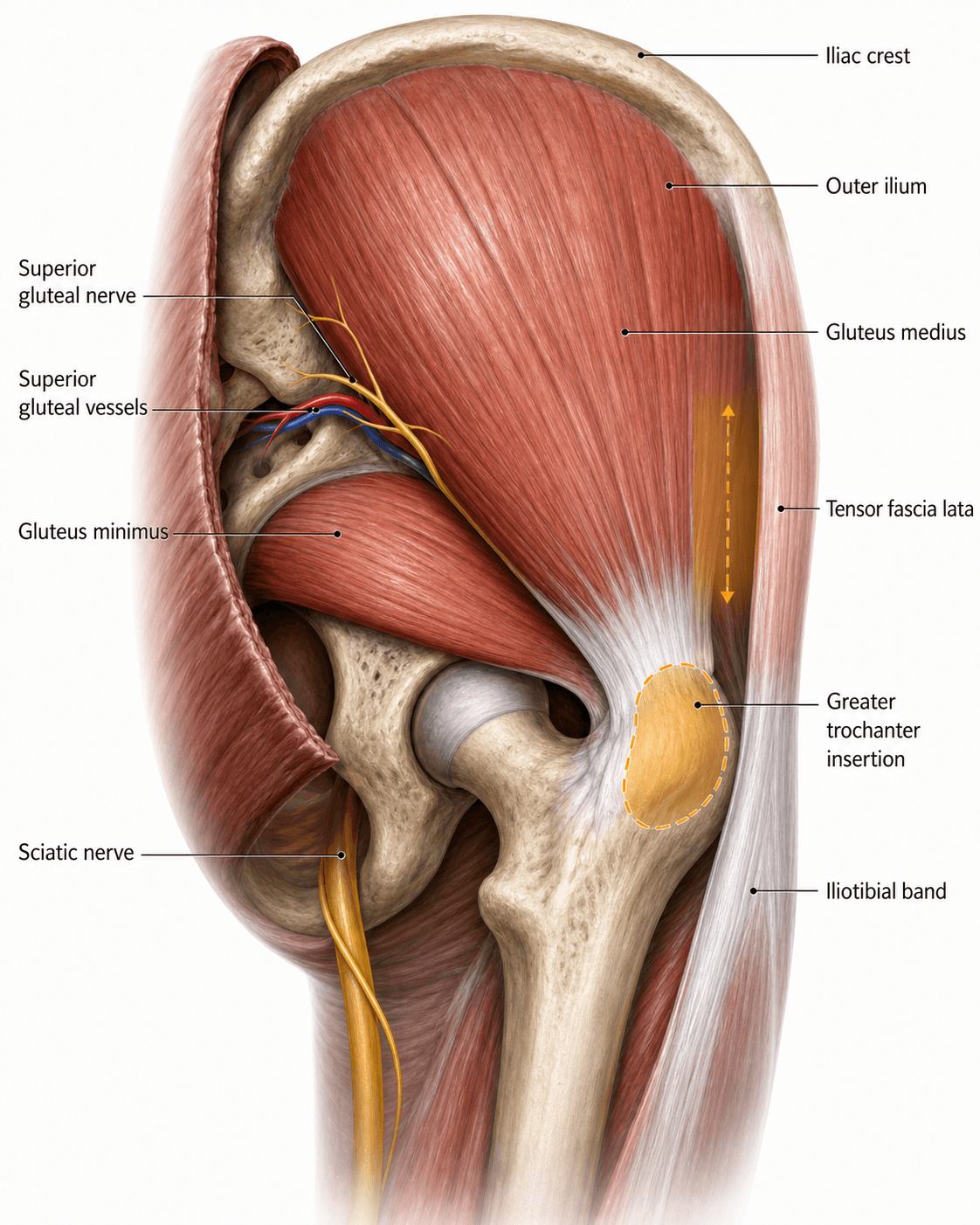
The Rotator Cuff of the Hip
- Originates from the Gluteal Surface of the Ilium (between Anterior and Posterior Gluteal Lines).
- Inserts onto the Lateral and Superoposterior Facets of the Greater Trochanter.
- Innervated by the Superior Gluteal Nerve (L4, L5, S1).
- Damage causes a positive Trendelenburg Sign (Pelvis drops to the CONTRALATERAL side).
- Commonly implicated in Greater Trochanteric Pain Syndrome (GTPS).
- “The 'Safe Zone' for intragluteal injection is the Upper Outer Quadrant (to avoid Sciatic and Superior Gluteal Nerves).
- “Trendelenburg Gait is uncompensated (pelvis drops); Duchenne Gait is compensated (trunk leans to affected side).
- “Tears behave like Rotator Cuff tears: Degenerative, painful, and prone to fatty atrophy.
- “The Superior Gluteal Nerve runs between Gluteus Medius and Minimus.
Proximal Extent.
- Running the split in a Hardinge approach too proximally (greater than 5cm from tip of GT) risks denervating the anterior tensor fasciae latae and anterior gluteus medius fibres.
- Result: Persistent limp (Trendelenburg).
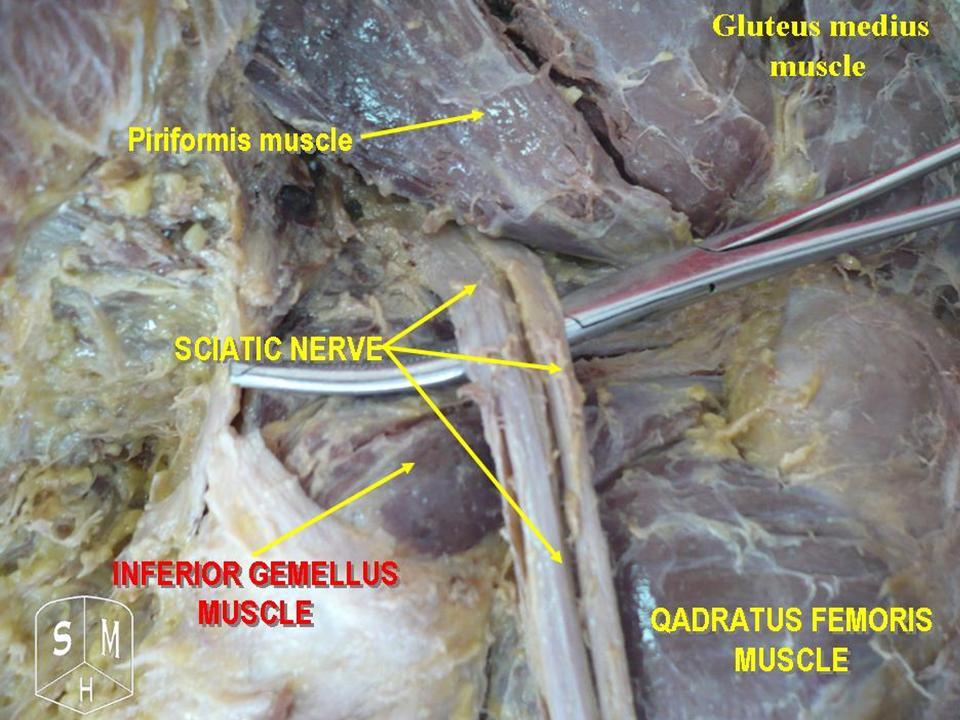
Posterior Relation.
- Although Gluteus Medius covers it, the Sciatic nerve emerges deep to Pyramidalis (Piriformis). Deep injections or incorrect retractor placement in the posterior approach can cause palsy.
- Safe Zone: Upper Outer Quadrant for injections minimizes risk.
- Origin
- Post Ilium/Sacrum
- Insertion
- ITB / Gluteal Tuberosity
- Nerve
- Inferior Gluteal (L5-S2)
- Origin
- Ilium (b/w Ant/Post Lines)
- Insertion
- GT (Lateral Facet)
- Nerve
- Superior Gluteal (L4-S1)
- Origin
- Ilium (b/w Ant/Inf Lines)
- Insertion
- GT (Anterior Facet)
- Nerve
- Superior Gluteal (L4-S1)
- Origin
- ASIS / Iliac Crest
- Insertion
- ITB
- Nerve
- Superior Gluteal (L4-S1)
SIPGluteal Nerves
Hook:Major nerves of the gluteal region.
LAMPInsertions on Greater Trochanter
Hook:The facets of the Greater Trochanter.
Sound Side SinksTrendelenburg Test
Hook:If strict logic fails, remember the Sound Side Sinks.
Overview
The Gluteus Medius is the 'deltoid of the hip'. It is fan-shaped and covers the Gluteus Minimus. It is critical for normal gait, stabilizing the pelvis in the coronal plane during the single-leg stance phase of walking. Weakness leads to a Trendelenburg gait.
The gluteus medius is the key to the single-leg-stance free-body diagram examiners love (Pauwels):
- In single-leg stance the pelvis pivots about the femoral head (the fulcrum). Body weight acts medially at a long moment arm; the abductors must pull laterally at a short moment arm to keep the pelvis level. Because the body-weight lever arm is roughly 2.5 times the abductor lever arm, the abductors generate about 2.5 times body weight of force, and the resultant hip joint reaction force is about 3 to 4 times body weight in stance and gait (more on stairs or running).
- What REDUCES the joint force / abductor demand: a walking stick in the CONTRALATERAL hand (it acts at a long lever arm and substantially cuts the joint force); leaning the trunk over the stance hip (the Duchenne lurch shifts the centre of gravity over the fulcrum); increasing femoral offset or lateralising the trochanter (lengthens the abductor lever arm); and medialising the acetabular cup (shortens the body-weight lever arm) — all relevant in hip arthroplasty.
- What INCREASES it: loss of offset, coxa valga (shortens the abductor lever arm), obesity, and carrying load on the ipsilateral side.
This is why restoring offset and a level pelvis matters in arthroplasty, and why a Trendelenburg-positive hip mechanically overloads the joint.
Neurovascular
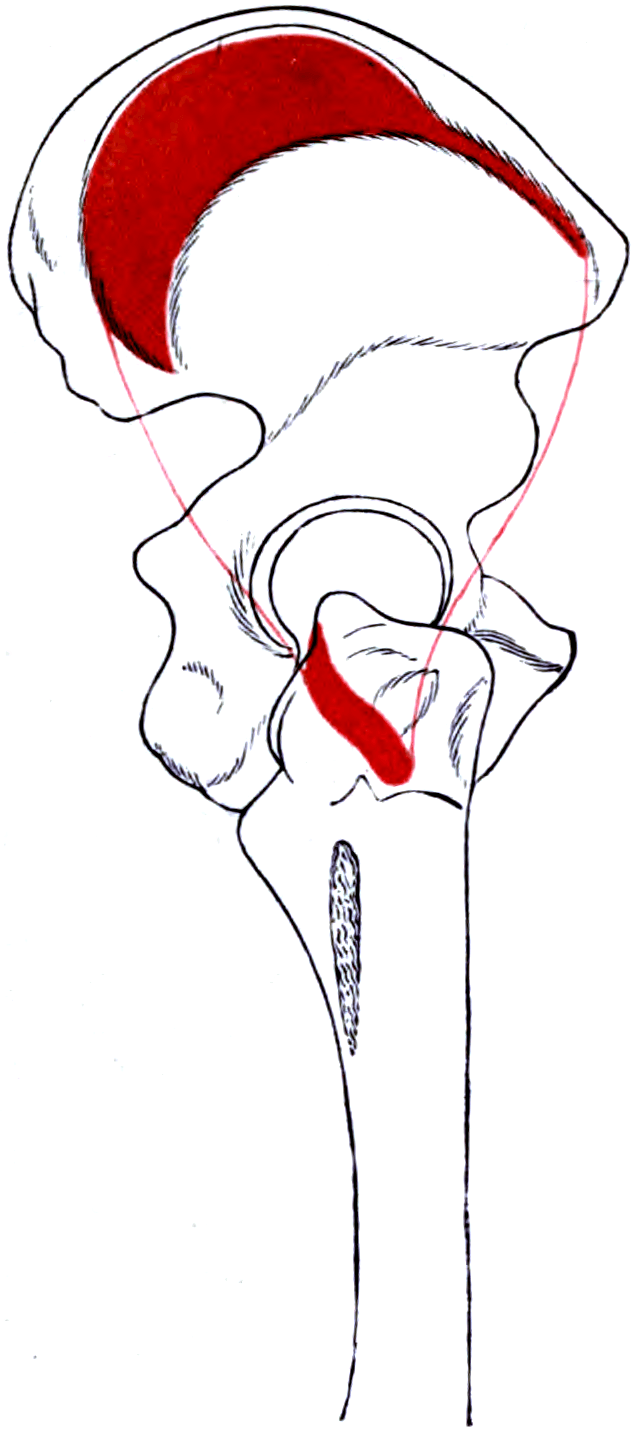
Origin
- Outer surface of Ilium: Between the Anterior Gluteal Line and the Posterior Gluteal Line.
- Fascia: Also originates from the overlying Gluteal Aponeurosis (covering fascia).
Insertion
- The fibers converge into a strong tendon.
- Greater Trochanter: Specifically the Lateral Facet and the Superoposterior Facet.
- Bursa: Two bursae are associated:
- Trochanteric Bursa: Between the tendon and the Greater Trochanter (main cause of GTPS).
- Subgluteus Medius Bursa: Deep to the muscle near insertion.
Surface Anatomy
Palpable Landmarks
- Iliac Crest: The superior border of the muscle.
- Greater Trochanter: The insertion point. Palpable on the lateral aspect of the hip.
- ASIS: Anterior Superior Iliac Spine.
Injection Safety (Upper Outer Quadrant)
- Draw a line from PSIS to Greater Trochanter.
- Injection should be superior and lateral to this line (Upper Outer Quadrant).
- This avoids the Sciatic Nerve (which is medial and inferior) and the Superior Gluteal Neurovascular bundle (which is deep but central).
Identifying these landmarks is crucial for safe practice to avoid iatrogenic nerve injury.
Pathology: GTPS
Greater Trochanteric Pain Syndrome (GTPS)
- Formerly called "Trochanteric Bursitis".
- Now understood as a spectrum: Tendinosis → Partial Tear → Complete Tear.
- "Rotator Cuff of the Hip": Similar pathophysiology to shoulder cuff disease.
- Risk Factors: Female gender (wider pelvis → increased varus moment), Obesity, LLD (Leg Length Discrepancy).
Understanding the mechanical overload is key to successful conservative management.
Classification Systems
MRI Classification of Tears
- Grade 1: Peritrochanteric edema (Bursitis/Tendinosis).
- Grade 2: Partial thickness tear.
- Grade 3: Full thickness tear (undisplaced).
- Grade 4: Full thickness tear with retraction (less than 2cm).
- Grade 5: Massive retraction (greater than 2cm) with fatty atrophy.
This classification guides the decision between endoscopic repair, open repair, and muscle transfer.
Clinical Assessment
Assessment of Stability.
-
Patient stands on ONE leg (the affected leg).
-
Negative (Normal): The contralateral pelvis rises (abductors pull ipsilateral pelvis down to level).
-
Positive (Abnormal): The contralateral pelvis DROPS.
-
Mechanism: Weakness of the stance-leg Gluteus Medius.
-
Note: The test must be held for 30 seconds to detect subtle weakness (fatigue).
Compensated vs Uncompensated.
- Trendelenburg Gait: Uncompensated. Pelvis drops with each step on affected side.
- Duchenne Gait: Compensated. Patient leans trunk TOWARDS the affected side during stance to shift center of gravity and reduce abductor demand.
- Bilateral Weakness: Results in a "Waddling Gait" (often seen in hip dysplasia or myopathy).
Resisted Abduction
- Patient in lateral decubitus.
- Abduct leg against gravity and resistance.
- Result: Pain indicates tendinopathy; weakness indicates a tear or nerve palsy.
The Trendelenburg test is the classic sign but is insensitive for a degenerate tear; examiners reward the more specific tests for gluteal tendinopathy / abductor tears:
- 30-second single-leg-stance test: the patient stands on the affected leg for up to 30 seconds; reproduction of lateral (trochanteric) pain is a sensitive sign of gluteal tendinopathy (distinct from the pelvic drop of a Trendelenburg test).
- Hip lag sign: in the lateral decubitus position the examiner passively holds the hip in extension, abduction and internal rotation with the knee flexed, then asks the patient to hold the leg there; the leg dropping (inability to actively maintain abduction) indicates an abductor tendon tear or insufficiency.
- Resisted external-derotation test (Lequesne): with the hip flexed to 90 degrees and externally rotated, the patient actively returns the leg to neutral against resistance; trochanteric pain indicates gluteal tendinopathy.
- Palpation of the greater trochanter for point tenderness and a lumbar/neurological screen (to exclude L5 radiculopathy) complete the examination.
The hip lag sign and the 30-second single-leg-stance test are highlighted in the Kenanidis review as useful clinical indicators of abductor insufficiency.
Investigations
X-Ray
- AP Pelvis: Check for calcification at insertion (calcific tendonitis) or avulsion fractures.
- Fleck Sign: Bony fragment superior to GT suggests avulsion.
Ultrasound
- Excellent for dynamic assessment and guided injection.
- Can visualize fluid in the bursa and tendon tears.
MRI
- Gold Standard.
- Shows muscle quality (fatty atrophy).
- T2 Fluid Signal: At insertion indicates tear/bursitis.
- Evaluate for muscle belly atrophy (nerve injury?).
Fatty infiltration is best assessed on the T1 axial sequence.
Differential Diagnosis of Lateral Hip Pain
Lateral hip and abductor-region pain has a wide differential. The examiner expects a structured separation of intra-articular, peritrochanteric, neurogenic and referred causes.
- Discriminating Feature
- Point tenderness over greater trochanter; night pain lying on side
- Key Test / Investigation
- Resisted abduction, single-leg stance; MRI/US
- Discriminating Feature
- Groin pain, stiffness, reduced internal rotation
- Key Test / Investigation
- FADIR, AP pelvis radiograph
- Discriminating Feature
- Groin pain, C-sign, younger patient
- Key Test / Investigation
- FADIR, MR arthrogram
- Discriminating Feature
- Radiating pain, neurology in foot (tibialis anterior, peronei)
- Key Test / Investigation
- Neurological exam, lumbar MRI, EMG
- Discriminating Feature
- Pain more distal/lateral with activity
- Key Test / Investigation
- Ober test, clinical
- Discriminating Feature
- Anterolateral thigh burning/numbness (LFCN)
- Key Test / Investigation
- Sensory mapping, nerve block
- Discriminating Feature
- Painless abductor weakness, positive Trendelenburg
- Key Test / Investigation
- EMG isolated to medius/minimus/TFL
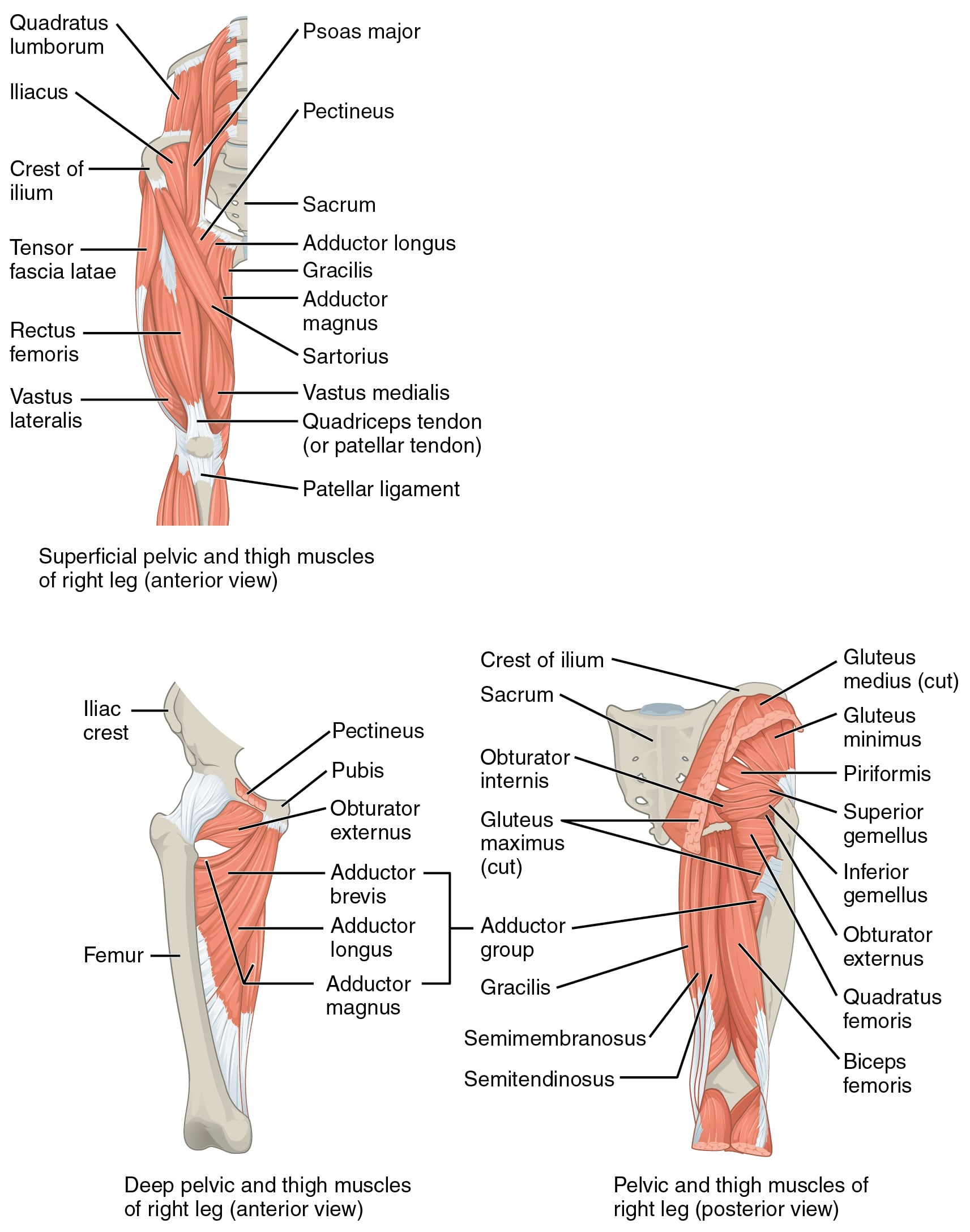
Surgical Technique
Anterolateral (Hardinge)
- Concept: Splits the Gluteus Medius (anterior 1/3) and Vastus Lateralis.
- Exposure: Excellent view of acetabulum.
- Risk: Superior Gluteal Nerve injury if split extends more than 5cm proximal to GT.
- Closure: Must repair the tendon meticulously to prevent limp.
Posterior (Moore)
- Concept: Splits Gluteus Maximus (Safe).
- Retraction: Gluteus Medius is retracted anteriorly.
- Risk: Traction injury to Superior Gluteal Nerve if retractor is too vigorous.
The posterior approach relies on the integrity of the anterior abductor muscle sleeve for stability.
Complications
- Persistent Limp: Failure of repair or nerve injury.
- Nerve Injury: Superior Gluteal (Abductor lurch), Sciatic (Foot drop).
- Recurrence: Re-tear rates are significant (10-20%).
- Heterotopic Ossification: Especially with lateral approaches.
Rehabilitation Protocol
- Phase 1 (0-6 weeks): Protected weight bearing (Crutches). No active abduction. Avoid adduction (crossing legs) which stretches repair.
- Phase 2 (6-12 weeks): Wean crutches. Aqua therapy. Isometric abduction.
- Phase 3 (3+ months): Strengthening. Return to sport/full activity.
Prognosis
- Conservative: 70-80% success for GTPS.
- Repair: Good pain relief (90%). Strength recovery is variable and takes longer (1 year).
- Fatty Atrophy: Presence of Goutallier 3/4 changes significantly lowers success rate.
Clinical Relevance
Treatment by Pathology
- Treatment
- Physio, NSAIDs, Injection
- Rationale
- Load management usually successful
- Treatment
- PRP? Shockwave? Repair?
- Rationale
- Conservative first. Repair if failed.
- Treatment
- Endoscopic/Open Repair
- Rationale
- Relieves pain and restores gait
- Treatment
- Gluteus Maximus Transfer
- Rationale
- Salvage for massive retraction
- Injections: Corticosteroids provide short term relief but may weaken tendon. PRP is controversial but gaining popularity.
Surgical intervention is reserved for those who fail 6 months of dedicated rehabilitation.
Guidelines, Registries & Global Practice
Global Epidemiology
- GTPS affects an estimated 10-25% of patients referred with hip/lateral thigh pain, with a population prevalence around 15% in women aged 50-79 versus roughly 6% in men (Segal NA et al., Arch Phys Med Rehabil 2007).
- Demographics: Female predominance (wider pelvis, larger abductor moment arm), peri-/post-menopausal age, obesity, leg-length discrepancy and ipsilateral knee/back pathology are recurrent risk associations.
- Abductor tears are increasingly recognised as a degenerative enthesopathy ("rotator cuff of the hip") found incidentally in up to 20% of older women on MRI and in a notable proportion of THA candidates.
Side-by-Side Guideline & Society Positions
- Position on Gluteal Tendinopathy / Abductor Tears
- Staged care: load modification, exercise, then image-guided injection; surgery for refractory tears
- Emphasis
- Evidence-graded conservative-first
- Position on Gluteal Tendinopathy / Abductor Tears
- Physiotherapy-led education plus exercise as first line; caution on repeated corticosteroid
- Emphasis
- Tendon-load rehabilitation
- Position on Gluteal Tendinopathy / Abductor Tears
- Respect superior gluteal nerve safe zone in transgluteal approaches; meticulous abductor repair
- Emphasis
- Surgical safety
- Position on Gluteal Tendinopathy / Abductor Tears
- MRI staging of fatty infiltration before repair; muscle transfer for irreparable tears
- Emphasis
- Prognostic stratification
- The LEAP randomised trial (Mellor R et al., Br J Sports Med 2018) underpins the global shift towards education plus exercise as first-line therapy, outperforming a single corticosteroid injection at one year.
Registry & Approach Notes
- Arthroplasty registries (NJR UK, AOANJRR Australia, AJRR US) track surgical approach but not abductor integrity directly; the posterior approach dominates worldwide, with the direct anterior and lateral (Hardinge) approaches as the main alternatives.
- Comparative MRI data show the transgluteal (Hardinge) approach produces more measurable abductor damage and a higher rate of post-operative limp than the intermuscular direct anterior approach (Bremer AK et al., JBJS Br 2011) - a key trade-off against the Hardinge's low dislocation rate.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: MRI staging, ultrasound-guided injections, endoscopic and arthroscopic abductor repair, and PRP/shockwave for tendinopathy.
- Limited-resource settings: Diagnosis rests on clinical examination (Trendelenburg, resisted abduction, single-leg stance) and plain radiographs; management is predominantly supervised exercise and selective open repair, with MRI and arthroscopy reserved for complex or surgical cases.
Controversies & Areas of Uncertainty
- Corticosteroid injections: Provide rapid short-term relief but are inferior to exercise at one year and may be catabolic to tendon. The role and number of injections remains debated, with a clear trend away from repeated steroid (LEAP trial, Mellor 2018).
- PRP and orthobiologics: Platelet-rich plasma and other biologics are increasingly used for gluteal tendinopathy, but high-quality comparative evidence is limited and results are inconsistent.
- Endoscopic vs open repair: Both achieve good pain relief; endoscopic techniques offer less soft-tissue dissection but have a steep learning curve. No large randomised comparison establishes superiority, and selection (tear size, retraction, atrophy) drives outcomes more than technique.
- The "safe zone" myth: The classic 5cm rule for the superior gluteal nerve is not reliably safe - cadaveric work shows the nerve runs lower in taller patients (Eksioglu 2003), so the true margin is patient-specific.
- Surgical approach for THA: The abductor-sparing advantage of the direct anterior approach (less measurable abductor damage on MRI) is weighed against its learning curve and complication profile; no approach is universally superior.
MCQ Practice Points
Q: Injury to the Superior Gluteal Nerve results in which gait deviation? A: Trendelenburg Gait (Uncompensated) or Duchenne Gait (Compensated). It does NOT cause a foot drop (that is Sciatic/Peroneal).
Q: A small bony fleck seen superior to the Greater Trochanter on AP Pelvis X-ray indicates what? A: Avulsion of the Gluteus Medius (or Minimus) insertion. It is the hip equivalent of a Segond fracture (ACL) or bony Bankart (Shoulder).
Q: Onto which facet does the Gluteus Medius primarily insert? A: Lateral Facet. The Minimus inserts on the Anterior Facet.
Q: The safe zone for intragluteal injection to avoid the Sciatic Nerve is? A: Upper Outer Quadrant.
Q: Besides abduction, what is the action of the anterior fibers of Gluteus Medius? A: Internal Rotation and Flexion. Posterior fibers do Extension/ER.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 70F presents 6 months after a Hardinge approach THR (Total Hip Replacement). She has a persistent limp. Why?”
“50F office worker, localized lateral hip pain, worse at night lying on that side. No trauma. X-ray normal. Diagnosis?”
“You are performing a lateral approach and need to extend your split proximally. How far can you go?”
Anatomy
- Origin: Ilium (Ant-Post Lines)
- Insert: Lateral Facet GT
- Nerve: Sup. Gluteal (L4-S1)
- Action: Abduct + Stabilize
Clinical
- Trendelenburg: Contralateral Drop
- Duchenne: Ipsilateral Lean
- GTPS: Lat Hip Pain
- Resisted Abd: Pain/Weakness
Surgery
- Hardinge: Split less than 5cm
- Repair: Lat Facet Anchor
- Safe Zone: Upper Outer Q
- Nerve @ Risk: Sup Gluteal
Evidence Base
Endoscopic Gluteus Medius Repair Outcomes
- 34 patients (32 women, mean age 57), 10 full-thickness and 24 partial-thickness tears, minimum 2-year follow-up
- Mean VAS pain fell from 6.6 to 2.4 (p less than 0.001) with significant gains across all four hip outcome scores
- 15 of 26 patients (58%) with a pre-operative gait deviation regained a completely normal gait; mean satisfaction 8.5/10
- No difference between suture-bridge and transtendinous techniques; 4 patients progressed to total hip replacement
LEAP Trial: Exercise vs Corticosteroid for Gluteal Tendinopathy
- Three-arm RCT of 204 patients with MRI-confirmed gluteal tendinopathy: education plus exercise (EDX) vs single corticosteroid injection (CSI) vs wait-and-see (WS)
- At 8 weeks, EDX gave the highest success rate on global change (77%) versus CSI (58%) and WS (29%)
- EDX outperformed CSI for both global improvement and pain at 8 weeks
- At 52 weeks EDX remained superior to CSI for global improvement; both beat wait-and-see
Reliability of the Superior Gluteal Nerve 'Safe Area'
- Cadaveric study of 23 hips measuring the distance from the SGN entry point into gluteus medius to the greater trochanter
- Distance correlated significantly with cadaver body height in both anterior and posterior regions
- The nerve lay within the classic 'safe area' in all anterior regions but only 78% of posterior regions
- Demonstrates the conventional safe zone is not reliably safe, especially in taller patients
Greater Trochanteric Pain Syndrome: Epidemiology
- Population-based cross-sectional study of 3026 community-dwelling adults aged 50-79
- Prevalence of GTPS was markedly higher in women (15.0% unilateral, 8.5% bilateral) than men (6.6% and 1.9%); odds ratio for women 3.37
- GTPS was independently associated with iliotibial band tenderness, knee osteoarthritis and low back pain
- Bilateral GTPS correlated with slower walk and chair-stand times
Abductor Preservation: Direct Anterior vs Transgluteal Approach
- Comparative MRI study of 50 hips (25 per group) one year after total hip replacement
- Tendon detachment, partial tears and tendinitis of gluteus medius and minimus were significantly less frequent with the direct anterior approach
- Peritrochanteric bursal fluid and fatty atrophy of the abductors were also reduced with the anterior approach
- No difference in tensor fasciae latae findings between approaches
Lesions of the Hip Abductors: Diagnosis and Management
- Comprehensive review confirming abductor tendinopathy is the commonest cause of lateral thigh pain, more prevalent in women and increasing with age
- MRI is the gold standard and the degree of muscle fatty infiltration has predictive value for repair outcome
- The hip lag sign and 30-second single-leg stance test are useful clinical indicators of abductor insufficiency
- Muscle transfers (gluteus maximus / vastus lateralis) are salvage options for chronic irreparable tears with significant atrophy