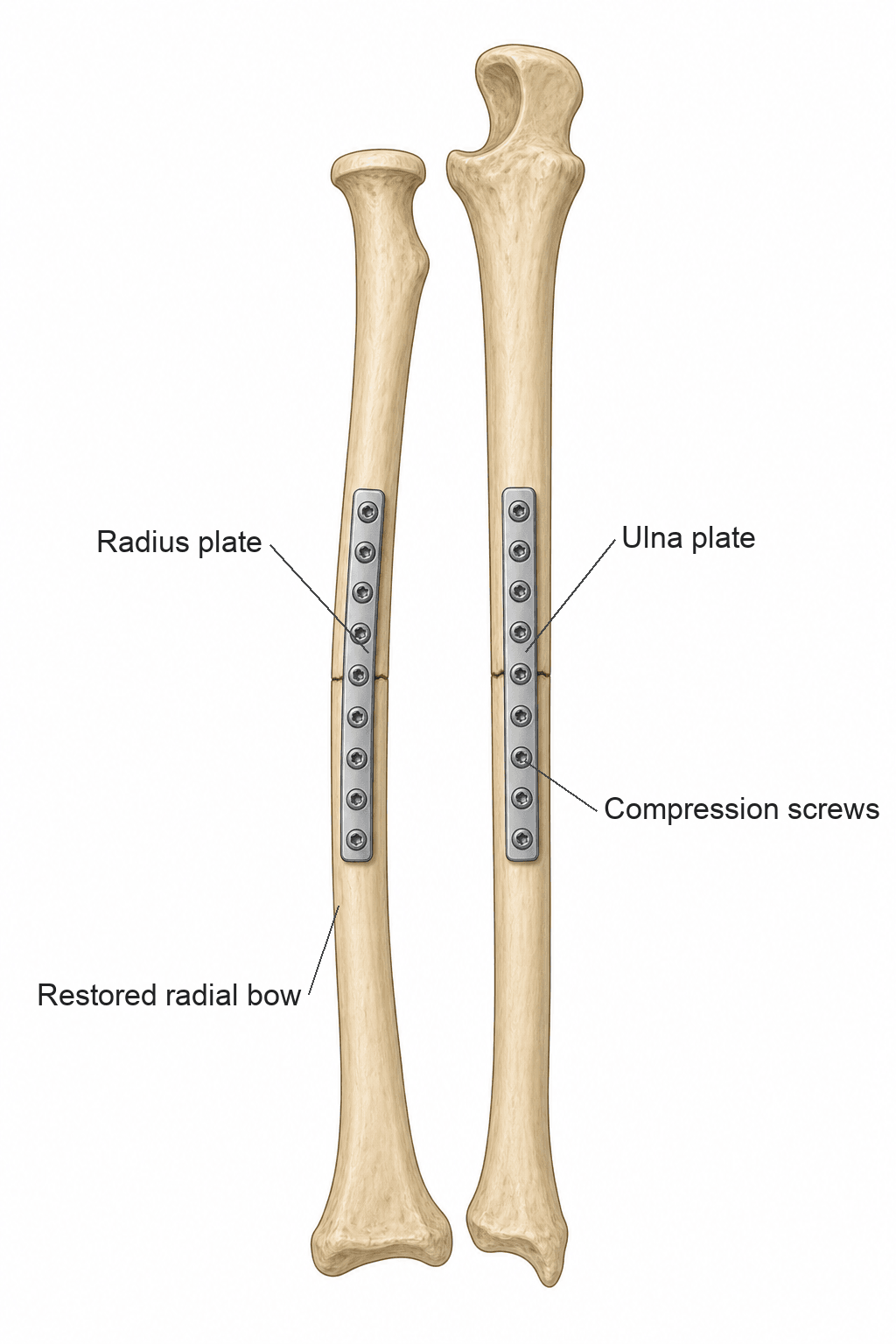
Diaphyseal Radius and Ulna Fractures - The 'Forearm Joint'. ORIF with 3.5mm compression plates remains the gold standard treatment for displaced adult injuries.
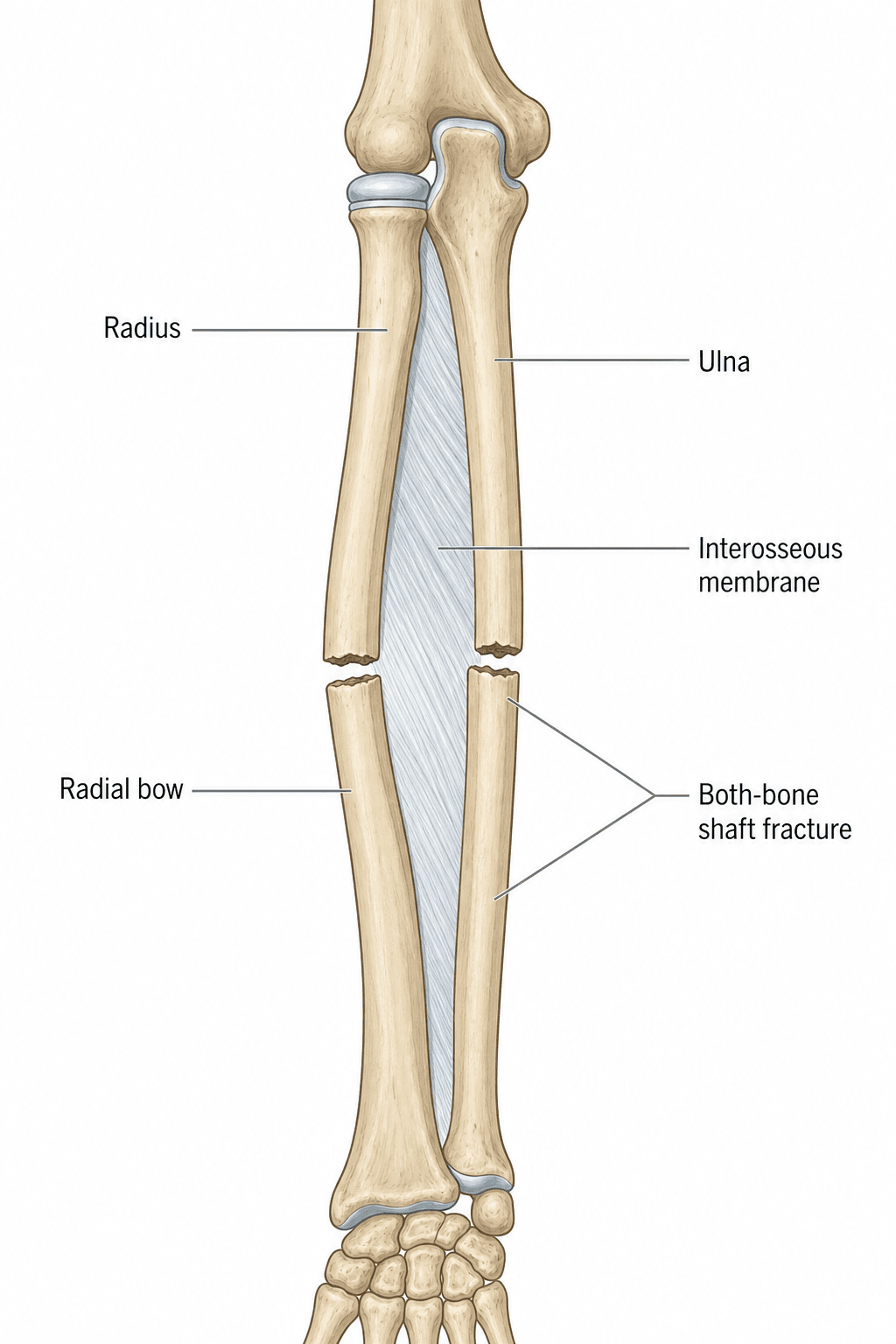
- Restoration of the radial bow is critical for rotation; loss of bow creates a mechanical block.
- The 6-cortex rule (minimum 3 screws per fragment) is the mechanical requirement for stable fixation.
- Always exclude Monteggia (ulna + radial head) and Galeazzi (radius + DRUJ) injuries by imaging elbow/wrist.
- Volar compartments are at highest risk for compartment syndrome; check pain on passive stretch.
- “The PIN is at highest risk in proximal Henry approaches; protect by fully supinating the forearm.
- “Synostosis risk increases from 2% to 11% if a single incision is used for both bones.
- “Isolated ulnar fractures ('Nightstick') with under 50% displacement and under 10° angulation can be treated in a brace.
Forearm Shaft Fracture (Adult)
Functionally, the forearm is a single articular unit. The radius rotates around the fixed ulna. Anatomic reduction is mandatory in adults to restore pronation/supination.
Restoring the lateral radial bow is critical. A straight radius blocks rotation. Fixation requires 3.5mm compression plates manually contoured to the bow.
For definitive fixation, a minimum of 6 cortices (3 screws) on each side of the fracture is required to prevent instability and nonunion.
Overview and Epidemiology
Adult forearm shaft fractures are significant injuries because the forearm behaves as a functional joint allowing an average rotation of 180°. Unlike many other long bone fractures, non-operative management of displaced adult forearm fractures leads to poor functional outcomes, loss of rotation, and high nonunion rates.
- Incidence: Approximately 1-2% of all adult fractures.
- Demographics: Bimodal distribution. Young males (15-30) related to high-velocity trauma; older females (greater than 65) related to low-energy osteoporotic falls.
- Location: Most commonly involve both bones (60%); isolated ulna (25%) and isolated radius (15%) are less frequent.
- High-Energy: MVA, motorcycle accidents, falls from height. Leads to comminution and significant soft tissue compromise.
- Low-Energy: Ground-level falls in the elderly.
- Direct Blow: The "Nightstick" fracture occurs when an individual raises their arm to protect against a strike (classic defensive injury).
A frequent viva framing is "why ORIF the adult but not the child?" - the contrast is examinable and explains the whole adult anatomic-reduction imperative:
- Remodelling potential: the child has open physes and powerful remodelling, so considerable angulation (and even some malrotation in the very young) corrects with growth; the adult has none, so any malreduction is permanent and directly costs pronation/supination.
- Fracture patterns: children sustain plastic (bowing) deformation, greenstick and buckle (torus) patterns that adults do not - these are often managed by closed reduction and casting, with the caveat that a plastic deformation must be corrected (it blocks rotation and will not remodel like an angulated fracture).
- Acceptable thresholds: children tolerate age-dependent angulation (more in the young, with remodelling); the adult threshold is essentially anatomic for displaced both-bone/radius fractures.
- Implant choice: the paediatric workhorse for fractures needing fixation is flexible (elastic/titanium) intramedullary nailing, whereas the adult standard is open compression plating to restore the radial bow and rotation precisely.
Exam point: the adult forearm is plated to anatomy because it cannot remodel and behaves as a rotation-critical joint; the child's remodelling, distinct fracture patterns (plastic/greenstick/buckle) and flexible-nail option allow far more closed/conservative management - except a plastic deformation, which must be corrected.
Anatomy/Biomechanics
The forearm consists of the radius and ulna, which are connected by the Interosseous Membrane (IOM). Functionally, it is a ring structure; a fracture with displacement in one bone almost always implies a second fracture or a dislocation of either the proximal (PRUJ) or distal (DRUJ) radioulnar joint.
- Structure: Complex ligamentous structure with 5 parts.
- Central Band: The strongest portion, providing 70% of the longitudinal stiffness.
- Function: Transfers load from the radius to the ulna and maintains the relationship between the two bones during rotation.
- The radius is not straight but has a lateral convex curvature; the apex lies at the junction of the proximal and middle thirds (pronator teres insertion).
- Axis of rotation: A line from the centre of the radial head proximally to the ulnar fovea distally; the radius rotates around the fixed ulna while the IOM maintains tension throughout the arc.
- Clinical Significance: Loss of the bow (straightening the radius) produces a mechanical block to rotation and significant loss of supination/pronation. Schemitsch and Richards (1992) showed that restoration of the magnitude and location of the radial bow to within approximately 5% of the contralateral limb correlates directly with the recovered rotational arc and grip strength.
- Supinators: Biceps brachii (proximal insertion on radial tuberosity) and Supinator muscle (proximal).
- Pronators: Pronator teres (middle) and Pronator quadratus (distal).
- Fracture proximal to PT insertion: Proximal fragment is supinated; distal fragment is pronated.
- Fracture distal to PT insertion: Proximal fragment stays neutral (counterbalanced); distal fragment remains pronated by PQ.
Pathophysiology of Bone Healing
Fracture healing in the forearm requires a delicate balance between mechanical stability and molecular signaling. In the context of ORIF with compression plating, the goal is absolute stability, leading to primary (direct) bone healing.
- Immediate release of pro-inflammatory cytokines:
TNF-alpha,IL-1beta,IL-6, andIL-10. - Activation of the MAPK (Mitogen-Activated Protein Kinase) and NF-kappaB pathways in osteoblast precursors.
- Recruitment of mesenchymal stem cells (MSCs) via
SDF-1andCXCR4gradients.
- Occurs when fracture gaps are under 0.1mm and strain is under 2%.
- No external callus is formed.
- Cutting Cones: Osteoclasts (formed via
RANKL/OPGsignaling) tunnel across the fracture site, followed by osteoblasts depositing new lamellar bone. - Key growth factors:
BMP-2,BMP-4,BMP-7, andTGF-beta1.
- Occurs if bridging or IM nailing is used.
- Inflammation: Hematoma formation and fibrin clot.
- Soft Callus: Chondrocytes produce Type II collagen; regulated by
Sox9. - Hard Callus: Endochondral ossification; Type X collagen and
VEGFfor angiogenesis. - Remodeling: Conversion of woven bone to lamellar bone over months/years.
Classification Systems
AO/OTA Region 22 (Forearm):
- 22A: Simple Fracture
- 22A1: Simple ulna, radius intact
- 22A2: Simple radius, ulna intact
- 22A3: Simple both bones
- 22B: Wedge Fracture
- 22B1: Wedge ulna, radius intact
- 22B2: Wedge radius, ulna intact
- 22B3: Wedge both bones
- 22C: Complex Fracture
- 22C1: Complex ulna, radius intact
- 22C2: Complex radius, ulna intact
- 22C3: Complex both bones
The AO system provides a standardized language for describing fracture morphology and complexity.
Clinical Assessment
A thorough clinical assessment is mandatory to exclude limb-threatening complications, particularly compartment syndrome.
- Obvious deformity, swelling, and localized tenderness.
- Patient often supports the injured limb in a neutral position.
- Significant pain with any attempt at passive or active rotation.
- Skin Integrity: High incidence of open fractures in the forearm (ulna is subcutaneous). Check for small "poke-through" wounds.
- Neurovascular Status:
- AIN (Median N): Check "OK sign" (FPL/FDP index).
- PIN (Radial N): Check finger extension at MP joints (EIP/EDC).
- Ulnar N: Check interossei strength and sensation in the 5th digit.
- Joint Stability: Always palpate the elbow (PRUJ) and the wrist (DRUJ). Tenderness at these joints suggests a Galeazzi or Monteggia pattern.
- Compartment Check: Palpate for tenseness. The most sensitive sign is pain on passive stretch of the fingers (extension for volar compartment).
Investigations
- Views: AP and Lateral of the entire forearm.
- Requirement: Must include the elbow AND the wrist joints on the same film or separate orthogonal views of the joints.
- Check for "Parallelism": On a true lateral, the radius and ulna should appear parallel. Crossing or overlap suggests malrotation or dislocation.
- Monteggia: The radiocapitellar line must intersect the center of the capitellum in all views.
- Galeazzi: Look for signs of DRUJ instability:
- Ulnar styloid fracture at its base.
- Widening of the DRUJ on AP view (greater than 2mm).
- Dorsal/Volar displacement of the ulna relative to the radius on the lateral view.
- Radial shortening greater than 5mm relative to the distal ulna.
- Rarely indicated for simple shaft fractures.
- Useful for complex intra-articular extension (elbow/wrist) or planning for nonunion surgery.
- Reserved for suspected IOM injury (Essex-Lopresti suspected) or assessing occult tendon/joint injury.
Management Algorithm
+-----------------------------------------------------------+
| Adult Forearm Shaft Fracture Assessment |
| (Clinical Exam + AP/Lat Elbow & Wrist) |
+-----------------------------------------------------------+
|
+-------------+-------------+
| |
[Isolated Ulna Shaft] [Radius or Both Bones]
| |
+-------+-------+ +-------+-------+
| | | |
[Stable/Simple] [Unstable] [ORIF GOLD STANDARD]
(under 50% disp, (greater than (3.5mm Comp Plates)
under 10° ang) 50% disp) |
| | +-------+-------+
[FUNCTIONAL [ORIF 3.5mm] | |
BRACE] | [Henry Volar] [Thompson/Ulna]
| | (Radius) (Radius/Ulna)
[Weekly X-ray] [6-Cortex] | |
(x 3 weeks) [Rule] [PIN Safety] [Internervous]
| | [Supination] [Planes]
+-------+-------+ | |
| +-------+-------+
| |
+-------------+-------------+
|
[Post-operative Protocol]
[0-2w: Splint + Elevation]
[2-6w: Early AROM No-Load]
[6-12w: Advancing Load ]
[12w+: Return to Activity]
In closed injuries without compartment syndrome, surgery can be delayed until soft tissues are favorable. However, open fractures require urgent debridement and stabilization. In both-bone fractures, if one bone is simple and one is complex, fix the simple fracture first to restore length, then fix the complex one.
Surgical Technique
- Proximal/Middle Third: Henry Approach (volar). Internervous plane between Brachioradialis (Radial N) and PT/FCR (Median N). Caution: PIN as it wraps around the radius in the supinator.
- Distal Third: Henry Approach is standard.
- Dorsal (Thompson) Approach: Internervous plane between ECRB (Radial N) and ED (PIN). Best for proximal/middle third radial neck or dorsal pathology.
- Subcutaneous Approach: Direct incision over the subcutaneous border of the ulna. Internervous plane between FCU (Ulnar N) and ECU (PIN).
When performing a proximal Henry approach, the PIN is at risk. It should be protected by supinating the forearm during dissection; this moves the PIN laterally away from the radial neck and protects it within the supinator muscle fibers.
The 10-Step Forearm ORIF
- Positioning: Supine on a hand table with a tourniquet.
- Approach: Standard Henry or Thompson (Radius) and Subcutaneous (Ulna).
- Reduction: Direct reduction with pointed reduction forceps. Restore radial bow apex.
- Provisional Fixation: K-wires or forceps.
- Plate Selection: 3.5mm LCDCP or LCP (contoured).
- Lag Screwing: If oblique/spiral pattern exists.
- Compression: Apply across the transverse component.
- Screw Placement: Achieve 6 cortices minimum per fragment.
- Irrigation/Closure: Hemostasis, layered closure.
- Assessment: Confirm full pronation/supination arc under GA.
Plating is the default, but the candidate should know when an IM nail is genuinely considered in the adult forearm and why it is not the routine choice:
- Why not routine: older/non-interlocked nails do not control rotation or restore the radial bow reliably, so they historically gave higher malunion/nonunion and worse rotation than plates - hence plating is standard.
- Genuine indications: segmental fractures (a nail spans multiple levels with one device), poor soft-tissue envelope (burns, degloving, multiple prior incisions) where extensile plate exposure is hazardous, selected open fractures, the polytrauma/damage-control patient needing rapid closed stabilisation, and cosmesis (small incisions) in selected patients.
- The modern caveat: contemporary rigid, anatomically-bowed, interlocked forearm nails are designed to reproduce the radial bow and control rotation, narrowing the gap with plating in selected fractures - but they still require the same goals (length, bow, rotation) and exclusion of DRUJ/PRUJ injury.
- Always: whichever device, restore the radial bow and length, confirm a full rotational arc on the table, and address any associated Monteggia/Galeazzi joint injury.
Exam point: reserve IM nailing for segmental fractures, compromised soft tissues, selected open/polytrauma cases or cosmesis; modern bowed interlocked nails improve rotational control, but plating remains the standard because the bow and rotation must be restored exactly.
Complications
- Incidence: 1-10% (highest in high-energy or crush injuries).
- Three compartments at risk: Volar (FPL/FDP - most commonly affected), Dorsal (extensors), and the Mobile Wad (BR, ECRL, ECRB - often overlooked).
- Earliest sign: pain out of proportion, then pain on passive finger extension (stretches the volar flexors); the median nerve is affected first.
- Management: Emergency dual-incision (volar + dorsal) fasciotomy releasing all three compartments.
- PIN Palsy: Most common with proximal radius surgery; the dorsal (Thompson) approach carries a documented postoperative PIN palsy rate of approximately 18% even when the nerve is identified and protected (Perretta and Tejwani, 2016). Usually a transient neurapraxia.
- Median/Ulnar Nerve: Higher risk in distal third fractures or penetrating trauma.
- Across pooled compression-plating series, postoperative nerve injury is the single most common adverse event (approximately 7%; Vasara et al., 2024).
- Risk: under 2-3% in closed fractures; significantly higher in Gustilo III open fractures (deep infection approximately 2-4% even with immediate fixation of open injuries; Moed et al., 1986).
- Management: I&D, retention of hardware if stable, suppressive antibiotics.
Postoperative Care and Rehabilitation
- Splint or heavy dressing in neutral rotation.
- Elevation and finger ROM to minimize edema.
- Neurovascular checks in postoperative clinic.
- Suture removal.
- Active and active-assisted ROM (flexion/extension/pronation/supination).
- Lifting restricted to "cup of tea" weight.
- Progressive resistance once early bridging callus is visible.
- Weight-bearing status progressed based on radiology.
Outcomes and Prognosis
Adult forearm ORIF consistently achieves high union and good function.
- Union Rate: Over 95% with modern 3.5mm compression plating in closed injuries.
- Range of Motion: Most patients recover a functional rotational arc when the radial bow and length are anatomically restored; a good result (over 80% of normal rotation) tracks with restoration of the bow (Schemitsch & Richards, 1992).
- Patient Scores: Pooled DASH scores average around 12.5, i.e. good function with a minor residual disability in some patients (Vasara et al., 2024). Subjective weakness can persist despite an objectively good arc.
Guidelines, Registries & Global Practice
Adult forearm shaft fractures are managed with broadly convergent principles worldwide, with the main variation driven by resource setting and the timing/logistics of definitive care.
Global epidemiology
- Diaphyseal forearm fractures represent roughly 1-2% of adult fractures, with a bimodal pattern: high-energy injuries in young men (road traffic and sport) and low-energy osteoporotic injuries in older women.
- High-energy and open patterns predominate where road-traffic and occupational trauma are common; fragility-type injuries dominate in ageing populations.
Side-by-side society guidance
- AO Foundation: Anatomic reduction, restoration of the radial bow, and absolute stability with 3.5mm compression plates (minimum 3 screws / 6 cortices per main fragment) for displaced injuries.
- AAOS / general trauma consensus (US): ORIF is standard for displaced both-bone and displaced isolated radius fractures; selected isolated ulnar (nightstick) fractures with under 50% displacement and under 10° angulation are braced.
- BOA / BOAST (UK) open-fracture principles: Prompt IV antibiotics, early senior-led debridement, and combined ortho-plastic management with early definitive skeletal fixation and soft-tissue cover for open injuries (the ulna is subcutaneous and frequently open).
- EFORT / European practice: Similar plate-osteosynthesis emphasis; intramedullary nailing is reserved for selected segmental or open injuries with poor soft tissues rather than as a default in adults.
Registry and outcome signals
- There is no dedicated arthroplasty-style registry for forearm shaft fractures; the best pooled outcome data come from systematic review (Vasara et al., 2024): 944 adults, 24% adverse-event rate, nerve injury approximately 7% and nonunion approximately 5%, mean DASH 12.5.
High- vs limited-resource variation
- In well-resourced systems, displaced fractures undergo early ORIF, often within 24-72 hours once soft tissues allow.
- In limited-resource or remote settings, initial management is a well-padded above-elbow backslab in neutral rotation with the elbow at 90°, then transfer for definitive plating; the "image both joints" rule (elbow and wrist) is critical at first contact to avoid missing a Galeazzi or Monteggia pattern.
- Functional outcome scores (e.g. DASH) are used internationally to track recovery and guide return to manual work.
MCQ Practice Points
Q: Why is ORIF the standard treatment for adult forearm shaft fractures?
A: The forearm functions as a ring structure requiring anatomic restoration for pronation/supination (180° arc). Non-anatomic reduction causes loss of rotation and radioulnar synostosis. Radial bow must be restored - maximum bow at junction of proximal and middle thirds. Cast treatment acceptable only for isolated ulna fractures with minimal displacement.
Q: What is the optimal plate position for forearm fractures?
A: Radius: Volar (Henry) approach - plate on volar surface (tension side); Thompson approach - plate on dorsal surface. Ulna: Plate on dorsal or medial surface (tension side), avoiding subcutaneous border. 3.5mm LC-DCP or locking plates. Minimum 6 cortices (3 screws) each side of fracture. Compression plating preferred.
Q: What is a nightstick fracture and its treatment?
A: Isolated ulna shaft fracture from direct blow (defensive injury blocking strike). Treatment depends on displacement: Less than 50% displacement and less than 10° angulation: Cast/functional bracing acceptable. Greater than 50% displacement: ORIF. Associated injuries (radial head dislocation = Monteggia) must be excluded - always image elbow and wrist.
Q: What must be assessed with any isolated forearm bone fracture?
A: Always assess for associated joint injury: Monteggia: Ulna fracture + radial head dislocation (check radiocapitellar line). Galeazzi: Radius fracture + DRUJ disruption (check DRUJ on lateral, ulnar fovea tenderness). Essex-Lopresti: Radial head fracture + IOM disruption + DRUJ instability. "Fracture of necessity."
Q: What is the risk of compartment syndrome in forearm fractures?
A: Forearm has three compartments (volar, dorsal, mobile wad) all at risk. High-energy fractures, crush injuries, and combined radius-ulna fractures increase risk. Volar compartment most commonly affected. Monitor closely post-op. Fasciotomy via volar (Henry) + dorsal incisions if suspected. Median nerve first affected.
At a Glance
- Criteria
- under 50% disp, under 10° ang
- Management
- Functional Brace
- Criteria
- Displaced
- Management
- ORIF (DCP/LCP)
- Criteria
- Fracture + Joint Dislocation
- Management
- Emergency ORIF + Joint Stability
SP-PDeforming Forces
Hook:Supinators are up top, Pronators are down low. Muscle pull based on fracture level relative to Pronator Teres (PT).
MU-RNerve Review
Hook:Median, Ulnar, Radial cross the forearm. Key nerves at risk in forearm trauma.
GRU-MGaleazzi vs Monteggia
Hook:Galeazzi-Radius-Ulna-Monteggia. Differentiating complex forearm patterns.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old male labourer presents to the emergency department after a fall from height, landing on his outstretched dominant right forearm. X-rays show displaced mid-shaft fractures of both the radius and ulna at the middle third level. The fractures are transverse with minimal comminution. Neurovascular examination is intact, the skin is closed, and there are no signs of compartment syndrome. How do you manage this patient?”
“A 45-year-old man presents after an assault where he raised his forearm to block a blow from a baseball bat. X-rays show an isolated ulnar shaft fracture at the middle third with 60% displacement and 15 degrees of angulation. There is no radial fracture. He is complaining of severe pain in the forearm that seems out of proportion to the injury, and pain is worse with passive finger extension. The forearm feels tense on palpation. What are your immediate concerns and how do you proceed?”
“You are asked to see a 35-year-old man in clinic who underwent ORIF of both-bone forearm fractures 9 months ago at another hospital. He is very frustrated because despite the fractures healing well on X-ray, he has essentially no pronation or supination - his forearm is fixed in approximately 30 degrees of pronation. He works as an electrician and cannot perform his job. X-rays show healed radius and ulna fractures with well-positioned plates, but there is a 4cm bridge of heterotopic bone connecting the radius and ulna in the middle third of the forearm. What has happened and how do you manage this complication?”
Mandatory Steps
- Include elbow AND wrist in all imaging.
- Check PIN function (EIP/EDC) before every Henry approach.
- Restore radial bow apex to within 5% of contralateral side.
- Use 3.5mm plates with minimum 6 cortices per fragment.
Approaches
- Radius Volar: Henry (Interval: BR & FCR)
- Radius Dorsal: Thompson (Interval: ECRB & EDC)
- Ulna: Subcutaneous (Interval: FCU & ECU)
Surgical Dangers
- PIN in proximal third (Henry/Thompson).
- Median Nerve (Henry approach retraction).
- Synostosis (Single incision both-bone exposure).
- Compartment Syndrome (Missed deep volar release).
Evidence Base
Anderson et al. (1975) - Landmark
- Radius union 97.9%, ulna union 96.3%
- Established rigid compression plating as definitive treatment
- Underpins the modern 6-cortex / 3.5mm plating principle
Schemitsch & Richards (1992) - Landmark
- Restoring the normal radial bow correlated with a good result (over 80% of normal rotation, p less than 0.05)
- Recovery of grip strength linked to restoring the location of the bow (p less than 0.005)
- 84% achieved an excellent/good/acceptable result
Chapman et al. (1989)
- 98% union rate; 92% excellent or satisfactory function
- Infection rate 2.3%
- No refractures after removal of a 3.5mm plate (vs refracture after 4.5mm) - basis for choosing 3.5mm implants
Vasara et al. (2024) - Systematic Review
- Overall adverse-event rate 24%; major (reoperation/persistent) 14%
- Most common AEs: nerve injury 7% and nonunion 5%
- Mean DASH 12.5 (range 0-61) - good function with minor residual disability
Bergeron et al. (2012) - Review
- Risk relates to injury severity and surgical management (e.g. single shared exposure)
- Patients present with complete loss of active and passive rotation
- Early resection at 6-12 months is safe once radiographs show bony maturation; low recurrence after primary excision
Nappo et al. (2019)
- Final union 96% (primary 85%); nonunion linked to bone loss and infection
- Heterotopic ossification in 55%, radioulnar synostosis in 19%
- Synostosis (not HO alone) was the main driver of lost pronation-supination arc
- ORIF Plating
- 95-98%
- IM Nailing
- 80-90%
- ORIF Plating
- Low (under 2%)
- IM Nailing
- Very Low
- ORIF Plating
- Excellent
- IM Nailing
- Poor
References
- Anderson LD, Sisk D, Tooms RE, Park WI. Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am. 1975;57(3):287-97. PMID: 1091653
- Schemitsch EH, Richards RR. The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am. 1992;74(7):1068-78. PMID: 1522093
- Chapman MW, Gordon JE, Zissimos AG. Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am. 1989;71(2):159-69. PMID: 2918001
- Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986;68(7):1008-17. PMID: 3745238
- Vasara H, Stenroos A, Aspinen S, Kosola J, Anttila T, Nordback PH. Both-Bone Forearm Shaft Fractures Treated with Compression Plate Fixation in Adults: A Systematic Review on Adverse Events and Outcomes. JB JS Open Access. 2024;9(4). PMID: 39600799 DOI
- Bergeron SG, Desy NM, Bernstein M, Harvey EJ. Management of posttraumatic radioulnar synostosis. J Am Acad Orthop Surg. 2012;20(7):450-8. PMID: 22751164 DOI
- Nappo KE, Hoyt BW, Balazs GC, Nanos GP, Ipsen DF, Tintle SM, Polfer EM. Union Rates and Reported Range of Motion Are Acceptable After Open Forearm Fractures in Military Combatants. Clin Orthop Relat Res. 2019;477(4):813-820. PMID: 30811353 DOI
- Perretta DJ, Brock KM, Tejwani NC. Early Complications Associated with the Thompson Approach to the Proximal Radius. Bull Hosp Jt Dis (2013). 2016;74(4):293-297. PMID: 27815953
- Ryan MK, MacKay BJ, Tejwani NC. Both-bone forearm fracture with distal radioulnar joint dislocation. Am J Orthop (Belle Mead NJ). 2013;42(5):E30-2. PMID: 23710483
- Galeazzi R. Di una particolare sindrome traumatica dello scheletro dell'avambraccio. Arch Ortop. 1934;50:823. (Historical citation - predates PubMed indexing)