The repeating sequence of limb movements from one foot's initial contact to the next contact of the same foot
- Definition: One complete gait cycle runs from initial contact of one foot to the next contact of the same foot, divided into stance (60%) and swing (40%)
- Double vs single support: Double support occupies 20% total (10% at the start and 10% at the end of stance) and disappears at running speeds; single support equals the contralateral swing time
- Key kinetics: Vertical ground reaction force is an M-shaped double hump (first peak ~110% body weight at loading, valley ~80% at midstance, second peak ~110-120% at terminal stance)
- Clinical use: Phase-by-phase muscle and joint analysis localises pathology (Trendelenburg, antalgic, steppage, equinus) and guides surgical and rehabilitation planning
- “Quadriceps fire eccentrically at loading response (shock absorption); gastrocnemius-soleus fire concentrically at terminal stance (push-off)
- “Trendelenburg gait reflects weakness on the STANCE limb (gluteus medius), not the dropping side
- “Three ankle rockers (heel, ankle, forefoot) smooth centre-of-mass progression; losing them after ankle fusion raises walking energy cost
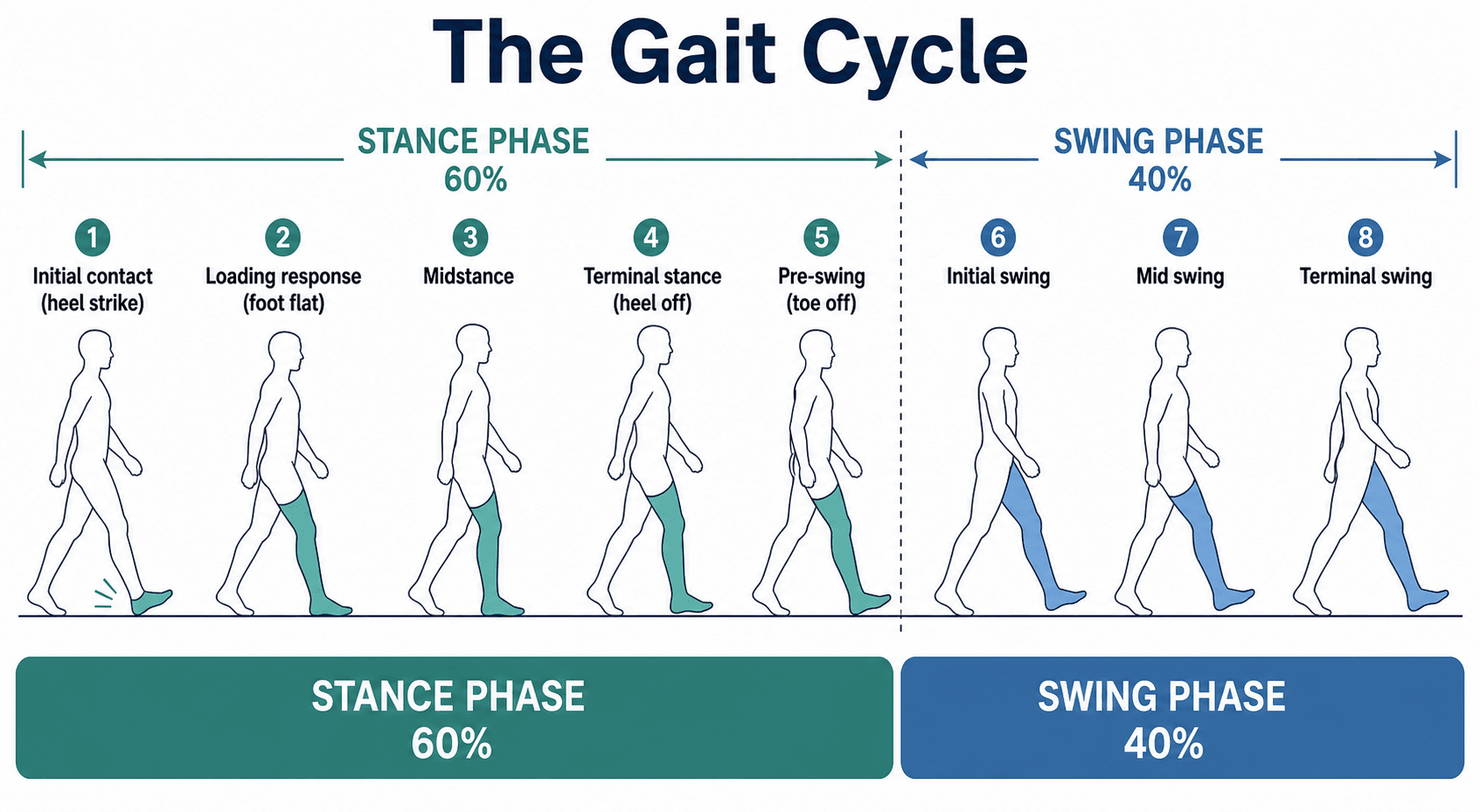
Gait Cycle Analysis
Stance phase: 60% of gait cycle. Swing phase: 40%. Double support: 20% (10% at beginning and end of stance). Single support: 40%. These percentages are exam favorites.
Initial contact: ankle dorsiflexors eccentric. Loading response: quadriceps eccentric. Terminal stance: gastrocnemius-soleus plantarflexion. Pre-swing: hip flexors initiate swing. Know the timing.
Vertical GRF shows double-hump pattern: first peak at loading response (110% body weight), second peak at terminal stance (120% body weight). Anterior-posterior force shows braking then propulsion.
Trendelenburg: weak hip abductors (gluteus medius). Antalgic: shortened stance on painful limb. Steppage: foot drop (weak dorsiflexors). Equinus: tight gastrocnemius. Know the underlying causes.
Overview
Definition
The gait cycle represents one complete sequence of walking from the initial ground contact of one foot to the subsequent ground contact of the same foot. [1] Normal human gait is characterized by alternating periods of single and double limb support, with each limb progressing through a repeating sequence of stance and swing phases that enable efficient forward progression while maintaining balance and minimizing energy expenditure. [2]
Temporal Parameters
Gait Cycle Division:
- Stance Phase: 60% of the gait cycle (from initial contact to toe-off)
- Swing Phase: 40% of the gait cycle (from toe-off to next initial contact)
- Double Support: 20% of the cycle (10% at beginning and 10% at end of stance)
- Single Support: 40% of the cycle (when contralateral limb is in swing)
The stance-to-swing ratio changes with walking speed, with faster speeds showing decreased stance time and increased swing time. [1,2]
Speed-Dependent Variables:
- Cadence: 90-120 steps per minute (normal adult walking)
- Stride length: 1.2-1.5 meters (distance between successive contacts of same foot)
- Step length: 0.6-0.8 meters (distance between contacts of opposite feet)
- Walking velocity: 1.2-1.4 meters per second (average adult)
These parameters vary with age, gender, height, and pathology. [3]
Epidemiology and Clinical Relevance
Gait analysis is fundamental to orthopaedic assessment:
- Diagnosis: Identifies specific gait abnormalities indicating underlying pathology
- Treatment planning: Guides surgical interventions (lengthening, osteotomy, fusion)
- Outcome assessment: Objective measurement of intervention effectiveness
- Rehabilitation: Informs physical therapy protocols and assistive device prescription
Three-dimensional gait analysis is the gold standard for quantifying gait deviations in cerebral palsy, neuromuscular disorders, and complex deformities. [4,5]
Gait Cycle Phases and Characteristics
Stance Phase (60% of Cycle)
Stance Phase Subdivisions
1. Initial Contact (0-2% of cycle)
- First moment when foot touches ground (historically termed "heel strike")
- Hip: 30 degrees flexion
- Knee: Near full extension (0-5 degrees flexion)
- Ankle: Neutral position (0 degrees)
- Foot: Supinated position preparing for contact
- Tibialis anterior: Maximum activity (eccentric) to control plantarflexion
- Quadriceps: Beginning activation to prepare for loading
- Hamstrings: Active to decelerate forward swing of leg
- Gluteus maximus: Active to control hip flexion
- Vertical force begins to rise from zero
- Posterior force component (braking) begins
- Center of pressure at heel contact point [1,6]
2. Loading Response (0-10% of cycle)
- Period from initial contact to contralateral toe-off
- Represents first period of double support
- Hip: 30 degrees flexion maintained
- Knee: Flexes to 15-20 degrees (shock absorption)
- Ankle: Plantarflexes 10-15 degrees (controlled by dorsiflexors)
- Foot: Progresses from supination to pronation
- Quadriceps: Eccentric contraction (critical for controlled knee flexion)
- Tibialis anterior: Eccentric contraction (controls foot slap)
- Hip abductors (gluteus medius/minimus): Activate to stabilize pelvis
- Hip extensors: Continue activity from initial contact
- Vertical force rapidly increases to first peak (110% body weight)
- Braking force reaches maximum
- Lateral force shows small lateral component
- This phase is critical for shock absorption and weight acceptance [1,6,7]
3. Midstance (10-30% of cycle)
- Single limb support phase begins
- Body weight passes over supporting foot
- Hip: Extends from 30 to 0 degrees
- Knee: Extends from 15-20 degrees to 5 degrees
- Ankle: Dorsiflexes from 10 degrees plantarflexion to 5 degrees dorsiflexion
- Foot: Pronated and flattened (shock absorption)
- Ankle plantarflexors (gastrocnemius-soleus): Begin activity to control tibial advancement
- Hip abductors: Maximum activity (single limb support stability)
- Quadriceps: Decreasing activity as knee extends
- Intrinsic foot muscles: Active for arch support
- Vertical force decreases from first peak to valley (80-90% body weight)
- Braking force transitions to propulsive force
- Center of pressure moves anteriorly along foot [1,6,7]
4. Terminal Stance (30-50% of cycle)
- From heel rise to contralateral initial contact
- Hip: Continues extension to 10-20 degrees hyperextension
- Knee: Remains near full extension (0-5 degrees flexion)
- Ankle: Dorsiflexes to maximum (10 degrees) as tibia advances over foot
- Foot: Heel rises, weight transfers to forefoot
- Gastrocnemius-soleus: Maximum activity (concentric plantarflexion for push-off)
- Hip extensors: Continue activity
- Intrinsic foot muscles: Maximum activity for rigid lever formation
- Tibialis posterior: Active for supination and arch support
- Vertical force increases to second peak (120% body weight)
- Propulsive force reaches maximum
- Center of pressure at metatarsal heads
- This phase generates forward propulsion [1,6,7]
5. Pre-swing (50-60% of cycle)
- From contralateral initial contact to toe-off
- Second period of double support
- Hip: Neutral to slight flexion
- Knee: Rapidly flexes to 40 degrees
- Ankle: Plantarflexes to 20 degrees (passive)
- Foot: Final push-off from hallux
- Hip flexors (iliopsoas, rectus femoris): Begin activation for swing initiation
- Ankle dorsiflexors: Begin activation preparing for swing
- Gastrocnemius-soleus: Decreasing activity
- Adductor longus: Active for limb advancement
- Vertical force rapidly decreases to zero
- Propulsive force decreases
- Center of pressure at toe [1,6,7]
Swing Phase (40% of Cycle)
Swing Phase Subdivisions
6. Initial Swing (60-73% of cycle)
- From toe-off to feet adjacent
- Acceleration phase of swing
- Hip: Rapidly flexes to 20 degrees
- Knee: Flexes to maximum (60 degrees) for toe clearance
- Ankle: Dorsiflexes from plantarflexion toward neutral
- Foot: Clears ground by approximately 1 cm
- Hip flexors (iliopsoas): Concentric contraction for limb advancement
- Tibialis anterior: Active to achieve foot clearance
- Short head of biceps femoris: Assists hip flexion
- Rectus femoris: Active for both hip flexion and knee extension initiation
- No ground contact (zero force on swinging limb)
- Contralateral limb in single support [1,8]
7. Mid-swing (73-87% of cycle)
- From feet adjacent to tibia vertical
- Hip: Continues flexion to 30 degrees
- Knee: Begins extension from 60 to 30 degrees (passive pendular motion)
- Ankle: Achieves neutral position (0 degrees)
- Foot: Maintains clearance
- Tibialis anterior: Maintains dorsiflexion for clearance
- Hip flexors: Continue activity
- Quadriceps: Begin activity to extend knee
- Hamstrings: Begin activity to decelerate knee extension
- No ground contact
- Minimum muscle activity during this phase (most efficient part of gait) [1,8]
8. Terminal Swing (87-100% of cycle)
- From tibia vertical to next initial contact
- Deceleration phase
- Hip: Maintains 30 degrees flexion
- Knee: Extends to near full extension (0-5 degrees flexion)
- Ankle: Maintains neutral dorsiflexion
- Foot: Prepares for initial contact
- Hamstrings: Maximum activity (eccentric) to decelerate knee extension
- Tibialis anterior: Maintains ankle dorsiflexion
- Quadriceps: Active to achieve full knee extension
- Gluteus maximus: Begins activation for upcoming stance
- No ground contact until next initial contact [1,8]
Principles of Joint Kinematics and Range of Motion
Each lower-limb joint follows a characteristic, repeatable angle-versus-cycle curve. The core principle is that motion is task-specific: the hip and ankle drive progression and power, while the knee provides two flexion waves - one for shock absorption in stance and one for toe clearance in swing. Deviations from these normative curves localise pathology to a joint, plane and phase.
Joint Motion During Gait
Hip Joint Motion
- Maximum flexion: 30 degrees (at initial contact and terminal swing)
- Neutral: 0 degrees (at midstance)
- Maximum extension: 10-20 degrees (at terminal stance)
- Total range of motion: 40-50 degrees
- Small amplitude motion (5-7 degrees total)
- Slight abduction during single limb support
- Returns to neutral during double support
- Internal rotation during loading response (5 degrees)
- External rotation during terminal stance (5 degrees)
- Total rotation: approximately 10 degrees
The hip joint serves as the primary controller of limb advancement and body progression. [9]
Knee Joint Motion
- Initial contact: 0-5 degrees flexion
- Loading response: 15-20 degrees flexion (shock absorption)
- Midstance: 5 degrees flexion
- Terminal stance: 0-5 degrees flexion
- Pre-swing: 40 degrees flexion
- Initial swing: Maximum flexion 60 degrees
- Terminal swing: Returns to 0-5 degrees
- First wave: Loading response flexion (shock absorption)
- Second wave: Swing phase flexion (toe clearance)
The knee demonstrates the largest range of motion of any lower extremity joint during gait (0-60 degrees). [9,10]
Ankle Joint Motion
- Initial contact: Neutral (0 degrees)
- Loading response: 10-15 degrees plantarflexion (controlled)
- Midstance to terminal stance: Progressive dorsiflexion to 10 degrees
- Pre-swing: Rapid plantarflexion to 20 degrees
- Swing phase: Return to neutral dorsiflexion
- Controlled plantarflexion prevents foot slap
- Dorsiflexion accommodates forward tibial progression
- Plantarflexion generates propulsive power
- Neutral position enables toe clearance [9,10]
Foot and Subtalar Motion
Pronation-Supination Sequence:
- Initial contact: Supinated (rigid structure for heel contact)
- Loading response to midstance: Pronation (shock absorption, adaptation)
- Terminal stance: Resupination (rigid lever for push-off)
This pronation-supination cycle is essential for:
- Shock absorption during loading
- Adaptation to uneven terrain
- Conversion to rigid lever for propulsion [11]
Muscle Activation Patterns (Neuromuscular Control)
Ankle Dorsiflexors (Tibialis Anterior)
- Terminal swing to initial contact: Concentrically activate to achieve neutral ankle position
- Loading response: Eccentrically contract (maximum activity) to control plantarflexion and prevent foot slap
- Swing phase: Active throughout to maintain toe clearance
- Weakness produces foot drop and steppage gait
- Excessive activity seen in spastic gait patterns [6,12]
Ankle Plantarflexors (Gastrocnemius-Soleus)
- Midstance to terminal stance: Progressive increase in activity
- Terminal stance: Maximum concentric contraction for push-off (second rocker)
- Pre-swing: Rapidly decreasing activity
- Gastrocnemius-soleus complex generates majority of propulsive power
- Contributes to forward acceleration of center of mass
- Critical for normal walking speed and efficiency [6,12]
Quadriceps Muscle Group
- Terminal swing: Begins activation to extend knee
- Initial contact to loading response: Maximum eccentric activity to control knee flexion (critical for shock absorption)
- Midstance: Decreasing activity as knee extends
- Weakness produces instability during loading response
- May cause knee hyperextension or flexed knee gait as compensation [12]
Hamstring Muscle Group
- Terminal swing: Maximum eccentric activity to decelerate knee extension and control hip flexion
- Initial contact: Continue activity for hip extension
- Loading response to midstance: Decreasing activity
- Decelerate lower leg during terminal swing
- Assist hip extension during early stance [12]
Hip Abductors (Gluteus Medius and Minimus)
- Loading response through midstance: Maximum activity during single limb support
- Terminal stance: Decreasing activity
- Stabilize pelvis in coronal plane during single limb support
- Prevent contralateral pelvic drop (Trendelenburg sign)
- Weakness produces characteristic Trendelenburg gait [12,13]
Hip Flexors (Iliopsoas)
- Pre-swing: Begin activation to initiate swing
- Initial swing to mid-swing: Continue activity for limb advancement
- Terminal swing: Decreasing activity
- Primary driver of swing phase initiation
- Advance limb forward during swing [12]
Ground Reaction Forces: Kinetic Analysis
Vertical Ground Reaction Force
- Loading response: Rapid rise to first peak (110% body weight)
- Midstance: Decrease to valley (80-90% body weight)
- Terminal stance: Increase to second peak (120% body weight)
- Pre-swing: Rapid decrease to zero
- First peak: Weight acceptance and impact absorption
- Valley: Single limb support with body passing over foot
- Second peak: Push-off and propulsion
- Shape varies with walking speed and pathology [7,14]
Anterior-Posterior Ground Reaction Force
- Loading response to midstance: Posterior (braking) force reaches maximum (15-20% body weight)
- Midstance: Transition from braking to propulsion
- Terminal stance: Anterior (propulsive) force reaches maximum (20-25% body weight)
- Braking force decelerates forward progression
- Propulsive force accelerates body forward
- Forces approximately equal in normal gait (net zero horizontal acceleration) [7,14]
Mediolateral Ground Reaction Force
Lateral Stability:
- Small amplitude forces (5% body weight)
- Medially directed during loading response
- Laterally directed during terminal stance
- Maintains mediolateral stability [7,14]
Center of Pressure Progression
Path During Stance:
- Initial contact: Lateral heel
- Loading response to midstance: Progresses along lateral border of foot
- Terminal stance: Moves medially toward metatarsal heads
- Pre-swing: Terminates at hallux
This progression reflects the foot's rocker mechanism and weight transfer pattern. [11,14]
Perry's Six Determinants of Gait
Saunders, Inman, and Eberhart described six major determinants that minimize energy expenditure during normal gait by reducing vertical and lateral displacement of the center of mass. [15]
1. Pelvic Rotation
- Mechanism: Pelvis rotates approximately 4 degrees forward on the swing side
- Effect: Effectively lengthens the limb during initial contact and terminal swing
- Energy saving: Reduces amplitude of vertical displacement of center of mass
2. Pelvic Tilt
- Mechanism: Pelvis drops approximately 5 degrees on the swing side (contralateral hip adduction)
- Effect: Lowers the peak of vertical displacement during single limb support
- Energy saving: Flattens the sinusoidal curve of center of mass trajectory
3. Knee Flexion During Stance
- Mechanism: Knee flexes 15-20 degrees during loading response
- Effect: Lowers the body during what would otherwise be highest point
- Energy saving: Reduces vertical displacement amplitude
4. Foot and Ankle Motion
- Mechanism: Foot serves as rocker in three phases (heel, ankle, forefoot)
- Effect: Smooths the forward progression of center of mass
- Energy saving: Prevents abrupt changes in velocity
5. Knee Mechanism
- Mechanism: Coordinated knee flexion-extension pattern throughout stance
- Effect: Works with ankle motion to smooth progression
- Energy saving: Reduces energy required for limb advancement
6. Lateral Pelvic Displacement
- Mechanism: Pelvis shifts laterally approximately 4-5 cm from side to side
- Effect: Keeps center of mass closer to supporting limb
- Energy saving: Reduces need for excessive hip abductor force
Clinical Application: Loss of any determinant (e.g., fused knee, ankle arthrodesis) increases energy cost of walking by requiring greater muscular effort and increased vertical displacement. [15,16]
Pathological Gait Patterns
Differential Diagnosis of Common Gait Patterns
Pattern recognition is the highest-yield exam skill: match the visible deviation to the underlying lesion.
- Key Visible Feature
- Shortened stance on painful limb
- Phase Affected
- Stance
- Underlying Lesion / Cause
- Pain (arthritis, fracture, infection) in any lower-limb joint
- Key Visible Feature
- Contralateral pelvic drop / trunk lean over stance leg
- Phase Affected
- Single-limb stance
- Underlying Lesion / Cause
- Hip abductor weakness - gluteus medius, superior gluteal nerve, hip OA/DDH
- Key Visible Feature
- Exaggerated hip/knee flexion, foot slap
- Phase Affected
- Swing and initial contact
- Underlying Lesion / Cause
- Foot drop - common peroneal palsy, L5 radiculopathy, peripheral neuropathy
- Key Visible Feature
- Forefoot initial contact, no heel strike
- Phase Affected
- Stance
- Underlying Lesion / Cause
- Gastrocnemius-soleus contracture, spastic CP, idiopathic toe-walking
- Key Visible Feature
- Swing limb traces a lateral semicircle
- Phase Affected
- Swing
- Underlying Lesion / Cause
- Functional limb lengthening - stiff/fused knee or ankle, hip flexor weakness, spasticity
- Key Visible Feature
- Rises onto stance-side toes to clear the swing limb
- Phase Affected
- Swing
- Underlying Lesion / Cause
- Inadequate swing-limb clearance (long leg, knee/ankle stiffness, prosthesis)
- Key Visible Feature
- Stiff extended limb, circumduction, equinovarus foot
- Phase Affected
- Whole cycle
- Underlying Lesion / Cause
- Upper motor neurone lesion - stroke, TBI, hemiplegic CP
- Key Visible Feature
- Shuffling short steps, reduced arm swing, stooped posture
- Phase Affected
- Whole cycle
- Underlying Lesion / Cause
- Basal ganglia dysfunction - Parkinson disease, parkinsonism
- Key Visible Feature
- Wide base, irregular step length, instability
- Phase Affected
- Whole cycle
- Underlying Lesion / Cause
- Cerebellar disease or sensory (proprioceptive) ataxia
- Key Visible Feature
- Pelvic drop and trunk dip to short side each step
- Phase Affected
- Stance
- Underlying Lesion / Cause
- True or apparent limb-length discrepancy
Common Gait Abnormalities
Antalgic Gait
- Shortened stance phase on painful limb
- Rapid transfer of weight to opposite limb
- Decreased vertical ground reaction force on affected side
- May show decreased hip and knee motion
- Arthritis (hip, knee, ankle)
- Fracture or stress fracture
- Muscle strain or tendinopathy
- Any painful lower extremity condition [17]
Trendelenburg Gait
- Contralateral pelvic drop during stance on affected limb
- Trunk lean toward affected side (compensated Trendelenburg)
- Decreased stance time on affected side
- Gluteus medius weakness or paralysis
- Hip joint pathology (arthritis, developmental dysplasia)
- L5 radiculopathy (superior gluteal nerve)
- Post-hip surgery (nerve injury) [13,17]
Steppage Gait (Foot Drop)
- Exaggerated hip and knee flexion during swing phase
- Foot slap at initial contact
- Dragging toe if compensation inadequate
- Common peroneal nerve palsy
- L5 radiculopathy
- Anterior compartment syndrome
- Peripheral neuropathy
- Sciatic nerve injury [17]
Equinus Gait (Toe Walking)
- Initial contact with forefoot instead of heel
- Excessive plantarflexion throughout stance
- Shortened stride length
- May show knee hyperextension (compensation)
- Gastrocnemius-soleus contracture
- Achilles tendon shortening
- Cerebral palsy (spastic)
- Clubfoot (residual or recurrent)
- Idiopathic toe walking (children) [17]
Vaulting Gait
- Excessive plantarflexion on stance limb
- Rising up on toes to clear opposite limb
- Seen during swing phase of affected limb
- Functional leg length discrepancy
- Inability to flex knee or dorsiflex ankle on swing side
- Compensation for inadequate limb clearance [17]
Circumduction Gait
- Swing limb traces semicircular path
- Hip abduction and external rotation during swing
- Increased energy expenditure
- Limb length discrepancy
- Knee or ankle fusion/stiffness
- Hip flexor weakness
- Spasticity (stroke, cerebral palsy) [17]
Spastic Gait (Hemiplegic)
- Affected limb held in extension
- Circumduction during swing phase
- Equinovarus foot position
- Decreased knee flexion during swing
- Stroke (cerebrovascular accident)
- Traumatic brain injury
- Cerebral palsy (hemiplegic type) [17]
Parkinsonian Gait
- Shuffling steps with reduced stride length
- Decreased arm swing
- Flexed posture (trunk, hips, knees)
- Festinating gait (rapid small steps)
- Difficulty initiating movement
- Parkinson disease
- Parkinsonism (drug-induced, vascular) [17]
Clinical Gait Assessment: Observational Gait Analysis
Systematic Visual Assessment
- Initial contact: Heel strike, knee extended, ankle neutral
- Loading response: Knee flexion, controlled plantarflexion
- Midstance: Tibia advances over foot, knee extends
- Terminal stance: Heel rise, ankle dorsiflexion
- Pre-swing: Toe-off, rapid knee flexion
- Swing phase: Knee flexion peak, ankle dorsiflexion
- Pelvic stability during single limb support
- Hip abduction-adduction
- Knee varus-valgus alignment
- Foot progression angle (internal/external rotation)
- Base width (normal: 5-10 cm)
- Decreased stance time (antalgic)
- Excessive pelvic drop (Trendelenburg)
- Knee hyperextension (quadriceps weakness, knee instability)
- Foot slap (dorsiflexor weakness)
- Toe walking (equinus contracture) [17,18]
Instrumented Gait Analysis
- Gold standard for quantifying gait deviations
- Uses multiple cameras and reflective markers
- Measures joint angles in three planes
- Calculates joint moments and powers
- Essential for complex deformity assessment (cerebral palsy) [4,5]
- Measures ground reaction forces in three directions
- Calculates center of pressure trajectory
- Determines temporal parameters
- Assesses asymmetry between limbs [14]
- Records muscle activation timing and amplitude
- Identifies abnormal muscle firing patterns
- Guides treatment (e.g., selective dorsal rhizotomy, botulinum toxin) [12]
Guidelines, Registries & Global Practice
Global Epidemiology and Clinical Drivers
- Gait disorders are common and rise steeply with age: a frequently cited US community study (Verghese and colleagues) found abnormal gait in roughly one-third of adults over 70, with neurological and multifactorial causes predominating.
- Cerebral palsy, the single largest indication for instrumented gait analysis, has a global prevalence of approximately 2 per 1000 live births, higher in preterm and low-birth-weight infants and in lower-resource perinatal settings.
- Reduced walking speed is an established marker of frailty and predicts falls, hospitalisation and mortality, making spatiotemporal gait a low-cost global health metric.
Guideline and Society Positions (Side by Side)
- Position on Gait Analysis
- Supports 3D instrumented gait analysis to inform single-event multilevel surgery and to evaluate outcomes in cerebral palsy
- Position on Gait Analysis
- Cerebral palsy guidance recommends specialist assessment, with instrumented gait analysis used in tertiary centres before complex multilevel surgery
- Position on Gait Analysis
- Routine use of motion-analysis laboratories for surgical planning and outcome measurement in CP and complex deformity
- Position on Gait Analysis
- Endorse 3D gait laboratories as the reference standard for quantifying gait deviation and guiding orthopaedic intervention
The common thread worldwide: observational analysis is universal and free; instrumented 3D analysis is reserved for complex (mainly neuromuscular) cases and for pre-/post-surgical assessment, with concentration in tertiary referral laboratories.
Standardisation and Outcome Measures
- There is no implant/arthroplasty-style registry for gait; instead, standardisation comes from shared marker models (Helen Hayes / Plug-in-Gait, derived from Kadaba's work) and validated summary scores - the Gait Deviation Index (GDI) and the Gait Profile Score (GPS) - which enable comparison across laboratories.
- Movement-analysis societies (e.g. ESMAC in Europe, GCMAS in North America) publish laboratory accreditation and good-practice standards to improve cross-centre comparability.
High- vs Limited-Resource Practice Variation
- High-resource settings: dedicated optoelectronic gait laboratories with force plates, dynamic EMG and, increasingly, markerless/wearable systems; routine pre-operative analysis for cerebral palsy multilevel surgery.
- Limited-resource settings: reliance on structured observational gait analysis (Edinburgh Visual Gait Score, Physician Rating Scale), smartphone video and timed walk tests (10-metre and 6-minute walk), which are validated, portable and inexpensive substitutes that capture most clinically actionable information.
Controversies and Areas of Uncertainty
Gait analysis is mature science, but several issues remain genuinely debated and are favourite "higher-order" viva topics.
- Validity of the six determinants of gait. The Saunders/Inman/Eberhart model remains the standard teaching framework, yet dynamic-walking and inverted-pendulum studies (e.g. Gard and colleagues) showed that pelvic rotation and pelvic list contribute little to flattening the centre-of-mass trajectory. The determinants are now best taught as a conceptual scaffold rather than a quantitatively exact energy model.
- Clinical impact of instrumented 3D gait analysis. It is the reference standard for quantifying deviations, but high-level evidence that it changes hard outcomes is limited. It demonstrably alters and often de-escalates surgical recommendations in cerebral palsy, yet routine 3D analysis before all multilevel surgery is not universally funded or adopted, and reliability depends on marker placement and modelling.
- Single global indices vs full curve interpretation. Summary scores such as the Gait Deviation Index and Gait Profile Score give reproducible severity tracking, but a single number can mask which joint or plane is abnormal; experts disagree on how far they should replace expert reading of kinematic curves.
- Terminology and normative ranges. "Heel strike" versus "initial contact", differing phase percentage boundaries between texts, and laboratory-specific normative bands mean reported joint angles and force values are approximate and method-dependent rather than fixed constants.
- Markerless and wearable gait analysis. Inertial-sensor and video/AI markerless systems are rapidly emerging as cheaper, clinic-friendly alternatives, but their agreement with gold-standard optoelectronic systems and their role in surgical decision-making are still being established.
High-Yield MCQ Topics
Temporal Parameters
- Stance phase = 60% of gait cycle
- Swing phase = 40% of gait cycle
- Double support = 20% total (10% at beginning and end of stance)
- Single support = 40% of cycle
- As walking speed increases, stance time decreases and swing time increases
Ground Reaction Forces
- First peak: 110% body weight (loading response)
- Valley: 80-90% body weight (midstance)
- Second peak: 120% body weight (terminal stance)
- Braking force maximum: 15-20% body weight
- Propulsive force maximum: 20-25% body weight
Joint Range of Motion
- Hip: 30 degrees flexion to 20 degrees extension (total 50 degrees)
- Knee: 0-60 degrees flexion (maximum at initial swing)
- Ankle: 10 degrees dorsiflexion to 20 degrees plantarflexion (total 30 degrees)
Muscle Activation
- Loading response: quadriceps eccentric (shock absorption)
- Terminal stance: gastrocnemius-soleus concentric (propulsion)
- Midstance: hip abductors maximum (pelvic stability)
- Terminal swing: hamstrings eccentric (knee deceleration)
Pathological Gait Recognition
- Trendelenburg = hip abductor weakness (gluteus medius)
- Steppage = foot drop (tibialis anterior weakness)
- Antalgic = shortened stance on painful side
- Equinus = toe walking (gastrocnemius contracture)
Joint Moments and Powers: the Kinetics of Gait
The topic covers kinematics (joint angles) and ground reaction forces in depth, the instrumented-analysis section lists "joint moments and powers", and the Winter EvidenceCard is entirely about joint power phases - but the body never explains what an internal joint moment or a joint power actually is, which is the higher-order kinetic layer examiners probe.
- Internal (net) joint moment. The ground reaction force acts at a distance (a moment arm) from each joint, creating an external moment that tends to collapse the limb; the muscles and passive structures generate an equal-and-opposite internal moment to control it. The net internal moment through the cycle is the kinetic signature of what the muscles are doing. Example: at loading the GRF passes behind the knee (external flexion moment → the quadriceps generate an internal EXTENSOR moment); at midstance the GRF passes in front of the knee (external extension moment → the knee is passively stable and quadriceps demand falls). The "support moment" - the sum of the hip, knee and ankle sagittal moments - stays net-extensor through stance to stop the limb collapsing, a key stability concept.
- Joint power = moment x joint angular velocity. Positive power = the muscle is generating energy (concentric, shortening) - a "burst"; negative power = the muscle is absorbing energy (eccentric, lengthening) - a "sink". This converts the qualitative "eccentric/concentric" description into a measurable quantity.
- The classic power profile (Winter). The ankle shows early absorption (controlled dorsiflexion in stance) then a large positive-work push-off burst ("A2") at terminal stance - the single biggest power generator in gait; the knee shows several smaller absorption/generation phases; the hip contributes a pull-off/flexion burst. This is exactly why calf weakness, ankle fusion or a below-knee amputation is so disabling - the dominant A2 power source is lost.
- Why it matters clinically. Moments and powers, not angles alone, reveal which muscle group is failing or over-working and where mechanical energy is lost - the basis of instrumented-gait surgical decisions such as tendon transfers (see the Dreher rectus-transfer trial).
Q: What is the difference between a joint moment and a joint power in gait? A: The internal joint moment is the net muscular effort opposing the external ground-reaction-force moment (e.g. an internal knee EXTENSOR moment at loading resists the GRF trying to flex the knee); the sum across hip/knee/ankle is the net-extensor support moment that keeps the limb from collapsing. Joint power = moment x angular velocity: positive = energy generation (concentric burst), negative = absorption (eccentric sink). The ankle A2 push-off burst is the largest power generator in gait, which is why losing it (calf weakness, ankle fusion, BKA) is so costly.
The Inverted Pendulum Model and Pendular Energy Exchange
The controversies section notes that "inverted-pendulum studies" challenged the six determinants, and the whole energy-conservation theme rests on this model - but the topic never explains it.
- The model. During single-limb stance the body vaults over the relatively stiff stance leg like an inverted pendulum pivoting at the foot: the centre of mass rises to its highest point at midstance and falls during double support, tracing a smooth arc rather than a flat line.
- Energy exchange is the whole point. In a pendulum, potential energy (PE) and kinetic energy (KE) trade back and forth out of phase. At midstance the COM is highest and slowest - maximum PE, minimum KE; at double support it is lowest and fastest - minimum PE, maximum KE. Because they are out of phase, much of the energy is exchanged passively rather than supplied by muscle - normal walking recovers roughly 60-70% of the mechanical energy this way, which is why level walking is metabolically cheap.
- How it reframes Perry's determinants. The Saunders/Inman determinants were taught as flattening the COM path to save energy; the inverted-pendulum view shows that a smooth pendular arc (not a flat path) is what maximises PE-KE exchange, and modelling (Gard and colleagues) found pelvic rotation and pelvic list actually contribute little - so the determinants are best treated as a teaching scaffold, with the inverted pendulum the better mechanical account of walking economy.
- Clinical corollary. Anything that disrupts the pendulum - a stiff/fused joint that cannot vault smoothly, an antalgic gait that shortens stance, or loss of the ankle push-off that re-launches the COM into the next step - breaks the PE-KE exchange and raises the metabolic cost of walking (as the Waters energy-expenditure data quantify).
Q: What is the inverted pendulum model and why does it explain the low energy cost of walking? A: In stance the body vaults over the stiff stance limb like an inverted pendulum; potential and kinetic energy exchange out of phase (max PE/min KE at midstance, min PE/max KE at double support), so about 60-70% of the mechanical energy is recovered passively without muscular work. It reframes Perry's determinants (a smooth pendular arc, not a flattened COM path, maximises the exchange; pelvic rotation/list add little - Gard). Losing the smooth vault (fused joint, antalgic gait, absent ankle push-off) breaks the exchange and raises walking energy cost.
MCQ Practice Points
Q: What are the phases of the gait cycle and their relative durations?
A: Stance phase: 60% of cycle (heel strike to toe-off). Swing phase: 40% of cycle (toe-off to heel strike). Stance subdivided: initial contact (0-2%), loading response (2-12%), mid-stance (12-31%), terminal stance (31-50%), pre-swing (50-60%). Double limb support occurs at 0-12% and 50-60%.
Q: What are the six determinants of gait described by Saunders?
A: 1) Pelvic rotation (4° each direction), 2) Pelvic tilt (5° drop on swing side), 3) Knee flexion in stance (15-20°), 4) Foot mechanisms (ankle plantarflexion/dorsiflexion), 5) Knee mechanisms, 6) Lateral displacement of pelvis. These minimize vertical and lateral center of mass displacement, reducing energy expenditure.
Q: What muscle activity occurs during loading response phase of gait?
A: Tibialis anterior: Eccentric contraction controlling plantarflexion (foot slap prevention). Quadriceps: Eccentric contraction controlling knee flexion. Gluteus maximus/medius: Hip stabilization. This phase absorbs impact forces as body weight transfers onto the limb. Peak ground reaction force occurs here.
Q: What causes Trendelenburg gait?
A: Weakness of hip abductors (gluteus medius/minimus) on stance side causes contralateral pelvis to drop during single-limb support. Patient compensates with trunk lean toward affected side (compensated Trendelenburg). Causes: L5 radiculopathy, superior gluteal nerve injury, hip pathology, abductor mechanism failure post-THA.
Q: What is the center of mass displacement during normal gait?
A: Normal gait has approximately 5cm vertical displacement (sinusoidal pattern, lowest at double support, highest at mid-stance) and 4cm lateral displacement (side to side with each step). The determinants of gait minimize these excursions. Greater displacement = increased energy expenditure.
At a Glance
The gait cycle is the repeating sequence of limb movements from heel strike to next heel strike, divided into stance phase (60%) and swing phase (40%). Double support occurs for 20% of the cycle (10% at beginning and end of stance). Critical muscle activations include eccentric dorsiflexors at initial contact, eccentric quadriceps during loading, and gastrocnemius-soleus push-off at terminal stance. Recognise pathological patterns: Trendelenburg (weak hip abductors), antalgic (shortened stance on painful side), steppage (foot drop from weak dorsiflexors), and equinus (tight gastrocnemius).
I Love My Two PillowsPhases of Stance Phase
Hook:Think of resting on pillows through the stance phase from heel to toe
I Must TryPhases of Swing Phase
Hook:Like swinging a baseball bat: accelerate, maintain arc, decelerate
PELVIC KneeGait Determinants of Perry
Hook:Perry's PELVIC movements plus Knee mechanics reduce energy cost of walking
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An examiner asks you to describe the phases of the gait cycle and their relative durations. They then ask about the muscle activity patterns during these phases.”
“A 65-year-old patient presents with a noticeable limp. On observation, you note that the pelvis drops on the right side when standing on the left leg. The examiner asks you to explain this finding and its underlying causes.”
“The examiner presents a patient with bilateral ankle arthrodesis who complains of fatigue with walking. They ask you to explain why ankle fusion increases the energy cost of gait.”
Temporal Divisions
- Stance phase: 60% of cycle (initial contact to toe-off)
- Swing phase: 40% of cycle (toe-off to next initial contact)
- Double support: 20% total (10% early stance, 10% late stance)
- Single support: 40% of cycle (contralateral limb in swing)
Stance Phase Subdivisions
- Initial contact (0-2%): heel strike, knee extended
- Loading response (0-10%): foot flat, knee flexes 15 degrees, first double support
- Midstance (10-30%): single limb support, body over foot
- Terminal stance (30-50%): heel rise, maximum ankle dorsiflexion
- Pre-swing (50-60%): toe-off, rapid knee flexion, second double support
Swing Phase Subdivisions
- Initial swing (60-73%): acceleration, knee flexion to 60 degrees
- Mid-swing (73-87%): toe clearance, passive knee extension
- Terminal swing (87-100%): deceleration, knee extends, prepare for contact
Key Muscle Actions
- Tibialis anterior: eccentric loading response (prevent foot slap), active swing (toe clearance)
- Quadriceps: eccentric loading response (control knee flexion 15-20 degrees)
- Gastrocnemius-soleus: concentric terminal stance (push-off, 120% BW force)
- Gluteus medius: maximum midstance (pelvic stability, prevent Trendelenburg)
- Hamstrings: eccentric terminal swing (decelerate knee extension)
Ground Reaction Forces
- Vertical GRF: first peak 110% BW (loading), valley 80-90% BW (midstance), second peak 120% BW (push-off)
- Anterior-posterior: braking 15-20% BW, then propulsion 20-25% BW
- Mediolateral: small amplitude 5% BW for lateral stability
Joint ROM During Gait
- Hip: 30 degrees flexion to 20 degrees extension (total 50 degrees)
- Knee: 0 degrees to 60 degrees flexion (max at initial swing, 15-20 degrees at loading response)
- Ankle: 10 degrees dorsiflexion (terminal stance) to 20 degrees plantarflexion (pre-swing)
Perry's Six Gait Determinants
- 1. Pelvic rotation (4 degrees forward on swing side)
- 2. Pelvic tilt (5 degrees drop on swing side)
- 3. Knee flexion during stance (15-20 degrees at loading response)
- 4. Foot-ankle motion (three rockers: heel, ankle, forefoot)
- 5. Knee mechanism (coordinated flexion-extension)
- 6. Lateral pelvic displacement (4-5 cm side-to-side)
- Function: minimize vertical and lateral displacement of center of mass to conserve energy
Pathological Gait Patterns
- Trendelenburg: pelvic drop on unsupported side = hip abductor weakness (gluteus medius)
- Antalgic: shortened stance on painful limb = pain avoidance
- Steppage: excessive hip/knee flexion in swing = foot drop (tibialis anterior weakness)
- Equinus: toe walking, forefoot initial contact = gastrocnemius contracture
- Vaulting: rising on stance toes = inadequate swing limb clearance
- Circumduction: swing limb traces semicircle = limb length discrepancy or joint stiffness
Energy Expenditure
- Normal walking: 0.063 mL O2/kg/m
- Bilateral ankle fusion: 20-30% increase in metabolic cost
- Hemiplegic gait: 60% increase
- Loss of any gait determinant increases energy cost
- Rocker-bottom shoes can partially restore efficiency after ankle fusion
Evidence Base and Key Studies
The Major Determinants in Normal and Pathological Gait (Foundational Theory)
- Described six kinematic determinants that flatten the sinusoidal path of the body centre of mass and so reduce the energy cost of walking
- The six determinants: pelvic rotation, pelvic tilt (list), knee flexion in stance, foot-ankle interaction (rockers), knee-ankle interaction, and lateral pelvic displacement
- Argued that loss of any determinant (e.g. a fused joint) forces compensatory motion and raises metabolic demand
The Development of Mature Gait - Landmark EMG/Kinematic Series
- Combined cinematography, force-plate and EMG data to define normal and maturing gait in children
- Identified five maturity determinants and showed adult-pattern gait is essentially established by about age 7
- Documented the phasic timing of muscle activity (e.g. quadriceps at loading response, gastrocnemius-soleus at terminal stance) that underpins modern gait interpretation
Energy Generation and Absorption at the Ankle and Knee (Joint Power Analysis)
- Biomechanical analysis of 15 normal adults at slow, natural and fast cadences
- The ankle has two power phases: negative work (absorption) during weight acceptance then a dominant positive-work burst at push-off, identifying the plantarflexors as the prime movers of forward propulsion
- The dominant plantarflexor push-off burst falls as walking speed decreases; the knee shows four distinct power phases
Measurement of Lower Extremity Kinematics During Level Walking (3D Marker Model)
- Developed and validated an external marker set and Euler-angle algorithms (the basis of the Helen Hayes / Plug-in-Gait model) on a VICON system
- Gait analysis repeated on 40 normal young adults across three separate test days produced repeatable hip, knee, ankle and pelvis angle curves
- Quantified the effect of marker-placement and embedded-axis uncertainty on joint-angle error
Energy Expenditure of Normal and Pathologic Gait (Comprehensive Review)
- Synthesised oxygen-consumption data across neurological and orthopaedic conditions, using the rate of energy expenditure and energy cost per metre as the key metrics
- Pathological gait raises energy cost broadly in proportion to the level and severity of disability, with patients typically self-selecting a slower speed to keep the rate of expenditure near normal
- Hemiplegic, paraplegic and high-level amputation gaits carry the largest penalties; more proximal amputation and greater neurological involvement cost more
Comfortable and Maximum Walking Speed - Reference Values (Age 20-79)
- 230 healthy adults timed over a 7.62 m walkway, generating decade- and sex-specific reference speeds
- Comfortable speed ranged from ~127 cm/s (women in their 70s) to ~146 cm/s (men in their 40s); maximum speed up to ~253 cm/s in young men
- Walking speed correlated with age, height and lower-limb muscle strength and was highly reliable (coefficients greater than 0.9)
The Significance of the Trendelenburg Test (Standardisation Study)
- Examined 50 normal subjects and 103 patients with spine or hip disorders to standardise single-leg stance testing
- Defined the test as an assessment of hip abductor function and specified a standard performance method
- Catalogued the main false-positive (pain, poor cooperation, rib-iliac impingement) and false-negative (trunk/pelvic compensation) pitfalls
The Gait Deviation Index (GDI) - Comprehensive Index of Gait Pathology
- Derived a multivariate, single-number index of overall gait pathology from 15 independent kinematic gait features
- GDI is scaled so 100 represents the mean of typically developing children and every 10 points below 100 is one standard deviation of pathology
- Validated against the Gillette Gait Index and functional walking scales and shown to track severity across cerebral palsy topographical types
Distal Rectus Femoris Transfer in Multilevel Surgery - Randomized Trial
- 32 children with spastic diplegia indicated for distal rectus femoris transfer (DRFT) randomised to single-event multilevel surgery with or without DRFT, with 3D gait analysis at baseline and 1 year
- Peak knee flexion in swing was preserved in the DRFT group but fell in the non-DRFT group; benefit was confined to patients with a pre-operative knee-flexion deficit (stiff-knee gait)
- Around one third of DRFT patients did not benefit and roughly half of non-DRFT patients avoided an unnecessary procedure, so DRFT is not recommended as a prophylactic add-on for severe flexed-knee gait
References
- Perry J, Burnfield JM. Gait Analysis: Normal and Pathological Function. 2nd ed. Thorofare, NJ: SLACK Incorporated; 2010.
- Whittle MW. Gait Analysis: An Introduction. 4th ed. Edinburgh: Butterworth-Heinemann; 2007.
- Bohannon RW. Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants. Age Ageing. 1997;26(1):15-19. doi:10.1093/ageing/26.1.15
- Baker R. Measuring Walking: A Handbook of Clinical Gait Analysis. London: Mac Keith Press; 2013.
- Gage JR, Schwartz MH, Koop SE, Novacheck TF. The Identification and Treatment of Gait Problems in Cerebral Palsy. 2nd ed. London: Mac Keith Press; 2009.
- Sutherland DH, Olshen R, Cooper L, Woo SL. The development of mature gait. J Bone Joint Surg Am. 1980;62(3):336-353.
- Winter DA. Biomechanics and Motor Control of Human Movement. 4th ed. Hoboken, NJ: John Wiley & Sons; 2009.
- Murray MP, Drought AB, Kory RC. Walking patterns of normal men. J Bone Joint Surg Am. 1964;46:335-360.
- Kadaba MP, Ramakrishnan HK, Wootten ME. Measurement of lower extremity kinematics during level walking. J Orthop Res. 1990;8(3):383-392. doi:10.1002/jor.1100080310
- Neumann DA. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 3rd ed. St Louis, MO: Elsevier; 2017.
- Leardini A, Benedetti MG, Berti L, et al. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture. 2007;25(3):453-462. doi:10.1016/j.gaitpost.2006.05.017
- Perry J. Gait Analysis: Normal and Pathological Function. Thorofare, NJ: SLACK Incorporated; 1992.
- Hardcastle P, Nade S. The significance of the Trendelenburg test. J Bone Joint Surg Br. 1985;67(5):741-746. doi:10.1302/0301-620X.67B5.4055873
- Whittle MW. Gait analysis in the assessment of soft tissue injuries. Defense Sci J. 1999;49(5):437-443. doi:10.14429/dsj.49.3852
- Saunders JB, Inman VT, Eberhart HD. The major determinants in normal and pathological gait. J Bone Joint Surg Am. 1953;35(3):543-558.
- Gard SA, Childress DS. The effect of pelvic list on the vertical displacement of the trunk during normal walking. Gait Posture. 1997;5(3):233-238. doi:10.1016/S0966-6362(96)01089-2
- Kirtley C. Clinical Gait Analysis: Theory and Practice. Edinburgh: Churchill Livingstone; 2006.
- Waters RL, Mulroy S. The energy expenditure of normal and pathologic gait. Gait Posture. 1999;9(3):207-231. doi:10.1016/S0966-6362(99)00009-0