Suture Techniques and Biomechanics
- A 4-strand core suture is the absolute minimum for Early Active Motion.
- The Epitendinous suture adds 10-20% strength and reduces gapping.
- Gapping greater than 3mm leads to poor outcomes (adhesions/rupture).
- Preserve A2 and A4 pulleys to prevent bowstringing.
- Repair should be performed within 7-10 days (before myostatic contracture).
- WALANT (Wide Awake) allows intra-operative testing of glide.
- “Strength is proportional to the number of strands crossing the repair site.
- “Locking loops prevent suture pull-out but can strangle the tendon (ischemia).
- “The placement of the knot (inside or outside) is debated; mostly inside to reduce friction.
Gap greater than 2mm Gap formation at the repair site allows fibrous tissue ingrowth (adhesions) rather than tendon healing. A gap weakens the repair significantly and predisposes to rupture.
Pre-tensioning & Epitendinous Pre-tensioning the core suture ensures faces are opposed. The epitendinous running suture is CRITICAL for resisting gap formation. It smooths the edges and adds strength.
- Modified Kessler
- Locking Rectangular
- Adelaide
- Cross-Locking (4 strand)
- Cruciate
- Cross-Stitch
- Modified Kessler
- 2 (Standard)
- Adelaide
- 4 (Standard)
- Cruciate
- 4 (Standard)
- Modified Kessler
- Moderate
- Adelaide
- High
- Cruciate
- High
- Modified Kessler
- Low
- Adelaide
- Moderate
- Cruciate
- Low
SCENERepair Strength Factors
Hook:Create a SCENE for strong repair.
DAP-CT-FVerdan Zones
Hook:Distal to Proximal mapping.
Overview
Flexor tendon repair aims to restore digital flexion while minimizing adhesion formation. The challenge is balancing Mechanical Strength (to allow early motion) against Gliding Resistance (bulkiness of the repair).
The history of flexor tendon repair has evolved from "primary repair is impossible" (Bunnell's 'No Man's Land') to the current standard of primary repair with robust constructs allowing Early Active Motion (EAM).
Key historical milestones include:
- Bunnell: Advocated tendon grafting in Zone II.
- Kleinert: Introduced immediate controlled active motion with rubber bands.
- Strickland: Defined the biomechanical requirements for EAM (Work of Flexion vs Repair Strength).
Pathophysiology and Mechanisms
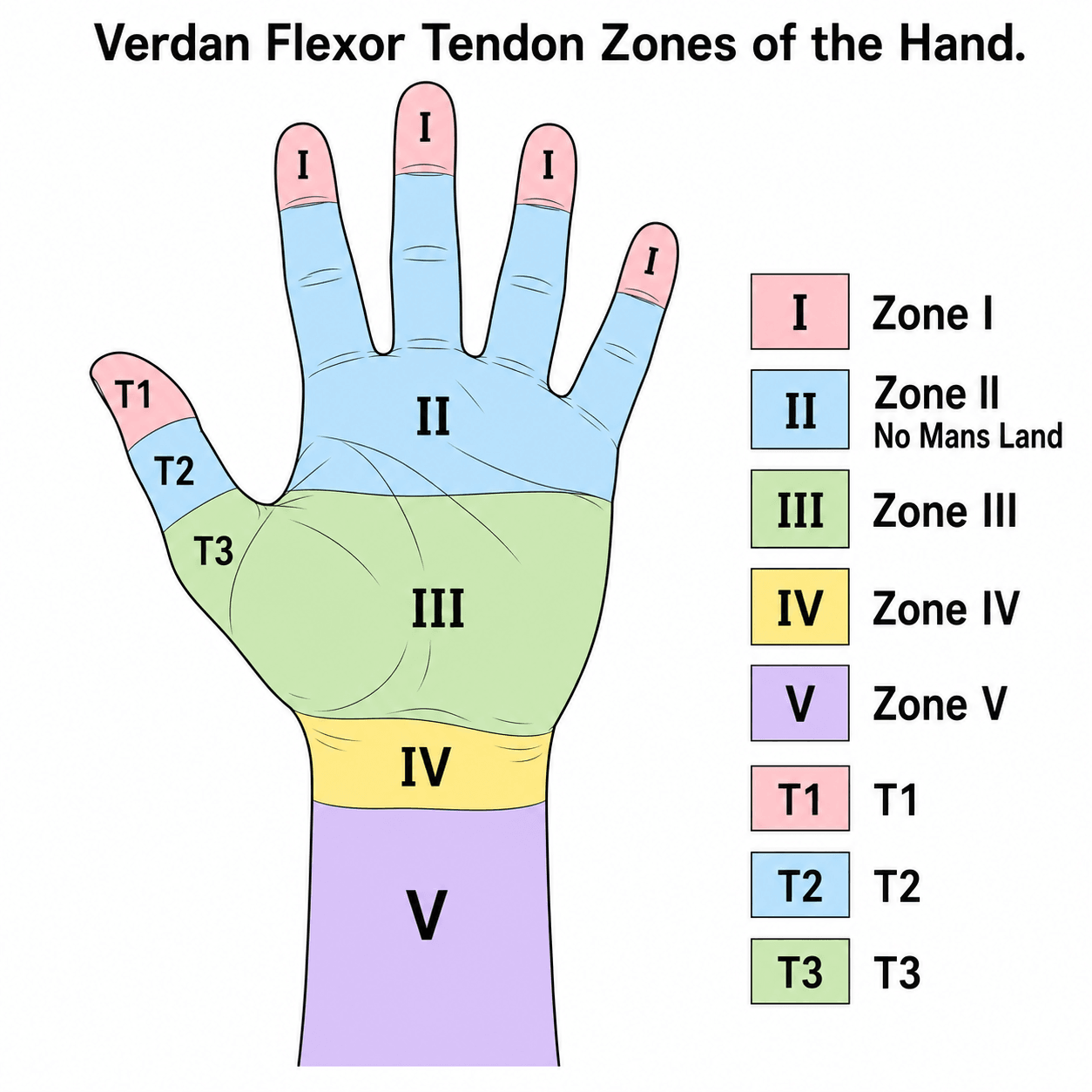
Verdan Zones
- Zone I: FDP only. Distal to FDS insertion. Repair is straightforward (or advancement).
- Zone II: FDS and FDP share the sheath (A1 to FDS insertion). Most complex. Adhesion risk is highest here.
- Zone III: Lumbrical origin. Good prognosis.
- Zone IV: Carpal Tunnel. Crowded.
- Zone V: Forearm. Good prognosis.
The transition from Zone II to Zone III is defined by the distal palmar crease.
Tendon Healing Biology: Intrinsic vs Extrinsic
How a flexor tendon heals determines whether it glides or scars, and is the biological justification for early motion.
- Intrinsic healing: mediated by the tenocytes within the tendon itself, nourished by synovial diffusion and the vincula. It restores tendon continuity without binding the tendon to its surroundings, so glide is preserved. Early controlled motion promotes this pathway.
- Extrinsic healing: fibroblasts invade from the surrounding sheath and soft tissues, laying down scar that bridges the repair but tethers the tendon as adhesions. Immobilisation, rough tissue handling, sheath and pulley damage, and gapping all push healing toward this pathway.
Three overlapping phases:
- Inflammatory (0 to about 5 days): the repair is held almost entirely by the suture and tensile strength is at its lowest - the classic early "soft" period.
- Proliferative / fibroblastic (about 5 days to 3-4 weeks): collagen is laid down and strength climbs, often after an early dip.
- Remodelling (from about 3-4 weeks, continuing for months): collagen aligns along lines of stress and the repair regains functional strength; controlled loading guides this alignment.
Controlled early motion shifts healing toward the intrinsic pathway and remodels collagen along the line of pull, improving glide and final strength - but only if the core repair is strong enough (4-strand minimum) to survive the loads applied during the weak inflammatory phase. This is the biological reason a strong repair and early motion are inseparable.
Classification Systems
Repair Configurations
- Modified Kessler: Rectangular locking. 2 strands per pass.
- Adelaide: 4 strands. Locking. Developed for EAM.
- Cruciate: Cross pattern. 4 strands.
- Tajima: Locking loops for grasping the end.
- Lim/Tsai: 6-strand loops.
The mechanical strength of the repair is linearly related to the number of strands.
FDP Avulsion (Jersey Finger): Leddy-Packer Classification
A closed avulsion of the FDP from the distal phalanx ("jersey finger" - classically the ring finger caught in a jersey) is a distinct Zone I injury graded by how far the tendon retracts and whether a bony fragment is attached - the Leddy-Packer classification, which sets the urgency.
- Retraction / fragment
- Tendon retracts into the palm
- Vincula / blood supply
- Both vincula ruptured (no nutrition)
- Implication
- Surgical emergency - repair within about 7-10 days before the tendon necroses and the muscle contracts
- Retraction / fragment
- Retracts to the PIP joint (most common)
- Vincula / blood supply
- Held by an intact long vinculum (vincula preserved)
- Implication
- More time available, but still repair early; can convert to type I if the vinculum tears
- Retraction / fragment
- Large bony fragment avulsed, caught at the A4 pulley
- Vincula / blood supply
- Vincula usually intact
- Implication
- Fix the fragment (suture or screw); the tendon stays attached to bone
- Retraction / fragment
- Bony fragment PLUS tendon avulsed off the fragment ('double avulsion')
- Vincula / blood supply
- Variable
- Implication
- Two-level problem: fix the fragment AND reattach the tendon
When reattaching an avulsed or lacerated FDP to the distal phalanx (a pull-out suture over a dorsal button, or a bone anchor), the tendon must not be advanced more than about 1 cm. Over-advancing shortens the FDP and, because the profundi share a common muscle belly, produces a quadriga effect (the other fingers cannot fully flex) and a DIP flexion contracture.
Clinical Presentation
A flexor tendon injury classically presents after a sharp laceration to the volar finger, hand or wrist with loss of the normal resting flexion cascade of the affected digit (the injured finger lies more extended than its neighbours).
- FDP division: Loss of active DIPJ flexion.
- FDS division: Loss of active PIPJ flexion (tested with adjacent fingers held in extension).
- Both divided (Zone II): Loss of active flexion at both PIPJ and DIPJ.
- FPL division: Loss of active thumb IP flexion.
- Partial laceration: Active flexion may be preserved but painful, with weakness, triggering or catching - a high-risk trap for missed injury.
- Associated injuries: Digital nerve injury (altered sensation on the side of the laceration) and digital artery injury are frequently concomitant because they lie adjacent to the tendon.
The resting cascade and individual FDS/FDP testing are the cornerstone of bedside diagnosis; imaging is rarely needed acutely.
History
History Taking
- Mechanism: Sharp (knife, glass) vs Crush (machinery).
- Time: Hours since injury. Ideal repair within 24-72 hours.
- Contamination: Animal bite, soil, marine environment.
- Occupation: Manual worker, musician, typist.
- Hand Dominance: Right or left handed.
- Smoking: Major risk factor for complications.
- Diabetes: Impaired healing.
- Previous Hand Surgery: Scarring, previous tendon injury.
Sharp, clean lacerations have best prognosis.
Examination
Pre-operative Examination
- FDS Test: Hold other fingers in extension. Ask patient to flex PIPJ.
- FDP Test: Hold PIPJ in extension. Ask patient to flex DIPJ.
- Index Quirk: Some patients have independent FDP to index (absent FDS).
- Neuro: Digital nerves are lateral to tendons and often cut concomitantly.
- Perfusion: Digital arteries. Check cap refill, Allen's test.
- Wound: Assess depth, contamination, tissue loss.
Ensure you test FDS function for each digit individually.
Investigations
Ultrasound
- Can locate retracted tendon ends.
- Confirm diagnosis in partial tears.
- X-Ray: Rule out avulsion fracture (Jersey finger) or foreign body.
MRI is rarely needed for acute lacerations but useful for chronic ruptures. It can visualize:
- Tendon stump location (retraction).
- Integrity of the pulley system.
- Presence of scar tissue/adhesions.
This helps in planning tenolysis or staged reconstruction.

Differential: Why Is the Finger Not Flexing?
A common exam and clinic problem is the digit that will not actively flex. The differential turns on the passive versus active discrepancy, timing, and the integrity of the repair.
- Active ROM
- Absent
- Passive ROM
- Full
- Timing / Clue
- Often a sudden 'pop'; resting cascade lost
- Action
- Explore early; re-repair if possible, else graft/reconstruct
- Active ROM
- Reduced
- Passive ROM
- Full
- Timing / Clue
- Gradual; weeks 6-12; passive much greater than active
- Action
- Therapy first, then tenolysis once tissues mature
- Active ROM
- Reduced
- Passive ROM
- Reduced
- Timing / Clue
- Loss of passive extension; capsular
- Action
- Aggressive splinting; capsulotomy if fixed
- Active ROM
- Absent or weak
- Passive ROM
- Full
- Timing / Clue
- Initial assessment; FDS vs FDP test
- Action
- Re-examine and explore
- Active ROM
- Limited fist (all fingers)
- Passive ROM
- Full
- Timing / Clue
- Over-tightened/advanced FDP; adjacent fingers short
- Action
- Release/lengthen the tethering tendon
- Active ROM
- Curls, incomplete flexion
- Passive ROM
- Full
- Timing / Clue
- Lost A2/A4; tendon lifts off bone
- Action
- Pulley reconstruction
Treatment

Primary Repair
- Gold Standard: Repair within 24-72 hours ideally.
- Limit: Up to 10-14 days. After this, pulleys collapse and muscle contracts.
- Delayed: If greater than 3 weeks, may need 2-stage reconstruction (Hunter Rod).
Immediate repair is always technically easier than delayed repair.
Surgical Considerations
Exposure (Bruner)
- Incisions: Zig-zag (Bruner) incisions prevent scar contracture.
- Flaps: Full thickness flaps raised.
- Sheath: Window the sheath between pulleys (e.g. C1 window) to access the tendon. Do not vertically slice A2/A4 if possible.
Good exposure is key. Extend incisions proximally and distally.
Antibiotic Protocol
Prophylaxis:
- Cefazolin (Kefzol) 2g IV at induction.
- Post-op oral antibiotics (Cephalexin) often given for 5 days due to length of procedure and implant material, though evidence is debated.
- Contaminated Wounds: Augmentin.
Complications
- Adhesions: Most common complication. Loss of active flexion despite good passive ROM. Needs Tenolysis.
- Rupture: Catastrophic failure. Occurs if rehab is too aggressive or repair is weak (less than 4 strands).
- Bowstringing: Loss of A2/A4 pulleys results in an increased moment arm but loss of excursion (finger curls but doesn't fully flex).
- Contracture: PIPJ flexion contracture is common if not splinted in extension.
- Quadriga Effect: Overtightening FDP in one finger tethers the others (common muscle belly). The patient cannot make a full fist because the repaired finger hits the palm first.
- Infection: Deep space infection is disastrous for tendon gliding.
Rehabilitation
- Splint: Dorsal Blocking Splint (Wrist 30° flex, MCP 70° flex, IP extended).
- Passive Flexion: Duran protocol - passive flexion exercises within splint.
- Active Extension: Controlled active extension to splint limits.
- Synergistic Motion: Wrist extension with finger flexion (Tenodesis effect).
- Early Active: Gentle active flexion to 1/3 fist if 4-strand repair (Manchester/Stark).
- Edema Control: Coban wrap, elevation, retrograde massage.
- Wrist Neutral: Progress wrist position to neutral.
- Place and Hold: Active extension, passive flexion, then hold.
- Tendon Gliding: Hook, Straight, Fist, Table-top positions.
- Differential Glide: Isolated FDS vs FDP exercises.
- Scar Management: Silicone gel sheets, massage.
- Splint Wean: Day use only, night splint continues.
- Full Active Motion: Unrestricted active ROM exercises.
- Blocking Exercises: Isolated joint motion (DIP blocking for FDP).
- Light Functional Use: ADLs with precautions.
- Splint Discontinue: Week 8.
- Progressive Resistance: Putty, hand exercisers.
- Work Hardening: Task-specific conditioning.
- Return to Work: Light duties Week 8, full duties Week 12.
- Sport: Full contact sports at Week 12.
GLIDERehabilitation Goals
Hook:The goal is GLIDE.
Prognosis
- Zone I/III/V: Excellent results.
- Zone II: "Fair" to "Good". Stiffness and adhesions remain a challenge. 10-15% rupture rate depending on compliance.
- Tenolysis: Required in 15-20% of Zone II repairs.
- Children: Excellent healing potential but poor compliance with rehab creates high risk of rupture or adhesion. Cast immobilization is often used.
- Smokers: Higher rates of complications (infection, poor healing).
Guidelines, Registries & Global Practice
Global Epidemiology
- Demographics: Peak incidence in working-age males (20-40 years) worldwide; hand lacerations are among the most common reasons for emergency hand referral.
- Mechanism: Sharp lacerations (glass, knives, sheet metal) dominate in high-income settings; agricultural and machinery injuries are proportionally higher in rural and lower-resource regions.
- Occupational burden: Construction, manufacturing, food/meat processing and fishing industries carry the highest occupational rates.
- Zone II predominance: Zone II remains the most frequently injured and the most outcome-determining zone across all populations.
Injury patterns shift with economy and occupation, but the surgical principles are universal.
Controversies & Areas of Uncertainty
- 4-strand vs 6-strand: Six-strand repairs are stronger biomechanically, but added bulk increases gliding resistance and work of flexion. Most surgeons accept a robust 4-strand repair as the pragmatic standard; the incremental clinical benefit of 6 strands is unproven.
- Knot placement (inside vs outside): Internal knots reduce surface friction but may bulk the juncture; external knots are simpler but can catch. Evidence does not strongly favour one.
- Pulley venting limits: How much A2/A4 can be vented before bowstringing matters clinically is debated; small partial venting is widely accepted but the safe upper limit is not precisely defined.
- Optimal rehabilitation protocol: Early active motion improves motion (Level I) but demands a strong repair and skilled therapy; where therapy is unavailable the trade-off against rupture risk remains contested.
- Slightly bulky repair philosophy: The Tang/Lalonde approach tolerates a slightly bulky repair plus venting to favour strength; traditionalists prioritise a slim, low-resistance juncture. Both have advocates.
- FDS repair in Zone II: Whether to repair one or both FDS slips (or excise FDS) when the sheath is tight is individualised, not standardised.
MCQ Practice Points
Q: How much strength does a standard epitendinous suture add to a repair? A: 10-20%.
Q: Which nutrient pathway is most important in Zone II? A: Synovial diffusion (Imbibition).
Q: What is the Quadriga Effect? A: Limitation of flexion in adjacent fingers due to overtightening/shortening of the FDP in the repaired finger (shared muscle belly).
Q: What is the minimum strand count for Early Active Motion? A: 4 Strands.
Q: Why is Zone II called 'No Man's Land'? A: FDP and FDS travel within a tight fibro-osseous tunnel, making repair technically challenging and historically associated with poor outcomes due to adhesion formation.
Q: Which pulleys are critical and must be preserved during flexor tendon surgery? A: A2 and A4 - They prevent bowstringing. A1, A3, and A5 can be released if needed for exposure.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old carpenter presents with a laceration over Zone II of the index finger. FDS and FDP are non-functional. He wants a quick return to work. Discussion?”
“6 weeks post-op Zone II repair, a patient feels a 'pop' lifting a coffee cup. Finger is extended, no active flexion. What now?”
“4 months post-op. Full passive flexion, but no active flexion. What is the diagnosis and management?”
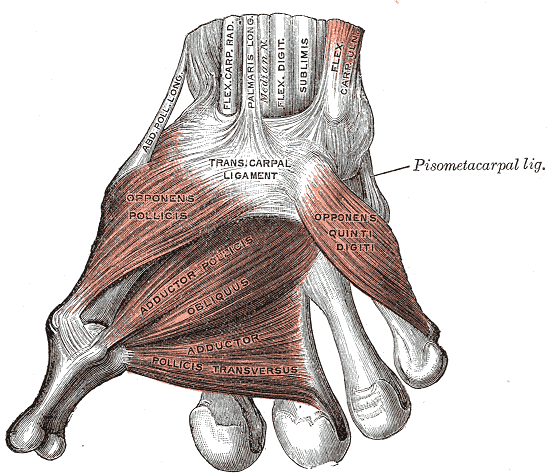
“A 35-year-old presents with a glass laceration at the thenar crease. FPL is non-functional. Describe the anatomy and management.”
Technique
- 4-Strand Core (Min)
- Epitendinous Running
- Vent Pulleys if tight
- Preserve A2/A4
Rehab
- Dorsal Block Splint
- Early Active Motion
- Passive Flexion (Duran)
- Place and Hold
Complications
- Rupture (Worst)
- Adhesion (Common)
- Bowstringing (Pulley loss)
- Quadriga (Length mismatch)
Evidence Base
Scientific Basis for Modern Flexor Tendon Surgery
- Synthesis of 40 years of basic-science research on tendon structure, biomechanics, healing and suture methods
- Articulates the attributes of an ideal repair: easily placed sutures, secure knots, smooth juncture, minimal gapping, preserved vascularity and adequate strength throughout healing
- Repair strength scales with the number of core suture strands crossing the juncture
- Early controlled motion increases gliding and tensile strength of the healing repair
Cruciate Four-Strand Repair
- Cadaveric biomechanical study of 40 FDP tendons (modified Kessler, Strickland, modified 4-strand Savage, Cruciate)
- Cruciate repair was nearly twice as strong to 2mm gap formation (44 N) as the Kessler, Strickland and Savage repairs
- Ultimate tensile strength was significantly higher for the Cruciate (56 N)
- Performed with the speed of a 2-strand technique while exceeding the strength of existing 4-strand repairs
Comparative 4-Strand Zone II Repairs
- In-situ testing of six 4-strand repairs in 54 cadaver profundus tendons at Zone II
- Locked cruciate, modified double Tsuge and modified Becker were strong enough for an early active motion protocol
- Mean gaps after 1000 load-unload cycles did not approach the 3mm clinical limit in any group
- Locked cruciate and modified double Tsuge were easier to perform with less gliding interference than the modified Becker
Active vs Passive Motion After Zone II Repair (RCT)
- Randomised prospective trial: 103 patients (119 digits) with Zone II repairs, active place-and-hold vs passive motion
- Active group achieved greater IP joint motion at final follow-up (156 degrees vs 128 degrees, p less than 0.05) with smaller flexion contractures and higher satisfaction
- Rupture occurred in only 2 digits per group - active motion did not increase rupture risk
- Smoking, concomitant nerve injury and multiple-digit injury all worsened outcomes; certified hand-therapist supervision improved them
WALANT and Wide-Awake Flexor Tendon Repair
- Wide Awake Local Anaesthesia No Tourniquet (WALANT) allows intra-operative active flexion to test the repair before closure
- Strong sutures, a slightly bulky repair, intra-operative active testing and judicious venting of the A2 and A4 pulleys improve flexor tendon results
- Intra-operative testing detects gapping or triggering so it can be corrected before skin closure
- Reduces cost and improves accessibility, particularly in resource-limited settings
Ex-Vivo Comparison of 4-Strand Core Techniques
- Biomechanical comparison of double-modified Kessler, augmented Becker, Savage and modified Tang 4-strand repairs in 56 tendons (all with a 5-0 epitendinous running suture)
- All peripheral (epitendinous) sutures ruptured near the yield point, confirming their load-sharing contribution
- Augmented Becker had the greatest ultimate strength (98.7 N); the double-modified Kessler was weakest against 2mm gapping
- Modified Tang was fastest to perform; technique choice trades operative time against gap resistance
General Principles of Flexor Tendon Repair
- Contemporary review confirming Strickland's 1995 attributes of the ideal repair still hold
- A stout multi-strand repair with a smooth juncture and minimal gapping is sufficient for early mobilisation and intrinsic healing
- Reaffirms preservation of tendon vascularity and a secure, low-friction knot
- Modern repair philosophy favours strong constructs that permit immediate controlled active motion
AO Foundation / AO Surgery Reference - Flexor Tendon Repair
- Recommends a multi-strand (minimum 4-strand) core suture with a circumferential epitendinous suture for Zone I-II injuries
- Advocates atraumatic tendon handling, preservation of critical pulleys and judicious venting to allow glide
- Supports early controlled mobilisation under hand-therapy supervision
- Consensus surgical-technique resource used internationally for training and exam preparation