Nail Bed Repair and Local Flaps
- Defects less than 1cm with NO exposed bone heal excellently by secondary intention.
- Exposed bone requires flap coverage or shortening.
- The Germinal Matrix produces the nail plate; the Sterile Matrix allows adherence.
- Germinal Matrix scarring causes SPLIT nail.
- Sterile Matrix scarring causes NON-ADHERENT nail.
- A Hook Nail results from loss of bony support to the nail bed tip.
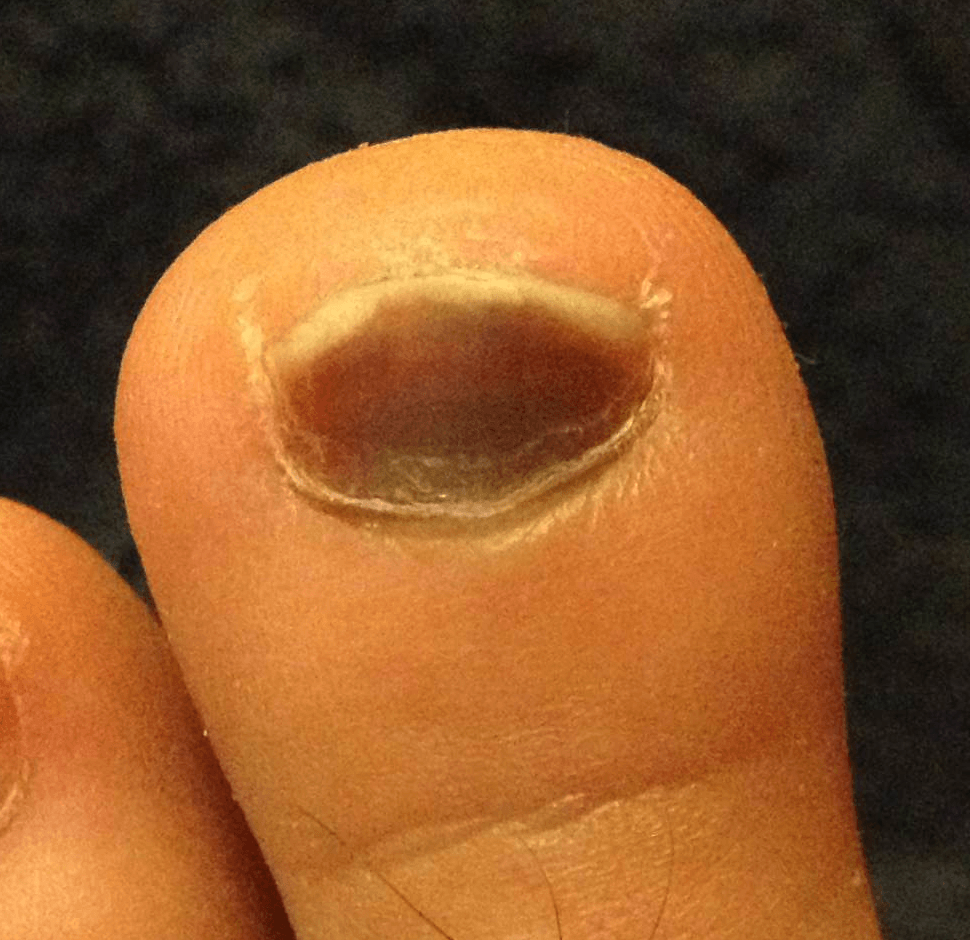
- Subungual hematoma greater than 50% does NOT mandate removal unless nail plate is disrupting the fold.
- “Moberg flap is for the THUMB only (Dorsal blood supply allows volar advancement).
- “Never advance Volar skin on a standard finger greater than 1cm (Necrosis risk).
- “Trephination is for pain relief, not volume reduction.
Overview
Fingertip injuries are defined as those occurring distal to the insertion of the Flexor Digitorum Profundus (FDP) and Extensor tendons. They involve the specialized organs of the nail complex and the highly sensate digital pulp.
The goal of treatment is to restore a functional, sensate, and non-painful tip. While complex reconstruction (flaps) is elegant, simple management (secondary intention) often yields superior functional and cosmetic results for small defects.
Pathophysiology and Mechanisms
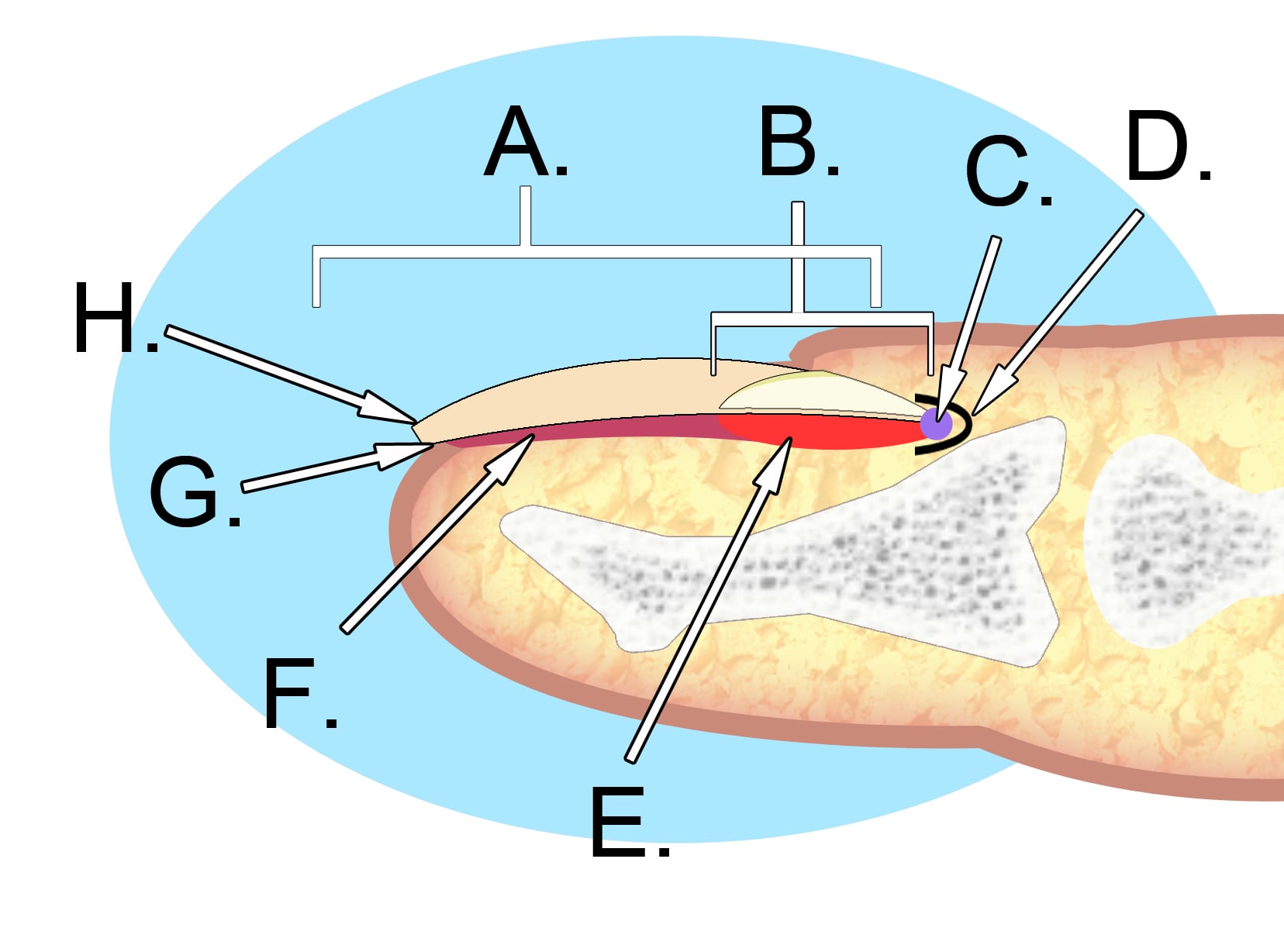
The Perionychium
- Nail Plate: Hard keratin structure.
- Germinal Matrix: Proximal section (under the fold). Produces 90% of the nail plate. Injury here causes the nail to stop growing or split.
- Sterile Matrix: Distal section (under the plate, distal to lunula). Produces a thin layer of keratin that adheres the plate to the bed. Injury here causes non-adherence.
- Hyponychium: Thickened skin at the distal edge, a barrier to infection.
- Eponychium: Dorsal skin fold (cuticle).
- Paronychium: Lateral skin folds.
The germinal matrix extends proximally to the insertion of the extensor tendon.
Classification Systems
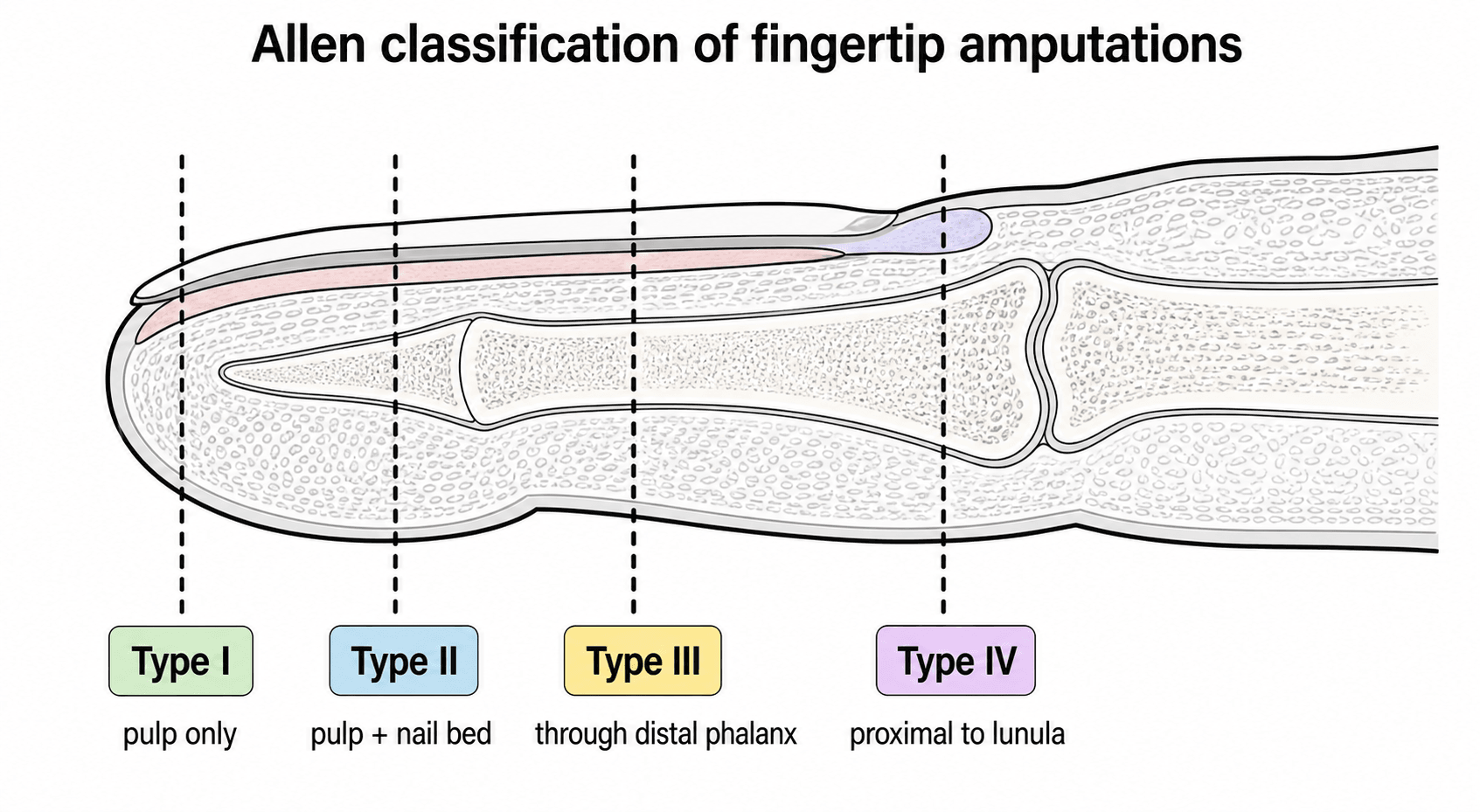
Allen Classification
- Type I: Pulp only. (No bone exposed).
- Type II: Pulp + Nail bed. (Bone exposed).
- Type III: Partial loss of distal phalanx.
- Type IV: Proximal to lunula (Germinal matrix loss).
Type I and II are the most amenable to conservative management.
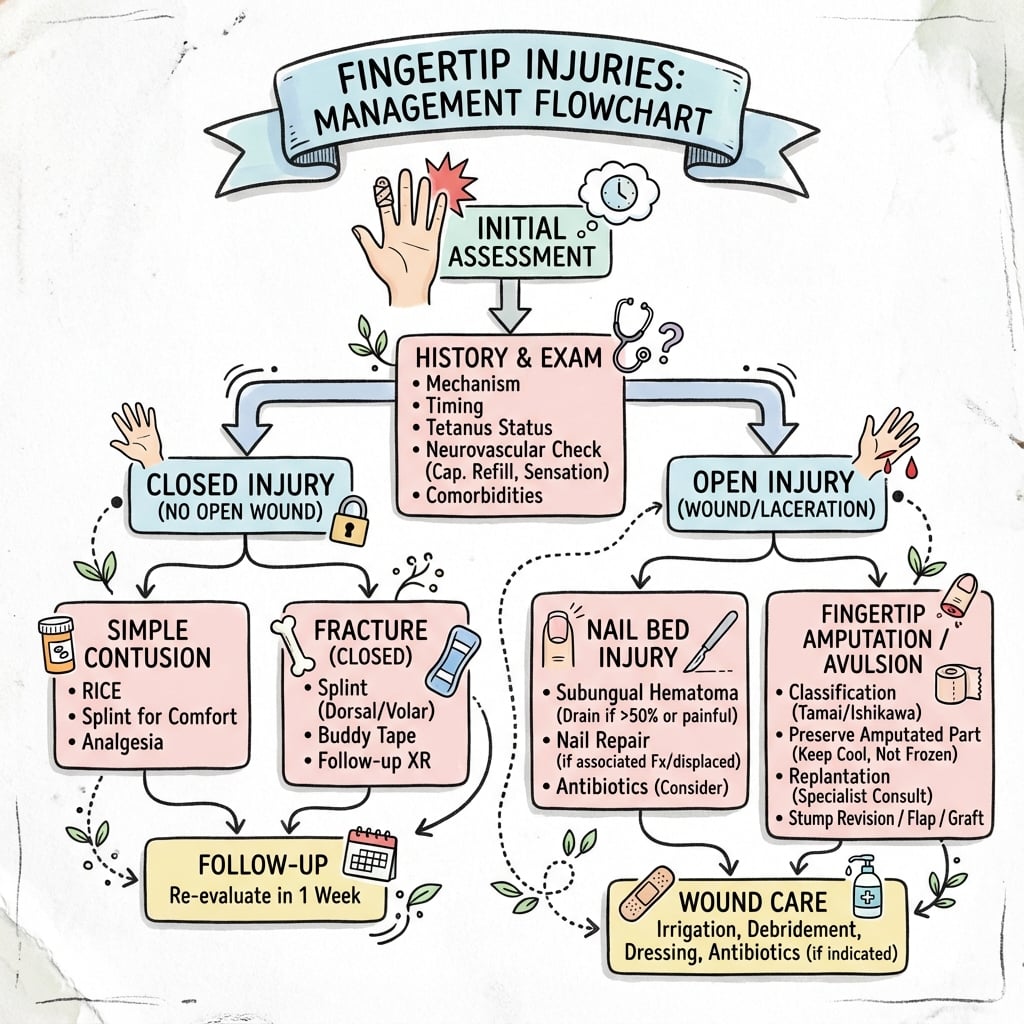
Clinical Presentation
Fingertip injuries present acutely after a clearly remembered mechanism — a crush (door, hammer), a sharp laceration (knife, saw) or an avulsion (ring, pulling). The patient reports throbbing pain, bleeding and an obvious deformity or tissue loss. The key clinical task is rapid triage into a treatable category: is there exposed bone, is the nail bed disrupted, and is there a concealed tendon injury (loss of active DIP flexion or extension)? Sensation and perfusion of the tip must be documented before any local anaesthetic is given.
History
History Factors
- Mechanism: Crush (burst nail bed) vs Laceration (clean cut) vs Avulsion (pulling).
- Time: How long since injury? Clean wounds can be closed up to 12-24 hours.
- Occupation: Manual labourer (needs durable tip) vs Pianist (needs sensation/shape).
- Hand Dominance: Right or left handed? Index/Thumb are critical.
- Hobbies: Musical instruments, sports, fine motor activities.
- Smoker: Risk for flap necrosis. Counsel for cessation.
- Diabetes: Impaired healing, infection risk.
- Medications: Anticoagulants, immunosuppressants.
Smoking cessation is critical for flap survival (Moberg/Atasoy).
Examination
Physical Examination
- Bone Exposure: Look carefully. Probe the wound. Small exposed tufts may granulate.
- Nail Bed: Check for subungual hematoma, laceration, or avulsion.
- Nail Plate: Is it intact, lacerated, or avulsed from the fold?
- Tendons: Verify FDP/Extensor function (if injury is proximal to insertion).
- Sensation: Test 2PD before local anaesthetic (Normal: 2-4mm).
- Perfusion: Cap refill, temperature, Allen's test to digits.
- Defect Size: Measure in mm. Critical for treatment planning.
Always document sensation BEFORE injecting lignocaine.
Investigations
Radiology
- Standard: PA and Lateral views.
- Look for:
- Tuft Fracture: Comminuted fracture of distal tip (very common with crush). Usually needs no fixation.
- Shaft Fracture: May need K-wire.
- Avulsion: FDP avulsion (Jersey finger) or Extensor (Mallet).
- Foreign Body: Glass/Metal.
Ultrasound is useful for radiolucent foreign bodies (thorn/wood).
Differential Decision-Making
The "differential" in fingertip trauma is less about disease and more about correctly categorising the injury, because the category dictates the treatment. Misclassification is the commonest source of error.
- Key Discriminator
- X-ray shows comminuted distal tuft
- Pitfall if Missed
- Calling an open tuft # a 'simple cut'
- Action
- Treat as open #: irrigate, repair nail bed
- Key Discriminator
- Plate stable in fold vs avulsed/disrupted
- Pitfall if Missed
- Trephining over a displaced nail bed laceration
- Action
- Stable plate: trephine. Disrupted: remove and repair
- Key Discriminator
- DIP extensor lag vs loss of active DIP flexion
- Pitfall if Missed
- Missing a Zone 1 tendon injury behind a tip wound
- Action
- Examine FDP/extensor before anaesthetic
- Key Discriminator
- Tense, throbbing, fluctuant closed pulp space
- Pitfall if Missed
- Draining a felon too late (osteomyelitis)
- Action
- Incise and drain the septated pulp space
- Key Discriminator
- More nail lost (dorsal) vs more pulp lost (volar)
- Pitfall if Missed
- Planning a V-Y for a volar-oblique defect
- Action
- Volar oblique: cross-finger / homodigital flap
Treatment
Defect Management Algorithm
- No Exposed Bone (Defect less than 1cm):
- Secondary Intention: Dressings. Best sensation. Best padding.
- Exposed Bone:
- Shortening: Simple, effective. Good for labourers.
- Local Flap: If length must be preserved.
- Graft: Poor take over bone (needs periosteum).
- Thumb: Distinct entity. Length is critical. Use Moberg flap.
Preserving thumb length outweighs cosmetic concerns.
Surgical Considerations
The V-Y Advancement Flap (Atasoy)
- Indication: Transverse or Dorsal Oblique amputations.
- Design: V-shaped incision with apex at DIPJ crease.
- Dissection: Cut skin only. Tease fibrous septae deep to flap to mobilize it. DO NOT undercut the base (blood supply).
- Movement: Advance distally over bone.
- Closure: Y-shape closure.
- Limit: Advances about 5-10mm max.
Ensure the "V" apex is at the DIPJ crease to avoid scar contracture across the joint.
Examiners expect more than the three common flaps — know where these named options sit on the fingertip reconstructive ladder:
- Kutler bilateral V-Y flaps: two lateral triangular flaps (one on each side) advanced to the midline for a transverse tip amputation — an alternative to the single volar Atasoy flap, giving less advancement but a midline closure.
- Thenar flap: the injured volar pulp of the index or middle finger is buried into a flap raised from the thenar eminence and divided at about two weeks. Good pulp bulk and colour match, but the risk is a PIP flexion contracture from the flexed inset, so it is reserved for younger patients with supple joints.
- Homodigital (Venkataswami) island flap: an antegrade neurovascular island advanced on one digital artery and nerve of the same finger — sensate, single-stage coverage for a volar-oblique defect without sacrificing an adjacent finger.
- Littler neurovascular island flap: sensate skin transferred on its neurovascular pedicle (classically from the ulnar border of the middle/ring finger) to resurface a critical sensory area, especially the thumb pulp; cortical re-education is needed because sensation is initially referred to the donor digit.
- Reconstructive ladder principle: choose the simplest adequate option first — secondary intention / dressing → local advancement (V-Y, Moberg) → regional (cross-finger, thenar, homodigital island) → distant or free tissue only for the largest composite defects.
Surgical Technique: Innervated Cross-Finger Pulp Flap
Tight Closure over Bone If you pull the nail bed tightly over the tip of a shortened distal phalanx, or if there is insufficient bony support, the nail bed curves volarly. As the nail grows, it curves around the tip like a parrot's beak.
Adequate Bone Support The bone must support the nail bed fully. If the bone is short, trim the nail bed back or advance bone/soft tissue. Do not suture the nail bed under tension over the steep cliff of the amputation.
- Indication
- Transverse / Dorsal Oblique
- Vessel
- Subcutaneous perforators
- Movement
- Advancement
- Indication
- Transverse / Volar Oblique
- Vessel
- Lateral digital
- Movement
- Bilateral Advancement
- Indication
- Thumb Tip
- Vessel
- Neurovascular Bundles
- Movement
- Volar Advancement
- Indication
- Volar Oblique / Large
- Vessel
- Dorsal Digital (Donor)
- Movement
- Transposition
SPDSGoals of Reconstruction
Hook:A fingertip must have SPDS (Speed).
0.1mmNail Growth
Hook:Nails grow 0.1mm per day.
GLUENail Bed Repair
Hook:Don't forget the glue option.
Complications
- Neuroma: Painful nerve ending. Requires resection and burying in muscle/bone.
- Hook Nail: Curvature of nail over tip. Difficult to trim. Catching.
- Split Nail: scar in germinal matrix.
- Non-Adherent Nail: scar in sterile matrix.
- Hypersensitivity: Common. Needs desensitization therapy (tapping, texture rubbing).
- Cold Intolerance: Persistent problem with replants and flaps.
The composite-graft option for a child's tip sits at the distal end of a larger replantation framework examiners test:
- The thumb, at any level (functional priority).
- Multiple digits.
- Any amputation in a child.
- Amputation through the palm, wrist or forearm.
- A clean amputation distal to the FDS insertion (better functional outcome than a single digit amputated within zone 2).
- A single finger amputated proximal to the FDS insertion in an adult (poor functional return, stiffness, the digit often gets in the way).
- Severe crush or avulsion, multi-level injury, or gross contamination.
- Prolonged warm ischaemia, significant comorbidity, or a patient unable/unwilling to comply with rehabilitation.
replantation distal to the lunula is technically possible but limited by the lack of a suitable vein for venous outflow (managed with controlled bleeding / leech protocols). In young children a composite graft is the pragmatic, reliable alternative to microsurgical replant. Because digits carry little muscle, ischaemia tolerance is comparatively long — roughly up to about twelve hours warm and twenty-four hours cold.
Rehabilitation
- Splint: Aluminum tip protector or thermoplastic cap.
- Wound: Keep dry. Occlusive dressing for secondary intention.
- Nail: Keep stent (nail plate or foil) in place.
- Elevation: Reduce swelling.
- Pain: Simple analgesia. Avoid NSAIDs initially (may affect healing).
- Sutures: Remove non-absorbable sutures (if used).
- Nail Stent: Can remove at 3 weeks.
- Desensitization: Start early tapping/rubbing to prevent hypersensitivity.
- ROM: Mobilize DIPJ. Active flexion/extension.
- Edema Control: Coban wrap if needed.
- Grip Exercises: Putty, stress ball.
- Pinch Strength: Key pinch, tripod pinch exercises.
- Scar Massage: Soften and desensitize scar tissue.
- Light Activities: Typing, writing.
- Nail: New nail plate grows in (3-4 months for full replacement).
- Sensation: Returns gradually over 6-12 months.
- Cold Intolerance: May persist, improves with time.
- Return to Work: Manual workers 4-8 weeks; fine motor 8-12 weeks.
Hand Therapy Principles
- Early Motion: Critical to prevent DIPJ stiffness.
- Desensitization Program: Texture grading from soft to rough materials.
- Protective Splinting: Custom tip guard for return to work.
- Work Hardening: Simulate occupational demands.
- Psychological Support: Fingertip injuries can be distressing.
Prognosis
- Sensation: Secondary intention healing gives BETTER sensation (2PD 3-4mm) than grafts or Cross Finger flaps (2PD 6-8mm).
- Aesthetics: Flaps look better initially but secondary intention creates a surprisingly normal fingerprint pattern.
- Nail: Deformity is the most common long-term complaint.
- Pain: Cold intolerance is rare with secondary intention but common with flaps.
Guidelines, Registries & Global Practice
Global Epidemiology
- Burden: The fingertip is the single most commonly injured part of the hand worldwide; distal phalanx/fingertip trauma accounts for a large share of all hand injuries presenting to emergency departments across high- and low-income settings.
- Demographics: Bimodal pattern. A working-age male peak (roughly 20-50 years) driven by machinery, power tools and crush injuries; and a young-child peak (1-4 years) driven by door-crush injuries to the dominant-hand digits.
- Mechanism: Doors are the leading cause in children; industrial machinery, saws and presses dominate occupational injury globally.
- Most-injured digits: Middle and ring fingers (longest, most exposed in grip); the thumb is treated as a distinct priority because of its functional dominance.
Guidelines Compared Side by Side
- BSSH / BOA (UK)
- Not routine after thorough irrigation
- ASSH / AAOS (US)
- Not routine for uncomplicated open distal tuft fracture
- AO / EFORT (Europe)
- Selective; wound toilet emphasised
- BSSH / BOA (UK)
- Decompress if painful; nail removal not mandated by size
- ASSH / AAOS (US)
- Trephination for painful haematoma; repair if plate unstable
- AO / EFORT (Europe)
- Decompress; preserve a stable plate as a biological stent
- BSSH / BOA (UK)
- Conservative / secondary intention favoured
- ASSH / AAOS (US)
- Secondary intention or occlusive dressing
- AO / EFORT (Europe)
- Semiocclusive dressing (Mennen-Wiese tradition)
- BSSH / BOA (UK)
- Local flap or shortening per patient need
- ASSH / AAOS (US)
- Local flap (V-Y, Moberg for thumb), shortening
- AO / EFORT (Europe)
- Reconstructive ladder; homodigital/regional flaps
Registry & Outcome Notes
- Fingertip injuries are not implant procedures, so they do not feature in joint registries (NJR, AJRR, AOANJRR). The evidence base instead rests on RCTs and systematic reviews (antibiotics, glue vs suture, subungual haematoma) and large conservative-management series.
- National hand-trauma networks (e.g. UK BOAST hand-trauma standards, regional trauma datasets) emphasise early senior decision-making and access to hand therapy as the key determinants of outcome.
High- vs Limited-Resource Practice Variation
- High-resource settings: Ready access to operating theatres, microsurgery and dedicated hand therapy enables flap reconstruction, composite grafting in children and formal nail bed repair under loupe magnification.
- Limited-resource settings: Conservative management (secondary intention / semiocclusive dressing) is especially valuable — it is cheap, avoids theatre time, needs no microsurgical skill and reliably restores a sensate, durable pulp for small and moderate defects.
- Universal principles: Tetanus prophylaxis per local immunisation status, meticulous wound toilet, preservation of length (especially the thumb), and early mobilisation to prevent DIPJ stiffness apply everywhere regardless of resource level.
Controversies and Areas of Uncertainty
Traditional teaching mandated nail removal and formal nail bed repair for any subungual haematoma over 50 percent. Systematic review evidence (Dean et al.) shows no cosmetic advantage of repair over simple decompression when the plate is stable. The pragmatic position: decompress the painful nail, reserve formal repair for a clearly avulsed or disrupted plate.
A small area of exposed bone is not an absolute indication for a flap. Many tips granulate and epithelialise over a small exposed tuft with occlusive dressings, yielding excellent sensation. Flaps preserve length faster but add donor morbidity, stiffness and cold intolerance. The decision is patient-specific (occupation, length needs, comorbidity).
Replacing the amputated tip as a composite graft is reliable in young children but unpredictable in adults, where take is poor distal to a few millimetres. There is no firm age cut-off; success falls with age and proximal level of injury.
The RCT evidence against routine antibiotics applies to clean, well-irrigated open distal phalanx fractures in healthy adults. It should not be extrapolated uncritically to grossly contaminated, bite, farmyard or immunocompromised injuries, where prophylaxis remains reasonable.
MCQ Practice Points
Q: Which part of the nail matrix is responsible for nail plate adherence? A: The Sterile Matrix.
Q: What deformity results from scarring of the germinal matrix? A: Split Nail (as the nail plate is not formed uniformly).
Q: The Moberg flap is contraindicated in which digit? A: The Index Finger (and all except Thumb).
Q: What is the maximum size defect that heals well by secondary intention (if no bone exposed)? A: 1 cm (can heal up to 1.5 cm but slower).
Q: How do you prevent a Hook Nail deformity? A: Ensure adequate bony support for the nail bed. Do not suture nail bed under tension over shortened bone.
Q: For a volar oblique fingertip amputation with exposed bone, which flap is most appropriate? A: Cross Finger Flap (Atasoy V-Y advances less volar tissue; Cross Finger provides volar coverage).
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A carpenter hits his thumb with a hammer. There is a large subungual hematoma (90%) and a transverse laceration through the nail plate. X-ray shows a comminuted tuft fracture. How do you manage this?”
“A chef slices off the tip of his index finger. There is a 1cm x 1cm defect with bone exposed. The cut is transverse. He wants to return to work ASAP.”
“A 2-year-old shuts their finger in a door. The tip is amputated through the nail bed, held on by a bridge of skin. It looks dusky. What do you do?”
“A patient presents 6 months after fingertip amputation with a curved, painful nail that catches on clothing. The tip looks like a parrot's beak. What happened and what are the options?”
Classification
- Allen I: Pulp only
- Allen II: Pulp + Nail
- Allen III: Distal Phalanx
- Allen IV: Proximal to Lunula
Management
- No Bone: Secondary Intention
- Bone Exposed: Atasoy (Transverse), Kutler (Lateral)
- Thumb: Moberg
- Large/Volar: Cross Finger
Nail Bed
- Repair: 6-0 Chromic
- Hematoma: Trephine if painful
- Hook Nail: Prevent by bone support
- Stent: Replace nail plate or foil
Evidence Base
Prophylactic Antibiotics for Open Distal Phalanx Fractures
- Double-blind RCT of flucloxacillin vs placebo in 193 adults with open distal phalanx fracture
- Overall infection rate 4 percent; no osteitis or deep infection in either arm
- 3 of 98 infections with antibiotic vs 4 of 95 with placebo (no significant difference)
- Thorough wound toilet and soft-tissue repair is the key intervention, not antibiotics
2-Octylcyanoacrylate vs Suture for Nail Bed Repair (RCT)
- Prospective RCT, 40 patients: Dermabond (n=18) vs 6-0 chromic suture (n=22)
- Repair time 9.5 min with glue vs 27.8 min with suture (p less than 0.0003)
- No difference in cosmesis, pain or function at 1, 3 and 6 months
- Tissue adhesive is a faster, equally effective alternative to suture
Glue vs Suture Nail Bed Repair in Children (1-year follow-up)
- 74 paediatric nail bed lacerations; glue (n=36) vs absorbable suture (n=38)
- Nail dystrophy 14 percent overall (5 percent major), independent of technique
- Glue repair faster (10.2 vs 20.3 min, p less than 0.001)
- Higher early infection when repaired in ED vs operating room
Management of Acute Subungual Haematoma (Systematic Review)
- Systematic review of subungual haematoma management
- No difference in nail cosmesis between formal nail bed repair and simple decompression
- Complication rates low across all treatment methods
- An acutely painful haematoma should simply be decompressed (trephine or nail removal)
Semiocclusive Dressing for Fingertip Defects (Mennen-Wiese)
- Conservative semiocclusive film dressing for fingertip defects, including some with exposed phalanx
- Series of 200 injuries healed within 20-30 days with weekly undisturbed dressing changes
- Restored bulky pulp, fingerprint pattern and near-normal sensibility (2PD 2-8mm in pooled data)
- Avoids donor-site morbidity of local flaps
The Volar Advancement (Moberg) Flap for the Thumb
- Original description of the volar neurovascular advancement flap for the thumb tip
- Feasible because the thumb retains an independent dorsal blood supply, allowing the volar skin to be elevated on both digital bundles
- Contraindicated in the fingers, where elevating volar skin on both bundles risks dorsal skin necrosis