most FAI cases
Central Compartment Work (Under Traction)
Systematic evaluation of central compartment:
Diagnostic Sequence
- Anterosuperior labrum: Most common tear location in CAM FAI
- Posterior labrum: Check for contre-coup pincer lesion
- Classify tear: Radial flap, longitudinal, bucket-handle, degenerative
- Stability testing: Probe to assess for unstable flap
- Acetabular cartilage: Map areas of damage (Beck classification)
- Femoral head cartilage: Usually better preserved than acetabular
- Delamination: Look for carpet phenomenon (cartilage lifted off bone)
- Wave sign: Indicates delaminated cartilage
- Assess for partial or complete tear
- Debride if degenerative and symptomatic
- Not routinely reconstructed
- Remove any loose bodies
- Common in FAI from cartilage delamination
- May be in anterior or posterior recess
Peripheral Compartment Work (Traction Released)
CAM Resection Technique
- Release hip from traction
- Flex and externally rotate hip to expose femoral neck
- Access peripheral compartment between capsule and femoral neck
- May need to perform limited capsulotomy for access
High-speed burr osteoplasty:
- Identify CAM lesion at anterior-superior head-neck junction
- Use high-speed burr to resect aspherical portion of head
- Goal: Restore concave waist at head-neck junction
- Alpha angle target: Reduce to under 50° (confirmed on fluoroscopy)
- Resect conservatively to avoid creating femoral neck notch
Extent of resection:
- Typically anterosuperior quadrant of head-neck junction
- May extend to 1 o'clock to 4 o'clock positions (right hip)
- Smooth transition from head to neck
- Avoid creating stress riser
Fluoroscopic confirmation:
- AP view: Check head-neck offset restored
- Lateral view: Alpha angle under 50-55°
- Dynamic examination: Flex hip and confirm no impingement
- May use arthroscope to visualize from anterolateral portal
If capsulotomy performed:
- Repair capsule with arthroscopic sutures
- Restoration of capsular integrity may reduce post-op instability
- Some surgeons leave capsulotomy open (controversial)
Technical Pearls and Pitfalls
- Preserve labrum whenever possible - repair is better than debridement
- Conservative CAM resection - avoid creating femoral neck notch
- Dynamic fluoroscopy - confirm clearance after osteoplasty
- Limit traction time - release every 2 hours to prevent nerve injury
- Address both components - CAM and pincer if mixed morphology
- Smooth osteoplasty - avoid sharp edges or stress risers
- Over-resect acetabular rim - causes iatrogenic instability
- Create femoral notch - stress riser, risk of neck fracture
- Excessive traction - pudendal nerve injury risk
- Ignore labral tears - address all pathology found
- Incomplete CAM resection - residual impingement leads to failure
- Leave capsulotomy open (controversial) - may increase instability risk
Closure
Closure Steps
- Release traction completely
- Perform final arthroscopic inspection
- Confirm no retained instruments or debris
- Ensure hemostasis achieved
- Remove all cannulas and instruments
- Close portal sites with simple interrupted sutures
- Typically 1-2 sutures per portal (small incisions)
- Apply sterile dressings
- Apply compression dressing
- Ice and elevation
- Mobilize with crutches (partial weight-bearing initially)
- DVT prophylaxis as per protocol
SCOPESCOPE - Hip Arthroscopy Indications
Hook:SCOPE out the right candidates - not everyone with FAI morphology needs arthroscopy
Complications
- Incidence
- 5-8%
- Risk Factors
- Prolonged traction, excessive force
- Management
- Usually resolves 3-6 months, observe
- Incidence
- Less than 1%
- Risk Factors
- Same as above
- Management
- May require nerve specialist referral
- Incidence
- 3-5%
- Risk Factors
- Extensive CAM resection, genetic predisposition
- Management
- Usually asymptomatic, excision if limiting motion
- Incidence
- 15-20%
- Risk Factors
- Severe cartilage damage, persistent morphology
- Management
- May require revision or conversion to THA
- Incidence
- 1-2%
- Risk Factors
- Excessive rim trimming, capsulotomy not closed
- Management
- Activity modification, may need capsular plication
- Incidence
- Less than 1%
- Risk Factors
- Excessive CAM resection creating notch
- Management
- Usually requires ORIF or arthroplasty
- Incidence
- Less than 1%
- Risk Factors
- Standard surgical risk factors
- Management
- Arthroscopic washout, antibiotics
- Incidence
- Less than 1%
- Risk Factors
- Standard orthopedic risk factors
- Management
- Anticoagulation as per protocol
- Incidence
- Less than 1%
- Risk Factors
- Technical error
- Management
- Retrieve broken instrument intraoperatively
Nerve injuries:
The most common nerve injuries in hip arthroscopy are:
- Pudendal nerve: From perineal post pressure or excessive traction (numbness, sexual dysfunction)
- Lateral femoral cutaneous nerve: From portal placement or positioning (lateral thigh numbness)
- Sciatic nerve: From traction or positioning (rare)
- Femoral nerve: Very rare
Heterotopic ossification (HO) occurs in 3-5% of hip arthroscopy cases, usually asymptomatic. Risk factors include extensive CAM resection, history of HO, male gender, and genetic predisposition. Prophylaxis is controversial - options include indomethacin 75mg daily for 2-3 weeks or single-dose radiation (7 Gy). Not routinely used by all surgeons. More common in revision cases or after open surgery.
Failure to improve symptoms:
The most common "complication" is failure to achieve symptom improvement (15-20% of cases). Causes include:
- Severe cartilage damage at surgery (Outerbridge grade 3-4)
- Incomplete correction of morphology (residual impingement)
- Progression of osteoarthritis despite surgery
- Incorrect diagnosis (pain from other source)
- Unrealistic patient expectations
- Poor rehabilitation compliance
Prevention: Careful patient selection (Tonnis 0-1, confirmed FAI morphology, mechanical symptoms), complete correction of both CAM and pincer, realistic counseling.
Femoral neck fracture after CAM resection is rare (less than 1%) but devastating. Risk factors include excessive resection depth (greater than 30% neck diameter), creating a notch at the femoral neck, and early weight-bearing before healing. Prevention: Conservative resection depth, smooth gradual transition from head to neck, avoid creating sharp corners or notches, protected weight-bearing for 6 weeks post-op.
Hip Microinstability and Capsular Management
The complication table lists "iatrogenic instability" and an unrepaired "capsulotomy" as risks, and the labral-repair literature cites reduced "microinstability" - concepts the topic relies on but never develops. Hip microinstability is symptomatic, extra-physiological motion of the femoral head within the socket without frank dislocation, and the hip resists it through three structures this surgery can compromise:
- The capsule, principally the iliofemoral ligament (Y-ligament of Bigelow), the strongest anterior stabiliser limiting external rotation and extension - divided by the interportal or T-capsulotomy used for access.
- The labral suction seal, which maintains negative intra-articular pressure and fluid sealing - lost if the labrum is debrided rather than repaired (the mechanism behind the better outcomes of labral repair).
- The bony architecture - which is why over-resecting the acetabular rim (iatrogenic under-coverage) destabilises the joint.
Capsular management is therefore part of the operation, not an afterthought: many surgeons now repair or plicate the capsule, particularly in patients with ligamentous laxity, borderline acetabular coverage, or revision surgery, although routine closure remains debated.
Hip arthroscopy can create microinstability by three mechanisms: over-resecting the acetabular rim (bony under-coverage), debriding rather than repairing the labrum (losing the suction seal), and leaving a large capsulotomy unrepaired (losing the iliofemoral-ligament restraint). In patients with ligamentous laxity or borderline dysplasia the threshold for capsular repair/plication and labral preservation - and against aggressive rim resection - is lower. The aim is to relieve impingement without destabilising the joint.
Postoperative Care and Rehabilitation
Hip Arthroscopy Rehabilitation
Protection phase:
- Partial weight-bearing with crutches (20-30 pounds foot-flat)
- Hip brace optional (some surgeons, especially if capsulotomy)
- Ice and elevation
- DVT prophylaxis (aspirin or LMWH as per protocol)
- Pain management (multimodal analgesia)
- Passive ROM exercises (avoid extremes)
- Avoid hip flexion greater than 90°, avoid combined flexion-IR
Progressive weight-bearing:
- Week 2: Increase to 50% weight-bearing if comfortable
- Week 4: Wean off crutches to full weight-bearing
- Week 6: Should be walking normally without aids
ROM exercises:
- Gentle active-assisted ROM
- Supine hip flexion to 90° (avoid end-range flexion)
- Hip abduction and extension exercises
- Avoid combined flexion and internal rotation (impingement position)
Stationary cycling: Start at 3-4 weeks (high seat position)
Progressive loading:
- Advance ROM exercises (gradual increase in flexion)
- Begin closed-chain strengthening (squats, leg press - limited depth)
- Hip abductor strengthening (gluteus medius focus)
- Core stability exercises
- Pool exercises if available
- Avoid impact activities
Goals: Full ROM, normalized gait, good hip control
Sport-specific training:
- Progress to jogging (flat surface) at 3 months
- Agility and cutting drills at 4-5 months
- Sport-specific training at 5 months
- Return to full sport at 6 months if strength testing adequate
Criteria for return:
- Pain-free full ROM
- Hip strength 90% of contralateral side
- Functional testing: Single-leg squat, hop tests
- No effusion or mechanical symptoms
- Continue hip strengthening indefinitely
- Avoid high-impact activities if possible (controversial)
- Monitor for symptom recurrence
- Follow-up X-rays at 1 and 2 years (assess for OA progression)
Key rehabilitation principles:
- Protected weight-bearing first 6 weeks
- Progressive ROM avoiding impingement positions
- Hip strengthening focus on gluteal muscles
- Patience - full recovery takes 6-12 months
- Communication with therapist about procedure details
- Criteria-based progression not time-based
- Early full weight-bearing risks femoral neck stress
- Aggressive ROM early risks labral repair failure
- Return to sport too early increases failure risk
- Ignore persistent symptoms - may indicate problem
- Skip strengthening - hip control is critical
- Resume high-impact too soon - need full healing
Outcomes and Prognosis
Outcomes with modern hip arthroscopy:
Modern hip arthroscopy for FAI produces good to excellent outcomes in approximately 85% of appropriately selected patients at 2-year follow-up. Patient satisfaction is high, with significant improvements in pain, function, and return to sport.
- 2-Year Success
- Greater than 90%
- Prognostic Factors
- Age under 40, alpha angle 55-70°, Tonnis 0, minimal cartilage damage
- 2-Year Success
- 80-90%
- Prognostic Factors
- Age 40-50, mixed morphology, Tonnis 0-1, moderate cartilage damage
- 2-Year Success
- 60-70%
- Prognostic Factors
- Age over 50, Tonnis 1, significant cartilage damage (Outerbridge 3)
- 2-Year Success
- Less than 50%
- Prognostic Factors
- Tonnis 2-3, severe cartilage loss, unrealistic expectations
Return to sport:
- Recreational athletes: 80-90% return to sport at 6-12 months
- Elite/professional athletes: 70-85% return to pre-injury level
- Contact sports: May have lower return-to-play rates
- Time to return: Average 6 months (range 4-12 months)
Poor prognostic factors for hip arthroscopy in FAI:
- Tonnis grade 2-3 osteoarthritis - strongest negative predictor
- Severe cartilage damage (Outerbridge grade 3-4 or Beck grade 3-4)
- Age over 50 years - lower success rates
- Severe joint space narrowing (less than 2mm)
- Worker's compensation claim - psychosocial factor
- Isolated pincer morphology - worse than CAM or mixed
- Previous hip surgery - revision cases have worse outcomes
These patients should be counseled about higher failure risk and potential need for arthroplasty.
Long-term outcomes and OA progression:
The critical question: Does FAI surgery prevent osteoarthritis?
- Short-term (2-5 years): High satisfaction, improved function
- Medium-term (5-10 years): Good outcomes maintained in most
- Long-term (10+ years): Data emerging - 20-30% may develop OA despite surgery
Factors affecting OA progression:
- Severity of cartilage damage at surgery (most important)
- Completeness of morphology correction
- Age at surgery (younger better for prevention)
- Genetic factors and joint loading patterns
While hip arthroscopy for FAI improves symptoms and function, it may not prevent progression to osteoarthritis in all patients, especially those with significant cartilage damage at time of surgery. The goal is to improve symptoms and delay OA progression, not necessarily prevent it entirely. Long-term studies (15-20 years) are still lacking.
- Incidence: 10-15% require revision within 5 years
- Reasons: Incomplete initial correction, progression of cartilage damage, adhesions
- Outcomes: Revision surgery has lower success rates (60-70%) than primary
- Rate: 5-10% progress to THA within 10 years
- Risk factors: Severe cartilage damage at index surgery, older age, incomplete correction
- Timing: Average 5-7 years after failed arthroscopy
Guidelines, Registries & Global Practice
Global epidemiology:
- Finding
- Common; markedly higher in male athletes performing high-impact sports during skeletal maturation
- Source population
- Imaging cohorts and athlete screening studies
- Finding
- Moderate cam (alpha over 60°) adjusted OR 3.67; severe cam (alpha over 83°) adjusted OR 9.66 within 5 years
- Source population
- CHECK cohort, Ann Rheum Dis 2013 (PMID 22730371)
- Finding
- Most people with cam/pincer morphology are asymptomatic - morphology alone is NOT FAI syndrome
- Source population
- Warwick Agreement, Br J Sports Med 2016 (PMID 27629403)
- Finding
- Cam-predominant FAI more common in young men; pincer-predominant pattern described more in middle-aged women
- Source population
- Clinical cohorts (descriptive)
The defining, registry- and cohort-level numbers for FAI are the CHECK cohort odds ratios for cam-driven OA and the FASHIoN / FAIT treatment-effect sizes. Quote these with their sources. Precise single-figure "prevalence", "satisfaction" and "return-to-sport" percentages vary widely between studies and populations - present them as ranges or attribute them, never as universal facts.
Major guidelines and consensus, side by side:
- Position on diagnosis
- FAI syndrome = symptoms + clinical signs + imaging (cam/pincer); incidental morphology is not a disease
- Position on treatment
- Conservative care/rehabilitation AND arthroscopic or open surgery are all legitimate options
- Evidence basis
- Expert consensus (Level V), PMID 27629403
- Position on diagnosis
- FAI is a recognised cause of young-adult hip pain warranting structured assessment
- Position on treatment
- Open and arthroscopic FAI surgery supported for use with standard arrangements for governance and audit
- Evidence basis
- Procedure-specific review
- Position on diagnosis
- Diagnosis as per Warwick; exclude established OA (KL grade 2 or more) and dysplasia
- Position on treatment
- Arthroscopy gives a clinically meaningful benefit over physiotherapy in referred secondary/tertiary patients
- Evidence basis
- Level 1, PMID 29893223 and 30733197
- Position on diagnosis
- Confirm intra-articular source (e.g. diagnostic injection) before surgery
- Position on treatment
- Trial structured physiotherapy first; reserve surgery for confirmed, refractory, Tonnis 0-1 disease
- Evidence basis
- Cohort and consensus
No major national body publishes a prescriptive step-by-step FAI algorithm. The Warwick Agreement is the closest thing to a global standard and is endorsed by societies across the UK, USA, Europe, Australasia and beyond. Examiners worldwide expect the symptom-sign-imaging triad and the principle that imaging morphology without symptoms is not treated.
Registry evidence:
Unlike arthroplasty, FAI/hip-preservation surgery is tracked mainly through dedicated hip arthroscopy registries rather than the national joint replacement registries. The most informative is the Danish Hip Arthroscopy Registry (DHAR), which reported significant improvements in HAGOS, EQ-5D and pain scores across 2054 procedures (PMID 28630739). National joint replacement registries (NJR, AJRR, AOANJRR, SHAR, NZJR) become relevant only once FAI has progressed to end-stage OA requiring total hip arthroplasty, where they inform implant and bearing selection.
Global practice variation:
- Hip arthroscopy concentrated in specialist hip-preservation and sports units with traction tables and intra-operative fluoroscopy
- MRI arthrogram and 3D CT readily available for planning
- Strong emphasis on labral preservation/repair and capsular management
- Access still varies by funding model and surgeon volume
- Diagnosis may rest on history, examination and plain radiographs (alpha angle, crossover sign, Tonnis grade)
- Structured physiotherapy and activity modification are the mainstay first-line treatment everywhere
- Arthroscopy availability limited by equipment and trained surgeons; open surgical dislocation may be used where expertise exists
- End-stage disease managed with arthroplasty as elsewhere
Regardless of health system, consent for hip arthroscopy should cover: transient nerve injury (commonly quoted around 5-8%, usually traction-related and resolving), permanent nerve injury (under 1%), heterotopic ossification (around 3-5%), infection (under 1%), failure to improve (commonly 15-20%, higher with cartilage damage), iatrogenic instability or femoral neck fracture from over-resection, and possible future conversion to arthroplasty. Document the conservative trial, patient-selection criteria (Tonnis grade, alpha angle, symptoms) and realistic expectations.
MCQ Practice Points
Q: What are the two main morphological types of femoroacetabular impingement? A: CAM impingement (aspherical femoral head with decreased head-neck offset) and Pincer impingement (acetabular overcoverage, focal or global). Mixed morphology with both CAM and pincer components is present in 85% of symptomatic FAI cases.
Q: What is the diagnostic threshold for CAM morphology based on alpha angle measurement? A: Alpha angle greater than 55 degrees is diagnostic for CAM morphology. The alpha angle is measured on frog-leg lateral X-ray or MRI axial oblique view. It represents the angle between the femoral neck axis and the point where the femoral head becomes aspherical. Normal is under 50-55 degrees.
Q: Which clinical test has the highest sensitivity for diagnosing FAI and how is it performed? A: The FADIR test (Flexion-Adduction-Internal Rotation) has 94-99% sensitivity. Patient supine, flex hip to 90 degrees, then adduct across the body and internally rotate. Positive test = reproduction of anterior groin pain. This position maximizes impingement at the anterosuperior acetabulum.
Q: What is the crossover sign and what does it indicate? A: The crossover sign is when the anterior acetabular wall projects lateral to (crosses over) the posterior wall on AP pelvis X-ray. It indicates acetabular retroversion (focal anterior overcoverage), a type of pincer morphology. Normal acetabulum has anterior wall medial to posterior wall throughout.
Q: What is the contraindication to hip arthroscopy for FAI based on osteoarthritis status? A: Tonnis grade 2-3 osteoarthritis is a contraindication to hip arthroscopy. Only Tonnis grade 0-1 (no OA or mild OA) should be considered for arthroscopy. Patients with established OA (grade 2-3) have poor outcomes with arthroscopy and should be offered total hip arthroplasty instead.
Q: In hip arthroscopy for FAI, is labral repair or labral debridement preferred, and why? A: Labral repair is preferred over labral debridement where the tissue is repairable. The labrum functions as a suction seal maintaining negative intra-articular pressure and reducing microinstability. Meta-analysis data show repair trends toward better patient-reported outcomes, pain and satisfaction than simple debridement, with comparable complication rates. Preserve the labral seal whenever possible; debridement remains acceptable for irreparable or degenerate tissue.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old semi-professional soccer player presents with 12 months of progressive right groin pain. Pain is worse with running, changing direction, and getting out of his car. He has tried rest and physiotherapy without improvement. On examination, he has a positive FADIR test reproducing his groin pain. X-rays show an alpha angle of 68 degrees on frog-leg lateral view. What is your assessment and management?”
“You are planning hip arthroscopy for a 32-year-old female with mixed CAM-pincer FAI and anterosuperior labral tear on MRI. Alpha angle is 62 degrees, and she has crossover sign indicating acetabular retroversion. Tonnis grade 0. Walk me through your surgical approach and decision-making.”
“A 45-year-old patient had hip arthroscopy for FAI 18 months ago with CAM osteoplasty and labral debridement. She initially improved for 6 months but now has recurrent groin pain, mechanical symptoms, and limited hip flexion. X-rays show alpha angle now 52 degrees (was 70 degrees pre-op), but joint space has narrowed from 4mm to 2mm with Tonnis grade 2 changes. What is your assessment and management?”
Key Anatomy and Biomechanics
- Normal head-neck offset = concave waist at anterosuperior junction allows clearance
- CAM = aspherical femoral head, decreased offset, shear forces cause outside-in damage
- Pincer = acetabular overcoverage, rim contact causes inside-out damage via levering
- Labrum = suction seal maintaining negative intra-articular pressure and load distribution
- Impingement zone: CAM damages anterosuperior labrum/cartilage, pincer damages posteroinferior
Classification and Diagnosis
- CAM (25%) = alpha angle greater than 55°, male predominance 3:1
- Pincer (10%) = crossover sign, coxa profunda, center-edge angle greater than 40°
- Mixed (85%) = both CAM and pincer components - most common
- FADIR test = 94-99% sensitivity (flex 90°, adduct, internal rotate)
- Tonnis 0-1 = arthroscopy candidate, Tonnis 2-3 = contraindication (need THA)
Imaging and Measurements
- X-rays: AP pelvis + frog-leg lateral (alpha angle, crossover sign, Tonnis grade)
- Alpha angle greater than 55° = CAM morphology (measure on frog-leg or MRI)
- MRI arthrogram = gold standard (labral tears 90% sensitivity, cartilage assessment)
- Crossover sign = anterior wall crosses posterior wall (acetabular retroversion)
- Center-edge angle greater than 40° = pincer overcoverage
Treatment Algorithm
- Conservative first: 3-6 months physio, activity modification, NSAIDs (30-40% success)
- Surgery if: failed conservative, confirmed morphology, Tonnis 0-1, positive FADIR
- Hip arthroscopy (95% of cases): CAM osteoplasty + labral repair + pincer trimming if needed
- Target: alpha angle under 50°, center-edge angle 25-35° if pincer resection
- Contraindications: Tonnis 2-3 OA, active infection, severe dysplasia, unrealistic expectations
Surgical Pearls and Complications
- Labral repair preferred to debridement where repairable (better pain/function/satisfaction on meta-analysis; restores suction seal)
- Conservative resection: avoid femoral notch (fracture risk) or over-trimmed rim (instability)
- Limit traction under 2 hours (pudendal nerve injury risk 5-8% transient, less than 1% permanent)
- Post-op: partial weight-bearing 6 weeks, return to sport 6 months if criteria met
- Complications: nerve injury 5-8%, HO 3-5%, failure to improve 15-20%, revision 10-15% at 5 years
Key Evidence and Outcomes
- FASHIoN (Lancet 2018) and FAIT (BMJ 2019): arthroscopy superior to physiotherapy (Level 1)
- Warwick Agreement: diagnose FAI syndrome on symptoms + signs + imaging triad (not morphology alone)
- Poor predictors: Tonnis grade 2-3, severe cartilage damage, age over 50, worker's comp
- Long-term: 20-30% may develop OA by 10 years despite surgery
- Conversion to THA: 5-10% within 10 years, higher if severe cartilage damage at index surgery
Evidence Base and Key Trials
CHECK Cohort - Cam Morphology and Incident Hip Osteoarthritis
- Nationwide prospective cohort of 1002 patients with early symptomatic OA (CHECK), with standardised radiographs at baseline, 2 and 5 years
- Moderate cam deformity (alpha angle over 60 degrees) gave an adjusted OR of 3.67 (95% CI 1.68-8.01) for end-stage OA within 5 years
- Severe cam deformity (alpha angle over 83 degrees) gave an adjusted OR of 9.66 (95% CI 4.72-19.78) for end-stage OA
- Severe cam plus reduced internal rotation (20 degrees or less) gave a 52.6% positive predictive value for end-stage OA
- Only 2.76% of hips developed end-stage OA overall, so most cam morphology does NOT progress quickly
UK FASHIoN Trial - Hip Arthroscopy vs Personalised Hip Therapy
- Pragmatic multicentre RCT across 23 UK NHS hospitals: 348 participants randomised (171 hip arthroscopy, 177 personalised hip therapy)
- Primary outcome: hip-related quality of life (iHOT-33) at 12 months
- iHOT-33 improved 39.2 to 58.8 (arthroscopy) versus 35.6 to 49.7 (physiotherapy)
- Adjusted mean difference 6.8 points (95% CI 1.7-12.0) favouring arthroscopy, exceeding the 6.1-point minimum clinically important difference
- Both treatments improved hip-related quality of life; one post-surgical hip joint infection reported
FAIT Trial - Arthroscopic Surgery vs Physiotherapy and Activity Modification
- Two-group assessor-blinded pragmatic RCT across seven NHS England sites: 222 participants aged 18-60 (112 arthroscopy, 110 physiotherapy and activity modification)
- Primary outcome: Hip Outcome Score Activities of Daily Living (HOS-ADL) subscale at 8 months
- Adjusted HOS-ADL was 10.0 points higher (95% CI 6.4-13.6) in the surgery group, exceeding the 9-point minimum clinically important difference
- Patients with established osteoarthritis (Kellgren-Lawrence grade 2 or more) and dysplasia (centre-edge angle under 20 degrees) were excluded
- No serious adverse events reported in either group
Labral Debridement vs Repair - 10-Year Survivorship
- Single-surgeon prospective cohort with minimum 10-year follow-up: 79 labral repair and 75 labral debridement hips (94% followed)
- 50 patients (34%) underwent total hip arthroplasty within 10 years
- Independent predictors of conversion to THA: increased age, joint space 2 mm or less (HR 4.26), and acetabular microfracture
- After adjustment, no significant difference in THA hazard or outcome scores between repair and debridement
- Both groups had large, durable improvements in HOS, modified Harris Hip Score and SF-12 in hips that survived
Labral Repair vs Debridement - Meta-analysis
- Systematic review and meta-analysis of five studies (four observational, one RCT) comparing arthroscopic labral repair and debridement
- Modified Harris Hip Score, VAS pain and satisfaction favoured labral repair (statistically significant)
- Non-Arthritic Hip Score, failure rate and complication rate did not differ significantly between the two techniques
- Repair is proposed to better re-create the suction-seal effect and reduce microinstability
- Low to moderate risk of bias across included studies
Danish Hip Arthroscopy Registry (DHAR) - National Outcomes
- National web-based prospective registry: 2054 FAI procedures in 1835 patients (219 bilateral), 2012-2015
- Radiographic definitions used: cam = alpha angle over 55 degrees, pincer = lateral centre-edge angle over 35 degrees
- All Copenhagen Hip and Groin Outcome Score (HAGOS) subscales improved significantly at 1 and 2 years
- EQ-5D improved 0.66 to 0.78 and Hip Sports Activity Scale 2.5 to 3.3 by 2 years
- Pain scores fell (NRS-rest 39 to 17, NRS-walk 49 to 22)
Warwick Agreement - International Consensus on FAI Syndrome
- International multidisciplinary consensus: 22 panellists and 1 patient from 9 countries and 5 specialties, endorsed by 25 clinical societies
- Introduced the term 'FAI syndrome' to emphasise that symptoms - not morphology alone - define the disorder
- Diagnosis requires a triad: appropriate symptoms, positive clinical signs, and imaging findings of cam or pincer morphology
- Endorsed treatment options of conservative care/rehabilitation and arthroscopic or open surgery
- Imaging morphology in an asymptomatic person is NOT FAI syndrome and should not be treated